Clinical and Mycological Profiles of Chronic and Recalcitrant Dermatophytosis: Türkiye, 2022–2024
Murat Durdu, Hazal Kandemir, Ayşe Sultan Karakoyun, Pavlína Lysková, Daniela Kolarczyková, Oğuzhan Bingöl, Yasemin Erdem, Funda Aktürk-Gözel, Özlem Su-Küçük, Melisa Özay, Aslan Yürekli, İlayda Muslu, İsa An, Sinan Özçelik, Tuğba Falay-Gür, Tuğba Tehçi, Abdullah Demirbaş

TL;DR
This study analyzed 91 patients in Türkiye with chronic fungal infections and found high resistance to antifungal drugs in certain fungi, suggesting new treatment approaches.
Contribution
The study identifies specific genetic mutations in fungi and evaluates novel adjunct therapies for drug-resistant dermatophytosis.
Findings
Most isolates were Trichophyton mentagrophytes ITS genotype VIII with high resistance to terbinafine and fluconazole.
Phe397Leu and Tyr414His substitutions were common in TmVIII isolates, with five novel substitutions observed.
Adjunct therapies with resveratrol and curcumin showed promise in treating resistant infections despite in vitro limitations.
Abstract
This study investigated the treatment outcomes of 91 patients with chronic and recalcitrant dermatophytosis from 20 hospitals in Türkiye between June 2022 and March 2024, as well as the in vitro antifungal susceptibility and squalene epoxidase (SQLE) substitution profiles of the dermatophytes obtained from these patients. Molecular identification by sequencing 91 isolates, revealed 76 Trichophyton mentagrophytes ITS genotype VIII (TmVIII; also known as T. indotineae) isolates, 13 Trichophyton rubrum, one Trichophyton tonsurans, and one Microsporum canis. The Phe397Leu substitution predominated in the SQLE, and Tyr414His co-occurred in nine TmVIII isolates. Five novel substitutions were observed in TmVIII. Among 13 T. rubrum isolates, three showed different SQLE substitution patterns compared to the wild-type strain. EUCAST antifungal susceptibility testing revealed high minimum…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1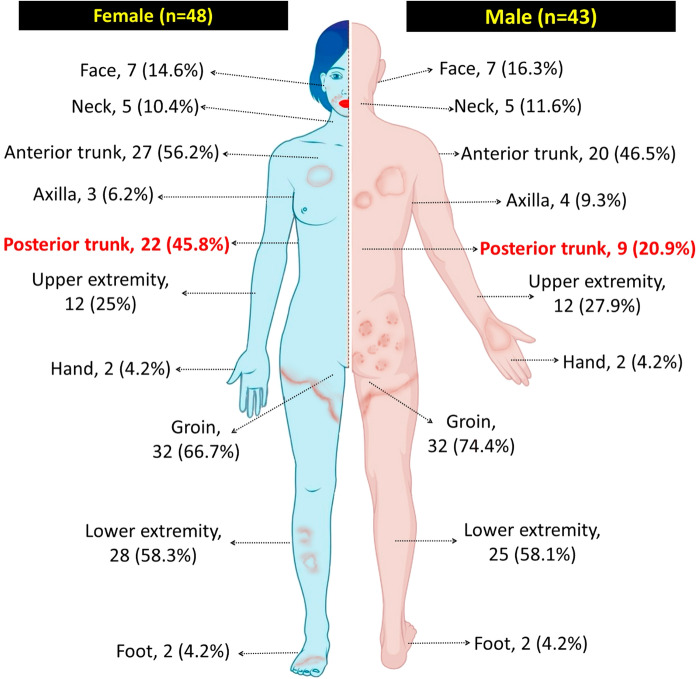 Figure 2
Figure 2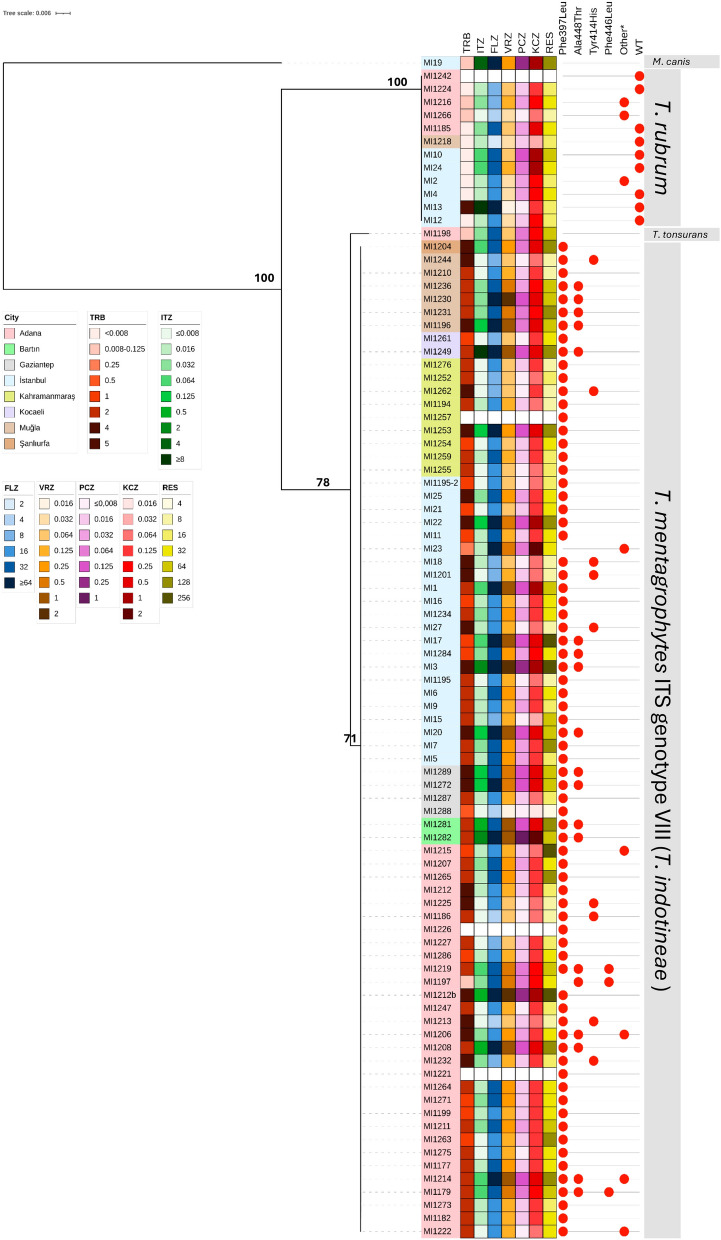 Figure 3
Figure 3 Figure 4
Figure 4- —Czech Academy of Sciences
- —Cukurova University
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNail Diseases and Treatments · Acne and Rosacea Treatments and Effects · Dermatology and Skin Diseases
Introduction
Trichophyton species are the most common causative agents of dermatophytoses worldwide. The genus comprises strictly anthropophilic species, such as T. rubrum, T. tonsurans, and T. violaceum, as well as zoophilic species including T. benhamiae, T. equinum, and T. mentagrophytes [1]. The classification of Trichophyton species has been challenging due to the difficulty in differentiating closely related species. The use of multiphasic approaches, i.e., integrating host specificity, virulence, growth characteristics, sporulation, microscopic features, metabolite production, and mating behavior with molecular data, has significantly improved dermatophyte species definition and identification. However, due to the complexity of distinguishing closely related species, dermatophytes are often grouped into “species complexes”, referred to as “varieties” or named after their internal transcribed spacer (ITS) genotypes [1–4]. Based on recent developments in the taxonomy of Trichophyton [5–7], T. indotineae is also accepted as the ITS genotype VIII or variety indotineae within the T. mentagrophytes complex; however, the name T. indotineae is commonly used in clinical applications for practical reasons.
TmVIII has been reported in at least 49 countries across six continents [7, 8] and is drawing considerable attention due to its frequent resistance to terbinafine (TRB), commonly used first-line treatment for dermatophytoses worldwide [9]. A large proportion of TmVIII isolates reported from various countries are TRB-resistant, with one or multiple specific substitutions in their squalene epoxidase (SQLE) gene linked to resistance [8].
