Epidemiological and Economic Factors in Facelift Surgery in the USA: A Retrospective Multi-center Analysis
Leonard Knoedler, Alexandre G. Lellouch, Raffaele Aguglia, Kevin Sadati, Samuel Knoedler, Andreas Kehrer, Curtis L. Cetrulo, Carsten Rendenbach, Max Heiland, Jakob Fenske

TL;DR
This study analyzes trends in facelift surgeries in the USA, highlighting demographic patterns, economic factors, and regional disparities.
Contribution
The paper provides a comprehensive retrospective multi-center analysis of facelift surgery epidemiology and economics using national inpatient data.
Findings
Facelift patients were predominantly female, White, and self-paying with high-income status.
Minimally invasive procedures were more common among higher-income individuals.
Facial feminization was an indication in 12.3% of cases, showing a growing trend.
Abstract
The demand for surgical facial rejuvenation procedures, such as facelifts, has risen in recent decades. However, limited research has addressed the epidemiological and economic aspects of these procedures. This study examines trends in facelift surgeries using data from the Healthcare Cost and Utilization Project (HCUP) National Inpatient Sample (NIS) database. The HCUP-NIS database, which includes all-payer inpatient cases in the USA, was analyzed for facelift procedures identified through ICD-10 codes from 2016 to 2020. A total of 723 patients met the inclusion criteria. Patient demographics, hospitalization details, and procedural characteristics were evaluated using descriptive statistics. Exploratory comparisons were made across the three surgical technique subgroups, as allocated in ICD-10 procedural coding: open, percutaneous, and percutaneous endoscopic. The cohort included…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
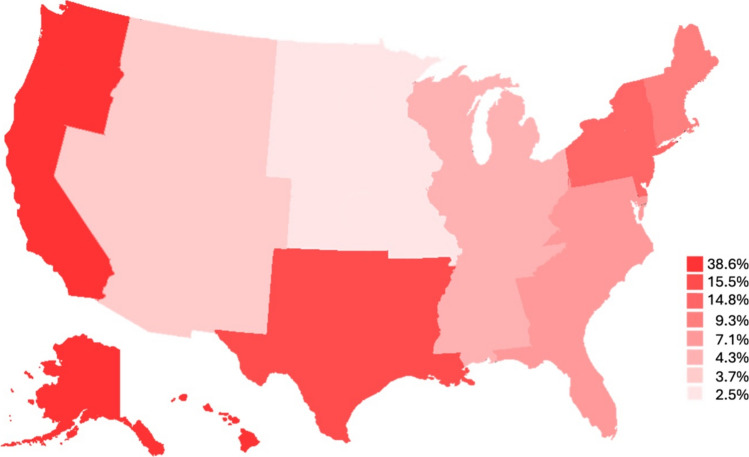 Figure 1
Figure 1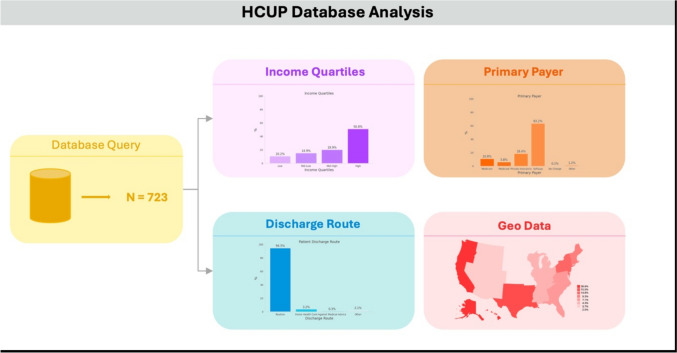 Figure 2
Figure 2- —Charité - Universitätsmedizin Berlin (3093)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFacial Rejuvenation and Surgery Techniques · Body Image and Dysmorphia Studies · Dermatologic Treatments and Research
Introduction
Surgical facial rejuvenation procedures, including facelift surgeries, represent a significant sector within the field of cosmetic and reconstructive surgery. Over the past several decades, the demand for these procedures has risen due to various factors, including aging population demographics, advancements in surgical techniques, and evolving societal perceptions of esthetics [1–5]. Understanding the epidemiological trends and economic implications of these procedures is essential for facial surgeons, healthcare policymakers and hospital administrators in optimizing resource allocation and patient care strategies [6]. While facelift procedures are commonly performed in outpatient practice settings, little is known for inpatient hospital procedures. In fact, a recent analysis found that 18% of facelifts are performed in a hospital setting with an increasing trend, underlining its impact on health care [7].
