A gender-based investigation of risk factors for infectious complications after percutaneous nephrolithotomy for kidney stones: insight for personalized management
Federica Passarelli, Ludovico Maria Basadonna, Fabio Ciamarra, Gianpaolo Lucignani, Francesco Ripa, Stefano Paolo Zanetti, Elisa De Lorenzis, Giancarlo Albo, Emanuele Montanari, Luca Boeri

TL;DR
This study finds that women have a higher risk of infections after kidney stone surgery than men, with different risk factors for each gender.
Contribution
The study identifies gender-specific risk factors and thresholds for postoperative infections after PCNL.
Findings
Females had a higher rate of postoperative infectious complications than males.
In females, longer operative time and residual stones were key infection predictors.
In males, preoperative urine culture and residual stones were significant predictors.
Abstract
To investigate gender-related predictors of infectious complications after percutaneous nephrolithotomy (PCNL) in a large cohort of patients with kidney stones. We retrospectively analysed data from 492 consecutive patients who under-went PCNL at a single tertiary-referral academic center (01/2016-09/2024). Patient’s demographics, stones characteristics and operative data were collected. Stone-free status was defined as no residual stones. Complications were graded according to modified Clavien classification. Descriptive statistics and logistic regression models were used to identify factors associated with postoperative infectious complications according to patient’s gender. Females accounted for 39.2% of the population and showed a significantly higher rate of postoperative infectious complications compared to males (24.9% vs. 16.7%, p = 0.02). Preoperative positive bladder urine…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
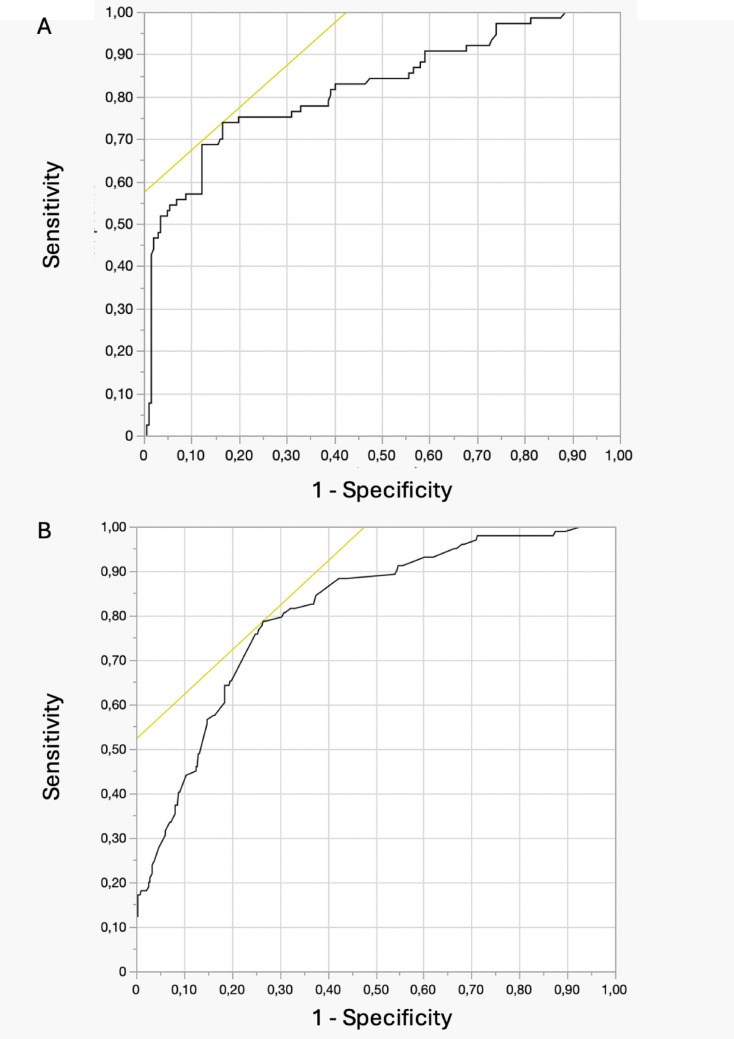 Figure 1
Figure 1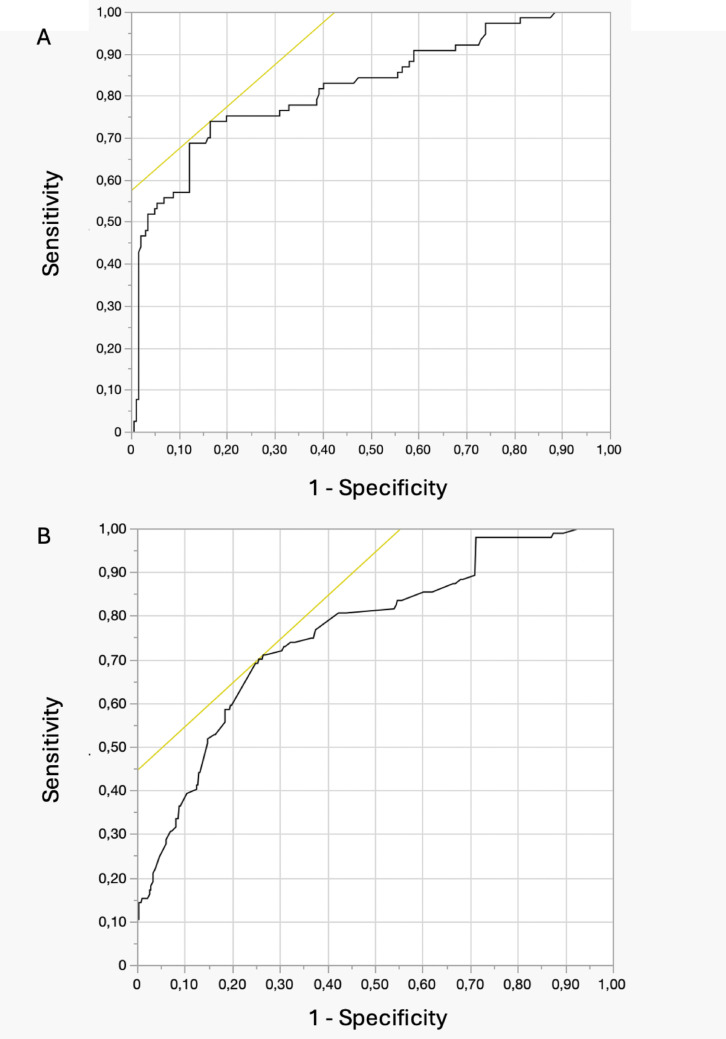 Figure 2
Figure 2- —Università degli Studi di Milano
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsKidney Stones and Urolithiasis Treatments · Urinary Tract Infections Management · Dialysis and Renal Disease Management
