Outcomes of combined carbazochrome sodium sulfonate plus tranexamic acid therapy versus tranexamic acid monotherapy in traumatic brain injury: a retrospective cohort study in Japan
Jinsuke Mizuno, Yoshihisa Miyamoto, Yuichiro Matsuo, Kiyohide Fushimi, Ryota Inokuchi, Kent Doi, Hideo Yasunaga

TL;DR
This study compared the effectiveness of combining carbazochrome sodium sulfonate with tranexamic acid versus using tranexamic acid alone in treating traumatic brain injury in Japan.
Contribution
The study provides new evidence on the clinical outcomes of combined therapy versus monotherapy for traumatic brain injury in a large Japanese cohort.
Findings
Combined therapy did not significantly reduce 28-day in-hospital mortality compared to monotherapy.
Subgroup analysis showed a significant reduction in 7-day mortality for unarousable patients receiving combined therapy.
Routine use of carbazochrome sodium sulfonate may not be recommended based on the overall findings.
Abstract
Traumatic brain injury (TBI) is a major public health concern associated with substantial morbidity and mortality. In Japan, carbazochrome sodium sulfonate (CSS) is widely used, often in combination with tranexamic acid (TXA), for the management of various types of bleeding; however, studies on the effectiveness of CSS in TBI are scarce. Therefore, this study aimed to investigate the association between the use of CSS plus TXA versus TXA alone and the clinical outcomes in patients with TBI. This observational study was conducted using data retrieved from the Japanese Diagnosis Procedure Combination database between July 2010 and March 2022. We enrolled adult patients aged ≥ 16 years diagnosed with TBI who received TXA on the day of admission. Patients with chronic subdural hematoma, suspected TBI diagnosis, or severe extracranial trauma were excluded. The exposure was CSS plus TXA…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
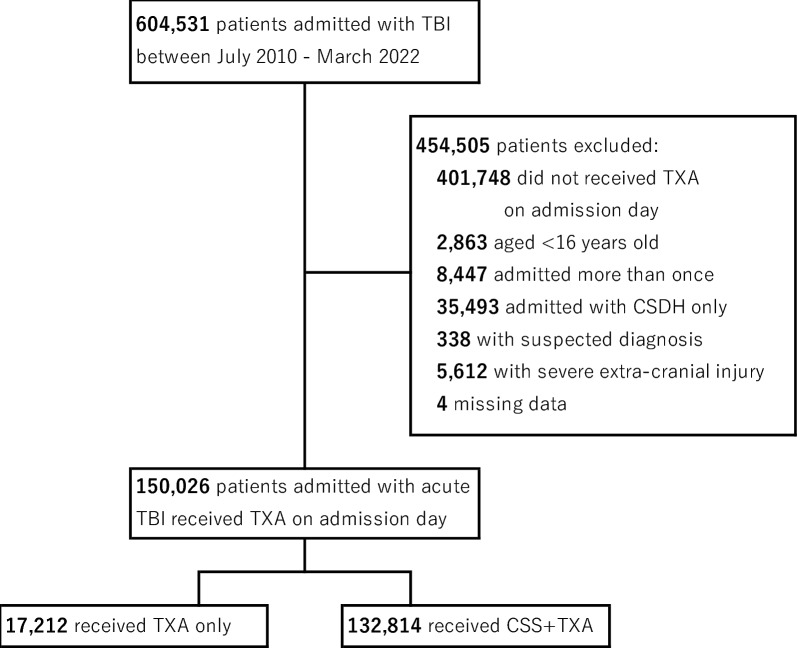 Figure 1
Figure 1- —https://doi.org/10.13039/501100003478Ministry of Health, Labour and Welfare
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBlood transfusion and management · Trauma, Hemostasis, Coagulopathy, Resuscitation · Traumatic Brain Injury and Neurovascular Disturbances
Background
Traumatic brain injury (TBI) is a major public health concern associated with substantial morbidity and mortality [1–3]. Secondary brain injury resulting from progressive intracranial hemorrhage (ICH), hematoma, and cerebral edema is an extremely serious complication of TBI, whose expansion can worsen the patient’s condition [4]. These conditions often require invasive surgeries and prolonged hospital stay that can compromise the patient’s quality of life or even result in fatality [5].
