Experiences of women from ethnic minorities and underserved, marginalised and disadvantaged groups in communicating with health professionals during antenatal care: An overview of qualitative systematic reviews
Kusum Singal, Moira Cruickshank, Aniebiet Ekong, Clare Robertson, Pauline McDonagh Hull, Denitza Williams, Tara Fairley, Louise Locock, Mary Kilonzo, Mo Ade, Lilla Braithwaite, Debra Bick, Declan Devane, Magdalena Rzewuska Diaz, Gillian Taylor, Siladitya Bhattacharya

TL;DR
This study summarizes how women from ethnic minority and disadvantaged groups experience communication with healthcare professionals during pregnancy care in high-income countries.
Contribution
The study provides a thematic synthesis of qualitative reviews highlighting communication barriers and positive experiences in antenatal care for marginalized women.
Findings
Women faced challenges like language barriers, cultural differences, and discrimination in maternity care.
Positive experiences included respectful communication, interpreters, and culturally sensitive care.
Limited access to services was influenced by costs, transportation, and negative attitudes from staff.
Abstract
Maternal mortality rates show disproportional disparities among disadvantaged groups. To conduct an overview of qualitative systematic reviews to summarise the antenatal care experience of ethnic minority and underserved, marginalised and disadvantaged women in high-income countries. Seven electronic databases were searched to identify reviews published between 2011-2022. Two reviewers independently screened search results and full texts of potentially eligible articles. Data were extracted by two independent reviewers, critically appraised using the JBI tool and assessed for overlap. A thematic analysis was conducted. Nineteen qualitative reviews were included. Most were conducted in the UK (n=12) and provided a thematic synthesis of findings. Studied populations included women from minority ethnic groups and those who were migrants, homeless, refugees, asylum seekers, disabled,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
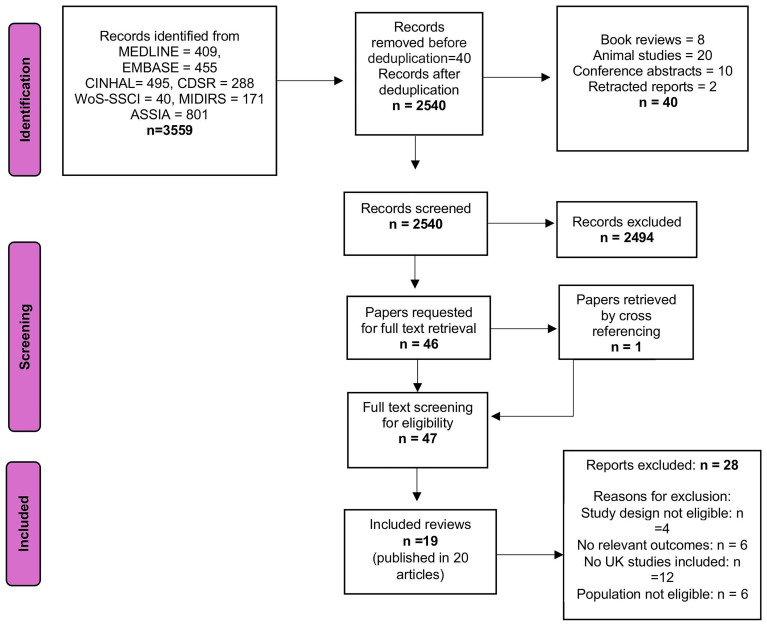 Figure 1
Figure 1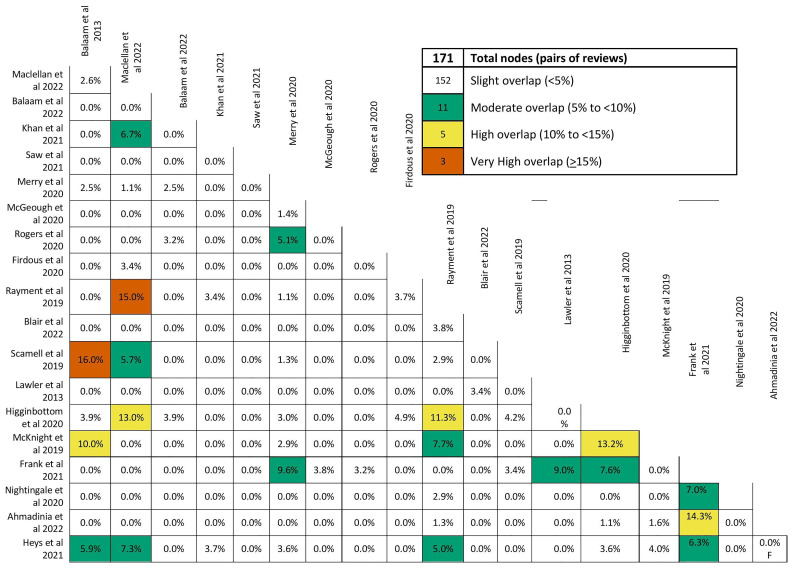 Figure 2
Figure 2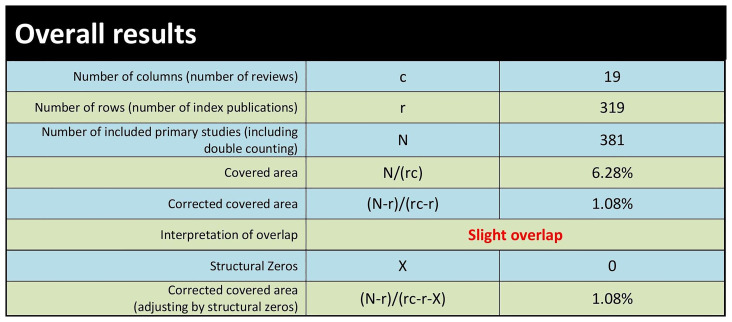 Figure 3
Figure 3| Inclusion criteria | Exclusion criteria | |
|---|---|---|
|
| Women from ethnic minorities and from underserved, marginalised and
| Population of unselected pregnant
|
|