Introduction
Percutaneous nephrolithotomy (PCNL) is the gold standard surgical treatment for large and complex kidney stones, offering high stone clearance rates, minimal surgical trauma, and rapid postoperative recovery [1, 2]. This approach is especially favored for challenging cases, including staghorn and infection-related stones [3, 4]. Despite its effectiveness, PCNL carries a risk of various postoperative complications, ranging from minor urinary leakage to severe bleeding and infectious events, which can significantly impact patient post-operative outcomes [5]. Among these, postoperative fever is the most frequent complication, occurring in 21.0% to 39.8% of cases [6]. Notably, fever is an established predictor of severe infectious outcomes, including sepsis and septic shock, highlighting its critical importance in patient management [6]. Furthermore, postoperative fever represents a key clinical component of the systemic inflammatory response syndrome (SIRS) and may reflect the early onset of a systemic inflammatory reaction even in the absence of positive microbiological cultures [7]. Several clinical and procedural factors have been identified as predictors of infectious complications following PCNL and are routinely considered in perioperative risk stratification. These include positive preoperative bladder urine culture (BUC), positive stone cultures, diabetes mellitus, multiple access tracts, larger stone burden, presence of hydronephrosis, staghorn calculi, struvite stone composition, residual fragments and prolonged operative time [8, 9].
In recent years, among various risk factors, growing attention has been directed toward gender-related differences in the epidemiology and clinical course of urolithiasis, particularly in relation to infectious complications. Recent studies have consistently shown that female patients exhibit a higher risk of developing stone-related infections and urosepsis compared to their male counterparts, a disparity potentially attributable to anatomical, hormonal, and microbiological differences in the urinary tract [10, 11].
