The role of radiotherapy in MPNST and the impact of NF1 status on outcomes: Insights from a multicenter cohort study
Christianne Y M N Jansma, Dirk J Grünhagen, Uta E Flucke, Willem-Bart M Slooff, Thijs van Dalen, Lukas B Been, Han J Bonenkamp, Monique H M E Anten, Martinus P G Broen, Marc H A Bemelmans, Jos A M Bramer, Gerard R Schaap, Arthur J Kievit, Winan J van Houdt, Jos van der Hage

TL;DR
This study examines how radiotherapy affects outcomes in MPNST patients, finding it reduces local recurrence in non-NF1 cases but not in those with NF1.
Contribution
The study provides insights into the differential impact of radiotherapy on MPNST outcomes based on NF1 status.
Findings
Radiotherapy reduced local recurrence risk in sporadic MPNST cases but not in NF1 patients.
RTx was more frequently used for high-grade and extremity tumors.
In NF1 patients, microscopically positive margins were the only risk factor for local recurrence.
Abstract
Malignant peripheral nerve sheath tumors (MPNSTs) are rare, aggressive sarcomas, with 40% associated with neurofibromatosis type 1 (NF1). Surgical excision is the main treatment for localized disease; however, local recurrence (LR) remains high. Radiotherapy (RTx) is increasingly used to enhance local control in STS, but its use remains controversial due to the potential for increased major wound complications and an increased risk of secondary malignancies in NF1 patients. This study investigated the use and impact of RTx on local control in MPNSTs, particularly in the NF1 setting. Surgically treated primary MPNSTs from 1988 to 2019 in the MONACO multicenter cohort were included. Differences in demographics, treatment, and RTx use between NF1 and non-NF1 cases were examined. Factors influencing RTx administration and LR were assessed via multivariable analyses. Among 499 patients…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
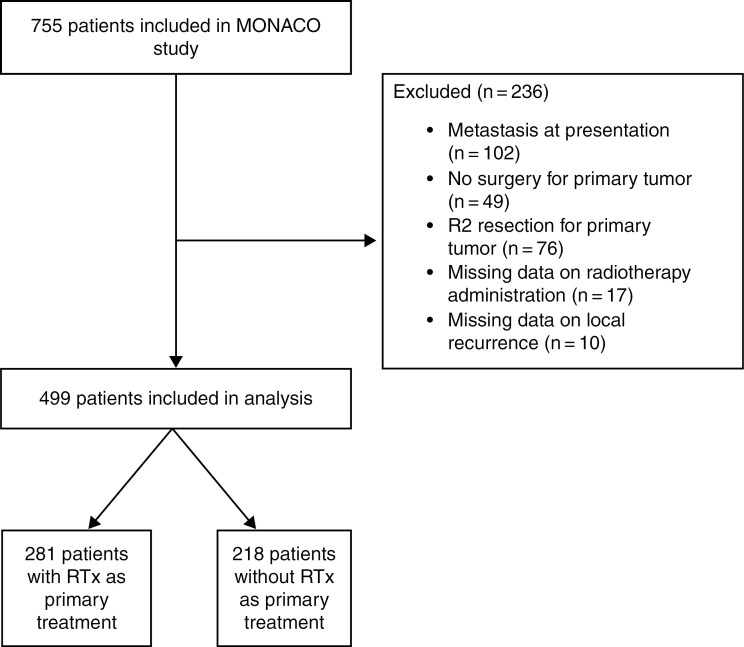 Figure 1
Figure 1| Variable | Overall | No radiotherapy | Any type of radiotherapy |
|
|---|---|---|---|---|
|
| 499 | 218 | 281 | |
| Age (years) | ||||
| Mean (SD) | 42.80 (21.14) | 43.52 (18.05) | .683 | |
| Male gender | 268 | 113 (51.8%) | 155 (55.4%) | .489 |
| NA | 1 | - | 1 | |
| ASA | ||||
| I | 158 | 71 (56.8%) | 87 (56.9%) | .923 |
| II | 106 | 47 (37.6%) | 59 (38.6%) | |
| III | 14 | 7 (5.6%) | 7 (4.6%) | |
| NA | 221 | 93 | 128 | |
| NF1 | ||||
| No | 324 | 144 (67.0%) | 180 (65.7%) | .840 |
| Yes | 165 | 71 (33.0%) | 94 (34.3%) | |
| NA | 10 | 3 | 7 | |
| Tumor size | ||||
| <5 cm | 130 | 66 (39.3%) | 64 (27.9%) | .043 |
| 5–10 cm | 162 | 65 (38.7%) | 97 (42.4%) | |
| >10 cm | 105 | 37 (22.0%) | 68 (28.7%) | |
| NA | 102 | 50 | 52 | |