| Experiences of communication and interaction with healthcare professionals during antenatal care.
| |
|
| Systematic reviews of primary qualitative studies. | |
|
| Studies conducted in settings relevant to the UK (defined as systematic reviews where most studies are conducted in
| |
|
| 2011 onwards. In the UK, the recommendation from the National Institute for Health and Care Excellence (NICE)
| |
| Author & Year | Geographical
| Population
| Number of
| Major identified themes and sub-themes | Quotes related to themes
| Overall
|
|---|---|---|---|---|---|---|
| Balaam
| UK | Migrant
| 495 women
|
| NR | Good |
| MacLellan
| UK | BAME women | 760
|
|
| Good |
| Balaam
| UK | Asylum-
| 760
|
|
| Good |
| Saw
| Australia | Women with
| 24676
|
|
| Good |
| Khan
| UK | Black, Asian
| 24645
|
| NR | Moderate |
| Merry
| Canada | Migrant
| 69 studies |
| NR | Good |
| McGeough
| Ireland | Homeless
| 277 women
|
|
| Good |
| Rogers
| Australia | Migrant
| 1499 women
|
| NR | Good |
| Firdous
| UK | Muslim
| 142 women
|
|
| |
| Rayment-
| UK | Women
| 22 studies |
|
| Moderate |
| Blair
| Australia | Women with
| 27 studies |
|
| Moderate |
| Scamell &
| UK | Women
| 609 women
|
|
| Moderate |
| Lawler
| Ireland | Women with
| 28 studies |
| NR | Poor |
| Higginbottom
| UK | Immigrant
| 40 studies |
|
| Good |
| McKnight
| UK | Asylum-
| 89 asylum
|
| NR | Good |
| Nightingale
| UK | Trafficked
| 13 studies |
|
| Moderate |
| Ahmadinia
| Europan
| Immigrants,
| 57 studies |
| NR | Moderate |
| Heys
| UK | Disadvantaged
| 593 women
|
|
| Moderate |
| Frank
| Australia | Asylum
| 116 women
|
| “
| Good |
- —National Institute for Health and Care Research Health (NIHR), Health and Social Care Delivery Research (HSDR) Programme
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMaternal and Perinatal Health Interventions · Interpreting and Communication in Healthcare · Maternal and fetal healthcare
Introduction
Antenatal care plays a key role in the health of pregnant women and their unborn babies ^ 1 ^. Effective communication between healthcare professionals and pregnant women during antenatal care is critical for shaping personalised care, addressing specific needs and achieving positive outcomes ^ 2 ^. Given the disproportionate adverse pregnancy outcomes in women from underserved and disadvantaged groups, a deep understanding of communication barriers and facilitators is essential for designing inclusive and patient-centred antenatal care services ^ 3 ^.