Despite these observations, the impact of gender on infection-related outcomes has not been systematically investigated in the context of surgical interventions such as PCNL, leaving a critical gap in our understanding of sex-specific risk stratification and perioperative management. Most available data focus on established clinical or procedural risk factors in the general population, with limited attention paid to sex-specific variables that may influence infection risk after surgical stone treatment. This represents a critical gap in literature, particularly given the increasing emphasis on personalized medicine and stratified perioperative care. Therefore, the aim of our study was to investigate gender-related predictors of infectious complications following PCNL in a large, real-life cohort of patients with kidney stones.
Materials and methods
We retrospectively analyzed data from 527 patients who underwent PCNL at a tertiary referral academic center between January 2016 and September 2024. Demographic and clinical data were collected. Health-relevant comorbidities were assessed using the Charlson Comorbidity Index (CCI) [12].
Stone characteristics were evaluated based on non-contrast-enhanced computed tomography (CT), which was performed in all patients prior to surgery. Stone volume was calculated using the ellipsoid formula (length × width × height × π × 1/6) [13]. The mean stone density in Hounsfield units (HU), presence of multiple stones and staghorn calculi were assessed. The results of preoperative bladder urine cultures were recorded [14]. Patients with negative results were administered a single dose of prophylactic parenteral antibiotics prior to surgery, with cephalosporins preferred in the absence of allergies. Patients with asymptomatic bacteriuria received targeted antimicrobial treatment for 48 to 72 h before surgery. If leukocytosis, urinary symptoms, or fever were present, the procedure was delayed until the patient completed a full course of antibiotics and obtained a sterile urine culture [15, 16]. Stones were classified as infected based on microbiological analysis.
All surgical procedures were performed under general anesthesia by experienced urologists using either standard or mini-PCNL (mPCNL) techniques. Among the mPCNL procedures, vacuum-assisted mPCNL (vamPCNL) [17, 18] and vacuum-cleaner mPCNL (vcmPCNL) [3] were adopted as previously described. The use of multiple percutaneous access tracts was recorded. Operative time was measured from the initial puncture to the completion of stone removal. Postoperative outcomes included length of hospital stay, presence of infectious complications and overall complication rate, classified according to the PCNL-adjusted Clavien-Dindo classification [19]. Infectious complications were defined as systemic inflammatory response syndrome (SIRS) with bacteremia or bacteriuria, as previously described [20]. Patients underwent a CT scan within three months postoperatively to assess the presence of residual fragments [21].
We excluded patients with congenital renal anomalies (n = 3), cases involving additional concomitant procedures other than mPCNL and endoscopic combined intrarenal surgery (n = 7), scheduled staged procedures for large stone burden (N = 27). A final sample of 492 (93.6%) patients was considered for statistical analysis.
Data collection followed the principles outlined in the Declaration of Helsinki. All patients signed an informed consent agreeing to share their own anonymous information for future studies. The study was approved by our Hospital Ethical Committee (Prot. 25508).
Statistical analysis
Distribution of data was tested with the Shapiro–Wilk test. Data are presented as medians (interquartile range; IQR) or frequencies (proportions). Statistical analysis was conducted in several stages. Initially, descriptive statistics were used to characterize the entire study cohort. Subsequently, differences in clinical and operative parameters between patients who developed infectious complications and those who did not (-infections) were assessed using the Mann–Whitney U test and Chi-square test, as appropriate.
To identify potential predictors of postoperative infectious complications, across the entire cohort, both univariate and multivariate logistic regression analyses were performed. Following the identification of gender as a potential risk factor for infections, further analyses were conducted to evaluate clinical and laboratory differences between male and female patients using the Mann–Whitney U test and Fisher exact test.
Next, we examined whether clinical characteristics and postoperative infectious risk factors varied by gender. Descriptive statistics were used to compare clinical and surgical variables between +infections and -infections patients within each gender group. Univariate and multivariate logistic regression analyses were then applied separately within male and female subgroups to identify gender-specific risk factors for infectious complications.
Lastly, Receiver Operating Characteristic (ROC) curve analysis, along with the Youden index, was employed to determine optimal cutoff values for infections prediction in each gender group.