| Tumor depth | ||||
| Superficial | 73 | 37 (26.8%) | 36 (20.7%) | .257 |
| Deep | 239 | 101 (73.2%) | 138 (79.3%) | |
| NA | 187 | 80 | 107 | |
| Tumor grade | ||||
| High grade | 281 | 114 (79.2%) | 167 (90.8%) | .005 |
| Low grade | 47 | 30 (20.8%) | 17 (9.2%) | |
| NA | 171 | 74 | 97 | |
| RTx-associated | ||||
| No | 448 | 193 (90.2%) | 255 (93.4%) | .258 |
| Yes | 51 | 21 (9.8%) | 18 (6.6%) | |
| NA | 12 | 4 | 8 | |
| Site of primary tumor | ||||
| Head and neck | 68 | 36 (16.5%) | 32 (11.4%) | .001 |
| Extremities | 249 | 87 (39.9%) | 162 (57.7%) | |
| Central | 180 | 94 (43.1%) | 86 (30.6%) | |
| Unknown | 2 | 1 (0.5%) | 1 (0.4%) | |
| Surgical margin | ||||
| R0 | 324 | 148 (67.9%) | 176 (62.6%) | .247 |
| R1 | 140 | 53 (24.3%) | 87 (31.0%) | |
| Unknown | 35 | 17 (7.8%) | 18 (6.4%) |
| Variable | OR (CI 95%) |
|
|---|---|---|
| Intercept | 0.308 (0.136–0.699) | .007 |
| Tumor size | ||
| <5 cm | 1.00 | |
| >5 cm | 1.53 (0.906–2.58) | .113 |
| Tumor depth | ||
| Superficial | 1.00 | |
| Deep | 1.10 (0.607–1.98) | .762 |
| Tumor grade | ||
| Low grade | 1.00 | |
| High grade | 2.41 (1.20–4.84) | .013 |
| Site of primary tumor | ||
| Head and neck | 1.00 | |
| Extremities | 1.82 (1.00–3.30) | .050 |
| Central | 0.862 (0.457–1.63) | .643 |
| Surgical margin | ||
| R0 | 1.00 | |
| R1 | 1.49 (0.977–2.26) | .079 |
| Univariate | Multivariate | |||
|---|---|---|---|---|
| Variable | HR (95%CI) |
| HR (CI 95%) |
|
| Age (per 10 years) | 1.05 (0.948–1.15) | .375 | ||
| NF1 | ||||
| No | 1.00 | 1.00 | ||
| Yes | 1.270 (0.850–1.90) | .246 | 0.908 (0.589–1.40) | .662 |
| Tumor size | ||||
| <5 cm | 1.00 | 1.00 | ||
| >5 cm | 2.36 (1.29–4.35) | .007 | 2.41 (1.22–4.76) | .014 |
| Tumor depth | ||||
| Superficial | 1.00 | 1.00 | ||
| Deep | 1.41 (0.801–2.47) | .240 | 1.21 (0.652–2.24) | .548 |
| Tumor grade | ||||
| Low grade | 1.00 | 1.00 | ||
| High grade | 1.85 (0.804–4.27) | .152 | 2.98 (1.26–7.06) | .016 |
| Any type of RTx | ||||
| No | 1.00 | 1.00 | ||
| Yes | 0.742 (0.505–1.09) | .131 | 0.530 (0.354–0.793) | .003 |
| Any type of CTx | ||||
| No | 1.00 | |||
| Yes | 0.786 (0.420–1.42) | .453 | ||
| Site of primary tumor | ||||
| Head and neck | 1.00 | 1.00 | ||
| Extremities | 1.22 (0.636–2.35) | .547 | 1.14 (0.563–2.31) | .717 |
| Central | 1.54 (0.793–2.97) | .207 | 1.34 (0.656–2.73) | .427 |
| Surgical margin | ||||
| R0 | 1.00 | 1.00 | ||
| R1 | 2.32 (1.57–3.44) | <.005 | 2.93 (1.94–4.41) | <.001 |
| Univariate | Multivariate | |||
|---|---|---|---|---|
| Variable | HR (95% CI) |
| HR (95% CI) |
|
| Tumor size | ||||
| <5 cm | 1.00 | 1.00 | ||
| >5 cm | 1.66 (0.706–3.90) | .253 | 1.34 (0.548–3.28) | .526 |
| Tumor depth | ||||