Although the current guidelines for TBI in the United States and Japan focus on decompressive craniectomy, therapeutic hypothermia, and osmotic drugs, evidence on the effectiveness of hemostatic drugs for preventing hematoma expansion has not been established [6, 7]. Recently, intensive investigations into the protective effects of tranexamic acid (TXA) have demonstrated an improvement in mortality in cases of severe trauma (CRASH-2 study [8]) and mild traumatic ICH (CRASH-3 study [9]). In addition to these major studies, the efficacy of TXA in TBI has been widely evaluated [10].
Carbazochrome sodium sulfonate (CSS) is another hemostatic agent introduced in the late 1940s [11, 12]. CSS is a stabilized metabolite of adrenochrome semicarbazone (an oxidized metabolite of adrenaline). Its hemostatic effect is primarily ascribed to the reduction in capillary permeability and increase in capillary resistance [13]. Another possible molecular mechanism involves inhibition of phosphatidylinositol hydrolysis in the vascular endothelial cells [14]. However, many studies have suggested that the direct effect of CSS on platelet aggregation and blood coagulation cascade is limited or non-existent [13, 14].
Currently, CSS is approved in countries such as Japan, China, Indonesia, and Egypt, but remains unapproved in the United States and most European countries. Since the 1960s, CSS has been commonly used in Japan, often in combination with TXA, for the management of a broad range of hemorrhagic conditions, including ICH, gastrointestinal bleeding, hemorrhoids, and hemoptysis [15–18], but the few studies conducted on its effectiveness have reported inconsistent results. According to single-center, observational studies, CSS use was not associated with an improved postprocedural bleeding rate (n = 304) [19] and lower mortality in patients with bleeding trauma (n = 259) [20]. A randomized controlled trial (n = 150) found that CSS reduced bleeding during hip replacement surgery [21], while a cohort study (n = 10) found that it controlled epistaxis in Osler’s disease [22]. However, the above-mentioned studies incorporated small sample populations, and none focused on TBI. Hypothetically, administering CSS in addition to TXA promotes capillary constriction, thereby leading to enhanced hemostasis and improved clinical outcomes in patients with TBI.
Therefore, we aimed to investigate the association of CSS plus TXA therapy versus TXA monotherapy with the outcomes in patients with TBI by analyzing large-scale data from the Diagnosis Procedure Combination (DPC) database. We compared TXA plus CSS with TXA monotherapy rather than comparing CSS with no-hemostats control for two reasons. First, TXA is already commonly used for hemostasis after TBI in Japan [23]. Second, the absence of hemostats may reflect a decision to limit care intensity, which would introduce significant selection bias.
Methods
Data source
This observational study was conducted using data retrieved from the Japanese DPC database [24]. The DPC database comprises discharge summaries and administrative claims data from voluntarily participating hospitals, representing over 1500 acute-care hospitals and encompassing approximately 50% of all beds from the latter [25]. It is a repository of patient demographics for all hospitalizations such as age, sex, and smoking history; diagnoses coded using the International Classification of Diseases, Tenth Revision (ICD-10); daily procedures recorded with the Japanese procedural codes; daily drug administration; and admission and discharge status. Interventions performed in the emergency department before hospital admission were designated as being performed on day 1 (the day of admission) when the patients were admitted through the emergency department. Pre-hospital administration of hemostatic agents is not performed in Japan. A previous validation study demonstrated high specificity and moderate sensitivity for the recorded diagnoses as well as high specificity and sensitivity for the recorded procedures [26]. This was a retrospective observational study and was not registered prospectively since trial registration is not applicable to this type of study.
Patient selection
We identified adult patients aged ≥ 16 years who were diagnosed with TBI (ICD codes: S061, S062, S063, S064, S065, S066, and S068; Supplemental Table 1) and treated with TXA on the day of admission between July 2010 and March 2022 from the database. Of note, the database utilizes the ICD-10 codes based on the Japanese standards issued in 2003 and revised in 2013, rather than ICD-10-CM. The revision in 2013 did not affect codes utilized in this study. Only the first admission was considered for patients who were admitted to the hospital more than once with a diagnosis of TBI. We excluded patients who fulfilled the following criteria: diagnosis of chronic subdural hematoma alone by text searching in the written Japanese diagnosis given along with the ICD-10 codes to focus on acute traumatic ICH since S065 includes both acute and chronic subdural hematoma; suspected diagnosis of TBI; and comorbid diagnosis of severe extracranial trauma according to the method described in the subsequent subsection.