Various studies have shown how underserved and disadvantaged women may experience a range of communication issues during antenatal care, which can result in misunderstandings, mistrust, and dissatisfaction with care, each of which could negatively impact engagement with maternity services ^ 4, 5 ^. Healthcare professionals should be aware of the unique needs of underserved and disadvantaged women and take steps to improve their communication and interaction with them, such as providing culturally competent care, using interpreters, and involving family members in decision-making processes. To develop training in these areas, the full range of antenatal care experiences reported by underserved and disadvantaged women in high-income countries should be considered.
This overview of systematic reviews considers the experiences of communication during antenatal care among women from ethnic minority and underserved, marginalised, and disadvantaged groups. Thus, it provides the opportunity to build more culturally sensitive and inclusive antenatal care services. This overview will also inform an ongoing study, which aims to develop a birth plan decision aid for UK antenatal care.
Methods
This overview of systematic reviews was conducted in line with current methodological standards and the PRISMA 2020 statement ^ 6, 7 ^. The research methods were predefined and registered in PROSPERO (registration number CRD42022372831, PROSPERO). This overview forms part of a larger mixed methods programme of research aimed at developing a decision aid for discussing planned modes of birth during routine antenatal care in the UK NHS and comparable healthcare settings (the Plan-A study; Research Registry ID: researchregistry8238). While a previous publication from this programme ( https://doi.org/10.1016/j.xagr.2025.100556.) employed similar methodological approaches and a comparable structure, it addressed a different research focus and reported distinct content and findings.
PPI involvement
Four Public and Patient Involvement (PPI) partners with lived experience of maternity care, including women from underserved backgrounds, contributed to this study to ensure inclusivity and meaningful engagement. They were members of the PPI panel for the wider Plan-A project, which comprised eight patient partners in total. PPI partners were involved throughout the entire research process, beginning as co-applicants at the grant proposal stage. They attended regular study meetings, contributed to key discussions, and played a central role in shaping the research question and defining the scope of the study. Their contributions were informed by their lived experience and experiential knowledge of maternity care.
Although one partner withdrew in the second year of the project, the remaining three PPI partners continued to make substantial contributions. They were closely involved in interpreting the study findings and reviewed and commented on draft versions of this manuscript. Their input helped ensure that the final outputs were clear, relevant, and accessible to a wide audience.
Inclusivity
The Plan-A decision aid will support all who become pregnant. See the project's language statement for more information ( https://www.abdn.ac.uk/acwhr/research/plan-a-193.php#panel201).
Eligibility criteria and search strategies
Table 1 outlines the study eligibility criteria. An Information Specialist developed search strategies using appropriate MeSH and text terms. From January 2011 to December 2022, relevant reviews were searched for in major general and specialised databases (MEDLINE, EMBASE, CINAHL, CENTRAL, MIDIRS, ASSIA, and the Social Sciences Citation Index). Details of the MEDLINE search are available in the data repository (see Data Availability statement); this strategy was adapted for searching other databases.
Study selection and data extraction
Two review authors (MC and CR) independently screened the search results and assessed the full texts of potentially eligible citations. Figure 1 (PRISMA diagram) summarises the selection process and the main reasons for exclusions. Data extraction was carried out by two independent authors (KS and MB) using a customised Excel form. To ensure consistency, a third author (MC) cross-checked 10% of the extracted data.
PRISMA Flow chart.
Quality assessment
The methodological quality of the identified reviews was assessed using the Joanna Briggs Institute (JBI) critical appraisal checklist for systematic reviews ^ 8 ^. One review author (AE) conducted the assessments, and a second review author (KS) cross-checked them. The original 11 JBI checklist questions were adapted for this overview. No reviews were excluded based on the quality assessment results. Additionally, one review author assessed the overlap of primary studies across reviews using the Graphical Representation of Overlap for Overviews (GROOVE) tool ^ 9 ^.
Any disagreements during study selection, data extraction and quality assessment were resolved by discussion between review authors or consultation with the research team.