The Healthcare Cost and Utilization Project (HCUP) National Inpatient Sample (NIS) provides a comprehensive database that captures nationwide inpatient healthcare data, offering insights into the utilization, demographics and financial burdens associated with facial rejuvenation procedures. Besides individual factors such as concerns regarding an unnatural outcome or fear of anesthesia, economic considerations play a pivotal role in the accessibility and feasibility of elective cosmetic procedures [8]. The financial burden of facelifts varies widely depending on hospital setting, insurance coverage, surgical technique and associated comorbidities [9–11]. Additionally, evolving reimbursement policies and technological advancements may contribute to shifting cost structures [12, 13].
While previous studies identified risk factors, such as obesity, and determined complication rates in facelift surgery [14–17], there is a paucity of research on epidemiological and health economic aspects for these procedures, as well as limited data on patients undergoing facelifts in a hospital setting. This study aims to analyze the HCUP-NIS database to evaluate trends in inpatient surgical facelift procedures, with a particular focus on patient demographics, procedural approaches, hospital characteristics and associated costs. By leveraging this dataset, we seek to identify patterns related to age, gender, ethnic and socioeconomic disparities, regional variations and shifts in hospital-based surgical trends over time.
Materials and Methods
Data Source and Patient Selection
Data were obtained from the Agency for Healthcare Research and Quality (AHRQ) HCUP-NIS database, which provides detailed records and accompanying clinical data of all-payer inpatient cases in the USA. Following consultation with the Institutional Review Board (IRB), it was determined that this study does not require IRB review, as it uses de-identified data that are publicly accessible (Cedars-Sinai Medical Center, CA, USA). The HCUP-NIS database was queried to identify all patients undergoing facial alteration surgery in an inpatient setting dating back to 2016 after the introduction International Statistical Classification of Diseases and Related Health Problems version 10 (ICD-10), as the previous versions did not capture facelift procedures. Specific ICD-10 procedure codes were applied to extract patient cases: 0W020ZZ (Alteration of Face, Open Approach), 0W023ZZ (Alteration of Face, Percutaneous Approach) and 0W024ZZ (Alteration of Face, Percutaneous Endoscopic Approach). In total, 723 patients were identified as eligible candidates for analysis.
Variable Extraction
For all eligible patient cases, epidemiological as well as hospital and procedural data were extracted. In detail, the following parameters were investigated: (a) demographic variables (gender, age, ethnicity, income quartile, primary payer/insurance, patient residence), (b) hospitalization parameters (length of stay, total costs, patient discharge route, hospital location) and (c) ICD-10 coded procedural characteristics (main face alteration procedure, number of total procedures, coded comorbidities, indications). Yearly income quartiles (Q1-Q4) are newly defined for each year in HCUP-NIS with the following value ranges from 2016 to 2020: <49,999 for Q1, 50,000 to 64,999 for Q2, 65,000 to 85,999 for Q3 and ≥86,000 for Q4.
Statistical Analysis
Data were collected, stored and managed using spreadsheet software (Microsoft Excel Version 16.56, Microsoft Corp., Redmond, WA, USA). Analyses were conducted using RStudio (Version 2024.09.0+375). First, parameters were descriptively analyzed for all eligible candidates reporting frequencies, means and standard deviations as well as medians and interquartile range where suitable. Subsequently, parameters were exploratively compared between three procedural subgroups, as allocated in the ICD-10 procedural coding: open, percutaneous and percutaneous endoscopic approach. In detail, Chi-square test was used for qualitative values and Kruskal–Wallis-test for quantitative variables.
Results
Patient Demographics
In total, 723 candidates with an average age of 56.7 ± 16.2 years received surgical procedures between 2016 and 2020, consisting of more females (n=574; 79.4%). Most candidates were Whites (n=585; 81%), self-paying for the procedure (n=457; 63.2%) and with mostly high income (n=367; 50.8%). Most patients resided in central counties in metro areas of ≥1 million inhabitants (n=313; 43.3%).
