Research progress on the influence of tumor microenvironment on immunotherapy for pancreatic ductal adenocarcinoma
Yuntao Yang, Yuying Zhang, Zhengchao Shen, Suhang Chen, Yajing Zhang, Xiaoming Wang

TL;DR
This paper reviews how the tumor microenvironment in pancreatic cancer limits immunotherapy effectiveness and explores strategies to overcome these challenges.
Contribution
The paper provides a comprehensive review of the tumor microenvironment's role in PDAC immunotherapy resistance and highlights potential reprogramming strategies.
Findings
The PDAC tumor microenvironment is highly immunosuppressive, limiting immunotherapy success.
Understanding TME components could lead to new treatment strategies for pancreatic cancer.
Reprogramming the TME may improve clinical outcomes for PDAC patients.
Abstract
Pancreatic ductal adenocarcinoma (PDAC) is a highly aggressive malignancy associated with a poor prognosis and considerable resistance to conventional therapies. While radical surgery may offer benefit for a subset of patients with early-stage disease, recent decades have witnessed notable progress in immunotherapy, yielding encouraging outcomes across both hematologic cancers and solid tumors in preclinical and clinical settings. Despite these advances, PDAC remains largely refractory to current immunotherapeutic strategies, owing largely to its unique tumor microenvironment (TME). The TME plays a pivotal role in modulating tumor progression, metastatic dissemination, and treatment response. It is commonly marked by a profoundly immunosuppressive milieu that attenuates effective anti-tumor immunity and complicates therapeutic intervention. The complex cellular and molecular composition…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
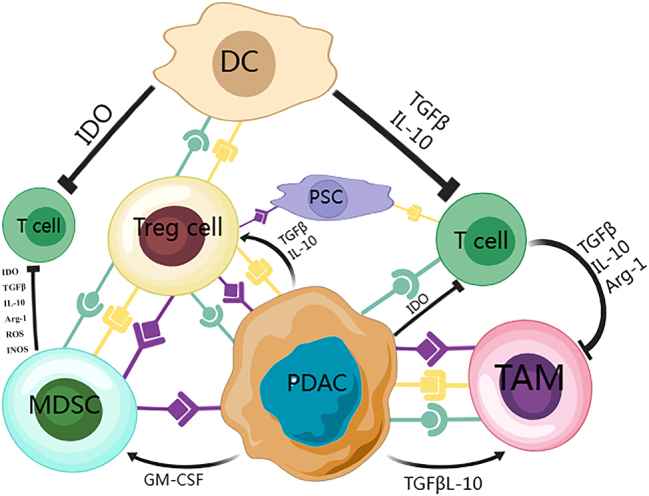 Figure 1
Figure 1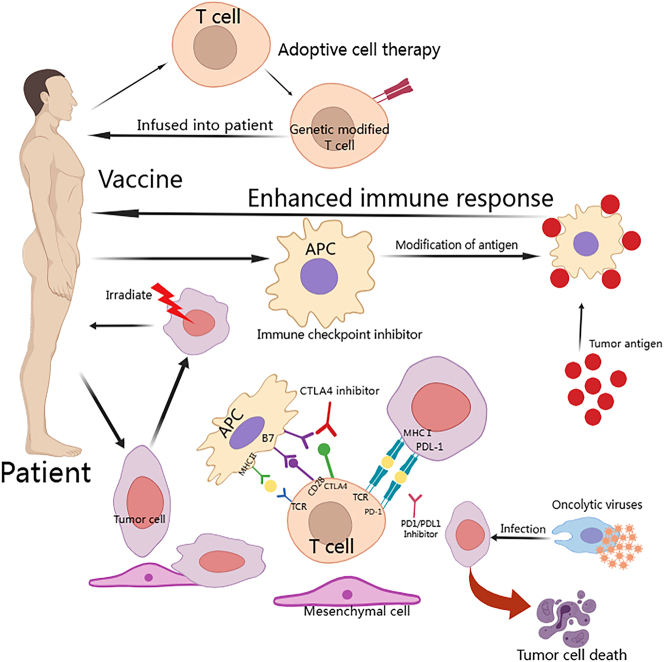 Figure 2
Figure 2| Immunotherapy treatment method | Description | Applicability | Major drugs/Technologies |
|---|---|---|---|
| Immune checkpoint inhibitors | By removing the negative regulatory molecules on T cells, the killing ability of T cells to tumors is enhanced | It is suitable for pancreatic cancer patients expressing the corresponding immune checkpoint molecules | Pembrolizumab nivolumab |
| Oncology vaccines | Fights tumors by activating the body’s immune response | It is mainly used for preventive immunization and is used in specific populations | Direct injection of tumor vaccines and genetically engineered vaccines |
| CAR-T cell therapy | The patient’s own T cells are genetically modified to give them the ability to recognize and destroy tumors | It is mainly for advanced, recurrent or unresectable locally advanced pancreatic cancer | CAR-T cell therapy technology |
| Adoptive T cell therapy | T Cells are harvested from the patient, expanded and modified | It can be used as an adjunct to improve the prognosis of patients with certain high-risk factors | Adoptive T cell therapy techniques |
| Immunomodulators | Cancer control is achieved by influencing the body’s immune microenvironment, such as regulating inflammatory responses or promoting immune cell activation | May be effective in patients with pancreatic cancer who have abnormalities in the immune microenvironment | Interferon a,y–interferon, etc |
| Vaccine name (type) | Clinical phase | Treatment regimen | Key outcomes | References |
|---|---|---|---|---|
| Autogene cevumeran (BNT122) (individualized mRNA neoantigen vaccine) | Phase 1 | Surgery + anti-PD-L1 (atezolizumab) + vaccine + mFOLFIRINOX chemotherapy | −50 % (8/16) of patients mounted a T-cell response | [ |
| ELI-002 2 P (off-the-shelf KRAS-targeted mRNA vaccine) | Phase 1 | Vaccine monotherapy (targeting KRAS mutations) | −84 % (21/25) T-cell response rate | [ |