Data synthesis
We organised the findings of the included reviews into two main descriptive themes based on our research question: i) barriers and ii) facilitators to positive antenatal care and birth experiences. One review author (KS) conducted a thematic analysis, examining the similarities and differences across the reviews to identify specific barriers and facilitators (subthemes). A second review author (MB) independently reviewed the analysis and subtheme structure to enhance reliability. Both review authors then discussed their interpretations, reviewed participants’ quotes, and considered the authors' conclusions of the included reviews.
Results
A total of 3,559 citations were identified. After deduplication and removing irrelevant records, 2,540 citations were screened for eligibility. Of these, 2,494 were excluded for not meeting the inclusion criteria, and 46 were retrieved for full-text assessment. Two additional reviews, Balaam 2013 ^ 11 ^ and Frank 2021 ^ 12 ^, were found by hand-searching the reference lists of the full-text reviews. After assessment, 19 systematic reviews published in 20 papers were deemed suitable for inclusion (see Figure 1).
Description of the included reviews
All included reviews were published between 2013 and 2022. Two reviews by Higginbottom et al., from 2019 and 2020, reported the same data, with the 2020 review selected as the primary source ^ 13, 14 ^. Most reviews (11/19) were conducted in the United Kingdom ^ 11, 14– 22 ^, four in Australia ^ 12, 23– 25 ^ two in Ireland ^ 26, 27 ^ one in Canada ^ 28 ^, and one in several European countries (Denmark, Finland, Germany, Ireland, Italy, Norway, Portugal, Sweden, Switzerland, The Netherlands, UK) ^ 29 ^. Across reviews, the number of primary studies, published between 1990 and 2020, ranged from six to 69. Most reviews used qualitative and thematic synthesis to analyse women’s communication experiences during pregnancy. One review used integrative systematic methods ^ 28 ^ and another used a realist synthesis technique ^ 19 ^. The methodological quality of primary studies was assessed using various tools: Walsh & Downe’s criteria (n=2) ^ 11, 16 ^, SCHEMA (n=1) ^ 30 ^, CASP tool (n=9) ^ 12, 15, 17– 22, 26 ^, JBI tool (n=2) ^ 23, 25 ^, MMAT (n=1) ^ 28 ^ and CEBMa (n=1) ^ 14 ^. Overall, the primary studies were reported to be of good quality, though three reviews did not provide information on the methodological quality of the included studies ^ 24, 27, 29 ^.
The quality of the included reviews, assessed using the JBI appraisal checklist, was generally moderate to high. Two studies were rated as low quality. Most reviews clearly described the research question, used appropriate inclusion criteria, identified relevant evidence, developed effective search strategies and summarised results effectively. In most cases, primary studies were independently appraised by two or more reviewers. However, four reviews exhibited unclear practices or did not follow current standards ^ 21, 23, 25, 27 ^. Some reviews also lacked clear recommendations for practice and policy ^ 15, 18, 22, 27 ^. Details of the quality assessment are available in the data repository as extended data (see Data Availability statement).
We evaluated the extent of overlap among primary studies included in the identified systematic reviews using the GROOVE tool and found only a minimal overall overlap (1.08%). A total of 381 primary studies were included in the assessment, with a visual representation showing the extent of overlap across reviews. Out of the 171 possible review pairs, 152 shared less than 5% of the primary studies, indicating a minor degree of overlap and a diverse focus. However, 11 pairs had moderate overlap (5% to <10%), 5 pairs had higher overlap (10% to <15%), and three pairs showed very high overlap (sharing 15% or more of primary studies), suggesting some reviews had a more significant degree of similarity or duplication in their content (see Figure 2 and Figure 3).
Extent of overlap among systematic reviews.
Extent of overlap among systematic reviews: Overall results.
The 19 systematic reviews included in this overview assessed the experiences of various groups, including immigrant, refugee, asylum-seeking women, and homeless women ^ 11, 12, 17, 19, 24, 26, 28– 30 ^, BAME ^ 21, 22 ^ and Muslim women ^ 20 ^, women with physical disabilities ^ 23, 27 ^, disadvantaged women (including those with obesity) ^ 16, 25 ^, survivors of female genital mutilation ^ 18 ^, and trafficked women ^ 15 ^. While all included reviews examined the challenges and barriers faced by women in accessing antenatal care, eight reviews provided also information on facilitators to improve interactions between women and healthcare professionals ^ 12, 14, 16, 20, 22, 24, 28, 30 ^. A summary of the major themes and sub-themes identified by the identified systematic reviews is presented in Table 2.