Assessment of extracranial trauma severity
The Abbreviated Injury Scale (AIS) and Injury Severity Score (ISS) were used to quantify the severity of injury [27]. The AIS grades individual injuries into six severity levels ranging from 1 (minor) to 6 (unsurvivable). The ISS aims to determine the injury severity of each patient with single or multiple traumas by summing the squares of the AIS scores from the three most severely injured anatomical body regions. A patient with any injury rated as 6 on the AIS is automatically assigned a maximum ISS of 75. To identify patients with significant extracranial trauma, we first converted the ICD-10 codes to the AIS scores and their corresponding six anatomical body regions using the ICD-PIC-R data Table [28, 29] To make this data table suitable for the Japanese context, we converted the ICD-10 CM codes from the original table into the corresponding ICD-10 codes used in Japan by matching both code sets up to the fifth digit. Subsequently, we excluded patients whose converted AIS score was 3 or higher for any body region, except for the head, because an AIS of 3 (severe, but not life-threatening) is a widely accepted criterion for severe trauma [30]. Furthermore, we excluded patients identified with unique Japanese comorbid ICD-10 codes that indicated trauma accompanied by vascular and/or thoracoabdominal organ injuries (Supplemental Table 2). This methodological approach was adopted from a previous study that focused on predicting trauma-related mortality using modified Japanese ICD-10 codes [31].
Exposure and outcomes
The exposure was co-administration of CSS and TXA on day 1 (the admission day), with TXA monotherapy on day 1 assigned as the control group. The primary outcome was 28-day in-hospital mortality. The secondary outcomes included 7-day in-hospital mortality, overall in-hospital mortality, consciousness at discharge, and length of hospital stay. The level of consciousness at discharge was categorized using the four-point Japan Coma Scale (JCS): alert (0), awake without stimulation (1-digit: 1–3), arousable with stimulation (2-digit: 10–30), and unarousable (3-digit: 100–300). These categories demonstrate strong predictive accuracy for in-hospital mortality in patients with trauma and correspond well with the Glasgow Coma Scale (GCS)-based severity classification of mild (GCS 13–15), moderate (GCS 9–12), and severe (GCS 3–8) TBI.
Covariates
Based on previous studies [32–34] and clinical relevance, we included covariates from the following three main categories: patient characteristics at admission, treatment and procedures on day 1, and institutional and contextual characteristics. Patient characteristics at admission included age, sex, body mass index (BMI), smoking status (categorized as nonsmoker, current, or former smoker), and comorbidities as defined by the Charlson Comorbidity Index (CCI) [35]. BMI was classified according to the World Health Organization criteria for the Asian population [36]: less than 18.5, 18.5–22.9, 23.0–24.9, and 25.0 kg/m^2^ or more. We also included the head AIS score, ISS, injury type (traumatic cerebral edema, diffuse brain injury, focal brain hemorrhage, epidural hemorrhage, subdural hemorrhage, subarachnoid hemorrhage, and other specified intracranial injuries), and the JCS score at admission [37]. The JCS score at admission was treated as a granular categorical variable with 10 distinct levels to allow for the most rigorous adjustment possible. Treatment and procedures on day 1 included neurosurgery, noninvasive oxygen administration, intubation, dialysis, vasopressors, transfusion of fresh-frozen plasma and platelet concentrate, and anticoagulant-antagonist. Vasopressor use was regarded as a proxy for hypotension, transfusion of fresh-frozen plasma or platelet concentrate for coagulopathy, and anticoagulant-antagonist for anticoagulant medication, respectively. Details on neurosurgery are provided in Supplemental Table 3.
Institutional and contextual characteristics included fiscal year, season, TBI-related hospital volume, ambulatory transport, night/holiday admission, admission ward type (general ward; intensive care unit [ICU]; high-dependency unit [HDU]; stroke care unit [SCU]), and university hospital or non-university hospital. Seasons were categorized into March–May, June–August, September–November, and December–February. The TBI-related hospital volume was categorized by the number of annual admissions for the study cohort: 1–30, 31–60, and > 60 cases.