| GVAX ± CRS-207 (whole-cell vaccine + bacterial vaccine) | Phase 2 | GVAX sequentially with CRS-207 vs. GVAX alone | − mOS 6.1 months in combo vs. 3.9 months with GVAX alone (HR=0.54) | [ |
| GVAX + nivolumab±urelumab (whole-cell vaccine + ICIs/agonist) | Phase 1/2 | Neoadjuvant/adjuvant setting. Three arms: A: GVAX; B: GVAX+Nivo; C: GVAX+Nivo+Urelumab | −30 % (3/10) achieved pathologic response (all partial) | [ |
| Trial name/Description | Treatment regimen | Phase | Primary outcomes | References |
|---|---|---|---|---|
| ICI + chemotherapy | Nivolumab + chemotherapy | Phase II | 1-year OS rate of 57.7 % (vs. 35 % in historical chemotherapy control) | [ |
| Meta-analysis: ICI + chemotherapy | ICI + chemotherapy vs. Chemotherapy alone | Meta-analysis | Improved OS (HR=0.82; 95 % CI: 0.78–0.87) | [ |
| Retrospective study in MSI-H/dMMR PDAC | Anti-PD-1 ± anti-CTLA-4 | Multicenter retrospective | ORR 48.4 %, median PFS 26.7 months, median OS not reached | [ |
| Meta-analysis: ICI + radiotherapy | ICI + radiotherapy vs. Control | Meta-analysis | Potential increased risk of death (HR=1.18; 95 % CI: 1.04–1.34) | [ |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPancreatic and Hepatic Oncology Research · Cancer Immunotherapy and Biomarkers · Immune cells in cancer
Introduction
Pancreatic cancer ranks among the deadliest cancers, exhibiting a notably high mortality rate. Approximately 90 % of these cases are classified as PDAC, which is recognized as the most aggressive variant. A large proportion of PDAC patients are diagnosed at an advanced stage, leading to a bleak 5-year survival rate of only 11 % [1]. The early signs of this disease are often subtle, leading to rapid progression and a generally poor prognosis. At present, the primary treatments for PDAC are surgery and chemotherapy, though their effectiveness remains limited.
In recent years, immunotherapy has gained recognition as a promising approach for cancer treatment, showing notable progress across various cancer types. However, its efficacy in pancreatic cancer has been mostly limited. This highlights the urgent need to explore the factors contributing to the limited success of immunotherapy in PDAC. Research indicates that a key factor is the tumor’s deep integration within a distinctive TME, where ongoing interactions among various cell types facilitate tumor progression [2], 3]. The TME has become increasingly acknowledged as a critical element that affects both tumor growth and response to therapy. In the sections that follow, we will examine how the TME and its predominant immunosuppressive elements play a role in the advancement of pancreatic cancer and the hurdles faced by immunotherapy.
Definition and composition of TME
TME refers to the surrounding area of tumor cells, which plays a critical role in tumor initiation, growth, metastasis, and response to treatment. It encompasses not only the structural, functional, and metabolic components of the tissue where the tumor resides, but also the internal environment of the tumor itself. The TME typically includes various immune cells, such as T lymphocytes, regulatory T cells (Tregs), tumor-associated macrophages (TAMs), and myeloid-derived suppressor cells (MDSCs). Additionally, it consists of the extracellular matrix (ECM) and several secreted molecules, including growth factors, cytokines, and chemokines. Stromal cells, especially cancer-associated fibroblasts (CAFs), are also key elements of this environment (Figure 1). These components often create an immunosuppressive environment that not only impedes normal mechanisms for tumor elimination but also enhances resistance to therapies.