Theme 1 – Barriers to positive maternity care and birth experience
Within this overarching primary theme, four subthemes were identified. These highlight the challenges faced by ethnic minority and underserved groups during antenatal care, emphasising the need for person-centred, culturally sensitive, and equitable care. Some barriers, like language barriers, are common across subthemes.
1. Communication challenges Across reviews, women described various communication issues with healthcare professionals. These include language and cultural barriers leading to misunderstandings that threatened the quality and value of the interaction with maternity care staff and affected their experiences of antenatal care. Language barriers, in terms of English competence and fluency, were particularly problematic for ethnic and marginalised groups, with 14 of 19 reviews highlighting this issue ^ 11, 12, 14– 17, 19– 22, 24, 28– 30 ^. The lack of interpreters and the use of complex medical terms led to misunderstandings. Women faced significant challenges in navigating the maternity care system and understanding the available services. Many reported feeling alone, isolated, and hesitant to ask questions or disclose their symptoms. They often expressed uncertainty about how the healthcare system operated, further complicating their ability to access appropriate care. 2. Attitudes of healthcare professionals Women from ethnic minorities and underserved, marginalised and disadvantaged groups often faced discrimination, disrespect and negative attitudes from healthcare professionals linked to personal characteristics such as ethnicity, disability, and immigration status. Fourteen reviews noted that women’s experiences, including lack of emotional support and culturally insensitive care, negatively impacted women’s maternity care experiences, leading to feelings of loneliness, anxiety, and diminished self-esteem ^ 11, 12, 14– 18, 20– 23, 26, 27, 29 ^. Previous negative experiences with the healthcare or social care system hindered women's ability to form meaningful relationships, leading to feelings of isolation and fear ^ 21, 26 ^. Some women reported judgmental and derogatory comments from healthcare professionals about their age, sexual orientation, ethnicity, physical characteristics, social status, and birth preferences ^ 12, 14, 16, 20, 22, 23, 26 ^. These prejudicial remarks lowered their self-esteem and made them doubt their ability to be effective mothers ^ 27 ^. Some reviews highlighted a lack of "respectful" care, with some women's experiences crossing into abusive and negligent care ^ 14, 21 ^. Women reported that healthcare professionals were sometimes insensitive to their cultural, religious, and social needs, failing to understand the differences between their native maternity care system and that in the UK ^ 13, 21 ^. For instance, Muslim women reported finding the presence of men in antenatal classes uncomfortable ^ 20 ^. These cultural mismatches led to clashes with healthcare professionals and influenced women’s decisions to use maternity services. The lack of culturally aware care made many women feel mistreated or fearful of mistreatment ^ 16 ^. 3. Access to and experiences of maternity services Fifteen reviews discussed the challenges that women from ethnic minorities and marginalised groups face in accessing antenatal care, such as immigration status, language and cultural barriers, and difficulties in navigating the healthcare system ^ 11, 12, 14– 17, 19, 21, 23– 27, 29, 30 ^. Migrant and refugee women struggled to access and maintain continuity of maternity care due to factors such as loss of social status and family support, low self-esteem, and insecurity about their identity ^ 11, 12, 19, 24, 30 ^. Economic and practical challenges were also reported, including travel costs, ineligibility for services, childcare needs and environmental barriers ^ 23, 27 ^. Reviews noted that local services often failed to meet the needs of those women who were late in registering for appointments and struggled to keep regular attendance due to language and cultural barriers, economic and social circumstances, limited social connections, and immigration status complications ^ 11, 14, 17, 19– 21, 26, 29 ^. Issues such as rushed appointments, inadequate provision of information, fragmented care, medicalisation and lack of personalised care were reported to be distressing and worrying ^ 11, 14, 21, 26 ^. Medicalisation, excessive scrutiny and dietary counselling were also reported to be upsetting by obese and immigrant women ^ 25 ^. The maternity system was frequently described as functional but not supportive, with healthcare professionals treating women as mere cases rather than individuals. As a result, women felt more 'processed' than genuinely cared for ^ 16 ^. Short staffing and high workloads further impacted care quality.4. Trust and sense of security Twelve reviews examined how safety and trust issues and legal concerns affected women's sense of security in the healthcare system ^ 12, 14– 20, 26, 27, 29, 30 ^. Some women explained they were reluctant to seek care or share personal information due to fears for their safety or that of their families. Distrust in healthcare professionals often stemmed from negative foster care experiences or the fear that Child Protection Services would take their babies away ^ 26 ^. Homeless women in particular, delayed seeking care due to viewing social agencies as punitive. Fear of childbirth, tension over traditional postnatal practices, and concerns about legal status, also influenced women’s attitudes toward maternity care ^ 14 ^. Immigrant women, including homeless, asylum seekers, and refugees, struggled with maintaining self-identity and bodily integrity and felt uncertain about what to expect during pregnancy, birth and after birth.