Statistical analysis
Missing values for BMI, smoking status, and ambulatory transport were imputed using multiple imputations with chained equations, and 20 sets of imputed data were created [38]. We used propensity score overlap weighting to account for potential confounding factors between the CSS plus TXA and TXA-only groups. The propensity score for the receipt of CSS plus TXA therapy was estimated by using a multivariable logistic regression model, which incorporated all the covariates mentioned earlier as independent variables. Overlap weighting was conducted using propensity scores. The overlap weighting method balances the treatment and control groups by assigning weights to each patient based on their probability of receiving the opposite treatment [39, 40]. As a result, individuals with a similar propensity to receive either of the two treatment regimens (viz. CSS plus TXA or TXA only) are assigned greater weights, whereas those with a lower propensity to receive the alternative treatment are assigned smaller weights. To evaluate balance, we calculated the absolute standardized mean differences (ASDs) for each variable between the two groups. An ASD value exceeding 10% indicates a significant imbalance. Finally, we conducted generalized linear regression analyses for the binomial outcomes to calculate the risk difference (RD) with its 95% confidence interval (CI) between the two treatment groups. We conducted proportional ordinal logistic regression to assess the distribution of the JCS scores at discharge and quartile regression for the length of hospital stay. We also performed a subgroup analysis according to the level of consciousness at admission: alert (JCS 0), awake (JCS 1–3), arousable (JCS 10–30), and unarousable (JCS 100–300). We also performed several sensitivity analyses. First, we performed a complete case analysis of missing values of smoking history and BMI. Second, we performed another analysis by adjusting for neurosurgery, intracranial pressure (ICP) monitoring, and administration of antihypertensive agents and osmotic agents on day 1. We excluded these interventions from the covariates in the main analysis because they could act as mediating factors in the pathway between the treatment and outcome. All statistical analyses were performed using STATA/SE version 19.0 (Stata Corp, College Station, TX, USA).
Results
A total of 150,026 adult patients with acute TBI were enrolled in this study. Of them, 11.5% (17,212/150,026) received only TXA and 88.5% (132,814/150,026) received CSS plus TXA (Fig. 1).Fig. 1. Patient selection flow diagram. TBI, traumatic brain injury; TXA, tranexamic acid; CSDH, chronic subdural hematoma; CSS, carbazochrome sodium sulfonate
Table 1 summarizes the baseline characteristics of the cohorts before and after propensity score overlap weighting (only major covariates are shown due to space limitation; the complete table is provided in Supplemental Table 4). In the unweighted cohort, patients in the CSS plus TXA group were less likely to be intubated or receive noradrenaline, fresh-frozen plasma, and platelets than those in the TXA-only group. TXA monotherapy was delivered more frequently in recent years, in teaching and university hospitals, when ambulances were used for patient transport, and less frequently on weekends or night admissions. Comorbidities and diagnosis of the type of head injury were not associated with treatment selection. After propensity score overlap weighting, the baseline characteristics appeared to be well balanced between the two groups. Table 1. Baseline patient characteristics before and after propensity score overlap weighting (summarized version)Before weightingAfter PS overlap weightingTXA onlyCSS plus TXAASDTXA onlyCSS plus TXAASDVariable(n = 17,212)(n = 132,814) Age, mean (SD)71.7(17.2)73.9(15.6)0.1372.4 (16.7)72.4 (16.6)0.00 Male10,584(61%)78,748(59%)0.05(61%)(61%)0.00Body mass index < 18.52774(16%)23,906(18%)0.05(17%)(17%)0.00 18.5–238029(47%)63,521(48%)0.02(47%)(47%)0.00 23–253081(18%)23,049(17%)0.01(18%)(18%)0.00 > 253328(19%)22,338(17%)0.07(19%)(19%)0.00 Current/past-smoker4938(29%)36,675(28%)0.02(29%)(29%)0.00Comorbidities Congestive heart failure535(3%)5284(4%)0.05(3%)(3%)0.00 Cerebrovascular disease1084(6%)10,749(8%)0.07(7%)(7%)0.00 Severe liver disease2180(13%)18,525(14%)0.04(13%)(13%)0.00 Diabetes323(2%)2428(2%)0.00(2%)(2%)0.00 Renal disease475(3%)4328(3%)0.03(3%)(3%)0.00 AIS of the head, mean (SD)1.8(0.8)1.7(0.7)0.061.8 (0.8)1.8 (0.8)0.00 ISS, mean (SD)4.4(4.1)3.9(3.3)0.144.2 (3.7)4.2 (4.1)0.00Details of head injury Brain edema16(0.1%)85(0.1%)0.01(0.1%)(0.1%)0.00 DAI3309(19%)22,853(17%)0.05(19%)(19%)0.00 Focal hematoma64(0.4%)482(0.4%)0.00(0.4%)(0.4%)0.00 AEDH85(0.5%)498(0.4%)0.02(0.5%)(0.5%)0.00 ASDH7747(45%)64,684(49%)0.07(46%)(46%)0.00 Traumatic SAH6517(38%)45,541(34%)0.07(37%)(37%)0.00 Others460(3%)4370(3%)0.04(3%)(3%)0.00Japan Coma Scale 0 (alert)4082(24%)37,718(28%)0.11(25%)(25%)0.00 1–3 (awake)6786(39%)59,850(45%)0.11(41%)(41%)0.00 10–30 (arousable)2424(14%)17,128(13%)0.04(14%)(14%)0.00 100–300 (unarousable)3920(23%)18,118(14%)0.24(20%)(20%)0.00 Intubation2861(17%)7886(6%)0.34(13%)(13%)0.00 Noradrenaline1042(6%)2808(2%)0.20(5%)(5%)0.00 FFP2100(12%)5999(5%)0.28(9%)(9%)0.00 Platelet625(4%)2529(2%)0.11(3%)(3%)0.00 Menatetrenone725(4%)6949(5%)0.05(4%)(4%)0.00Fiscal year 2010–2014^†^3734(22%)47,244(36%)0.31(24%)(24%)0.00 2015–2018^†^5470(32%)46,306(35%)0.07(33%)(33%)0.00 2019–2022^†^8008(47%)39,264(30%)0.36(44%)(44%)0.00TBI-related hospital volume, per year < 3111,023(64%)75,990(57%)0.14(62%)(62%)0.00 31–604783(28%)42,284(32%)0.09(29%)(29%)0.00 > 601406(8%)14,540(11%)0.10(9%)(9%)0.00Admission ward ICU4757(28%)22,414(17%)0.26(24%)(24%)0.00 HDU5714(33%)39,083(29%)0.08(33%)(33%)0.00 University hospital3054(18%)10,386(8%)0.30(15%)(15%)0.00Reported as n (%) or (%), unless indicated otherwise. The absolute standardized difference (ASD) was calculated after multiple imputations. †The Japan Coma Scale score at admission and the fiscal year were categorized due to space limitations. The SMD for the categorized covariates was separately calculated for the table. A complete version of the baseline characteristics is provided in the supplemental information (Supplemental Table 4)SD, standard deviation; AIS, Abbreviated Injury Scale; ISS, injury severity score; DAI, diffuse axonal injury; AEDH, acute epidural hemorrhage; ASDH, acute subdural hemorrhage; SAH, subarachnoid hemorrhage; FFP, fresh-frozen plasma; TBI, traumatic brain injury; ICU, intensive care unit; HDU, high-dependency unit
Table 2 shows the outcomes after propensity score overlap weighting. The primary outcome, i.e., the 28-day in-hospital mortality, was 11.7% and 11.9% in the TXA only and CSS plus TXA groups, respectively [RD, 0.1; 95% CI, -0.4 – 0.7%]. The 7-day in-hospital mortality, overall in-hospital mortality consciousness at discharge, and length of hospital stay were also similar between the two groups. Table 2. Comparison of clinical outcomes between the TXA-only and CSS plus TXA groups after propensity score overlap weightingOverlap weighted cohortOutcomesTXA onlyCSS plus TXARisk difference or effect size (95% CI)Primary outcome 28-day in-hospital mortality11.7%11.8%0.1% (− 0.4% to 0.7%)Secondary outcome 7-day in-hospital mortality7.9%7.6%− 0.4% (− 0.8% to 0.7%) In-hospital mortality13.1%13.6%0.5% (− 0.0% to 1.1%)Consciousness at discharge JCS 0 (alert)54.7%54.9%1.01 (0.96 to 1.05) JCS 1–3 (awake)27.7%26.7% JCS 10–30 (arousable)2.7%3.1% JCS 100–300 (unarousable)1.9%1.8% Length of hospital stay, days, median (IQR)14 (6–31)15(6–34)1 (− 0.2 to 2.2)For in-hospital