Statistical analyses were performed using SPSS v.28 (IBM Corp., Armonk, NY, USA). All tests were two sided and statistical significance level was set at p < 0.05.
Results
Table 1 depicts demographic and clinical characteristics of the cohort, stratified by gender. In the whole cohort, median age and BMI were 58 years (IQR 49–66) and 24.7 kg/m² (IQR 22.2–28.1), respectively. Females accounted for 39.2% of patients, and 193 (39.2%) had a CCI ≥ 1. The median stone volume was 2.6 cm³ (1.1–5.1), with 72.9% having multiple stones and 32.9% staghorn stones. Preoperative positive BUC was present in 20.7% of patients, more frequently in females than males (27.9% vs. 16.1%, p = 0.01), and infected stones were also more common in females (32.6% vs. 17.4%, p = 0.001). mPCNL was performed in 416 cases (84.6%), with a median operative time of 95 min (IQR 75–130). Infectious complications occurred in 19.9% of patients. Of these, 5.9% developed sepsis and 0.6% required intensive care unit admission. Among patients who developed infectious complications, Escherichia coli was identified in 38% of cases, Proteus mirabilis in 21%, Enterococcus faecalis in 29%, and mixed microbial flora in 22%. Concordance between preoperative and postoperative cultures was observed in 44.8% of cases. Overall, 23.9% of complications were low-grade (Clavien-Dindo I–II) and 5.5% high-grade (IIIa/b). The overall stone-free rate (SFR) was 78.9%.Table 1. Demographic characteristics of the study cohort according to gender (No. = 492)TotalMaleFemaleP Value*No. of patients [No. (%)]492299 (60.8)193 (39.2)Age (years)0.8Median (IQR)58 (49-66)55 (48-64)55 (44-62)Range19 - 8520 - 8519 – 81BMI (kg/m^2^)0.8Median (IQR)24.7 (22.2-28.1)24.9 (22.6-27.8)24.3 (21.2-28.7)Range17.9 – 38.817.9 – 36.818.1 – 38.8CCI0.9Mean (SD)0.7 (1.1)0.8 (1.2)0.4 (0.8)Median (IQR)0 (0-1)0 (0-2)0 (0-1)Range0 – 60 – 50 - 6CCI ≥1 [No. (%)]193 (39.2)118 (39.4)75 (38.8)0.8Stone volume (cm^3^) 0.3Median (IQR)2.6 (1.1-5.1)2.8 (1.0-5.6)2.5 (1.2-4.5)Range0.5 – 61.20.5 – 61.20.5 – 48.8Multiple stones[No. (%)] 359 (72.9) 224 (74.9) 135 (69.9) 0.2Staghorn stone[No. (%)] 162 (32.9) 91 (30.4) 71 (36.8) 0.1Mean stone density (HU)0.6Median (IQR)848 (600-1000)855 (607-1020)831 (624-1000)Range150 – 1983150 – 1983190 - 1500Preoperative positiveBUC No. [(%)] 102 (20.7) 48 (16.1) 54 (27.9) 0.01mPCNL procedure[No. (%)] 416 (84.6) 248 (82.9) 168 (87.0) 0.2Preoperative indwelling stent[No.(%)] 51 (10.4) 32 (10.7) 19 (9.8) 0.6Multiple access tracts[No. (%)] 78 (15.9) 47 (15.7) 31 (16.1) 0.8Operative time (min)0.1Median (IQR)95 (75-130)110 (80-135)105 (80-132)Range30 – 18040 – 18030 - 180Hospitalization time (days)0.5Median (IQR)5 (4-7)5 (3-7)4 (4-7)Range2 – 502 – 502 – 42Infected stone [No. (%)]115 (23.4)52 (17.4)63 (32.6)0.001Stone free rate [No. (%)]388 (78.9)240 (80.2)148 (76.6)0.2Any complications [No. (%)]145 (29.5)Postoperative complications[No. (%)] (Highest Clavien score)Clavien-Dindo I-II118 (23.9)Clavien-Dindo IIIa/b27 (5.5)*BMI: * body mass index; CCI: Charlson Comorbidity Index; HU: * Hounsfield unit; BUC: Bladder urine culture; mPCNL: mini percutaneous nephrolithotomyP value according to the Mann-Whitney U test for continuous data and the Fisher Exact Test for categorical variables, as indicated