Themes identified for specific ethnic, underserved, or marginalised groups
In addition to the above-reported themes, we identified subthemes specific to certain ethnic, underserved, or marginalised groups. Two systematic reviews focused specifically on women with disabilities ^ 23, 27 ^, one on women with obesity ^ 25 ^, one on women with female genital mutilation ^ 18 ^, one on trafficked women ^ 15 ^, and one on Muslim women ^ 20 ^. These subthemes are summarised below.
Women with disability
Desire for a normal pregnancy experience Women with physical disabilities expressed the desire to be treated as any other pregnant woman and not be labelled ‘high-risk’ because of their disability. They also stressed the importance of remaining in control of care decisions irrespective of the fact that during pregnancy, they could experience exacerbation of their physical symptoms ^ 27 ^. Accessibility Barriers Women with physical disabilities reported negative maternity experiences because maternity facilities were inaccessible to them or not properly equipped, such as the lack of adjustable tables and accessible weighting scales ^ 23, 27 ^. Many felt these barriers limited their independence and caused anxiety ^ 27 ^. They also expressed frustration over being unable to attend antenatal classes due to how they were organised, such as the need to move on and off the ground ^ 23 ^.
Women with obesity
Lack of accurate information on weight management Many women with obesity explained they did not receive adequate advice on weight management, obesity-related risks, or physical activity requirements during pregnancy. Some said the topic was often ignored by healthcare professionals, leaving them confused and unsure about whether losing weight during pregnancy was healthy or how it could be achieved ^ 25 ^. Stigma and stereotyping Women with obesity often described their interactions with healthcare professionals as embarrassing and humiliating due to obesity-related stigma. They questioned the accuracy of some medical advice and felt uncomfortable as conversations shifted from their pregnancy to their weight. Health professionals’ negative comments about obesity-related pregnancy risks left many women feeling guilty and devastated. During ultrasounds, they were embarrassed when obesity prevented visualisation of the foetus, especially when this issue was never mentioned during previous consultations. Extra tests and referrals caused anxiety and the sense that their pregnancy was not "normal." Some women even avoided antenatal appointments due to the insensitive manners and even bullying attitudes of healthcare professionals.
Women who underwent female genital mutilation
Sense of alienation and being objectified Women who had undergone genital mutilation often reported feeling alienated when seeking maternity care. For migrant women, this feeling of alienation was worsened by healthcare professionals' lack of cultural sensitivity and understanding. Women described being shocked by the intrusive questioning about their genital condition and often felt objectified or subject to disrespectful examinations, with little control during antenatal consultations. Clinical decisions often overrode their preferences, leaving them feeling stripped of autonomy ^ 18 ^.
Trafficked women
Access to care and safety issues A major barrier for trafficked women in accessing healthcare was the fear of being reported, arrested, or deported. Understanding and navigating the healthcare system could also be challenging due to being controlled by traffickers and lacking freedom of movement. As a result, they often sought maternity care late or only in emergencies. Some were forced to undergo illegal pregnancy terminations, facing an increased risk of complications and death. Healthcare professionals were not always familiar with the legal rights of trafficked women and tended to deny care if identification was incomplete ^ 15 ^.
Muslim women
Spirituality and faith Muslim women explained that their pregnancy choices, such as declining certain screenings, were influenced by their Islamic faith, which played a prominent role in their lives. However, they felt that healthcare professionals disregarded or disrespected these religious beliefs ^ 20 ^. Discriminatory behaviour and lack of cultural awareness Some Muslim women reported poor maternity care due to discriminatory and negative attitudes of healthcare professionals, particularly midwives. They felt their clothing, like veils and Hijabs, made them targets for prejudice. Many felt uncomfortable discussing birth plans, as midwives lacked an understanding of Islamic values and practices ^ 20 ^.