| Superficial | 1.00 | |||
| Deep | 0.984 (0.449–2.15) | .968 | ||
| Tumor grade | ||||
| Low grade | 1.00 | 1.00 | ||
| High grade | 1.76 (0.547–5.68) | .352 | 1.479 (0.434–5.05) | .538 |
| Any type of RTx | ||||
| No | 1.00 | |||
| Yes | 1.09 (0.614–1.92) | .779 | 1.00 (0.545–1.85) | .990 |
| Site of primary tumor | ||||
| Head and neck | 1.00 | 1.00 | ||
| Extremities | 1.74 (0.603–5.03) | .310 | 1.56 (0.526–4.65) | .426 |
| Central | 1.79 (0.620–5.20) | .286 | 1.53 (0.517–4.54) | .446 |
| Surgical margin | ||||
| R0 | 1.00 | 1.00 | ||
| R1 | 2.25 (1.28–3.94) | .007 | 2.12 (1.19–3.79) | .015 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeurofibromatosis and Schwannoma Cases · Vascular Malformations and Hemangiomas · Vascular Malformations Diagnosis and Treatment
Malignant peripheral nerve sheath tumors (MPNSTs) are rare and aggressive soft-tissue sarcomas (STS), with 25%–50% of cases occurring in individuals with neurofibromatosis type 1 (NF1).^1,2^ NF1 is an autosomal-dominant genetic disorder in which patients develop various tumor types, including superficial and deep neurofibromas.^3^ The incidence of MPNSTs in NF1 patients is 1 in 2000, compared to 1 in 100 000 in the general population, with a lifetime risk of 8%–13% in NF1 patients.^2–6^ Most NF-1-associated MPNSTs arise from pre-existing plexiform neurofibromas.^7^ Additionally, MPNSTs may also develop sporadically or as a result of radiation exposure in individuals without NF1.^3,7^ Surgical resection with negative margins is the primary treatment for localized MPNSTs, yet recurrence rates, both local and distant, remain high, even after aggressive surgical intervention.^7,8^ To improve local control, perioperative radiotherapy (RTx) is commonly employed.^9^ However, its effectiveness, particularly in NF1-associated MPNSTs compared to sporadic cases, remains inadequately studied.^10^ Clinical guidelines, such as those from the European Society for Medical Oncology (ESMO), recommend individualized treatment strategies based on tumor characteristics, including the use of RTx for high-grade tumors, larger tumors, or in cases with positive surgical margins.^11^ However, in practice, NF1-associated MPNSTs are frequently treated similarly to sporadic cases, even though differences in tumor biology and response to therapy may exist.^12^ While RTx is often employed with the expectation of improving clinical outcomes, its efficacy in NF1-related tumors compared to non-NF1 MPNSTs remains uncertain and warrants further investigation.^12^
Therefore, the primary aim of this project is to evaluate the use of RTx and impact on local recurrence (LR) in MPNST patients, particularly those with NF1.