Molecular interactions among different cells within the TME play a crucial role in PDAC. Cancer cells in PDAC employ various mechanisms, including cell surface molecules and soluble factors, to recruit and activate immune-suppressive cells, which directly or indirectly inhibit anti-tumor effector cells, thereby creating an immunosuppressive TME. These suppressive cells can impair effector cell function through mechanisms such as nutrient depletion, phenotypic changes, apoptosis, and energy regulation. Tregs are thought to play a central role in establishing the immunosuppressive TME in PDAC, as they promote the development of tumor-specific immune tolerance.
While the composition of the TME shows distinct variations, the immunosuppressive features and mechanisms that shape the diverse immune landscapes in PDAC have not been thoroughly investigated. Current research indicates that different ratios of stromal and immune cell types are associated with varying prognoses for patients with PDAC. In the sections that follow, we will examine the key factors within the TME that influence the effectiveness of tumor immunotherapy.
Immune cells
In numerous tumors, immune cells make up the largest portion of non-tumor components in the TME. The progression of PDAC is closely linked to various immunosuppressive cell types, such as Tregs, MDSCs, and TAMs, contributing to a highly immunosuppressive TME. Inflammatory responses primarily driven by myeloid cells, such as TAMs and MDSCs, are commonly seen in patients with PDAC. TAMs arise from either infiltrating monocytes or resident tissue macrophages [4]. These cells display considerable plasticity and can be found across a range of polarized states.
TAMs
Indeed, immune cells constitute one of the most pivotal stromal elements driving pancreatic ductal adenocarcinoma (PDAC) progression. Hijacking of the immune system is now recognized as a central route through which PDAC acquires therapeutic resistance [5]. Macrophages – key sentinels of innate immunity – dominate the immune landscape of PDAC, where they are commonly termed TAMs [6]. Derived from circulating monocytes, TAMs represent the principal inflammatory population in solid tumors and act as crucial mediators linking chronic inflammation to cancer development [7], [8], [9], [10]. TAMs influence cancer development through multiple pathways, such as initiating tumors via inflammation and supporting tumor progression and metastasis through immune evasion, angiogenesis, cancer cell invasion, and immunosuppression [11], 12]. In addition, TAMs exert potent immunosuppressive effects that shield tumor cells from natural killer (NK) cell- and T lymphocyte-mediated cytotoxicity, both during spontaneous tumor progression and following chemotherapy or immunotherapy.
TAMs, based on in vitro research, can be classified into two distinct polarization extremes. M1-like TAMs are believed to have antitumor functions, acting as antigen-presenting cells that produce IL-12, TNF, and inducible nitric oxide synthase. In contrast, M2-like TAMs promote tumor growth and possess immunosuppressive characteristics [13], [14], [15], [16]. Recent single-cell sequencing studies reveal that TAMs can account for 30–50 % of all immune cells in PDAC, predominantly display an M2-polarized phenotype, and are significantly associated with shorter overall survival [17]. Given the limited efficacy of conventional therapies that directly target cancer cells, TAMs have emerged as highly attractive targets for the prevention and treatment of pancreatic cancer.
MDSCs
The second key type of immunosuppressive cell in PDAC is MDSC. MDSCs are a group of cells with strong immunosuppressive properties, found in the spleens and tumor tissues of tumor-bearing mice, as well as in the blood and tumor sites of cancer patients [18]. Studies have shown that a network of immune cells, cytokines/chemokines, and signaling pathways critically governs the immunosuppressive activity of MDSCs [19]. In PDAC models, MDSCs mediate potent immune suppression and foster therapeutic resistance by dampening anti-tumor immune responses [20], [21], [22]. Consequently, MDSC frequency can serve as a liquid-biopsy biomarker for tracking disease progression and for predicting responsiveness to immunotherapy or chemotherapy in PDAC patients. Targeting MDSCs is therefore a promising strategy to potentiate both conventional cytotoxic drugs and immune-based agents. Indeed, the number of MDSCs in the peripheral circulation of PDAC patients correlates with advanced tumor stage [23]. Normally, bone marrow cells differentiate from hematopoietic stem cells (HSCs) into various mature cells like macrophages, dendritic cells (DCs), and granulocytes [24]. Novel therapeutic strategies are therefore being designed to elucidate the precise functional mechanisms underlying MDSC-mediated immunosuppression, with the ultimate goal of delivering a breakthrough for PDAC treatment.