Theme 2 - Facilitators to positive maternity care and birth experience
Eight of the included systematic reviews identified factors to enhance effective communication and antenatal care for women from ethnic minority, underserved and marginalised groups ^ 12, 14, 16, 20, 22, 24, 28, 30 ^.
Interaction with healthcare professionals Women generally reported positive antenatal and birth experiences when healthcare professionals met their emotional and psychological needs and adopted caring, responsive, and respectful attitudes ^ 14, 30 ^. Positive experiences included clear and respectful communication, receiving appropriate birth information, and continuity of care ^ 13, 16, 20, 22, 24 ^. Women, particularly from ethnic minority groups, felt reassured when they had access to interpreters, culturally responsive professionals, and information in their native language ^ 24, 28 ^. Some, such as Muslim women, reported feeling more comfortable with healthcare professionals who shared their cultural background ^ 20 ^. Social and emotional support Asylum seekers, refugees, and migrant women found educational, community-based, social, and peer support groups useful to tackle challenges like social isolation, poor mental health, and housing, financial, and legal issues ^ 14, 30 ^. These groups provided a safe space for building trusting relationships and sharing knowledge and experiences ^ 22 ^. The involvement of mentors, health advisors, bilingual/bicultural staff, and female staff was key in building trust, offering social and emotional support, and improving access to antenatal information and care ^ 22, 24 ^. Family members, especially partners, were also seen as a positive influence, encouraging women to seek maternity care ^ 26 ^. Access to maternity services Key factors reported to improve access to and experience of antenatal care included the location of services, availability and cost of transport, appointment scheduling (time, length, and flexibility), and the provision of a social model of care ^ 24 ^.
Discussion
This is the most comprehensive and up-to-date summary of evidence from qualitative systematic reviews on the barriers and facilitators experienced by women from ethnic minorities, underserved, and marginalised groups during antenatal care. We identified 19 qualitative systematic reviews on women's maternity care experiences, with the overall methodological quality rated as moderate to high.
Language barriers, cultural differences, and unfamiliarity with the healthcare system significantly impacted how women accessed and engaged with maternity care. Migrant, refugee, and ethnic minority women, in particular, faced challenges in establishing effective communication and trusting relationships with healthcare professionals, which became a major concern during pregnancy. Currently, interpretation services and multilingual information are often insufficient or unavailable in many UK centres. Policymakers should prioritise strategies to increase interpreter use and provide culturally appropriate social support, which is vital for migrant and ethnic minority women. These women face high levels of stress and vulnerability, struggling to adapt to the country's social norms and services. This overview highlights that many women miss antenatal appointments due to difficulties in navigating the healthcare system. Policymakers should improve information on maternity services and create tailored communication strategies.
The attitudes of healthcare professionals towards women from ethnic minorities, underserved, and marginalised groups were considered a major barrier to accessing antenatal care. Women felt they were treated with less dignity, respect, and attention compared to others, due to their cultural or religious background, deprived social status, ethnicity, or physical appearance. Some women, such as those with FGM or obesity, described feeling shocked and humiliated by rude, insensitive, and intrusive comments from healthcare professionals about their physical characteristics.
There is a clear need to improve the understanding and attitudes of maternity staff and policymakers toward women from ethnic minorities, as well as underserved, marginalised, and disadvantaged groups, including migrants and refugees. Future research should explore organisational models that consider these diverse needs and build partnerships with immigrant communities ^ 31 ^. Adopting an inclusive, individualised care approach, including cross-cultural training for healthcare professionals, could improve engagement with vulnerable women and better address their complex needs. Training of health professionals is essential, as these women often face severe mental health issues due to personal stressful circumstances and uncertainty about their future ^ 32 ^.