Although still less common than TmVIII, TRB resistance can also be detected in other dermatophytes driven by similar SQLE gene mutations [5, 6, 10, 11]. In such cases, azole-class antifungals are preferred for treatment. However, azole antifungals can pose challenges due to their potential for drug-drug interactions, particularly in patients on complex medication regimens [12]. In such cases, other safe and effective treatment options are urgently needed. Resveratrol (RES), a polyphenolic antioxidant found in red wine, grapes, and peanuts, has been shown to inhibit the growth of dermatophytes in vitro [13]. Other natural compounds, namely curcumin (CUR), derived from the rhizome of Curcuma longa plants, and turmeric oil, a product of CUR, have also demonstrated antifungal activity against dermatophytes in both in vitro and in vivo studies [14, 15]. Nevertheless, the susceptibility profile of TRB-resistant dermatophytes to these compounds has not been investigated, and clinical data supporting their therapeutic efficacy remain limited [14–17].
Recently, Durdu et al. [17] reported the first cases of TRB-resistant TmVIII from a hospital in Türkiye and successfully treated one of these patients with RES tablets without the need for further antifungal treatment. These cases formed the basis of the present study, which explores the resistance profile of isolates obtained from patients with chronic and recalcitrant dermatophytosis in various locations in Türkiye, along with patient characteristics and treatment responses to available antifungal compounds, including RES and CUR.
Materials and Methods
Patients
A total of 91 patients with chronic and recalcitrant dermatophytosis between June 2022 and March 2024 were enrolled from 20 hospitals across 10 cities in Türkiye (Fig. 1). Patients presented with erythematous, scaly patches and/or plaques on their bodies, diagnosed with dermatophyte infection on microscopic examination and/or cultivation, and whose symptoms persisted despite treatment with topical and systemic antifungals for at least 4 weeks were included in the study. Data were collected on patients’ age, sex, medical history, duration, and anatomical location of infection, and the presence of similar symptoms in household members. Informed consent was obtained from all participants or legal guardians for those under 18 years of age. Each hospital provided an approval letter to participate in the study, and the final ethical statement was issued by the Bezmialem Vakıf University Rectorate Technology Transfer Office Ethics Committees Unit, Istanbul, Türkiye, with the approval number: 2024/107.Fig. 1. Geographical location and the number of skin samples collected from 20 hospitals across 10 cities in Türkiye that participated in this study. Detailed information for the participant hospitals and the sample size from each hospital has been provided in the Table S1
Isolates
Skin scraping samples were collected and inoculated onto Sabouraud glucose agar (SGA; Merck, Darmstadt, Germany) supplemented with 100 µg/mL chloramphenicol (Sigma-Aldrich, Steinheim, Germany) and 50 µg/mL gentamicin (Sigma-Aldrich). The plates were incubated at 28 °C for up to 14 days at each hospital, and the isolates were sent to Charles University and the Westerdijk Fungal Biodiversity Institute for further molecular and antifungal susceptibility testing.
DNA was extracted from fresh colonies using the Wizard® Genomic DNA Purification Kit (Promega Corp., Madison, WI, USA). Molecular identification was performed by sequencing the nuclear ribosomal internal transcribed spacer region (ITS), the D1–D2 region of the large subunit (LSU), partial β-tubulin (tubb), and translation elongation factor 1-α (tef-1α) loci using the primers V9G/LS266 [18], LR0R-LR5 [19], T1/tub4rd [20, 21], and EF1/EF2 [22, 23] respectively. The partial SQLE gene was amplified and sequenced using primers described by Kong et al. [24] to detect amino acid substitutions. The PCR amplicons were visualized on a 1.5% agarose gel, and sequencing was performed using Applied Biosystems BigDye Terminator version 3.1 (Thermo Fisher Scientific). The sequences were assembled and edited using Geneious R11 [25] and aligned with MAFFT v.7 [26]. After the best-fit model for each gene was determined using ModelFinder [27] based on the Bayesian Information Criterion (BIC), phylogenetic analyses were conducted using the maximum likelihood method with ultrafast bootstrap option (1000 iterations) implemented on the IQ-TREE web server (http://www.iqtree.cibiv.univie.ac.t/) [28–30]. Trees were visualized using FigTree v1.4.4 [31] and the online Interactive Tree of Life (iToL) server v6 [32]. Reference SQLE sequences MW187977.1 (wild-type of TmVIII) and OM313296.1 (wild-type of T. rubrum) were used for detecting substitutions. The GenBank accession numbers of all sequences used in this study are listed in the Table S2.
Antifungal Susceptibility Testing
The broth microdilution method was performed following the EUCAST guidelines (E.Def 11.0) [33]. The antifungals (Sigma-Aldrich, Prague, Czech Republic) were dissolved in dimethyl sulfoxide (DMSO, Sigma Aldrich), and their test concentration ranges (mg/L) were as follows: fluconazole (FLZ; 0.06–64), terbinafine (TRB; 0.004–4), itraconazole (ITZ; 0.008–8), posaconazole (PCZ; 0.008–8), voriconazole (VRZ; 0.008–8), ketoconazole (KCZ; 0.008-8), and resveratrol (RES; 0.5–512). The isolates were subcultured at 25 °C on SGA (Trios, Prague, Czech Republic). Inoculum suspensions were prepared from 1- to 3-week-old colonies to achieve sufficient sporulation. The suspensions were prepared in sterile distilled water supplemented with 0.1% Tween 20 and filtered through sterile nylon filters (11 μm pore size; Merck, Prague, Czech Republic). To adjust the density of the suspension to 0.5 McFarland (concentration of 2–5 × 10^6^ conidia/mL), distilled water was added as needed, and density was verified using a DENSI-LA-METRB II densitometer (Erba Lachema, Brno, Czech Republic). The suspension was then diluted 1:10 with sterile distilled water to obtain a final working inoculum of 2–5 × 10^5^ conidia/mL. The inoculum suspension was supplemented with chloramphenicol (final concentration 50 mg/L; Sigma-Aldrich, St. Louis, USA) and cycloheximide (final concentration 300 mg/L; Sigma-Aldrich). The microplates were incubated at 25 °C in ambient air for 5–7 days. The MIC endpoints were read spectrophotometrically as 50% growth inhibition. The endpoints for RES were visually interpreted as complete inhibition of fungal growth. Candida krusei (ATCC 6258), C. parapsilosis (ATCC 22019), Aspergillus flavus (ATCC 204304), and A. flavus (CNM-1813) were used as quality control strains. In this study, CUR (C1386, Sigma-Aldrich) dissolved poorly in both water and dimethyl sulfoxide and was excluded from in vitro antifungal susceptibility testing.
Statistical Analysis
The Chi-square test was used in large samples (expected value ≥ 5 in each cell) to compare the frequency of dermatophyte infections between females and males across different anatomical regions, and Fisher’s exact test was used when any expected cell count was < 5. The significance threshold was set at p < 0.05. All statistical analyses were performed using the IBM SPSS Statistics v 21.0 (IBM Corp., Armonk, NY, USA).