Materials and Methods
Patient Population
A retrospective cohort investigation, the MONACO study, was conducted across 9 sarcoma centers in the Netherlands and the Mayo Clinic following the approval of institutional review boards at each participating center. This study included patients who underwent surgical treatment for their primary tumor and were diagnosed with pathologically confirmed primary MPNST between 1988 and 2019. Diagnosis for all patients adhered to the World Health Organization’s soft tissue and bone tumor classification guidelines.^13^ Patients whose pathological reports or diagnoses were uncertain based on available information during follow-up were not considered for inclusion in the study. Furthermore, patients who presented with LRs who had previously undergone resection elsewhere were also excluded.
Covariates
Covariates obtained from the medical records for analysis included patient demographics, tumor characteristics, treatment details, and survival-related data. An LR referred to the initial radiological or pathological sign of tumor recurrence at the primary tumor site. Age was determined as the patient’s age at the time of diagnosis. To assess the patients’ physical status, the American Society of Anesthesiologists classification system was employed.^14^ A tumor was classified as NF1-associated based on a confirmed genetic test identifying an NF1 mutation or through clinical assessment.^15^ Tumor size was determined by measuring the largest diameter of the tumor mass, using either imaging techniques or pathology reports. Pathological tumor size was used when available; otherwise, radiologic measurements were used. We could not systematically verify if assessment methods were balanced between groups. Tumor grade was classified into low-grade (grade 1) or high-grade (grade 2 or 3) based on the grading system established by the Fédération Nationale des Centres de Lutte Contre le Cancer (FNCLCC).^16^ Tumors originating below or within the deep fascia were classified as deep-seated. Information on NF1 status was extracted from pathology reports, explicitly stated or inferred from prior reports on plexiform neurofibroma resections or the presence of 2 or more neurofibromas. Surgical margins were classified into three categories with R0 (indicating microscopically negative with no presence of tumor cells in surgical borders), R1 (microscopically positive), and R2 (macroscopically positive). Tumor site was classified as extremity, central (thorax, abdomen, pelvis, retroperitoneal), or head and neck. Triton status was determined by extracting information from pathological reports, specifically when it was explicitly mentioned in the report or when there was a report of MPNST with rhabdomyoblastic differentiation. MPNST occurring in a previously irradiated area that overlapped with the primary tumor site was defined as RTx-associated MPNST. The study’s main endpoints included the use of RTx and the development of an LR in both NF-1 and non-NF1 groups.
Statistical Analysis
All statistical analyses were conducted using R software (version 4.2.2). Baseline characteristics and treatment modalities were compared between all patients with and without RTx administration. This comparison was also performed in a subset of NF1 patients. Overall survival (OS) was defined as the time from definitive surgery to death or the date of last follow-up for both NF1 and non-NF1 patients. Estimated median survival was calculated using the Kaplan–Meier method for several covariates of interest. Univariable and multivariable logistic regression analyses were performed in all patients to identify risk factors associated with RTx utilization. Multivariable Cox Proportional Hazards models were used to estimate the effect of several covariates on the development of LR1 in NF1 patients, considering death as a competing risk.
Candidate predictors were selected based on clinical knowledge and existing literature. Univariable and multivariable analyses with 95% confidence intervals (CIs) were used to assess the impact of covariates on outcomes. For multivariable models, variables with a P-value <.3 or <.4 in the univariable analysis were included, depending on the model criteria. Additionally, multivariable models were refined using backward selection to improve model fit and identify the most significant predictors. Proportional hazards were evaluated visually using Schoenfeld residuals. Missing data were addressed through multiple imputations (m = 20), with pooled estimates following Rubin’s rules.^17^ A P-value ≤.05 was considered statistically significant. Results from the Cox proportional hazards models were expressed as hazard ratios (HRs) with 95% CI. All statistical tests were 2-sided.