Effective communication, meaningful interaction with health professionals, and consistent continuity of care were key factors linked to a positive antenatal care experience. For women with past traumatic experiences or negative interactions with healthcare professionals, consistent, supportive care can help build a trusting and safe relationship during pregnancy, especially when prior experiences have diminished their confidence in the healthcare system. In 2021, NHS England introduced guidance for Local Maternity Systems and Integrated Care Systems to implement continuity of care as a standard model for all pregnant women ^ 33 ^. The midwifery continuity of carer (MCoC) model prioritises those at higher risk of poor outcomes. With the increasing number of women from ethnic minorities and underserved groups, there is a clear scope to tailor the MCoC model to these populations, supporting and enhancing their antenatal care experience and promoting a more inclusive, equitable approach to maternity care.
PPI partners acted as research collaborators and provided valuable insights that ensured the findings of this overview were interpreted from the perspectives of women making mode-of-birth decisions. We believe that integrating individuals with lived experiences into the data synthesis process even though requires time and support significantly enhances the research output. This approach grounds the findings in real-world experiences, enriching the analysis with greater cohesion, depth, and authenticity.
Strengths and limitations
This overview was conducted following current methodological standards by an interdisciplinary team of clinical and methodological experts, as well as independent PPI partners. By concentrating on disadvantaged, marginalised, and ethnic minority women in high-income countries, this overview addresses critical gaps in understanding the unique challenges faced by these populations, thereby highlighting opportunities for equitable care improvements. The clear identification of barriers and facilitators provides actionable insights for policymakers and healthcare professionals to design more inclusive maternity services. It is important to acknowledge that most included reviews were conducted in the UK, potentially limiting the generalisability of findings to other high-income countries with differing healthcare systems and cultural contexts. Moreover, demographic details of participants were often underreported, limiting the ability to fully characterise the study populations. The findings of this overview will inform the development of a decision aid designed to facilitate antenatal discussions within the UK NHS. This tool aims to support informed decision-making for expectant mothers, including those from ethnic minorities and marginalised and underserved groups.
Conclusions
This overview of systematic reviews highlights the challenges faced by ethnic minorities and underserved, marginalised, and disadvantaged women during antenatal care. To address health inequalities, maternity care must be re-evaluated at multiple levels. Our findings highlight the critical role of empathetic, accessible, and equitable communication for these women and stress the need for high-quality, personalised care encompassing attentive listening, psychological support, clear and unbiased information, and respect for individual choices. Building compassionate relationships, honouring cultural values, and acknowledging the diversity of women’s experiences should be central to positive maternity care. These insights can guide healthcare professionals and policymakers in enhancing the quality and inclusivity of maternity care and promoting woman-centred approaches.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Novick G : Women's experience of prenatal care: an integrative review. J Midwifery Womens Health. 2009;54(3):226–37. 10.1016/j.jmwh.2009.02.003 19410215 PMC 2754192 · doi ↗ · pubmed ↗
- 2World Health Organization: WHO recommendations on antenatal care for a positive pregnancy experience.Geneva: World Health Organization,2016. 28079998 · pubmed ↗
- 3Higginbottom GM Safipour J Yohani S : An ethnographic investigation of the maternity healthcare experience of immigrants in rural and urban Alberta, Canada. BMC Pregnancy Childbirth. 2016;16: 20. 10.1186/s 12884-015-0773-z 26818961 PMC 4729163 · doi ↗ · pubmed ↗
- 4Gurman TA Becker D : Factors affecting Latina immigrants' perceptions of maternal health care: findings from a qualitative study. Health Care Women Int. 2008;29(5):507–26. 10.1080/07399330801949608 18437597 · doi ↗ · pubmed ↗
- 5Barnett KS Banks AR Morton T : "I just want us to be heard": a qualitative study of perinatal experiences among women of color. Womens Health (Lond). 2022;18: 17455057221123439. 10.1177/17455057221123439 36168990 PMC 9523856 · doi ↗ · pubmed ↗
- 6Page MJ Mc Kenzie JE Bossuyt PM : The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Int J Surg. 2021;88: 105906. 10.1016/j.ijsu.2021.105906 33789826 · doi ↗ · pubmed ↗
- 7Page MJ Moher D Bossuyt PM : PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ. 2021;372: n 160. 10.1136/bmj.n 160 33781993 PMC 8005925 · doi ↗ · pubmed ↗
- 8Aromataris E Fernandez R Godfrey C : Umbrella reviews.In: JBI Manual for Evidence Synthesis. Adelaide: Joanna Briggs Institute,2020; (Accessed 30 May 2024). Reference Source