Table 2 reports demographic and clinical characteristics according to the occurrence of postoperative infectious complications. Infections were more frequent in females than males (24.9% vs. 16.7%, p = 0.02). Patients with infections had significantly larger stone volumes [5.3 (1.8–14.6) vs. 2.3 (0.9–4.2) cm³, p < 0.001], and a higher prevalence of multiple stones (p = 0.01) and staghorn calculi (p = 0.001). Preoperative positive BUC (p = 0.01) and infected stones (39.7% vs. 19.2%, p = 0.001) were also more common in the infected group. Patients with infections more often underwent standard PCNL (p = 0.01), required multiple access tracts (p = 0.01), had longer operative times [120 (90–156) vs. 90 (73–120) min, p < 0.001], and longer postoperative hospitalization (p < 0.001) than those without infections. SFR was significantly lower in patients with infections (61.2% vs. 83.2%, p = 0.001).Table 2. Demographic characteristics of the study cohort according to the presence of sepsis (No. = 492) Infections+ Infectionsp valueNo. of patients [No. (%)]394 (80.1)98 (19.9)Age (years)0.3Median (IQR)59 (49-67)58 (49-66)Range19 – 8520 - 84Gender [No. (%)]0.02Female145 (75.1)48 (24.9)Male249 (83.3)50 (16.7)BMI (kg/m^2^)0.5Median (IQR)24.7 (22.3-27.7)25.0 (21.9-29.4)Range17.9 – 38.818.1 – 37.9CCI0.4Mean (SD)0.7 (1.1)0.8 (1.2)Median (IQR)0 (0-1)0 (0-1)Range0 – 60 - 5CCI ≥1 [No. (%)]152 (38.5)41 (41.8)0.2Stone volume (cm^3^)<0.001Median (IQR)2.3 (0.9-4.2)5.3 (1.8-14.6)Range0.5 – 50.10.5 – 61.2Multiple stones [No. (%)]276 (70.1)83 (84.7)0.01Staghorn stone [No. (%)]111 (28.2)51 (52.0)0.001Mean stone density (Hounsfield unit)0.2Median (IQR)850 (650-1050)790 (595-930)Range150 – 1983300 - 1500Preoperative positive BUCNo. [(%)] 66 (16.7) 36 (36.7) 0.01Procedure type [No. (%)]0.01mPCNL346 (87.8)70 (71.4)standard PCNL48 (12.1)28 (28.5)Preoperative indwelling stent [No. (%)] 39 (9.8) 12 (12.2) 0.1Multiple access tracts [No. (%)] 50 (12.7) 28 (28.6) 0.01Operative time (min)<0.001Median (IQR)90 (73-120)120 (90-156)Range30 – 18048 - 180Hospitalization time (days)<0.001Median (IQR)4 (3-6)8 (5-12)Range2 – 303 – 50Infected stone [No. (%)]76 (19.2)39 (39.7)0.001Stone free rate [No. (%)]328 (83.2)60 (61.2)0.001BMI*: body mass index; CCI: Charlson Comorbidity Index; BUC: Bladder urine culture; mPCNL: mini percutaneous nephrolithotomy*P value according to the Mann-Whitney U test for continuous data and the Fisher Exact Test for categorical variables, as indicated
Table 3 shows univariate (UVA) and multivariate (MVA) logistic regression analyses of factors associated with postoperative infectious complications. In the MVA, female gender (OR 2.1; p = 0.02), preoperative positive BUC (OR 3.6; p < 0.01), and residual stones (OR 0.21; p = 0.01) were identified as independent predictors of post-PCNL infection, after adjusting for age and stone volume.Table 3. Logistic regression models predicting infectious complications in the whole cohortORP value95% CIORP value95% CIUVA modelMVA modelAge1.10.30.97 – 1.25Female gender2.3<0.011.12 - 4.952.10.021.02 – 3.76CCI≥11.10.570.72 - 1.78Stone Volume1.1<0.011.04 - 1.231.20.10.98 - 1.56Stone density (HU)0.90.20.98 - 1.09Preoperative indwelling stent1.10.20.96 – 1.34Preoperative positive BUC2.90.011.81 – 4.863.6<0.011.82 - 9.45Operative time1.10.011.02 - 1.341.080.10.97 – 1.12mPCNL vs standard0.40.010.21 – 0.62Stone free status0.30.010.23 – 0.610.210.010.09 – 0.52*UVA *:Univariate model; MVA: Multivariate model, CCI :Charlson Comorbidity Index; BUC: Bladder urine culture; mPCNL: mini percutaneous nephrolithotomy;
Table 4 compares baseline and intraoperative parameters between patients with and without postoperative infectious complications, stratified by gender.