Results
Patient Selection and Study Population
A total of 755 patients were included in the MONACO database. Patients were excluded if they presented with metastasis at diagnosis (n = 102), were not treated surgically for the primary tumor (n = 49), underwent R2 resection (n = 76), or had missing data on radiation administration (n = 17) or presented with LR (n = 10) (Figure 1). This left 499 patients eligible for analysis, of whom 281 (56.3%) received RTx as part of their primary treatment. The clinical and tumor characteristics of all patients are detailed in Table 1. The median follow-up time was 60.5 months (mean = 86.8 months, SD = 78.8 months, range = 1 day to 333 months). Radiotherapy was more commonly administered in patients with larger and high-grade tumors, with a median tumor size of 69 mm (IQR 46–104) compared to 59 mm (IQR 40–90.2) in patients who did not receive RTx (P = 0.018). Additionally, extremity tumors were more common among patients who received RTx. Furthermore, we identified a subset of 165 patients with NF1, among whom 57.0% (94 patients) received RTx. Similar trends in indication for RTx were seen among NF1 patients (Supplementary Table 1). Importantly, there was no significant difference in RTx utilization between patients with sporadic tumors and those with NF1, as confirmed in both univariate and multivariable analyses (Table 2). In the sporadic MPNST cohort, the median neoadjuvant RTx dose was 50 Gy (range: 30–56.25 Gy) with a range of 17–30 fractions, and the median adjuvant RTx dose was 60 Gy (range: 27–95 Gy) with a range of 15–38 fractions. Similar dose and fraction distributions were observed in the NF1-associated cohort, with a median neoadjuvant dose of 50 Gy (range: 45–56.25 Gy; 17–30 fractions) and a median adjuvant dose of 60 Gy (range: 27–75 Gy; 15–38 fractions), indicating no meaningful difference in administered RTx doses or fractionation between groups.
Consort flow diagram. A schematic representation of the study inclusion process, illustrating patient selection and exclusion criteria. N = number of patients included at each stage.
Impact of RTx on Local Recurrence
One hundred and forty-three (28.7%) patients (both sporadic and NF1-associated) developed a LR after surgery for their primary tumor. The median time to an LR was 10.9 months (interquartile range [IQR] 0.6–22.8 months). For the NF1 subgroup, the median time to an LR was 10.5 months (IQR 0.6–21.7 months). Multivariable analysis for risk factors associated with LR (Table 3) revealed that tumor size (>5 cm) and tumor grade (high grade) remained significant risk factors for LR, with HRs of 2.41 (95% CI, 1.22–4.76, *P *= .014) and 2.98 (95% CI, 1.26–7.06, P = .016), respectively. R1 margins were strongly associated with increased recurrence risk (HR: 2.93, 95% CI, 1.94–4.41, P < .001). In the full cohort, including both NF1-associated and sporadic MPNST patients, the use of RTx was independently associated with a significantly reduced risk of LR (HR 0.530; 95% CI, 0.354–0.793, P = .003), while NF1 status, tumor depth, and site of primary tumor did not show significant associations with LR. However, in the NF1 patient subgroup, RTx did not significantly reduce the risk of LR (HR 1.00; 95% CI 0.545–1.85; P = .990) (Table 4). In this NF1 subgroup, a total of 165 patients were analyzed, of whom 94 received RTx, and 57 experienced a LR. The only significant risk factor associated with LR risk in NF1 patients was R1 margin status (HR 2.12; 95% CI, 1.19–3.79, P = .015). In addition to multivariable analyses, crude LR rates were assessed to further illustrate subgroup differences. Among patients with sporadic MPNSTs, the LR rate was 27.8% in those who did not receive RTx and 23.3% in those who did. In contrast, NF1-associated MPNST patients exhibited higher LR rates overall, with 33.8% in patients without RTx and 35.1% in those who received RTx. The impact of RTx on OS was not significant across the entire cohort (P = .50) or within subgroups, including NF1 (P = .93) and non-NF1 patients (P = .62). Detailed survival analyses are presented in Supplementary Figures 1 and 2.