Results
Patients
Ninety-one patients with microscopically confirmed dermatophytosis and a history of prior treatment failure, identified across 20 hospitals in 10 cities in Türkiye, were included in this study (Fig. 1). The majority of cases were reported from Adana (n = 36) and Istanbul (n = 30). Of the 91 patients, 43 (47.3%) were male and 48 (52.7%) were female, with ages ranging from 4 to 69 years (median age = 35 years). The duration of infection ranged from 4 to 36 months, with a median of 11 months. One participant was pregnant, and 18 had preexisting conditions such as diabetes (n = 6), hypertension (n = 4), asthma (n = 4), HIV (n = 1), kidney transplantation (n = 1), STAT3 mutation (n = 1), or sickle cell anemia (n = 1). None of the patients had a history of travel to India or the surrounding areas. One patient was identified as a sex worker. One patient with asthma also had epilepsy. Thirty-two patients (35.2%) indicated that at least one family member was also affected, and this concerned mostly the partner (n = 15). Lesions were found in multiple anatomical locations in 75 patients (82.4%). The most frequently affected areas were the groin and gluteal regions (n = 64; 70.3%), followed by the lower extremities (n = 53; 58.2%), anterior trunk (n = 47; 51.6%), upper extremities (n = 35; 38.5%), posterior trunk (n = 31; 34.1%), and face (n = 16; 17.6%). Posterior trunk involvement was significantly more common in females (n = 22; 45.8%) than in males (n = 9; 20.9%) (p = 0.027) (Fig. 2). Only two patients reported no itching; in the remaining cases, pruritus was the most frequently reported symptom (n = 89). Dermatophytide (id) reactions, one with a maculopapular eruption and the other with dyshidrotic eczema, were observed in two patients with no underlying disease.Fig. 2. Distribution of the lesions among male and female patients
Isolates
Among the 91 isolates from treatment-refractory dermatophytosis, 76 were identified as TmVIII, 13 as T. rubrum, one as T. tonsurans, and one as Microsporum canis based on ITS, tubb, and tef-1α sequencing results (Fig. 3, Fig. S1). In total, 74/76 TmVIII isolates (97%) exhibited the Phe397Leu amino acid substitution in the partial SQLE gene, and in nine of these 74 isolates, Tyr414His co-occurred. In addition to Phe397Leu and Tyr414His, we observed the previously described substitutions Ala448Thr and Leu393Ser [24, 34, 35], along with several novel substitutions, that co-occurred with Phe397Leu (Phe446Leu, Phe446Gly, Phe446Cys, Phe446Val, and Val436Gly) (Table 1).Fig. 3. Phylogenetic tree based on ITS sequences, combined with the location, SQLE substitutions, and antifungal susceptibility test results of 90 isolates. The phylogenetic tree was constructed using the IQ-Tree web server, based on the best model TN + F + G4 (BIC). The alignment consists of 965 bp, 66 parsimony-informative, and 798 constant sites. Values of maximum likelihood are shown on the branches. Antifungal susceptibility test could not be performed with the isolates MI1221, MI1226, MI1242, and MI1257 due to contamination. See Table 1Table 1. Clinical features of the patients, including treatment history and SQLE substitutions in dermatophyte isolatesPatient noGenderAge (year)Location of the lesionsDuration of the infection (month)Similar complaints in the familyCo-existing conditionsPrevious treatment^a^Successful treatment^a^Species/StrainSQLE* substitutions^b^1F42Trunk-front and back, face, groin and gluteal regions, foot24–STAT mutationTRB 250 mg/d for 2 m, ITZ 200 mg/d for 3 mFLZ 200 mg/d for 2 m with RESTmVIII/MI1177Phe397Leu2F41Upper and lower extremities, trunk-back12Partner–TRB 3 m, ITZ 100 mg/d for 3 mFLZ 200 mg/d for 2 m with RESTmVIII/MI1179Phe397Leu Phe446Leu Ala448Thr3M31Trunk-front and back, upper and lower extremities, groin and gluteal regions12––TRB 250 mg/d for 2 m, ITZ 200 mg/d for 2 mFLZ 200 mg/d for 2 m with RESTmVIII/MI1182Phe397Leu4M39Groin and gluteal regions24––TRB 250 mg/d for 2 m, ITZ 100 mg/d for 2 m, FLZ 150 mg/w 3 mFLZ 200 mg/d for 2 m with RESTmVIII/MI1186Phe397Leu Tyr414His5M64Lower extremities, trunk-front, groin and gluteal regions6–Diabetes mellitusTRB 250 mg/d for 6 mITZ 200 mg/d for 1 m with CUR food supplementTmVIII/MI1194Phe397Leu6M31Trunk-back, armpit, face, groin and gluteal regions11––TRB 250 mg/d for 4 mITZ 200 mg/d for 2 m^c^TmVIII/MI1195Phe397Leu7F39Upper and lower extremities, trunk-front, face18Partner–TRB 250 mg/d, ITZ 200 mg/d for 3 mFLZ 200 mg/d for 3 m^c^TmVIII/MI1196Phe397Leu Ala448Thr8F62Trunk-front and back, upper extremities, groin and gluteal regions5––ITZ 100 mg/d for 2 m, FLZ 150 mg/w for 1 mTRB 250 mg/d for 2 mTmVIII/MI1197Phe446Leu Ala448Thr9F30Lower extremities24––TRB 250 mg/d and ITZ 200 mg/d for 3 mFLZ 200 mg/d 2 m with RESTmVIII/MI1199Phe397Leu10M49Face, groin and gluteal regions, trunk-back, neck, upper and lower extremities6–Allergic asthma, epilepsyTRB 250 mg/d for 1 m, FLZ 200 mg/d for 1 m, ITZ 100 mg/d for 7 m, ITZ 200 mg/d for 2 mITZ 200 mg/d for 2 m^d^TmVIII/MI1201Phe397Leu Tyr414His11M20Groin and gluteal regions7Partner–TRB 250 mg/d for 2 m, ITZ 100 mg/d for 1 mITZ 400 mg/d 2 mTmVIII/MI1204Phe397Leu12M47Lower extremities, trunk-front, groin and gluteal regions36Partner–TRB 250 mg/d for 3 m, ITZ 200 mg/d for 4 m, FLZ 200 mg/d for 3 mNoneTmVIII/MI1206Phe397Leu Phe446Gly Ala448Thr13F26Trunk-back, lower extremities, groin and gluteal regions12Partner–TRB 250 mg/d, ITZ 200 mg/d for 3 mFLZ 200 mg/d for 2 m with RESTmVIII/MI1207Phe397Leu14M35Upper and lower extremities^e^12Partner–TRB 250 mg/d for 1 mITZ 100 mg/d for 1 mTmVIII/MI1208Phe397Leu Ala448Thr15M28Trunk-front, groin and gluteal regions13––TRB 250 mg/d, ITZ 200 mg/d for 3 mFLZ 200 mg/d for 3 m with RESTmVIII/MI1210Phe397Leu16M45Groin and gluteal regions18Partner–TRB 250 mg/d for 2 m, ITZ 200 mg/d for 3 m, FLZ 200 mg/d for 3 mNoneTmVIII/MI1211Phe397Leu17M31Groin and gluteal regions, upper and lower extremities36Partner–TRB 250 mg/d for 8 m, ITZ 200 mg/d for 3 mNoneTmVIII/MI1212APhe397Leu18F29Groin and gluteal regions, upper and lower extremities36Partner–TRB 250 mg/d for 5 m, ITZ 200 mg/d for 3 