mortality, the risk difference was calculated using a generalized linear regression model to compare the event probability in the CSS plus TXA group relative to the TXA-only group. Ordinal logistic regression was used to calculate the proportional odds ratio for consciousness at discharge, comparing the odds of being in a higher category for the CSS plus TXA group relative to the TXA-only group. For the length of hospital stay, the difference in the median was calculated using a median regression model to compare the median in the CSS plus TXA group versus the TXA-only group. All analyses were conducted after propensity score overlap weighting and multiple imputations for missing valuesTXA, tranexamic acid; CSS, carbazochrome sodium sulfonate; JCS, Japan Coma Scale; IQR, interquartile range
Table 3 shows the results of the subgroup analysis according to the level of consciousness at admission. In the unarousable patient subgroup, the 7-day in-hospital mortality was significantly lower in the CSS plus TXA group [32.4% in TXA only vs. 29.5% in CSS plus TXA group, RD -2.8% (95% CI -4.6% to -1.1%)], whereas the 28-day and total in-hospital mortality did not differ significantly between the treatment groups. Consciousness at discharge and the length of hospital stay were similar between the CSS plus TXA and TXA-alone groups. The results of sensitivity analyses (Table 4) approximated those of the main analysis. Before overlap weighting, neurosurgery on day 1 was performed in 13% (2,284/17,212) of patients in the TXA group and 10% (13,764/132,814) in the CSS plus TXA group, whereas after overlap weighting, the proportion was 12% in both groups (Supplemental Table 6). Table 3. Comparison of clinical outcomes in subgroups by the Japan Coma Scale score at admissionOverlap weighted cohortOutcomesSubgroupsTXA onlyCSS plus TXARisk difference or Effect size (95% CI)Primary outcome 28-day in-hospital mortalityJCS 02.5%2.8%0.3% (− 0.2% to 0.8%)JCS 1–33.8%4.1%0.2% (− 0.3% to 0.7%)JCS 10–308.0%9.0%1.1% (− 0.1% to 2.3%)JCS 100–30042.4%41.2%− 1.2% (− 3.0% to 0.7%)Secondary outcome 7-day in-hospital mortalityJCS 01.2%1.5%0.4% (0.0% to 0.7%)JCS 1–31.6%1.8%0.2% (− 0.2% to 0.5%)JCS 10–304.1%4.3%0.3% (− 0.6% to 1.1%)JCS 100–30032.4%29.5%− 2.8% (− 4.6% to − 1.1%) In-hospital mortalityJCS 03.1%3.7%0.6% (0.0% to 1.2%)JCS 1–34.9%5.6%0.7% (0.1% to 1.7%)JCS 10–309.7%11.5%1.8% (0.4% to 3.1%)JCS 100–30045.1%44.1%− 1.0% (− 2.8% to 0.9%)Consciousness at discharge JCS0 (alert)JCS 087.2%88.2%0.87 (0.76 to 1.00) JCS 1–3 (awake)9.1%7.6% JCS 10–30 (arousable)0.4%0.4% JCS 100–300 (unarousable)0.2%0.2% JCS0 (alert)JCS 1–354.0%54.3%0.98 (0.91 to 1.05) JCS 1–3 (awake)39.4%38.3% JCS 10–30 (arousable)1.2%1.5% JCS 100–300 (unarousable)0.5%0.3% JCS0 (alert)JCS 10–3048.1%47.4%1.12 (1.00 to 1.26) JCS 1–3 (awake)34.9%33.9% JCS 10–30 (arousable)5.8%6.2% JCS 100–300 (unarousable)1.4%1.0% JCS0 (alert)JCS 100–30019.6%19.3%1.00 (0.91 to 1.10) JCS 1–3 (awake)21.4%22.2% JCS 10–30 (arousable)6.6%7.3% JCS 100–300 (unarousable)7.2%7.1% Length of hospital stay, median (IQR)JCS 09 (4–20)9 (4–21)0 (− 1.3 to 1.3)JCS 1–314 (7–29)15 (6–31)1 (− 0.6 to 2.6)JCS 10–3023 (10–39)24 (11–43)1 (− 2.8 to 4.8)JCS 100–30018 (3–43)21(4–48)3 (− 1.4 to 7.4)We conducted subgroup analysis stratified by consciousness at admission. For in-hospital mortality, the risk difference was calculated using a generalized linear regression model to compare the event probability in the CSS plus TXA group relative to the TXA-only group. Ordinal logistic regression was used to calculate the proportional odds ratio for consciousness at discharge, comparing the odds of being in a higher category for the CSS plus TXA group relative to the TXA-only group. For the length of hospital stay, the difference in the median was calculated using a median regression model to