Tregs
Tregs play a crucial role in balancing autoimmunity and immunosuppression. Within TME, they play a vital role, particularly in suppressing T cell activation. Increasing evidence shows that Tregs not only regulate abnormal immune responses against self-antigens but also significantly impair antitumor immunity and contribute to tumor development [25]. High Treg infiltration in the TME is associated with poor prognosis in multiple malignancies, including PDAC [26], 27]. In patients with PDAC, regulatory Tregs suppress anti-tumour immunity by crippling the activity of CD4^+^ and CD8^+^ T cells, macrophages, NKs and DCs [28], 29]. An expanded Treg pool in the PDAC TME also correlates with metastasis and shorter survival [30]. Yet across cancers, high intratumoural Treg numbers do not always portend a dismal prognosis. Selectively targeting Tregs to restore a pro-inflammatory, immunogenic TME is therefore an increasingly attractive therapeutic concept that has gained considerable momentum in recent years. Systemic ablation of Treg-mediated suppression, however, is constrained by the risk of severe autoimmunity that follows global Treg depletion. A deeper understanding of the molecular underpinnings of Treg inhibition – together with the metabolic reprogramming of both tumour and immune cells – will be essential for the development of safe, precision Treg-directed anti-cancer immunotherapies.
ECM
ECM is a dense meshwork of structural proteins, adhesive glycoproteins, proteoglycans and enzymes that provides both biochemical cues and mechanical integrity for tissue homeostasis. In PDAC, ECM deposition is markedly increased [31]. Both primary tumours and metastatic lesions display prominent desmoplasia and high abundance of ECM constituents such as hyaluronan and fibrillar collagens [32], indicating that robust fibrosis is a central driver of PDAC pathogenesis and prompting efforts to target ECM components therapeutically. Indeed, specific ECM molecules are linked to patient outcome: high intratumoural hyaluronan expression is associated with a median overall survival of 9.3 months compared with 24.3 months for low-expression tumours [32], whereas another study reported 6.4 vs. 14.6 months for high vs. low type I collagen levels [32]. In addition, aberrant ECM accumulation undermines therapeutic efficacy by acting as a physical barrier that impedes drug delivery while simultaneously activating integrin–focal adhesion kinase (FAK) signaling, which suppresses apoptosis, bolsters pro-survival pathways, and drives chemoresistance [33]. FAK activation is tightly linked to increased ECM stiffness in PDAC [34], and FAK1 itself has been identified as a key driver of both fibrosis and the immunosuppressive TME [35]. Indeed, the majority of human PDAC epithelia exhibit pronounced FAK expression and phosphorylation, a feature almost absent in normal pancreatic epithelium [36]. In KPC mice, treatment with a small-molecule FAK inhibitor markedly reduced tumor fibrosis, progression, and metastasis while concurrently decreasing infiltration of immunosuppressive myeloid cells, ultimately prolonging survival [35].
In summary, the ECM is a fundamental constituent of the pancreatic cancer stroma and plays a pivotal role in disease initiation and clinical progression. Regrettably, despite encouraging pre-clinical data, the most advanced ECM-targeting agent – PEGPH20 – failed to meet its primary end-point in PDAC clinical trials. Although this setback was disappointing, the ECM remains an attractive reservoir of therapeutic targets, and multiple follow-up studies rooted in positive pre-clinical PDAC models are now under way.
CAFs
CAFs are among the most crucial stromal cells within the TME. Activated CAFs play a role in promoting tumor progression, angiogenesis, invasion, metastasis, and even chemotherapy resistance, often through processes related to ECM remodeling. As key stromal components, CAFs display significant biological heterogeneity in terms of function, phenotype, and origin [37], 38]. In the pancreatic TME, various CAF subsets perform distinct roles [39], 40].
Although most CAF subsets promote tumor progression, some evidence suggests that certain subsets might have the opposite effect [41]. Numerous studies indicate that CAFs are involved in nearly every stage of tumor development via different pathways [42], 43]. By engaging in bidirectional communication with tumor cells and other components of the TME, and by secreting cytokines, chemokines, growth factors, and exosomes, CAFs not only promote tumor growth but also aid cancer cells in evading the immune system [44], 45]. Additionally, CAFs contribute to ECM degradation through the release of matrix metalloproteinases (MMPs) while simultaneously producing new matrix proteins, which supports tumor invasion and angiogenesis [46], 47].
Although therapies aimed at targeting CAFs need careful evaluation to ensure that they focus on tumor-promoting activities, they hold promise for enhancing PDAC treatment when combined with standard chemotherapy. In conclusion, while CAF-targeted therapies should be approached with caution, they offer a promising path to improving current PDAC treatments. Further research is essential to better understand the specific roles and mechanisms of CAFs in the progression of PDAC.
Immunotherapy for pancreatic cancer and its relationship with the TME
Pancreatic cancer is a highly aggressive malignancy with high rates of morbidity and mortality. Although immunotherapy has proven highly effective in many other cancers, it remains a relatively recent treatment option for pancreatic cancer, used alongside surgery and chemotherapy [48], [49], [50], [51], [52]. Treating PDAC remains a significant challenge, as standard treatments like FOLFIRINOX or gemcitabine-based chemotherapy provide only modest survival benefits, with most patients eventually experiencing disease progression and succumbing to it [53], 54]. One of the key characteristics of PDAC is its immunosuppressive microenvironment, which makes immunotherapy an attractive strategy. However, its effectiveness in pancreatic cancer is limited due to the unique biological behavior and TME of PDAC [55].