mNoneTmVIII/MI1212BPhe397Leu19M23Upper and lower extremities, trunk-front, groin and gluteal regions, face, neck9PartnerITZ 100 mg/d for 2 mFLZ 200 mg/d for 1.5 m with RESTmVIII/MI1213Phe397Leu Tyr414His20F46Face, groin and gluteal regions, armpit, trunk-back36Partner–TRB 250 mg/d for 4 m, ITZ 200 mg/d for 4 m, FLZ 200 mg/d for 3 mNoneTmVIII/MI1214Phe397Leu Phe446Cys Ala448Thr21F4Groin and gluteal regions, upper extremities6––TRB 125 mg/2 mITZ 50 mg/d for 2 mTmVIII/MI1215Phe397Leu Phe446Val22F18Groin and gluteal regions, upper and lower extremities, trunk-front and back9Sibling–TRB 250 mg/d for 3 mFLZ 200 mg/d for 2 mTmVIII/MI1219Phe397Leu Phe446Leu Ala448Thr23M22Groin and gluteal regions7––TRB 250 mg/d for 4 m, ITZ 200 mg/d for 7 mFLZ 200 mg/d for 2 m with RESTmVIII/MI1195-2Phe397Leu24M23Groin and gluteal regions, lower extremities8––TRB 250 mg/d for 1 m, ITZ 200 mg/d for 1 m, FLZ 200 mg/d for 2 mNoneTmVIII/MI1221Phe397Leu25F25Groin and gluteal regions, upper and lower extremities10ParentsSickle cell anemiaTRB 250 mg/d for 3 mITZ 100 mg/d for 1 mTmVIII/MI1222Phe397Leu Val436Gly26M21Groin and gluteal regions, trunk-front8–HIVTRB 250 mg/d for 2 m, ITZ 200 mg/d 1 mFLZ 200 mg/d for 2 m with RESTmVIII/MI1225Phe397Leu Tyr414His27F26Groin and gluteal regions8Colleague–TRB 250 mg/d for 2 mFLZ 200 mg/d for 2 m with RESTmVIII/MI1226Phe397Leu28F37Groin and gluteal regions6––TRB 250 mg/d for 1 mFLZ 200 mg/d for 2 m with RESTmVIII/MI1227Phe397Leu29M45Groin and gluteal regions, lower extremities, armpit, trunk-front4––ITZ 200 mg/d for 4 mFLZ 200 mg/d for 1 m with RESTmVIII/MI1230Phe397Leu Ala448Thr30F36Face, trunk-front, lower extremities9––TRB 250 mg for 2 m, ITZ 200 mg for 2 m, FLZ 150 mg/w, for 3 mFLZ 200 mg/d for 1 m with RESTmVIII/MI1231Phe397Leu Ala448Thr31M34Groin and gluteal regions12––TRB 250 mg/d for 2 m, FLZ 200 mg/d for 2 mITZ 200 mg/d 2 mTmVIII/MI1232Phe397Leu Tyr414His32M19Groin and gluteal regions, lower extremities, trunk-front9––TRB 250 mg/d for 1 m, ITZ 100 mg/d for 1 mFLZ 200 mg/d for 4 m with RESTmVIII/MI1234Phe397Leu33F36Face, lower extremities, trunk-front9––TRB 250 mg for 2 m, ITZ 200 mg for 1 m, FLZ 150 mg/w for 3 mFLZ 200 mg/d for 1 m with RESTmVIII/MI1236Phe397Leu Ala448Thr34M41Groin and gluteal regions, trunk-front and back12Partner–TRB 250 mg/d for 2 mFLZ 200 mg/d for 4 m with RESTmVIII/MI1244Phe397Leu Tyr414His35F58Groin and gluteal regions, trunk-front and back9––TRB 250 mg/d for 3 m, ITZ 100 mg/d for 3 mITZ 200 mg/d for 4 mTmVIII/MI1247Phe397Leu36F52Trunk-front and back^f^9––TRB 250 mg/d for 2 mFLZ 200 mg/d for 3 m with RESTmVIII/MI1249Phe397Leu Ala448Thr37M4Trunk-back, lower extremities12Parents and sibling–TRB 250 mg/d for 1 yrITZ 100 mg/d for 1 mTmVIII/MI1252Phe397Leu38M5Trunk-front and back, lower extremities12Parents and sibling–TRB 250 mg/d for 1 yrITZ 100 mg/d for 1 mTmVIII/MI1253Phe397Leu39M35Trunk-front and back, lower extremities, groin and gluteal regions12Parents and sibling–TRB 250 mg/d for 1y, FLZ 150 mg/w for 2 mITZ 200 mg/d for 1 mTmVIII/MI1254Phe397Leu40F30Trunk-front and back, upper and lower extremities, groin and gluteal regions5Parents and siblingDiabetes mellitusUnprescribed topical antifungalsTopical treatmentsTmVIII/MI1255Phe397Leu41M29Upper and lower extremities, groin and gluteal regions9––TRB 250 mg/d for 3 mITZ 200 mg/d and CUR food supplement for 1 mTmVIII/MI1257Phe397Leu42F22Lower extremities6–AsthmaTRB 250 mg/d for 1 mITZ 200 mg/d and CUR food supplement for 1 mTmVIII/MI1259Phe397Leu43F48Trunk-front and back, upper and lower extremities, groin and gluteal regions, neck14Parents and sibling–TRB 250 mg/d for 6 mITZ 200 mg/d for 3 mTmVIII/MI1261Phe397Leu44F51Trunk-front and back10–Diabetes mellitus, hypertensionTRB 250 mg/d for 3 mITZ 200 mg/d for 6 m, FLZ 200 mg/day for 1 mTmVIII/MI1262Phe397Leu Tyr414His45F45Trunk-front and back, upper and lower extremities, groin and gluteal regions11––ITZ 200 mg/d for 1 mFLZ 200 mg/d for 2 m with RESTmVIII/MI1263Phe397Leu46M22Upper extremities, groin and gluteal regions, lower extremities, neck8Mother–TRB 250 mg/d for 2 mFLZ 200 mg/d for 2 m with RESTmVIII/MI1264Phe397Leu47F49Upper extremities, trunk-front12Child–TRB 250 mg/d for 1 mFLZ 200 mg/d for 2 m with RESTmVIII/MI1265Phe397Leu48F22Lower extremities, groin and gluteal regions14Partner–TRB 250 mg/d for 1 mITZ 100 mg/d for 2 mTmVIII/MI1271Phe397Leu49F51Trunk-front and back, upper and lower extremities, groin and gluteal regions12Parents and sibling–TRB 250 mg/d for 1 mFLZ 200 mg/d for 2 m with RESTmVIII/MI1272Phe397Leu Ala448Thr50M30Trunk-front, face, groin and gluteal regions, upper extremities^g^6Parents and sibling–FLZ 150 mg/w for 1 m, TRB for 1 m, ITZ 100 mg/day for 1 mITZ 100 mg/d for 2 mTmVIII/MI1273Phe397Leu51M17Groin and gluteal regions7––TRB 250 mg/d for 1 mFLZ 200 mg/d for 2 mTmVIII/MI1275Phe397Leu52M21Groin and gluteal regions, face8––TRB 250 mg/day for 1 m, ITZ 100 mg/d for 2 mFLZ 200 mg/d for 2 m with RESTmVIII/MI1276Phe397Leu53F44Trunk-front and back, lower extremities, groin and gluteal regions, neck7PartnerDiabetes mellitus, hypertensionTRB 250 mg/day for < 1 m, ITZ 100 mg/d for 1 mFLZ 200 mg/d for 2 m with RESTmVIII/MI1281Phe397Leu Ala448Thr54F32Lower extremities, groin and gluteal regions8––TRB 250 mg/d for 1 m, ITZ 100 mg/d for 3 m, FLZ 200 mg/w for 1 mFLZ 200 mg/d for 4 m with RES partial progressTmVIII/MI1282Phe397Leu Ala448Thr55F32Face, groin and gluteal regions, upper and lower extremities, trunk-back, neck6–Allergic asthmaTRB 250 mg/d for 1 m, FLZ 200 mg/d for 1 m, ITZ 100 mg/d for 7 m, ITZ 200 mg/d 2 mITZ 200 mg/d for 3 m, partial progressTmVIII/MI1284Phe397Leu Ala448Thr56F40Groin and gluteal regions10Partner–TRB 250 mg/d for 1 mFLZ 200 mg/d for 2 m with RESTmVIII/MI1286Phe397Leu57F16Trunk-front and back, upper and lower extremities, groin and gluteal regions, face, neck, armpit9Parents and sibling–TRB 250 mg/d for 1 mFLZ 200 mg/d for 2 m with RESTmVIII/MI1287Phe397Leu58F51Trunk-front and back, upper and lower extremities, groin and gluteal regions12Parents and sibling–TRB 250 mg/d for 1 mFLZ 200 mg/d for 2 m with RESTmVIII/MI1288Phe397Leu59F16Trunk-front and back, upper and lower extremities, groin