compare the median in the CSS plus TXA group relative to the TXA-only group. All analyses were conducted after propensity score overlap weighting and multiple imputations for missing valuesTXA, tranexamic acid; CSS, carbazochrome sodium sulfonate; JCS, Japan Coma Scale; IQR, interquartile rangeTable 4Results of sensitivity analysis for the clinical outcomes, including a complete case analysis and an analysis with further adjustment for potential mediators (intracranial pressure monitoring, neurosurgery, and administration of antihypertensive agents and osmotic agents on day 1)Complete cases analysisOverlap weighted cohortOutcomesTXA onlyCSS plus TXARisk difference or effect size (95% CI)Primary outcome 28-day in-hospital mortality9.0%9.2%0.2% (− 0.4% to 0.7%)Secondary outcome 7-day in-hospital mortality5.6%5.4%− 0.2% (− 0.6% to 0.3%) In-hospital mortality10.4%10.9%0.6% (− 0.0% to 1.1%)Consciousness at discharge JCS 0 (alert)57.0%57.4%1.00 (0.95 to 1.06) JCS 1–3 (awake)28.6%27.1% JCS 10–30 (arousable)2.5%3.0% JCS 100–300 (unarousable)1.6%1.6% Length of hospital stay, median (IQR)15 (6–32)15 (6–35)0 (− 1.0 to 1.0)Further adjustment for possible mediatorsOverlap weighted cohortPrimary outcome 28-day in-hospital mortality11.6%11.7%0.1% (− 0.4 to 0.7%)Secondary outcome 7-day in-hospital mortality7.8%7.6%− 0.2% (− 0.7% to 0.2%) In-hospital mortality12.9%13.5%0.5% (− 0.1% to 1.1%)Consciousness at discharge JCS 0 (alert)54.8%55.4%0.99 (0.95 to 1.04) JCS 1–3 (awake)27.7%26.5% JCS 10–30 (arousable)2.7%3.0% JCS 100–300 (unarousable)1.9%1.7% Length of hospital stay, median (IQR)14 (6–31)14 (6–33)1 (− 1.2 to 1.2)The following sensitivity analyses were conducted: we performed complete cases analysis for missing values (body mass index, smoking history, and ambulance use); we further adjusted for potential mediators (intracranial pressure monitoring, neurosurgery, and administration of antihypertensive agents and osmotic agents on day 1) in propensity score overlap weighting. For in-hospital mortality, the risk difference was calculated using a generalized linear regression model to compare the event probability in the CSS plus TXA group relative to the TXA-only group. Ordinal logistic regression was used to calculate the proportional odds ratio for consciousness at discharge, comparing the odds of being in a higher category for the CSS plus TXA group relative to the TXA-only group. For the length of hospital stay, the difference in the median was calculated using a median regression model to compare the median in the CSS plus TXA group relative to the TXA-only group. TXA, tranexamic acid; CSS, carbazochrome sodium sulfonate; JCS, Japan Coma Scale; IQR, interquartile range
Discussion
Using a nationwide claims database, we found that the addition of CSS to TXA was not associated with improvements in in-hospital mortality in hospitalized adult patients with TBI. Consistent with this finding, there was no significant association with consciousness level at discharge or length of hospital stay, which we included as a proxy for post-discharge prognosis given that the DPC database does not provide follow-up data after discharge. It may be worth noting that the 7-day in-hospital mortality in unarousable patients was significantly lower in the CSS plus TXA group.
While previous studies have demonstrated meaningful differences in the intermediate outcomes (e.g., 5-unit difference in the packed red blood cell transfusion volume in trauma-related bleeding [41] and 200–500 mL difference in intraoperative blood loss during arthroplasty [21, 42, 43]), the difference in mortality reported by the other two studies investigating CSS use in trauma-related bleeding lacked statistical significance [20, 41]. Therefore, the absence of an overall benefit in our study is consistent with prior findings.