In exploratory subgroup comparison, statistically significant differences were found between the subgroup regarding income quartiles (p=0.037) with open approaches exhibiting lower rates in the high-income quartile (49.4% vs. 76.2% vs. 64.3%) and higher rates in the low-income quartile (10.8% vs. 4.8% vs. 0.0%) compared to percutaneous or percutaneous endoscopic approaches.
Hospitalization Parameters
Patients were hospitalized for a mean of 1.7 ± 1.6 days, causing total costs of 63,152.80. Most patients were discharged in routine route (n=683; 94.5%), defined as discharge to home or self-care, with most procedures occurring in the pacific region (n=279; 38.6%) (Figure 1). No significant differences were found in subgroup analysis.Fig. 1. Geographical distribution of hospitals with color-coded procedure frequency. More intense colors represent higher frequencies
Procedural Characteristics
The most common indication was plastic surgery due to cosmetic reasons. Facelift was also performed for gender dysphoria indications in 12.3% of the cases.
The five most common comorbidities were arterial hypertension (18.8%), history of nicotine abuse (13.7%), hyperlipidemia (11.5%), anxiety disorder (10.7%), and gastroesophageal reflux disease (10.4%). Patients presented with a mean of 5.7 ± 4.7 comorbidities and underwent 5.2 ± 3.0 total ICD-10 coded procedures. No significant differences were found in subgroup analysis.
Table 1 details data for the total cohort, while results of the subgroup analysis are displayed in Table 2. Table 1. Epidemiological, hospitalization and comorbidity data for the total cohortEpidemiological DataVariableTotal Cohort (N=723)Age [years ± SD]56.7 ± 16.2Female574 (79.4%)EthnicityWhite585 (80.9%)Black24 (3.3%)Hispanic45 (6.2%)Asian or Pacific23 (3.2%)Native American2 (0.3%)Other28 (3.9%)Unknown16 (22.1%)Income quartileLow (Q1)74 (10.2%)Mid-low (Q2)108 (14.9%)Mid-high (Q3)144 (19.9%)High (Q4)367 (50.8%)Unknown30 (4.1%)Primary Payer/InsuranceMedicare78 (10.8%)Medicaid42 (5.8%)Private insurance133 (18.4%)Self-pay457 (63.2%)No charge1 (0.1%)Other9 (1.2%)Unknown3 (0.4%)Patient LocationCentral counties in metro areas of ≥1 million population313 (43.3%)Fringe counties in metro areas of ≥1 million population209 (28.9%)Counties in metro areas of 250,000-99,999 population91 (12.6%)Counties in metro areas of 50,000-249,999 population45 (6.2%)Micropolitan counties32 (4.4%)Not metropolitan or micropolitan counties19 (2.6%)Unknown14 (1.9%)Hospitalization DataVariableTotal Cohort (N=723)Length of stay [days ± SD]1.7 ± 1.6Number of total ICD-10 procedures [mean ± SD]5.2 ± 3.0Total costs [US-Dollar ± SD]63,152.80Patient dischargeRoutine683 (94.5%)Home health care23 (3.2%)Against medical advice2 (0.3%)Other15 (2.1%)Hospital LocationNew England67 (9.3%)Middle Atlantic107 (14.8%)East North Central31 (4.3%)West North Central18 (2.5%)South Atlantic51 (7.1%)East South Central31 (4.3%)West South Central112 (15.5%)Mountain27 (3.7%)Pacific279 (38.6%)ComorbiditiesNumber of comorbidities [mean ± SD]5.7 ± 4.7SD Standard deviationTable 2Epidemiological, hospitalization