and gluteal regions, face, neck, armpit9Parents and sibling–TRB 250 mg/d for 1 mFLZ 200 mg/d for 2 m with RESTmVIII/MI1289Phe397Leu Ala448Thr60F55Lower extremities12––TRB 250 mg/d for 1 mITZ 200 mg/d for 2 mTmVIII/MI1Phe397Leu61F39Upper extremities, trunk-front, face, neck6–Diabetes mellitus, hypertensionTRB 250 mg/d for 3 mVRZ (2 × 200 mg for the first two days, then 200 mg/day for 2 m)TmVIII/MI3Phe397Leu Ala448Thr62M25Lower extremities9––TRB 250 mg/d for 2 mITZ 200 mg/d for 2 mTmVIII/MI5Phe397Leu63M27Lower extremities, face, neck11––TRB 250 mg/d for 3 mITZ 200 mg/d for 2 mTmVIII/MI6Phe397Leu64F38Lower extremities, trunk-front12–Transplant patientTRB 250 mg/d for 2.5 mITZ 200 mg/d for 2 mTmVIII/MI7Phe397Leu65F53Lower extremities, trunk-back7––TRB 250 mg/d for 1 m, FLZ 150 mg/w for 1 m, ITZ 100 mg/d for 3 mITZ 200 mg/d for 2 mTmVIII/MI9Phe397Leu66M28Trunk-front, groin and gluteal regions, face, neck11––FLZ 150 mg/w for 2 mITZ 200 mg/d for 2 mTmVIII/MI11Phe397Leu67M33Upper and lower extremities, groin and gluteal regions6––ITZ 100 mg/d for 2 mITZ 200 mg/d for 2 mTmVIII/MI15Phe397Leu68F24Trunk-front and back, upper and lower extremities18––TRB 250 mg/d for 2 m, ITZ 100 mg/d for 3 mITZ 200 mg/d for 3 mTmVIII/MI16Phe397Leu69F57Lower extremities, groin and gluteal regions12––TRB 250 mg/d for 3 mITZ 200 mg/d for 2 mTmVIII/MI17Phe397Leu Ala448Thr70M46Lower extremities, groin and gluteal regions7––TRB 250 mg/d for 2 mITZ 200 mg/d for 2 mTmVIII/MI18Phe397Leu Tyr414His71M40Upper extremities, trunk-front and back6––TRB 250 mg/d for 1 m, FLZ 150 mg/w for 1 m, ITZ 100 mg/d for 2 mITZ 200 mg/d for 2 mTmVIII/MI20Phe397Leu Ala448Thr72M54Lower extremities, groin and gluteal regions, trunk-front, armpit6––TRB 250 mg/d for 2 m, FLZ 150 mg/w for 1 mITZ 200 mg/d for 2 mTmVIII/MI21Phe397Leu73F43Upper and lower extremities, trunk-front and back, groin and gluteal regions9––FLZ 150 mg/w for 2 mTRB 250 mg/d for 3 mTmVIII/MI22Phe397Leu74F39Upper and lower extremities, trunk-front, groin and gluteal regions12––FLZ 150 mg/w for 1 mITZ 200 mg/d for 3 mTmVIII/MI23Leu393Ser75F47Trunk-front, groin and gluteal regions18––TRB 250 mg/d for 3 mTRB 250 mg/d for 2 mTmVIII/MI25Phe397Leu77M51Lower extremities, trunk-front7––TRB 250 mg/d for 2 mITZ 200 mg/d for 2 mTmVIII/MI27Phe397Leu Tyr414His78M32Lower extremities, groin and gluteal regions6––TRB 250 mg/d for 2 m, ITZ 100 mg/day for 2 mFLZ 200 mg/d for 2 mT. rubrum/MI1185T. rubrum WT79M63Upper and lower extremities24––TRB 250 mg/d, ITZ 200 mg/d for 3 mITZ 200 mg/d for 2 mT. rubrum/MI1216Leu393Ser80M27Trunk-front, groin and gluteal regions8––TRB 250 mg/d for 4 mITZ 200 mg/d for 2 mT. rubrum/MI1218T. rubrum WT81M19Lower extremities, groin and gluteal regions, armpit7F–TRB 250 mg/d for 2 mFLZ 200 mg/d for 2 mT. rubrum/MI1224T. rubrum WT82F69Trunk-front and back, groin and gluteal regions6CHypertensionTRB 250 mg/d for 2 mITZ 100 mg/d for 2 mT. rubrum/MI1242T. rubrum WT83F59Upper and lower extremities, trunk-front, groin and gluteal regions8–Asthma, Diabetes mellitusTRB 250 mg/d for 2 m, ITZ 200 mg/d for 2 mFLZ 200 mg/d for 2 mT. rubrum/MI1266Pro423Ser84F34Upper and lower extremities, trunk-front9––TRB 250 mg/d for 2 mITZ 200 mg/d for 2 mT. rubrum/MI2Ala445Gly85F49Upper and lower extremities, trunk-front7––NoneTRB 250 mg/d for 2 mT. rubrum/MI4T. rubrum WT86M41Groin and gluteal regions14––NoneTRB 250 mg/d for 2 mT. rubrum/MI10T. rubrum WT87F37Feet12––NoneITZ 200 mg/d for 2 mT. rubrum/MI12T. rubrum WT88F25Lower extremities, trunk-back10––TRB 250 mg/d for 2 mTRB 250 mg/d for 2 mT. rubrum/MI13T. rubrum WT89M26Lower extremities, trunk-front, groin and gluteal regions11––TRB 250 mg/d for 2 mITZ 200 mg/d for 2 mT. rubrum/MI24T. rubrum WT76M32Upper extremities, feet^f^14––NoneITZ 200 mg/d for 2 mT. rubrum/MI26T. rubrum WT90M49Trunk-front and back, groin and gluteal regions16––TRB 250 mg/d for 2 m, ITZ 100 mg/d for 2 mITZ 200 mg/d for 2 mT. tonsuransMI1198No WT data available for comparison91F33Groin and gluteal regions9––TRB 250 mg/d for 2 mTRB 250 mg/d for 2 mMicrosporum canis/MI19No dataThe amino acid substitutions detected for the first time in this study are shown in boldCUR curcumin, F female, FLZ fluconazole, ITZ itraconazole, M male, MI Macit Ilkit culture collection, RES resveratrol, T Trichophyton, TmVIII Trichophyton mentagrophytes ITS genotype VIII (T. indotineae), TRB terbinafine, VRZ voriconazole, WT wild type^a^d day, m month, w week, y year^b^Ala alanine, Cys cystein, Gly glycine, His histidine, Leu leucine, Phe phenylalanine, Pro proline, Ser serine, Thr threonine, Tyr tyrosine, Val valine^c^Full recovery during the treatment, recurrence when the treatment stops^d^Short-term recovery was achieved. Seizures were reported in this patient due to fluconazole and terbinafine^e^Maculopapular type id reaction was observed^f^Itchiness was not reported^g^Dyshidrotic type id reaction was observed
Among the 13 T. rubrum isolates, ten were identical to the wild-type T. rubrum reference strain (DK-Trub-sqle-WT; GenBank accession number OM313296.1), whereas three carried various substitutions in their SQLE gene, namely Ala445Gly, Leu393Ser, and Pro423Ser (Table 1). The only hitherto available T. tonsurans SQLE sequence in GenBank is the one reported by Salehi et al. [36] from a TRB-resistant strain in Iran (GenBank accession number MH523151.1). Our SQLE sequence from isolate MI1198 and the Iranian sequence differed by two bases; however, the short Iranian sequence (only 521 bp) limits the detection of additional substitutions potentially involved in TRB resistance. The partial SQLE sequence for the M. canis isolate could not be obtained.
Phylogenetic trees were constructed using ITS, tubb, and tef-1α sequences from our isolates, together with the ex-type strains of each species and variety. Based on the BIC, the best-fit models were TN + F + G4 for ITS (129 sequences, 608 bp, 152 parsimony-informative sites, and 442 constant sites), K2P for tubb (102 sequences, 392 bp, 80 parsimony-informative sites, and 309 constant sites), and TNe + I + F for tef-1α (109 sequences, 605 bp, 140 parsimony-informative sites, and 459 constant sites) loci.