The pancreatic TME is highly heterogeneous, posing significant obstacles to immunotherapy. Multiple studies have shown that immune checkpoint inhibitors have minimal efficacy, and although early-phase clinical trials have shown some promise, whole-cell therapeutic vaccines have not succeeded in later-stage trials [48], 56], 57].
Several factors contribute to these failures, with the TME being a major one, characterized by poor infiltration of effector T cells, prominent myeloid-driven inflammation [57], [58], [59], [60], and a low mutation burden, leading to a scarcity of tumor-associated antigens [61], 62]. However, a small subset of PDAC patients has shown high infiltration of effector T cells and improved overall survival [63], [64], [65], indicating that immunotherapy could be effective in specific cases. This review explores different immunotherapeutic approaches for pancreatic cancer, such as immune checkpoint inhibitors (ICIs), vaccines, adoptive T cell therapies (like CAR-T), and immunomodulatory agents (Figure 2) (Table 1).
A schematic representation of immunotherapy. The approaches to immune treatment encompass immune checkpoint inhibitors, vaccines, adoptive T cell therapies, oncolytic viruses, and more.
Monotherapy immunotherapy for pancreatic cancer
ICIs
Cancer immunotherapy has delivered striking efficacy across multiple solid tumours, a leap largely driven by the advent of ICIs that elicit robust anti-tumour activity in most malignancies [66], [67], [68], [69], [70], [71]. These agents are monoclonal antibodies that neutralize key negative regulators of immunity – cytotoxic T-lymphocyte-associated antigen-4 (CTLA-4), programmed cell-death protein-1 (PD-1) and its ligand PD-L1 – thereby dismantling the molecular shields tumours use to evade immune surveillance [72]. By blocking inhibitory receptor–ligand interactions on T cells, ICIs re-invigorate exhausted lymphocytes and amplify physiological anti-tumour responses [73], 74]. Yet this success has not been universal. Despite remarkable advances in nearly every other cancer type, immunotherapy – ICIs in particular – has encountered formidable resistance in pancreatic ductal adenocarcinoma PDAC [56], 75]. Numerous clinical trials testing ICIs or alternative immunotherapeutic strategies in PDAC have yielded largely disappointing outcomes, especially when contrasted with the dramatic responses seen in melanoma, lung, or renal cancers.
Single-cell sequencing of anti-PD-1-treated PDAC mice revealed a surge in IFN-γ and consequent PD-L1 re-expression by day 7 [76]. In a clinical cohort, peripheral Treg frequency rose 3 weeks after pembrolizumab initiation and correlated with early progressive disease [77]. Moreover, in patients who received combined STING agonist plus anti-PD-1 therapy, those developing acquired resistance showed marked intra-tumoral up-regulation of AXL [78].
PDAC is characterized by an “immune-excluded” phenotype in which CD8^+^ T cells are confined to the tumor periphery, rendering the lesion largely refractory to immune-checkpoint blockade. Recent single-cell analyses have begun to dissect the multilayered circuits that orchestrate this exclusion. Tumor-cell-overexpressed DDR1, for example, aligns collagen fibers parallel to the tumor border, erecting a physical wall that impedes CD8^+^ T-cell infiltration; in DDR1-null models, collagen architecture is relaxed, T-cell influx increases and sensitivity to ICI is restored [79]. Cancer-associated fibroblasts further amplify exclusion by secreting TGF-β, which activates the CXCL12-CXCR4 axis and sequesters T cells in the stroma; blockade of TGF-β reverses this process and synergizes with anti-PD-1 therapy [80]. Mechanically, elevated ECM stiffness triggers nuclear translocation of focal-adhesion kinase (FAK), and the resultant STAT1/STAT3 complex represses MHC-I expression, blunting tumor recognition by T cells; FAK inhibitors re-establish antigen presentation and augment ICI efficacy [81]. Finally, single-cell profiling has revealed a sex-specific pathway: FPR2^+^ macrophages are markedly expanded in female PDAC and, via CCL2-and TGF-β-rich secretomes, intensify collagen deposition and T-cell exclusion; pharmacological antagonism of FPR2 enhances anti-PD-1 activity in pre-clinical models [82].
Collectively, these high-resolution studies portray PDAC immune exclusion as a multifactorial process – involving collagen re-organization, aberrant signaling, mechanotransduction and sex-biased immune circuits – and provide a rational framework for designing combination regimens that convert immune-desert tumors into immune-responsive lesions.