and comorbidity data for surgical approach subgroupsEpidemiological DataVariableOpen Approach(n=674)Percutaneous Approach(n=21)Percutaneous Endoscopic Approach(n=28)pAge [years ± SD]56.4 ± 16.560.6 ± 14.060.1 ± 10.60.450Female530 (78.6%)18 (85.7%)26 (92.9%)0.164Ethnicity0.501White538 (79.8%)21 (100.0%)26 (92.9%)Black23 (3.4%)0 (0.0%)1 (3.6%)Hispanic45 (6.7%)0 (0.0%)0 (0.0%)Asian or Pacific23 (3.4%)0 (0.0%)0 (0.0%)Native American2 (0.3%)0 (0.0%)0 (0.0%)Other28 (4.2%)0 (0.0%)0 (0.0%)Unknown15 (2.2%)0 (0.0%)1 (3.6%)Income quartile0.037Low (Q1)73 (10.8%)1 (4.8%)0 (0.0%)Mid-low (Q2)99 (14.7%)3 (14.3%)6 (21.4%)Mid-high (Q3)141(20.9%)1 (4.8%)2 (7.2%)High (Q4)333 (49.4%)16 (76.2%)18 (64.3%)Unknown28 (4.2%)0 (0.0%)2 (7.2%)Primary Payer/Insurance0.559Medicare76 (11.3%)1 (4.8%)1 (3.6%)Medicaid40 (5.9%)1 (4.8%)1 (3.6%)Private insurance126 (18.7%)1 (4.8%)6 (21.4%)Self-pay420 (62.3%)17 (76.2%)20 (71.4%)No charge1 (0.2%)0 (0.0%)0 (0.0%)Other8 (1.2%)1 (4.8%)0 (0.0%)Unknown3 (0.5%)0 (0.0%)0 (0.0%)Patient Location0.587Central counties in metro areas of ≥1 million population291 (43.2%)8 (38.1%)16 (57.1%)Fringe counties in metro areas of ≥1 million population194 (28.8%)9 (24.9%)5 (17.9%)Counties in metro areas of 250,000-99,999 population84 (12.5%)2 (9.5%)5 (17.9%)Counties in metro areas of 50,000-249,999 population43 (6.4%)1 (4.8%)0 (0.0%)Micropolitan counties32 (4.8%)0 (0.0%)0 (0.0%)Not metropolitan or micropolitan counties16 (2.4%)1 (4.8%)2 (7.2%)Unknown14 (2.1%)0 (0.0%)0 (0.0%)Hospitalization DataVariableOpen Approach(n=674)Percutaneous Approach(n=21)Percutaneous Endoscopic Approach(n=28)pLength of stay [days ± SD]1.8 ± 1.71.1 ± 0.31.3 ± 0.70.060Number of total ICD-10 procedures [mean ± SD]5.2 ± 3.04.5 ± 2.25.8 ± 2.90.220Total costs [US-Dollar ± SD]63,397.0180,036,5240,280.760.713Patient discharge0.799Routine634 (94.1%)21 (100.0%)23 (100.0%)Home health care23 (3.4%)0 (0.0%)0 (0.0%)Against medical advice2 (0.3%)0 (0.0%)0 (0.0%)Other15 (2.2%)0 (0.0%)0 (0.0%)Hospital Location0.129New England67 (9.9%)0 (0.0%)0 (0.0%)Middle Atlantic100 (14.8%)3 (14.3%)4 (14.3%)East North Central30 (4.5%)0 (0.0%)1 (3.6%)West North Central15 (2.2%)2 (9.5%)1 (3.6%)South Atlantic49 (7.3%)2 (9.5%)0 (0.0%)East South Central30 (4.5%)0 (0.0%)1 (3.6%)West South Central103 (15.3%)4 (19.1%)5 (17.9%)Mountain22 (3.3%)3 (14.3%)2 (7.2%)Pacific258 (38.3%)7 (33.3%)14 (50%)ComorbiditiesNumber of comorbidities [mean ± SD]5.8 ± 4.85.1 ± 4.05.8 ± 4.50.830SD Standard deviation
Discussion
Facelift surgery has long been a hallmark of esthetic medicine, with its utilization shaped by geographical, socioeconomic and medical factors, as well as contemporary trends and techniques. This retrospective multi-center analysis reveals significant disparities in access, patient demographics, and indications, focusing on inpatient surgeries, a cohort with increasing prevalence [7]. By analyzing data from the HCUP-NIS database, we provide a comprehensive epidemiological and economic overview of inpatient facelift procedures in the USA, offering insights for clinicians, healthcare policymakers, and researchers.