Antifungal Susceptibility Testing
The in vitro antifungal susceptibility test results are summarized in Table 2. Briefly, the MIC_50_ values for FLZ were ≥ 16 mg/L in 71 isolates, consisting of 61 TmVIII, eight T. rubrum, one T. tonsurans, and one M. canis. Of these, 17 isolates (15 TmVIII) had MIC values ≥ 64 mg/L. Since no clinical breakpoints are available for dermatophytes, ITZ, TRB, and VRZ resistance were defined according to the EUCAST-tentative epidemiological cut-off values (TECOFF) [37]. MIC values for ITZ were ≥ 0.25 for six TmVIII (8.2%) and one T. rubrum isolates, suggesting reduced in vitro activity against the tested dermatophytes. TRB resistance was evaluated using TECOFF values of 0.03 mg/L for T. rubrum and 0.125 mg/L for T. indotineae. Overall, 72 TmVIII isolates (98.6%) and two T. rubrum isolates demonstrated non-WT profiles. Among those, 52 TmVIII isolates presented MICs between 0.25 and 2 mg/L, and 20 isolates had higher MICs (MICs ≥ 4 mg/L). VRZ activity was evaluated using TECOFF values 0.125 mg/L for T. rubrum and 1 mg/L for T. indotineae [37]. All T. rubrum isolates shared the WT-profile, while three TmVIII (4.1%) had MICs of 2 mg/L. Complete inhibition values for resveratrol ranged from 4 to 256 mg/L for TmVIII and from 8 to 64 mg/L for T. rubrum isolates. The MIC_50_ ranges for each antifungal agent, as well as the complete inhibition ranges for RES, are listed in Table 3. In this study, the results of the CUR activity were provided solely based on clinical response because its poor solubility during analysis precluded the reliable determination of MIC.Table 2. Antifungal susceptibility test results combined with the SQLE substitutions of the isolatesIsolateSpecies IDMIC 50 (mg/L)TGI (mg/L)SQLEFLZTRBITZPCZVRZKCZRESSubstitutionMI 1177TmVIII(T. indotineae)3220.0160.0160.250.12532Phe397LeuMI 1179TmVIII3220.0640.0640.50.2564Phe397Leu Phe446Leu Ala448ThrMI 1182TmVIII1620.0160.0160.1250.12532Phe397LeuMI 1186TmVIII42 ≤ 0,008 ≤ 0,0080.0640.0648Phe397Leu Tyr414HisMI 1194TmVIII1620.0160.0160.1250.0648Phe397LeuMI 1195TmVIII162 ≤ 0,008 ≤ 0,0080.1250.0648Phe397LeuMI 1196TmVIII6440.1250.06410.564Phe397Leu Ala448ThrMI 1197TmVIII320.0080.0320.0640.50.2532Phe446Leu Ala448ThrMI 1199TmVIII1610.0160.0160.1250.12532Phe397LeuMI 1201TmVIII8 > 4 ≤ 0,0080.0160.1250.0648Phe397Leu Tyr414HisMI 1204TmVIII32 > 40.0640.0640.250.5128Phe397LeuMI 1206TmVIII16 > 40.0320.0320.250.12532Phe397Leu Phe446Gly Ala448ThrMI 1207TmVIII3220.0320.0320.250.12532Phe397LeuMI 1208TmVIII6420.50.12510.5128Phe397Leu Ala448ThrMI 1210TmVIII162 ≤ 0,0080.0160.1250.1258Phe397LeuMI 1211TmVIII3220.0320.0320.250.12564Phe397LeuMI 1212ATmVIII16 > 40.0160.0160.1250.12516Phe397LeuMI 1212BTmVIII > 64 > 40.50.2521256Phe397LeuMI 1213TmVIII44 ≤ 0,0080.0160.0640.0648Phe397Leu Tyr414HisMI 1214TmVIII6420.0640.12510.5128Phe397Leu Phe446Cys Ala448ThrMI 1215TmVIII1610.0160.0160.1250.064256Phe397Leu Phe446ValMI 1219TmVIII3220.0640.0640.50.2564Phe397Leu Phe446Leu Ala448ThrMI 1195–2TmVIII161 ≤ 0,008 ≤ 0,0080.0640.06416Phe397LeuMI 1221TmVIIINDNDNDNDNDNDNDPhe397LeuMI 1222TmVIII162 ≤ 0,008 ≤ 0,0080.1250.06432Phe397Leu Val436GlyMI 1225TmVIII16 > 4 ≤ 0,008 ≤ 0,0080.0640.0648Phe397Leu Tyr414HisMI 1226TmVIIINDNDNDNDNDNDNDPhe397LeuMI 1227TmVIII82 ≤ 0,0080.0160.0640.12516Phe397LeuMI 1230TmVIII6420.0320.12520.564Phe397Leu Ala448ThrMI 1231TmVIII3220.0320.0640.50.25128Phe397Leu Ala448ThrMI 1232TmVIII8 > 40.0320.0160.1250.12516Phe397Leu Tyr414HisMI 1234TmVIII1620.0320.0320.250.12532Phe397LeuMI 1236TmVIII3220.0320.0320.50.2564Phe397Leu Ala448ThrMI 1244TmVIII84 ≤ 0,008 ≤ 0,0080.0640.0648Phe397Leu Tyr414HisMI 1247TmVIII162 ≤ 0,008 ≤ 0,0080.1250.12516Phe397LeuMI 1249TmVIII > 64280.12510.5128Phe397Leu Ala448ThrMI 1252TmVIII82 ≤ 0,008 ≤ 0,0080.0640.06416Phe397LeuMI 1253TmVIII64 > 40.1250.1250.250.5128Phe397LeuMI 1254TmVIII161 ≤ 0,0080.0160.0640.12532Phe397LeuMI 1255TmVIII162 ≤ 0,008 ≤ 0,0080.0640.06416Phe397LeuMI 1257TmVIIINDNDNDNDNDNDNDPhe397LeuMI 1259TmVIII3220.0160.0160.1250.12516Phe397LeuMI 1261TmVIII81 ≤ 0,008 ≤ 0,0080.0640.12532Phe397LeuMI 1262TmVIII8 > 4 ≤ 0,008 ≤ 0,0080.0640.1258Phe397Leu Tyr414HisMI 1263TmVIII161 ≤ 0,0080.0160.1250.125128Phe397LeuMI 1264TmVIII3220.0160.0160.250.12532Phe397LeuMI 1265TmVIII3220.0160.0160.250.125128Phe397LeuMI 1271TmVIII3210.0320.0160.250.12532Phe397LeuMI 1272TmVIII6440.1250.1250.50.564Phe397Leu Ala448ThrMI 1273TmVIII1620.0160.0160.1250.12516Phe397LeuMI 1275TmVIII162 ≤ 0,008 ≤ 0,0080.1250.12532Phe397LeuMI 1276TmVIII162 ≤ 0,0080.0160.0640.1258Phe397LeuMI 1281TmVIII3220.50.12510.5128Phe397Leu Ala448ThrMI 1282TmVIII642211264Phe397Leu Ala448ThrMI 1284TmVIII3210.0320.0320.250.2532Phe397Leu Ala448ThrMI 1286TmVIII1610.0160.0160.1250.12532Phe397LeuMI 1287TmVIII1620.0160.0160.1250.06416Phe397LeuMI 1288TmVIII40.5 ≤ 0,008 ≤ 0,0080.0160.0164Phe397LeuMI 1289TmVIII3240.1250.1250.50.564Phe397Leu Ala448ThrMI 1TmVIII > 6420.0640.1251164Phe397LeuMI 3TmVIII > 64420.2521256Phe397Leu Ala448ThrMI 5TmVIII3220.0160.0320.250.12516Phe397LeuMI 6TmVIII3220.0160.0160.250.12532Phe397LeuMI 7TmVIII3220.0320.0320.250.125128Phe397LeuMI 9TmVIII1620.0160.0320.1250.12516Phe397LeuMI 11TmVIII3210.0160.0160.1250.12532Phe397LeuMI 15TmVIII82 ≤ 0,008 ≤ 0,0080.1250.03264Phe397LeuMI 16TmVIII1610.0160.0160.1250.12532Phe397LeuMI 17TmVIII6410.0640.12510.5256Phe397Leu Ala448ThrMI 18TmVIII8 > 40.016 ≤ 0,0080.0640.0648Phe397Leu Tyr414HisMI 20TmVIII6440.1250.12510.564Phe397Leu Ala448ThrMI 21TmVIII161 ≤ 0,0080.0160.0640.12532Phe397LeuMI 22TmVIII64 > 40.1250.1250.51128Phe397LeuMI 23TmVIII > 640.250.0160.0640.5232Leu393SerMI 25TmVIII3240.0320.0320.250.12532Phe397LeuMI 27TmVIII164 ≤ 0,008 ≤ 0,0080.1250.0648Phe397Leu Tyr414HisMI 26T. rubrum32 ≤ 0,0040.0160.0320.0640.564T. rubrum WTMI 1185T.* rubrum32 ≤ 0,0040.0320.0320.0640.532T*. rubrum WTMI 1216T.* rubrum80.0640.0320.0320.1250.2532Leu393SerMI 1218T*.* rubrum2 ≤ 0,0040.0160.0160.0320.03216T*. rubrum WTMD1224T.* rubrum8 ≤ 0,0040.0160.0160.0640.12516T*. rubrum WTMD1242T.* rubrumNDNDNDNDNDNDNDT*. rubrum WTMI 1266T.* rubrum40.008 ≤ 0,008 ≤ 0,0080.0320.0648Pro423SerMI 2T*.* rubrum16 ≤ 0,0040.0160.0320.0320.2516Ala445GlyMI 4T*.* rubrum16 ≤ 0,0040.0160.0320.0320.2532T*. rubrum WTMI 10T.* rubrum32 ≤ 0,0040.0640.1250.064164T*. rubrum WTMI 12T.* rubrum16 ≤ 0,0040.0160.0160.0320.2516T*. rubrum WTMI 13T.* rubrum* > 64 > 4 > 8 ≤ 0,0080.0160.12516T. rubrum WTMI 24T.* rubrum32 ≤ 0,0040.0640.0640.125132T*. rubrum WTMI 1198T.* tonsurans320.0080.0320.0640.0640.2564No WT data available for comparisonMI 19M*. canis640.00840.250.251128No dataCUR curcumin, FLZ fluconazole, ITZ itraconazole, KCZ ketoconazole, MI Macit Ilkit culture collection, MIC minimum inhibitory concentration, PCZ posaconazole, RES resveratrol, T Trichophyton, TGI total growth inhibition concentration, TRB terbinafine, TmVIII T. mentagrophytes ITS genotype VIII, VRZ voriconazole, WT wild type. The amino acid substitutions detected for the first time in this study are shown in boldTable 3The minimum inhibitory concentration ranges for FLZ, ITZ, KCZ, PCZ, TRB, and VRZ, and total growth inhibition concentration ranges for RES, against the Trichophyton mentagrophytes ITS genotype VIII (T. indotineae) and T. rubrum isolatesIsolatesAntifungal drugMIC 50 range (mg/L)TGI range (mg/L)GM (mg/L)Trichophyton mentagrophytes ITS genotype VIII (n = 73)FLZ4–6422.52ITZ0.008–80.005KTZ0.016–20.17PCZ0.008–10.04TRB0.008–41.89VRZ0.016–20.21RES4–25634.2Trichophyton rubrum (n = 12)FLZ2–6415.1ITZ0.008–80.02KCZ0.032–10.24PCZ0.008–0.1250.03TRB0.004–40.009VRZ0.016–0.1250.05RES8–6424TGI total growth inhibition concentration, FLZ fluconazole, GM geometric means, ITZ itraconazole, KCZ ketoconazole, MIC minimum inhibitory concentration, PCZ posaconazole, RES resveratrol, TRB terbinafine, VRZ voriconazole