Although CSS is expected to promote hemostasis via reduced capillary permeability and vasoconstriction, our results showed no association between CSS and TBI-related in-hospital mortality. Two different hypotheses may explain this null finding. The first possible explanation involves a trade-off on mortality between hemostasis and perfusion. Previous trials in ICH have highlighted that hemostatic efficacy does not automatically translate to improved clinical outcomes [44, 45]. For instance, the FAST trial (recombinant activated factor VII) [45] and the TICH-2 trial (TXA) [44] demonstrated that while these agents reduced hematoma growth, they failed to improve functional outcomes, partly due to ischemic complications or other competing risks. Hypothetically, while CSS-induced vasoconstriction helps control bleeding, it may simultaneously decrease cerebral blood flow. This potential exacerbation of ischemia could cancel out the beneficial hemostatic effects of CSS on mortality. The other hypothesis involves the unique physiology of the cranium. In the closed intracranial space, hematoma expansion following TBI increases ICP, naturally leading to a tamponade effect that inhibits further bleeding [46, 47]. A retrospective study has reported that brain atrophy—which implies a reduced tamponade effect—was associated with hematoma expansion in ICH, particularly in the presence of coagulopathy [48]. This finding suggests that the tamponade effect likely plays a synergistic role with the coagulation system in maintaining hemostatic balance. Therefore, especially in severe cases where the physical tamponade effect is sufficiently operative, the added vasoconstrictive effect of CSS may offer little additional survival benefit. Moreover, our findings should be interpreted within the context of concurrent TXA use. When CSS is used in conjunction with TXA, the additional effect of CSS-induced vasoconstriction and reduced permeability beyond intracranial tamponade may be small, particularly when fibrinolysis-driven hematoma expansion—a major cause of early deterioration in TBI [49]—is already targeted by TXA.
Interestingly, our subgroup analysis showed that CSS co-administered with TXA yielded a small but significant short-term reduction in mortality among patients with JCS scores of 100–300 (unarousable). In such severe TBI, massive ICH may overwhelm the tamponade effect, particularly in the presence of excessive fibrinolysis and microvascular injury. In such situations, CSS may offer advantages by decreasing vascular permeability and promoting vasoconstriction [8, 9]. This could potentially be an advantage unique to CSS, conferred by a hemostatic mechanism that is distinct from that of TXA. However, the reduction in short-term mortality among unarousable patients should be interpreted with caution. The lack of difference in 28-day in-hospital mortality suggests that the initial survival benefit may have been offset by the severity of the primary injury or subsequent withdrawal of life-sustaining measures. Therefore, results of 7-day in-hospital mortality should be considered exploratory and hypothesis-generating. Further pharmacological investigations delving into the role of CSS in TBI that account for varying injury severities are expected to address this issue. The clinical relevance of CSS that extends beyond the reduction of mortality to the reduction of hematoma expansion and the subsequent need for surgical intervention may be of interest to future researchers.
Some limitations of this study should be acknowledged. First, this was a retrospective database study, and unmeasured confounders such as the mechanism of injury, exact timing of drug administration, pupillary findings, baseline prescriptions, and functional status may have influenced the results. Although we rigorously adjusted for available proxies such as reversal agents for anticoagulants and tracheal intubation for herniation signs, residual confounding cannot be fully excluded. Details of the drug regimen (e.g., dosage and method of administration) were not assessed. Although a study on endoscopic procedural bleeding did not suggest a dose-dependent difference in the hemostatic effect of CSS [50], existing evidence regarding CSS regimens in patients with TBI is scarce. Therefore, the optimal dosage and administration methods of CSS for TBI require further investigation in future studies. Second, some factors such as osmotic agents, antihypertensives, and neurosurgery were not included in the propensity score overlap weighting. As the DPC database does not provide the intraday treatment timing, we could not determine whether these agents functioned as confounders or mediators. To overcome this issue, we performed a sensitivity analysis adjusted for ICP monitoring, neurosurgery, and administration of antihypertensive agents and osmotic agents on day 1, which yielded results similar to those of the main analysis. Third, misclassification in ICD-10 diagnoses and extracranial injury severity from ICD to AIS mapping may have obscured the associations. Fourth, the specific cause of death could not be assessed due to the lack of coding in the database, restricting clinical interpretation. Fifth, the specific etiology of impaired consciousness at admission (e.g., post-traumatic seizures) could not be determined. Although it is unlikely that the decision to administer CSS differed systematically between groups, given the lack of seizure-related contraindications, residual confounding by unmeasured pathophysiological conditions cannot be fully excluded.
Conclusions
The co-administration of CSS with TXA was not associated with better clinical outcomes in terms of in-hospital mortality, consciousness at discharge, and length of stay in hospitalized adult patients with TBI compared with TXA monotherapy. Therefore, the routine use of CSS may not be recommended. While exploratory analyses suggested a potential short-term survival benefit among patients with severe consciousness impairment, these findings are hypothesis-generating. Future prospective studies are needed to validate these results and should ideally include assessment of intermediate outcomes, such as hematoma expansion and surgical interventions, to fully elucidate the clinical utility of CSS.
Supplementary Information
Supplementary Material 1.