Tumor vaccines
Tumor vaccines have demonstrated the ability to elicit robust immune responses against tumors, but their performance in early-stage pancreatic cancer has been underwhelming. These vaccines, which consist of whole tumor cells, peptides, proteins, and recombinant constructs, aim to stimulate circulating tumor-specific T cells to target and destroy cancerous cells. Some research has also investigated the effectiveness of therapeutic vaccines in PDAC, often in combination with ICIs or chemotherapy. Among these, GVAX is the most studied [83]. GVAX is a whole-cell vaccine system commonly used for treating various cancers, including PDAC (84). The PDAC-specific version of GVAX is derived from two pancreatic cancer cell lines that have been genetically engineered to express GM-CSF. The vaccines are given intradermally and release significant amounts of GM-CSF, which draws in antigen-presenting cells (APCs) and promotes their maturation. While the vaccine has proven safe, its clinical impact has been limited [83], 84].
It is important to note that GM-CSF alone is insufficient for full APC maturation, as the presence of IL-4 is also required. The GVAX vaccine, which involves allogeneic pancreatic cancer cells modified to produce GM-CSF, has sometimes been paired with cyclophosphamide to deplete the TME and has shown the ability to induce T cell infiltration into the PDAC microenvironment [85], 86]. In small-scale phase I trials, almost all such vaccines produced tumor-specific T cell immunity in some patients [87], 88]. Interestingly, patients who developed vaccine-specific T cell responses in early trials often had higher survival rates. However, these early results have not been replicated in larger trials. A phase III trial using a single peptide derived from human telomerase (hTERT) failed to show a survival benefit for patients with metastatic disease, even among those who had an immune response [89]. Whole-cell vaccines have the potential to enhance the immune response to both tumor-specific and self-antigens, but their overall effectiveness has been constrained. GVAX, which uses irradiated allogeneic PDAC cells expressing GM-CSF, did not improve survival in metastatic PDAC in a phase IIb/III trial, even among immune responders [90]. These outcomes have lessened enthusiasm for therapeutic vaccines (Table 2).
Adoptive T cell therapy
Adoptive cell therapy is another form of immunotherapy, commonly applied to hematological cancers but increasingly being tested for solid tumors. T cell therapy, which involves the adoptive transfer of genetically modified tumor-targeting T cells, is emerging as a promising treatment for challenging cancers like PDAC [91]. Two primary methods are used for genetic modification [1]: T cells are engineered to express T cell receptors (TCRs) that recognize tumor antigens in the context of human leukocyte antigen (HLA); or [2] T cells are engineered to express chimeric antigen receptors (CARs), which directly bind to proteins, carbohydrates, or glycolipids on cancer cell surfaces, allowing them to bypass the frequent HLA downregulation observed in solid tumors [92].
CAR-T cell therapy has demonstrated remarkable success in specific forms of B-cell leukemia and lymphoma, but it encounters substantial obstacles that restrict its wider use in solid tumors and other hematological malignancies. In blood cancers, studies have shown that lymphodepletion before CAR-T cell therapy can improve efficacy, but the role of such conditioning regimens in solid tumors remains unclear [93].
CAR-T cells function as a “living drug,” customized for each individual patient. Present treatments involve harvesting the patient’s T cells, altering them genetically to produce CARs that detect and attach to particular proteins (tumor antigens) found on the surfaces of cancer cells. While cyclophosphamide, alone or combined with fludarabine (Cy/Flu), is the most common chemotherapy used in CAR-T trials, these drugs are not typically used for PDAC. Whether these or other cytotoxic therapies commonly used for PDAC, such as gemcitabine- or fluoropyrimidine-based treatments, can improve CAR-T efficacy is still being studied. These treatments may modify the tumor microenvironment (TME) by inducing immunogenic cell death, promoting local T cell infiltration, Tregs and MDSCs [94].
Despite the potential, several hurdles impede the success of CAR-T therapy, including serious toxicities like cytokine release syndrome (CRS), insufficient anti-tumor efficacy, antigen escape, and limited T cell trafficking [95], 96].
Immunomodulator
In pancreatic cancer, tumor cells release immunosuppressive cytokines that shape the TME, aiding in immune evasion. Immunomodulators are non-specific biological agents that enhance, promote, and regulate immune function. In pancreatic cancer treatment, commonly used immunomodulators include interferons (IFNs), interleukins (ILs), and other related molecules. Research has demonstrated that combining IL-10 with oncolytic viruses based on the vaccinia virus can boost the immune response against pancreatic cancer cells. IL-10, however, inhibits the secretion of IFN-γ and granzyme B, reducing the antitumor activity of CAR-T cells. Depleting IL-10 in the TME can significantly restore CAR-T cell function [97].
TGF-β plays a role in inducing T cells to acquire a regulatory phenotype. Blocking TGF-β signaling can reduce the activity of regulatory T cells in pancreatic cancer, thereby enhancing anti-tumor immunity [98]. Furthermore, combining IL-6 inhibitors with anti-PD-1 therapy has been shown to increase the number of CD8+ T cells within tumors, improving antitumor effectiveness compared to using immune checkpoint inhibitors alone [99].