Clinical Response to Antifungal Treatments
Successful treatment was defined as complete lesion clearance and negative KOH microscopy. When there was no improvement of the lesions after 4 weeks, or erythema and/or scales were observed at 8 weeks, and microscopy analysis revealed positive results for fungal elements at these follow-ups, the cases were considered failed. If the erythema and/or scales were observed at the site of healed lesions during the follow-up of healed patients (at 8 weeks), these cases were considered as recurrence.
All patients had previously received topical and/or systemic antifungal therapy as monotherapy or in combination without clinical improvement. These failed regimens included TRB alone (n = 49), TRB + ITZ (n = 18), TRB + ITZ + FLZ (n = 10), ITZ alone (n = 7), TRB + FLZ (n = 6), and FLZ + ITZ (n = 1). During the study, 83/91 patients responded to the different treatment regimens (in terms of their doses, durations, or combinations) with FLZ (200 mg/d), ITZ (100‒200 mg/d), TRB (250 mg/d), or VRZ (200 mg twice daily for 2 days, followed by 200 mg/d for 8 weeks) (Table 1). The most commonly used antifungals were ITZ (n = 41) and FLZ (n = 36). Among patients with previous TRB failure (n = 83), ITZ and FLZ monotherapy provided clinical improvement in 36/83 (43.4%) and 33/83 (39.8%), respectively. Among 41 patients who received ITZ, three were successfully treated with ITZ (200 mg/d) in combination with CUR supplement (40 mg/d for 1 month) and the overall success rate of ITZ was 93%. In three other patients (isolates MI1195, MI1201, and MI1284), ITZ monotherapy (200 mg/d for 2 months) initially cleared lesions, but recurrence occurred shortly after treatment discontinuation. One patient (isolate MI1247) was successfully treated with ITZ (100 mg/d) in combination with topical sertaconazole, remaining 90 patients used luliconazole cream as a topical treatment. Thirty-five patients received FLZ therapy and 33 of them fully recovered; 25 of them were a combination of FLZ (200 mg/d for 1–4 months) and RES (2 × 200 mg/d for 1–4 months), and only one patient did not respond to this treatment. The overall success rate of FLZ was 94%. In 12 patients, lesions were resolved; however, post-inflammatory hyperpigmentation persisted. Recurrence and partial improvement of the lesions were observed in two (2.2%) and three patients (3.3%), respectively. Detailed information on the dosage and duration of both the most recent therapy applied before the study, and successful treatments is provided in Table 1.
An adverse event was observed in one patient receiving phenobarbital for epilepsy who developed seizures during both TRB and FLZ therapy, prompting discontinuation. This patient tolerated ITZ (200 mg/d), although only partial clinical remission was observed. Seven patients did not respond to TRB, ITZ, or FLZ (in combination with RES) treatments, despite the absence of drug-drug interactions.
The combined analysis of clinical outcomes, in vitro TRB susceptibility, and SQLE substitution profiles revealed several discordant findings. The patient from whom the MI1199 isolate (harboring the Phe378Leu SQLE substitution) was obtained had previously received combined TRB (250 mg/d) and ITZ (200 mg/d) therapy for 3 months without improvement. Surprisingly, the same patient achieved complete clinical remission with FLZ (200 mg/d for 2 months) despite in vitro MIC values of 16 mg/L and 1 mg/L for FLZ and TRB, respectively. Similarly, a combination of FLZ (200 mg/d) and RES (2 × 200 mg) was effective in 14/29 patients even though their isolates exhibited high MICs for FLZ (32 to ≥ 64 mg/L).
Discussion
Dermatophytosis has long been considered a neglected fungal infection, as it is not considered life-threatening, and has usually been straightforward to treat. However, the emergence of recalcitrant cases and antifungal resistance has complicated management in recent years. Easy access to over-the-counter topical antifungal-corticosteroid combinations likely contributes to selective pressure and rising resistance among dermatophytes [38]. Environmental factors (e.g., higher ambient temperatures and humidity) and social factors (e.g., crowded living conditions, poor hygiene, or sharing utensils within large households) further facilitate the survival and transmission of dermatophytes, complicating surveillance and control efforts. In the current study, more than one-third of the participants reported similar symptoms among their family members (Table 1). Therefore, where possible, all infected family members were invited for clinical evaluation and were followed throughout their treatment course to prevent reinfection and ongoing transmission. On the other hand, it was impossible to identify the source of the infection when there was no connection with any known sources of dermatophytosis, and if the patients were working or living in circumstances where they were constantly exposed to various possible sources of infection (for instance, as a sex worker or a prisoner).
Following the initial description in India [39], similar cases have been reported in several other countries [8]. The first such cases in Türkiye were reported in 2023 [17]. Although numerous studies have examined dermatophyte prevalence in Türkiye over the years [41–45], no retrospective study has re-examined the presence of TmVIII among previously identified T. mentagrophytes isolates. Consequently, whether resistant TmVIII strains were circulating in the country before 2023 remains unknown. In addition, 83 of 91 patients in the present study had prior TRB exposure (monotherapy or in combination), meaning that the clinical samples were collected after TRB therapy. Accordingly, we could not determine whether TRB resistance was primary or acquired during treatment.