In males, patients with infections had a higher comorbidity burden (CCI ≥ 1, p = 0.01), larger stone volumes (p = 0.01), higher rates of positive BUC, and longer operative times (p = 0.01) than those without infections. SFR was lower in males with infections (76.6% vs. 84.3%, p = 0.01). In females, those with infections also had significantly larger stone volumes (p = 0.01), longer operative times (p = 0.01), and higher rates of positive BUC (p = 0.01) compared to females without infections. SFR was lower in females with infections (60.4% vs. 82.1%, p = 0.01). Notably, stone volume and operative time in females with infections were significantly lower than in males with infections [2.8 (1.3–15.5) vs. 5.5 (2.7–15.5) cm³, p = 0.01; 115 (95–150) vs. 130 (85–166) min, p = 0.01].Table 4. Demographic characteristics and descriptive statistics of patients according to infections development in the male and female groupMale cohortFemale cohortInfections+ Infectionsp-value^^Infections+ Infectionsp-value^^No. of patients [No. (%)]249 (83.3)50 (16.7)145 (75.1)48 (24.9)Age (years)0.70.2Median (IQR)59 (49-66)58 (49-64)59 (48-70)56 (49-63)Range20 - 8520 – 8224 – 8124 - 81BMI (kg/m^2^)0.60.7Median (IQR)24.8 (22.5-27.7)24.9 (23.4-28.1)24.6 (21.9-27.6)25.1 (21.1-30.2)Range17.9 – 36.818.1 – 36.618.1 – 38.818.5 – 38.8CCI0.020.1Mean (SD)0.6 (0.9)1.2 (1.4)0.8 (1.3)0.7 (0.9)Median (IQR)0 (0-1)0 (0-2)0 (0-1)0 (0-1)Range0 – 50 – 50 – 60 - 5CCI ≥1 [No. (%)]91 (36.5)27 (54.0)0.0161 (42.1)14 (29.2)0.1Stone volume (cm^3^)0.010.01Median (IQR)2.6 (0.9-4.8)5.5 (2.7-15.5)1.9 (0.9-3.6)2.8 (1.3-15.5)Range0.5 – 61.21.2 – 53.50.5 – 18.90.5 – 48.8Multiple stones [No. (%)]224 (74.9)135 (69.9)0.295 (65.5)40 (83.3)0.02Staghorn stone [No. (%)]62 (24.8)29 (58.0)0.0149 (33.8)22 (45.8)0.1Mean stone density (Hounsfield unit)0.80.9Median (IQR)841 (585-1003)858 (605-925)900 (645-1032)750 (560-940)Range150 – 1983450 – 1200190 – 1500300 - 1500Preoperative positive BUC No. [(%)]29 (11.6)19 (38.0)0.0135 (24.1)19 (42.2)0.01mPCNL procedure [No. (%)]216 (86.7)32 (64.0)0.01129 (88.9)39 (81.3)0.2Multiple access tracts [No. (%)]34 (13.7)13 (26.0)0.0216 (11.0)15 (31.3)0.01Operative time (min)0.010.01Median (IQR)90 (75-120)130 (85-166)90 (70-113)115 (95-150)Range40 – 18050 – 18030 – 18048 - 180Hospitalization time (days)0.010.01Median (IQR)4 (3-6)9 (6-13)4 (3-5)7 (5-10)Range2 – 503 – 402 – 183 - 42Infected stone [No. (%)]31 (12.4)21 (42.0)0.00140 (27.5)23 (47.9)0.01Stone free rate [No. (%)]210 (84.3)30 (76.6)0.01119 (82.1)29 (60.4)0.01BMI: body mass index; CCI: Charlson Comorbidity Index; BUC: Bladder urine culture; mPCNL: mini percutaneous nephrolithotomyp < 0.01 vs. +infections group of the male cohort.