Discussion
In this study, a large cohort of patients with MPNST was analyzed, with just over half (56%) of the patients receiving RTx as part of their primary treatment. Factors such as tumor size, grade, and margin status were associated with an increased risk of LR. In patients with NF1, only positive surgical margins were significantly associated with the development of LR, whereas RTx did not affect LR risk in this group, in contrast to sporadic cases.
For MPNSTs, surgical excision remains the cornerstone of treatment, but achieving complete resection is often challenging in the balance between local controle and limbsalvage. One study, analyzing 784 MPNST, showed that complete resection (R0) was achieved in 66.3% of patients.^18^ As in other STS, RTx is commonly administered to decrease LR rates but has not been shown to correlate with improved survival.^19^ While surgical excision with negative margins remains the most important determinant of local control and potential cure, RTx serves as an adjunct in cases where adequate margins cannot be achieved.^11^ Importantly, in cases where tumors are located near critical neurovascular structures, neoadjuvant RTx can facilitate limb-sparing surgery by reducing tumor size and allowing for less extensive resections, thereby avoiding mutilating procedures such as amputation and preserving function.^20,21^ To date, no research has shown that MPNSTs require a different treatment approach compared to other high-grade STS.^22,23^ Therefore, the treatment guidelines for MPNSTs largely align with those established for general STS.^11,24^ Generally, according to ESMO guidelines, RTx is recommended for tumors with aggressive features such as ≥5 cm in size, high grade, or R1/R2 margins.^11^ In practice, however, RTx use varies significantly between centers, and not all eligible patients receive it.^19^ Differences in institutional protocols, specialist preferences, and biases can lead to inconsistent RTx use, even in high-grade sarcoma cases.^19^ In our cohort, similar variability was seen, with some patients not receiving RTx despite meeting guideline criteria. In our study, we observed that RTx usage patterns in NF1 patients were similar to those in sporadic cases, consistent with literature advocating RTx use in NF1 patients.^25^ It is important to note that there was an imbalance in baseline risk factors between patients who received RTx and those who did not. Specifically, patients treated with RTx were more likely to have larger and higher-grade tumors, which are known negative prognostic factors for LR. This imbalance may have influenced the observed outcomes and should be considered when interpreting the results. The role of RTx in decreasing LR rates remains inconclusive, as varying results have been reported across the literature.^26^ Our LR rate of approximately 30% reflects similar outcomes in other studies combining surgery and RTx.^8,27^ Our findings show that the effect of RTx on LR rates differs between NF1-associated and sporadic MPNSTs. In sporadic cases, RTx was significantly associated with a reduction in LR; however, in NF1-associated MPNSTs, no significant benefit of RTx on LR rates was observed.
A potential explanation for this could be the biological and pathological differences between NF1-associated and sporadic tumors. NF1-associated MPNSTs are often more aggressive and exhibit distinct tumor pathology.^28^ Additionally, in NF1 patients, the neurofibromas surrounding the tumor could have undergone pre-malignant changes, raising the risk of recurrence or secondary tumor formation and potentially limiting the effectiveness of RTx in improving LR rates. Another possible explanation may lie in the underlying molecular and genetic complexity of NF1-associated MPNSTs, which is not yet fully understood.^28^ Although studies have identified recurrent genomic alterations in MPNSTs, no consistent molecular differences between NF1-associated and sporadic MPNSTs have been confirmed.^29–33^ This lack of clarity complicates the prediction of treatment response and suggests that molecular differences may influence treatment outcomes, although specific pathways, such as those involving EGFR or TP53, remain speculative and unproven in their role of RTx resistance.^34–40^ Nevertheless, this finding should be interpreted with caution, as the possibility of a Type II error cannot be excluded. Our study may have been underpowered to detect a significant difference in LR risk reduction with RTx in NF1-associated MPNSTs. Further research with larger cohorts is warranted to validate these results and better define the role of RTx in NF1-associated MPNSTs.