Combination immunotherapy for pancreatic cancer
In solid tumors, low tumor immunogenicity and a highly immunosuppressive TME contribute to the intrinsic resistance to immune checkpoint blockade (ICB) therapy [100]. While immune checkpoint inhibitors (ICIs) can block inhibitory pathways that suppress effector T cell activity, the TME in pancreatic cancer contains numerous soluble factors that hinder the function of these effector T cells. Pancreatic cancer is characterized by a dense stroma, a low presence of tumor-infiltrating lymphocytes (TILs), and its classification as a “cold tumor,” which diminishes the efficacy of certain ICIs. The thick fibrotic matrix surrounding pancreatic cancer cells not only acts as a physical barrier but also limits drug penetration [101]. Reduced effector T cell presence and increased immunosuppressive cells within the TME contribute to creating a strongly immunosuppressive environment in pancreatic cancer, making ICI therapy alone largely ineffective [5]. Additionally, the fibrotic matrix may prevent TILs from infiltrating the tumor, while high expression of inhibitory receptors or ligands leads to T cell exhaustion. Immunosuppressive cells within the TME can further impair CD8+ T cell function, either through direct contact or paracrine signaling, contributing to resistance to ICIs [102]. Patients with low neoantigen heterogeneity and a higher number of clonal neoantigens tend to respond better to ICIs. However, given the low mutation burden in pancreatic cancer, the response to ICIs remains poor [103].
Although single-agent immunotherapy has not delivered the desired results, combining it with other treatment modalities has shown potential to significantly improve outcomes. Whole-genome analyses have revealed significant heterogeneity among pancreatic cancer patients, suggesting that personalized treatment approaches may enhance the effectiveness of immunotherapy. Given the variability in individual responses, some studies have developed an “immune score,” combining immunohistochemistry and gene expression data to evaluate immune cell infiltration and predict immunotherapy efficacy [104]. The role of the TME in pancreatic cancer metastasis highlights the importance of understanding its unique features in designing more effective immunotherapeutic strategies [50].
Looking ahead, future immunotherapies for pancreatic cancer are likely to shift from single-agent ICIs to combination therapies. This could include combinations of different immunotherapies or integrating immunotherapy with chemotherapy, radiotherapy, and targeted therapy [105], 106]. The success of immunotherapy depends on activating or modulating the immune system to specifically target tumor cells, and various immunotherapeutic approaches can achieve this [107] (Table 3).
Finding the most effective combination therapies will be essential for progressing immunotherapy in pancreatic cancer. While this review focuses on immunotherapy, key combinations will likely involve standard treatments like chemotherapy and radiotherapy, which can enhance the immune response through immunogenic cell death. The vast number of potential combinations exceeds the current capacity for clinical trials, so those targeting complementary mechanisms in the anti-tumor immune response will be prioritized. For instance, integrating therapeutic vaccines to stimulate T cells, checkpoint inhibitors to avoid exhaustion, and matrix modulation to improve T cell infiltration could address different mechanisms and may prove to be highly effective. However, challenges remain, including managing toxicity, optimizing dosage, and determining the best treatment sequence, especially for immune agonists. For instance, while the combination of nivolumab and ipilimumab has significantly improved survival in melanoma patients compared to monotherapy, it also increases toxicity and cost [108], [109], [110], [111].
An ideal combination therapy would also include reliable immune pharmacodynamic biomarkers to quickly assess treatment response. Because of the heterogeneity of tumors and individual differences, pancreatic cancer has exhibited a lower response rate to immunotherapy in comparison to other solid tumors. However, based on results from other cancers, combining immunotherapy with chemoradiotherapy and targeted therapies is expected to outperform single-agent treatments [90], 112]. These combination therapies can potentially improve survival by reshaping the immune microenvironment and converting “cold” tumors into “hot” ones [113]. Continued research into diverse immunotherapy approaches and rational combinations with other treatments may offer the most promising outcomes for PDAC.
Due to the heterogeneity of tumors and individual differences in pancreatic cancer, immunotherapy has not proven to be as effective as it is for other solid tumors. However, based on promising results from other cancers, combining immunotherapy with chemoradiotherapy and targeted therapies is expected to be more effective than single-agent approaches [90], 112]. With many possible combinations and a relatively small patient population, prioritizing treatments targeting distinct mechanisms supported by preclinical studies will be essential. Although treating PDAC is challenging, there is still hope for the development of effective therapies that can treat and eventually prevent this devastating disease.
Conclusion and prospect
The treatment landscape for PDAC is shifting, as therapies have historically been based on patient functional status and disease stage. In 2023, we are experiencing a time of therapeutic progress and heightened complexity, with a stronger focus on identifying biomarkers for categorizing patient subgroups. Nevertheless, there is still a demand for more reliable predictive and prognostic biomarkers to inform treatment choices. As clinical trials and technologies evolve over the next decade, outcomes for PDAC are expected to improve with the broader adoption of biomarker-driven strategies for cytotoxic chemotherapy, targeted therapies, and immunotherapy.