Table 5 presents gender-stratified logistic regression analyses of predictors for postoperative infectious complications. In males, MVA identified preoperative positive BUC (OR 1.8; p < 0.001) and stone-free status (OR 0.22; p = 0.02) as independent predictors of infection, after adjusting for CCI, stone volume, and operative time. In females, operative time (OR 1.1; p = 0.01), preoperative positive BUC (OR 2.0; p = 0.01), and SFR (OR 0.2; p = 0.02) were independently associated with postoperative infections, after accounting for stone volume.Table 5. Logistic regression models predicting infectious complications in the male and female cohortUVA modelMVA modelMale cohortOR, p-value95% CIOR, p-value95% CIAge1.1, 0.70.96 – 1.35CCI≥12.0, 0.021.09 - 3.792.1; 0.10.69 – 6.45Stone Volume1.1; <0.011.01 - 1.291.1; 0.20.97 - 1.21Preoperative positive BUC1.9; 0.011.11 – 4.861.8; <0.0011.21 - 5.87Operative time1.1; 0.011.02 - 1.371.01; 0.40.98 – 1.45mPCNL vs standard0.2; 0.010.13 – 0.60Stone free status0.4; 0.010.22 – 0.830.22; 0.020.06 – 0.83Female cohortAge1.1, 0.40.96 – 1.95CCI≥11.0, 0.60.82 - 1.23Stone Volume1.2; <0.011.05 - 1.311.1; 0.50.91 - 1.21Preoperative positive BUC2.1; 0.011.02 – 6.622.0; 0.011.12 - 6.67Operative time1.1; 0.011.01 - 1.441.1; 0.011.02 – 1.93mPCNL vs standard0.5; 0.10.22 – 1.33Stone free status0.3; 0.010.16 – 0.650.2; 0.020.03 – 0.48Infected stone1.0; 0.30.85 – 1.56UVA: Univariate model; MVA: Multivariate model, CCI: Charlson Comorbidity Index; BUC: Bladder urine culture; mPCNL: mini percutaneous nephrolithotomy
ROC curves showed that, in the female group, stone volume of 3.9 cm^3^ and operative time of 96 min had the best predictive ability for post-PCNL infectious complications. In men, stone volume of 5.1 cm^3^ and operative time of 137 min were the best predictors for infections (Table 6)(Figs. 1 and 2).Table 6ROC curves for predictors of infectious complications in the male and female cohortYouden indexSensitivitySpecificityAUCYouden indexSensitivitySpecificityAUCMaleFemaleStone volume (cm^3^)5.175.2%73.1%0.803.975.2%72.9%0.79Operative time (min)13774.9%72.8%0.779676.1%75.6%0.81
Fig. 1. Receiver Operating Characteristic (ROC) curve analysis showing the predictive ability of stone volume (A) and operative time (B) for infectious complications in the female cohort
Fig. 2. Receiver Operating Characteristic (ROC) curve analysis showing the predictive ability of stone volume (A) and operative time (B) for infectious complications in the male cohort
Discussion
The primary aim of our study was to evaluate gender-specific predictors of infectious complications following PCNL in a large, real-world cohort of patients with kidney stones.
We showed that, in our cohort, females were at higher risk of post-PCNL infections than males. Preoperative positive BUC and residual stones were independent predictors in both sexes, while operative time had a greater impact in females. ROC analysis showed that females developed infections at lower stone volumes and shorter operative times than males, suggesting sex-specific differences in susceptibility to surgical stress. These findings provide a novel and detailed understanding of sex-specific risk factors for postoperative infections after PCNL, highlighting the importance of individualized risk stratification.
Across literature, several risk factors have been consistently associated with postoperative infectious complications in the general population. These include older age, larger stone and tract sizes, longer operative time, positive preoperative BUC, multiple access tracts, hydronephrosis, and struvite stone composition [6, 8, 16, 22, 23]. Our results corroborate these studies and confirm the higher risk of infections following standard PCNL than miniaturized procedures. Although standard PCNL is generally associated with lower irrigation pressure, it is typically reserved for larger and more complex stones, which likely explains the higher rate of postoperative infectious complications in this group. Conversely, mPCNL, despite potentially higher irrigation pressures, in our cohort, is usually performed using suction techniques that reduce intra-renal pressure (IRP) by continuously aspirating irrigation fluid and stone fragments. This not only shortens operative and lithotripsy times but also lower infection risk [18, 24, 25].