Furthermore, the value of RTx for reducing LR in MPNSTs overall remains ambiguous in the literature.^7,27,41,42^ Many studies do not differentiate between NF1-associated and sporadic MPNSTs when assessing the efficacy of RTx.^8,12,27^ As a result, the reported benefit of RTx may primarily reflect its impact on sporadic tumors, where it has been more consistently associated with reduced LR rates. This conflation of NF1-associated and sporadic cases might mask crucial distinctions in treatment response, particularly given the unique molecular and pathological characteristics of NF1-associated MPNSTs. The lack of subgroup analyses obscures whether NF1-associated MPNSTs respond similarly, leaving a critical gap in understanding the true efficacy of RTx in this specific context. Future studies should prioritize the stratification of outcomes by NF1 status to determine whether and under what conditions RTx offers meaningful benefits for NF1-associated MPNSTs. While our study demonstrates the above findings, it is important to acknowledge that data on the dose of RTx were not available. The efficacy of RTx, particularly in reducing LR, is known to be dose-dependent, and the absence of dose data limits our ability to assess whether variations in dose could have influenced the outcomes observed in our cohort. Therefore, future studies should include detailed dose information to provide further insights into the optimal radiation dose for treating MPNSTs, particularly for those with NF1.
The role of RTx in reducing LR in MPNSTs must also be carefully weighed against potential disadvantages. It has been reported that MPNSTs have been caused by RTx.^43,44^ This concern is especially relevant in NF1 patients, where RTx has been associated with an increased risk of secondary malignancies, including radiation-induced MPNSTs, as documented in several studies.^45,46^ In addition to the risk of secondary MPNSTs in NF1 patients, RTx carries other potential complications that affect both NF1-associated and sporadic cases. For both groups, RTx has been associated with risks such as wound healing complications when administered preoperatively and late-onset radiation toxicities when used postoperatively.^47^ Balancing the benefits of RTx against the risks of secondary malignancies and functional impairments is crucial in treatment planning for both NF1-associated and sporadic MPNST patients. For NF1 patients in particular, careful consideration may be needed due to the elevated risk of secondary malignancies associated with RTx.^46,47^ A multidisciplinary evaluation for both patient groups is essential to ensure optimal care and to tailor treatment strategies to individual needs.^7^
Given the possible absence of significant improvement in LR rates with the use of RTx, it may be advisable to apply a more cautious approach to RTx in NF1 patients, particularly when tumors arise within plexiform neurofibromas. The inherent pre-malignant nature of the surrounding tissue in these cases and the limited impact of RTx on OS and LR outcomes suggest that RTx may offer minimal benefit while posing additional risks.
This multicenter retrospective study has limitations inherent to its design, such as potential selection bias resulting from selective loss of follow-up and missing data. Nevertheless, a multiple imputation technique was employed to reduce this risk of bias. Additionally, the extended study period of 30 years saw the introduction of various new techniques and advancements in radiation therapy delivery, which may have led to variations in treatment standards that could influence the findings. However, due to a lack of detailed data on modality and quality, potential improvements in imaging and RTx techniques over time could not be assessed. Other key limitations include variability in treatment protocols across different centers and the heterogeneity of tumors. Factors such as tumor size, resection margin, malignancy grade, and other often unknown factors likely influenced the decision to administer RTx, which could have affected the primary outcome. Moreover, variations in radiation doses and techniques over time may have influenced treatment effectiveness, an aspect that should be considered when interpreting the results. Another important limitation is the lack of detailed data on the margin extent beyond the R0 versus R1 classification. Precise information on margin width (eg, in millimeters) was not available. This limited our ability to explore more nuanced associations between the degree of surgical clearance and local control. Future studies could investigate whether variations in margin width within the R0 category, such as planned close margins in combination with adjuvant RTx, affect local control outcomes, as this remains a clinically relevant question. Despite these limitations, the large size of this international cohort study on MPNSTs provides valuable insights. To our knowledge, this is the largest cohort study on RTx in MPNSTs, allowing for a more comprehensive analysis of treatment outcomes. The study’s focus on specific histological subtypes, such as NF1, along with detailed clinical and treatment information, enhances our understanding of tumor behavior and aids in tailoring ideal treatment strategies. Furthermore, the multicenter design enhances the generalizability of the findings, as data were collected from multiple sarcoma centers, thus reflecting a diverse patient population and treatment practices.