TmVIII is usually reported from cases of tinea corporis, tinea cruris, and tinea faciei cases, but has recently also been reported in onychomycosis [6, 46]. This clinical heterogeneity limits the utility of clinical presentation as a taxonomic criterion. The lesions in cases of tinea corporis, tinea cruris, and tinea faciei caused by TmVIII are typically extensive, pruritic, and inflammatory [3] (Fig. 4). Tang et al. [4] proposed that the high virulence of TmVIII might indicate a zoonotic origin for this lineage. Several animal cases have been reported, supporting the hypothesis that animals may act as reservoirs of TmVIII and that zoonotic transmission cannot be excluded [47, 48]. However, in most studies, human cases without known animal contact were prevalent. Additionally, in our cohort, animal contact was not investigated. Nevertheless, it is non-negligible that this lineage might represent a zoophilic ancestor in the process of adaptation to humans. In this case, a decrease in apparent virulence over time might be anticipated, although this remains speculative for the time being.Fig. 4. Clinical appearance of the lesions before and after antifungal treatment in different patients. a,** b** A 5-year-old male patient (isolate MI1253, TmVIII), a erythematous scaly plaques on the back before treatment. b after ITZ treatment for 2 months. c,** d** A 18-year-old female patient (isolate MI1219, TmVIII) c annular erythematous scaly plaques in the gluteal region and thighs, d response to FLZ (200 mg/d) treatment for 2 months with post-inflammatory hyperpigmentation. e–h A 32-year-old male patient (isolate MI1185, T. rubrum), erythematous scaly plaques before the treatment, e on legs, g on the anterior thigh; f,** h** the response after FLZ (200 mg/d) treatment for 2 months. j–m A 31-year-old male patient (isolate MI1182, TmVIII) annular erythematous scaly plaques on j leg, and l the lower abdominal quadrant; k,** m** response to FLZ (200 mg/d) plus RES treatment for 2 months
Several amino acid substitutions in the SQLE gene have been associated with TRB resistance in TmVIII and other dermatophyte species. Among them, the Phe397Leu substitution was the most frequently observed [8]. In the current study, in addition to Phe397Leu, we also identified Ala448Thr and Leu393Ser, both of which have been previously reported [24, 35]. Conversely, Tyr414His was detected alongside Phe397Leu in nine TRB-resistant isolates (with MICs ranging from 2 to > 4 µg/mL). To date, Tyr414His has been reported only from England [49], Germany [50], and Türkiye [17].
Although TmVIII commonly exhibits high TRB resistance, in vitro TRB-susceptible isolates have also been reported [51–54]. Among those reports, in one case, clinical treatment with combined oral TRB and topical ketoconazole (KCZ) failed even though the isolate was susceptible to TRB (MIC 0.06 µg/mL) [53]. In our study, only one isolate (MI1197) had a low MIC value (0.008 mg/L) despite the presence of Phe446Leu Ala448Thr substitutions, and the patient of this isolate was successfully treated with TRB. Conversely, in two different patients, TRB treatment was effective despite their isolates displayed high TRB MICs (≥ 4 mg/L) and the Phe397Leu substitution.
In the current study, Ala448Thr substitutions occurred only in combination with other SQLE substitutions, except in one case, always found with Phe397Leu. The Ala448Thr substitution has not been shown to confer TRB resistance independently; however, it has been associated with higher MIC values for ITZ and VRZ [35]. In our study, higher MIC values with azoles were not directly linked to Ala448Thr substitution, as other isolates with only Phe397Leu substitutions also showed similar profiles (Table 2). In total, 19 isolates with multiple SQLE substitutions that contain Ala448Thr exhibited high MICs for FLZ (ranging from 16 to > 64 mg/L) and TRB MICs (1 to > 4 mg/L). However, 16/19 (84%) were successfully treated with azole-based regimens (Table 1), and 9/16 responded to FLZ therapy combined with RES. There was no significant difference in the success rates of ITZ and FLZ in the treatment of TRB-resistant dermatophyte infections; however, FLZ was slightly more effective than ITZ (94 vs. 93%, respectively), different from the findings reported by Singh et al. [55]. Collectively, these observations indicate that clinical response does not always align with in vitro MICs and SQLE genotype alone, implicating that additional factors such as host factors, drug exposure at the infection site, treatment adherence, and further resistance mechanisms may also affect the clinical outcome.
Alternative treatment strategies for dermatophytosis are increasingly considered due to limited access to common antifungals in some countries, the risk of resistance development, or contraindications such as drug–drug interactions. Although VRZ is not a routine first-line treatment nor is it considered standard practice for treating superficial dermatophytoses, in cases where TRB, ITZ, and FLZ treatments have failed, VRZ has been found to be effective [56–58]. Nevertheless, given its importance in the management of life-threatening systemic mycoses, use of VRZ in superficial dermatophytosis should be confined to cases unresponsive to all other antifungals or the presence of drug–drug interactions. Similarly, PCZ is another off-label triazole option and it has previously shown promising results in a multidrug-resistant T. indotineae infection [9]. KCZ has also been reported as alone or adjunctive topical treatment in TRB-resistant T. indotineae infections [59]. However, these azoles are currently not recommended as treatment options due to treatment safety and cost concerns [60]. In our study, among these azoles, only VRZ therapy was recommended for seven cases with multidrug resistance; however, these patients were lost to follow-up.
RES has been previously reported as a promising alternative, demonstrating in vitro activity against a broad spectrum of pathogens, including Aspergillus, Candida, and dermatophytes [13, 61]. In our first report of TRB-resistant TmVIII from Türkiye, a patient with a CD36 mutation was successfully treated with RES tablets without further antifungal therapy [17]. Recently, Kurmus et al. [62] reported a case of TRB-resistant TmVIII that was successfully treated with FLZ at 200 mg/d, oral RES at 200 mg/d, and 1% luliconazole cream over a period of 3 weeks. In the current study, the clinical efficacy of RES was not supported by its in vitro activity against the isolates. Such that, 29 patients received the combination of FLZ and RES, despite the isolates’ elevated in vitro MICs for both agents. All but one patient achieved clinical improvement, and 28 attained complete resolution.
In addition, three patients in this study were successfully treated with ITZ supplemented with CUR. CUR has been previously shown to be effective in vitro against dermatophytes and Candida species [63], as well as Cryptococcus neoformans and Paracoccidioides brasiliensis [64], with reports of enhanced effects when combined with antifungal agents [65]. Despite its in vitro activity against selected fungi and limited clinical efficacy, the application of CUR remains challenging due to its poor oral bioavailability and insufficient solubility in aqueous solvents [66, 67]. Standardized solubilization or formulation approaches and dedicated synergy assays are needed to assess the antifungal activity of CUR against dermatophytes more reliably.
Currently, in vitro discrimination of TRB-resistant TmVIII from susceptible isolates can be performed on SGA plates supplemented with TRB [68, 69]. However, definitive characterization should include the European Committee on Antimicrobial Susceptibility Testing (EUCAST) broth microdilution method to determine MICs (E.Def 11.0) [33] and sequencing of the SQLE hotspot region to identify resistance-associated substitutions. While the agar-based screening is simple and useful for surveillance, reporting precise MICs and the underlying SQLE substitutions is recommended to track temporal trends in TRB resistance and to detect the regional emergence of specific genotypes.
In conclusion, the cases reported in this study showed that, although the vast majority of TmVIII isolates carried Phe397Leu substitution, a specific Tyr414His substitution is also evident. Considering that 8/9 isolates harboring both Phe397Leu and Tyr414His substitutions showed MIC values ≥ 4 against TRB, Tyr414His might have an impact on TRB resistance in TmVIII. Further studies would reveal whether and how Tyr414His substitution in the SQLE gene affects the enzyme structure and functions. In our study group, ITZ-based regimens were the most effective, followed by FLZ-based regimens, in the treatment of TRB-resistant dermatophytosis. Despite efforts to identify TmVIII and treat infections caused by this genotype using certain key features (e.g., affected anatomical regions and high TRB resistance), worldwide reported cases have demonstrated that this genotype shares more similarities with other dermatophytes than previously shown. Reporting both failed and successful treatments, along with the patient and isolate profiles, may increase the chances for other clinicians to follow appropriate regimens earlier when encountering similar cases. Additionally, ongoing molecular surveillance that tracks local MIC distributions and SQLE substitution patterns, and compares them across regions, will help us to understand the resistance mechanisms as well as to develop more accurate identification tools and alternative treatments in the future.
Supplementary Information
Below is the link to the electronic supplementary material.Supplementary file1 (PDF 1083 KB)Supplementary file2 (XLSX 49 KB)Supplementary file3 (XLSX 16 KB)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Gupta AK, Susmita, Nguyen HC, et al. Trichophyton indotineae: epidemiology, antifungal resistance and antifungal stewardship strategies. J Eur Acad Dermatol Venereol. 2026;40(1):29–45.
- 2Rambaut A. Figtree. ver 1.4.4. Institute of Evolutionary Biology, University of Edinburgh, Edinburgh. 2018; https://tree.bio.ed.ac.uk.
- 3Rhodes J, Hui ST, Dellière S, et al. Emerging terbinafine-resistant Trichophyton indotineae between 2018 and 2023: A multinational genomic epidemiological study. Lancet Microbe. 2026. 10.1016/j.lanmic.2025.101273.