This study further emphasized the influence of gender-specific differences in terms of post-PCNL infectious complications. Xun et al. also reported a significant association between female gender, positive urine culture, and postoperative fever, supporting the hypothesis of a sex-related predisposition to infectious complications [26]. Although female sex has been frequently identified as a risk factor, to the best of our knowledge, no previous work has systematically investigated gender-stratified predictors of infectious complications following PCNL.
In our study, postoperative infections in males appeared to be primarily driven by preoperative infectious parameters, such as positive BUC, as well as the presence of residual stones, suggesting the persistence of infection-related risk factors and incomplete stone clearance may play a central role in the development of complications. Furthermore, residual fragments following PCNL have been shown to significantly influence patient outcomes [27]. In females, in addition to positive BUC and lower SFR, longer operative time emerged as the most relevant predictors of infectious events, highlighting the potential impact of surgical burden and procedural efficacy in this subgroup. Further supporting this sex-specific pattern, we showed that stone volume and operative time of females with infections were significantly lower than those of males who had infections complications, suggesting a potentially increased susceptibility or differing physiological response to surgical stress.
The higher susceptibility of female patients to post-PCNL infectious complications at lower stone volumes and shorter operative times may be explained by several biologically plausible mechanisms. Women have higher baseline rates of bacteriuria and urinary tract infections, in part due to anatomical differences, which facilitate bacterial ascent [28]. In patients with urolithiasis, the urinary microbial spectrum also differs by sex, with Escherichia coli being more frequently isolated in females [29]. Moreover, females are more likely to develop infection-related stones, such as struvite or carbonate apatite calculi, which are directly associated with bacterial colonization and may predispose to postoperative infectious events [30].
Interestingly, a similar host-related susceptibility has been observed in a large pediatric PCNL cohort, where prolonged operative time was an independent risk factor for postoperative SIRS [31]. Underweight children were particularly vulnerable to the inflammatory effects of longer procedures, supporting the notion that host biological characteristics can significantly influence the systemic inflammatory response to PCNL.
Recognizing that males and females may differ in their susceptibility and response to surgical stress highlights the need for personalized strategies that consider sex-specific risk profiles. Such an approach could optimize patient outcomes by guiding surgical planning, perioperative care, and postoperative monitoring. For example, in female patients, particular attention should be given to minimizing operative time; therefore, establishing operative time limits and utilizing instruments or techniques that expedite the procedure may be beneficial [18, 23, 24].
Our study has several strengths. It is innovative since it is the first to assess risk factors for infectious complications, stratified by gender, in a relatively large, homogeneous cohort of patients undergoing PCNL for kidney stones. Moreover, our results are relevant and with a strong clinical application, as they revealed that females are at higher risk of infectious complications than males. This study also highlights that commonly recognized predictors of infection in clinical practice should be interpreted with consideration of patient gender to more accurately assess the risk of infectious complications following PCNL. As a pilot study, it provides valuable preliminary evidence and establishes a foundation for future prospective cohort studies aimed at further exploring gender-specific differences in this context.
However, our study is not devoid of limitations. Larger multi-center studies are needed to externally validate our results. The retrospective nature of our study, spanning a 9-year period during which surgical techniques, instrumentation, and perioperative management evolved, may have influenced patient outcomes. Additional limitations include the single-center setting, which may affect the generalizability of the findings, and the lack of assessment of sex hormone levels, which could provide deeper insights into the biological mechanisms underlying gender differences in postoperative infection risk. Lastly, we lacked precise data about resistance pattern of each positive urine culture that could be of clinical relevance to increase the understanding of the post-op infectious cascade.
Conclusion
Female patients were at higher risk of post-PCNL infections than males. Infections in females were mainly associated with preoperative BUC, operative time, and stone-free status, whereas in males, preoperative BUC and residual stones were key factors. Notably, females developed infections at lower stone volumes and shorter operative times, highlighting the need for a gender-tailored approach to optimize outcomes and reduce postoperative infections.