Conclusion
In conclusion, this multicenter study demonstrates that while RTx is frequently utilized in the treatment of MPNSTs, its benefit may be limited to certain cases of sporadic MPNSTs, where it is associated with a lower risk of LR. However, this advantage may not extend to the NF1 subpopulation. Despite a substantial number of patients receiving RTx, factors such as tumor size, grade, and surgical margins play a critical role in determining treatment outcomes.
Supplementary material
Supplementary material is available online at Neuro-Oncology (https://academic.oup.com/neuro-oncology).
noaf186_Supplementary_Materials_1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Edizer DT , Özdoğan A, Karaman E, Işıldak H. Report of a case of malignant peripheral nerve sheath tumor of the neck with an early local recurrence. Ear Nose Throat J. 2011;90(10):E 1–E 3.10.1177/01455613110900101522033963 · doi ↗ · pubmed ↗
- 2Du P , Zhu J, Zhang ZD, et al Recurrent epithelioid malignant peripheral nerve sheath tumor with neurofibromatosis type 1: a case report and literature review. Oncolo Lett. 2019;18(3):3072–3080.10.3892/ol.2019.10676 PMC 670427931452784 · doi ↗ · pubmed ↗
- 3James AW , Shurell E, Singh A, Dry SM, Eilber FC. Malignant peripheral nerve sheath tumor. Surg Oncol Clin N Am.2016;25(4):789–802.27591499 10.1016/j.soc.2016.05.009 · doi ↗ · pubmed ↗
- 4Martin E , Geitenbeek RTJ, Coert JH, et al A Bayesian approach for diagnostic accuracy of malignant peripheral nerve sheath tumors: a systematic review and meta-analysis. Neuro-Oncology.2021;23(4):557–571.33326583 10.1093/neuonc/noaa 280PMC 8041346 · doi ↗ · pubmed ↗
- 5Geitenbeek RTJ , Martin E, Graven LH, et al Diagnostic value of 18F-FDG PET-CT in detecting malignant peripheral nerve sheath tumors among adult and pediatric neurofibromatosis type 1 patients. J Neurooncol.2022;156(3):559–567.35025020 10.1007/s 11060-021-03936-y PMC 8860956 · doi ↗ · pubmed ↗
- 6Uusitalo E , Rantanen M, KallionpääRA, et al Distinctive cancer associations in patients with neurofibromatosis type 1. J Clin Oncol. 2016;34(17):1978–1986.26926675 10.1200/JCO.2015.65.3576 · doi ↗ · pubmed ↗
- 7Kahn J , Gillespie A, Tsokos M, et al Radiation therapy in management of sporadic and neurofibromatosis type 1-associated malignant peripheral nerve sheath tumors. Front Oncol.2014;4(4):324.25452937 10.3389/fonc.2014.00324 PMC 4233912 · doi ↗ · pubmed ↗
- 8Bishop AJ , Zagars GK, Torres KE, et al Malignant peripheral nerve sheath tumors: a single institution’s experience using combined surgery and radiation therapy. Am J Clin Oncol.2018;41(5):465–470.27281262 10.1097/COC.0000000000000303 PMC 5145780 · doi ↗ · pubmed ↗