In the past decade, preclinical and clinical studies have highlighted the importance of both the adaptive and innate immune systems in the immune surveillance of PDAC. Yet, clinical results from PDAC immunotherapy trials have been less promising. It is critical to reconcile these encouraging preclinical findings with the underwhelming clinical trial outcomes and to understand why certain trials fail despite sound scientific foundations. This review focuses on the characteristics of the TME in PDAC and its influence on immunotherapy. Emerging evidence highlights the need to understand the complex roles that TME components play in both tumor suppression and progression, making it essential to study the drivers of TME organization and immunosuppression while exploring ways to target them effectively.
Although immunotherapy has shown initial promise in treating pancreatic cancer, achieving substantial clinical benefits has proven challenging. Each failed late-stage trial has highlighted the growing recognition that single-agent immunotherapy is unlikely to succeed in PDAC, making combination therapies a more promising approach. As immunological strategies for treating and managing PDAC continue to evolve, improving patient quality of life should remain a top priority. Many immunotherapy trials for PDAC have yielded disappointing results, largely due to the immunosuppressive nature of the TME. Consequently, existing immunotherapies must be refined and optimized to overcome this barrier, and novel immunotherapy targets identified in preclinical studies must be further explored in human clinical trials to confirm their potential.
One of the key questions yet to be answered is why many pancreatic cancer patients do not respond to immunotherapy. We must also explore the feedback mechanisms that occur during treatment and how they can be leveraged in combination therapies, particularly when factoring in prior chemotherapy and/or radiotherapy. Another important consideration is how to tailor treatment decisions based on the personalized characteristics of each patient’s TME. Given the relatively low incidence of PDAC, future trials should prioritize in-depth analysis of the TME and personalized treatment approaches to accelerate progress toward more effective therapies.
Despite numerous trial setbacks, our growing understanding of the PDAC TME and new therapeutic strategies offer hope for more effective future treatments. In summary, PDAC continues to be a highly deadly disease, underscoring the urgent need for innovative and enhanced treatment options. While immunotherapy has achieved significant success in other solid tumors, its application in PDAC, due to the complex TME, may require combination approaches rather than single-agent therapies. Although identifying the optimal combinations and selecting the right patients remain challenging, carefully designed studies are essential for maximizing the potential of immunotherapy and enhancing outcomes for this challenging disease.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Stoffel EM Brand RE Goggins M Pancreatic cancer: changing epidemiology and new approaches to risk assessment, early detection, and prevention Gastroenterology 20231647526510.1053/j.gastro.2023.02.01236804602 PMC 10243302 · doi ↗ · pubmed ↗
- 2Cheng K Cai N Zhu J Yang X Liang H Zhang W Tumor-associated macrophages in liver cancer: from mechanisms to therapy Cancer Commun 20224211124010.1002/cac 2.12345 PMC 964839436069342 · doi ↗ · pubmed ↗
- 3Ho WJ Jaffee EM Zheng L The tumour microenvironment in pancreatic cancer - clinical challenges and opportunities Nat Rev Clin Oncol 2020175274010.1038/s 41571-020-0363-532398706 PMC 7442729 · doi ↗ · pubmed ↗
- 4Zhu Y Herndon JM Sojka DK Kim KW Knolhoff BL Zuo C Tissue-resident macrophages in pancreatic ductal adenocarcinoma originate from embryonic hematopoiesis and promote tumor progression Immunity 20174732338.e 610.1016/j.immuni.2017.08.01828813661 PMC 5578409 · doi ↗ · pubmed ↗
- 5Sideras K Braat H Kwekkeboom J van Eijck CH Peppelenbosch MP Sleijfer S Role of the immune system in pancreatic cancer progression and immune modulating treatment strategies Cancer Treat Rev 2014405132210.1016/j.ctrv.2013.11.00524315741 · doi ↗ · pubmed ↗
- 6Balkwill FR Mantovani A Cancer-related inflammation: common themes and therapeutic opportunities Semin Cancer Biol 201222334010.1016/j.semcancer.2011.12.00522210179 · doi ↗ · pubmed ↗
- 7Chen Q Zhang XH MassaguéJ Macrophage binding to receptor VCAM-1 transmits survival signals in breast cancer cells that invade the lungs Cancer Cell 2011205384910.1016/j.ccr.2011.08.02522014578 PMC 3293160 · doi ↗ · pubmed ↗
- 8Fan QM Jing YY Yu GF Kou XR Ye F Gao L Tumor-associated macrophages promote cancer stem cell-like properties via transforming growth factor-beta 1-induced epithelial-mesenchymal transition in hepatocellular carcinoma Cancer Lett 2014352160810.1016/j.canlet.2014.05.00824892648 · doi ↗ · pubmed ↗