The analysis of the geographical distribution revealed a concentration of facelift procedures in the Pacific region, which accounted for nearly 40% of all cases. This regional clustering may reflect varying social attitudes toward cosmetic surgery, with coastal metropolitan areas demonstrating higher demand for esthetic procedures [18]. Cultural influences, media representation, and higher disposable income in these regions likely contribute to increased procedural rates [19, 20]. Additionally, regional variations in the availability of skilled surgeons and specialized healthcare facilities may further impact the distribution of facelift surgeries[21]. Conversely, rural and less densely populated regions exhibited lower facelift rates, which may be attributed to limited access to specialized surgical centers, reduced awareness, and differing socioeconomic priorities [20, 22]. Future research should explore the potential impact of telemedicine and digital consultations in bridging this urban-rural divide by facilitating patient education and preoperative planning.
Our data confirm long-standing demographic trends in facelift surgery, with most patients being middle-aged to older White females. The average age of 56.7 years aligns with previous studies indicating that facelifts are predominantly sought by individuals experiencing visible signs of facial aging, such as skin laxity and volume loss [23, 24]. Women represented nearly 80% of the cohort, underscoring the historical association between cosmetic surgery and femininity [25]. While societal expectations and gender norms likely influence this trend, increasing acceptance of cosmetic procedures among men may shift demographic patterns in the future [26]. Moreover, this study exclusively focused on facelift surgeries performed in an inpatient setting. Although commonly performed in private practices in an outpatient setting, Stein et al. found that 18% (n=608) of surgeries were performed in hospital, with 212 requiring inpatient setting [7]. Both even showed an increased trend from 2015 to 2021 compared to 2006–2014. A possible explanation for a required inpatient setting could be an increased number of comorbidities requiring extensive perioperative surveillance. In fact, patients in this cohort presented with 5.7 ± 4.7 comorbidities, thereby exceeding numbers reported for the general American public, which further underscores this assumption [27].
Facelift surgery remains an elective procedure with significant financial implications, as evidenced by the high mean total hospitalization cost of $85,259.60. Notably, 63.2% of patients self-paid for their procedures, reinforcing the perception of facelifts as a luxury rather than a medical necessity [28]. This finding is particularly relevant considering the increasing rates of medical tourism to countries such as the Dominican Republic or Colombia due to rising costs [29]. Our findings highlight a pronounced socioeconomic disparity, with patients from higher-income quartiles being overrepresented. Interestingly, subgroup analysis revealed that open facelift approaches were more frequently performed in lower-income individuals, while minimally invasive techniques were more common among higher-income patients. Although exploratory, this discrepancy may reflect differences in healthcare access, insurance coverage, or surgeon preference, as well as required extensive training leading to increased costs for highly technical procedures such as the deep plane facelift [30]. Furthermore, high procedural costs may disproportionately deter economically disadvantaged populations, perpetuating an inequitable distribution of esthetic care [10]. Although there are less invasive and expensive techniques, such as radiofrequency and ultrasound methods or the thread lift, aiming to delay the need for facelifts, these methods often struggle to treat the jowls and neck. Minimally invasive procedures can be effective for patients in their 30 s and 40 s by providing temporary skin tightening and contour enhancement. However, in patients over 50, these interventions may become counterproductive, as repeated treatments can lead to tissue fibrosis, compromised vascular supply, and deep scarring. The presence of fibrotic adhesions and altered soft tissue planes can make surgical dissection more challenging, potentially limiting the ability to achieve optimal repositioning of the SMAS and deep facial structures. Thus, they can only be partially regarded as effective alternative for low-income patients. Exploring financing options, insurance policies, and cost reduction strategies may be critical in improving access to facelift procedures for a broader patient demographic.
Traditionally, cosmetic motivations have dominated facelift indications, and our study confirms that nearly 41% of procedures were performed for esthetic reasons. However, an emerging trend is the increasing utilization of facelift techniques in facial feminization surgeries, accounting for over 12% of cases. As societal recognition of gender diversity grows, so does the demand for procedures that align an individual’s physical appearance with their gender identity [5, 31, 32]. Facial feminization facelifts may involve modifications to facial contours, jawlines, and soft tissue structures to enhance gender congruence [33]. This finding emphasizes the evolving role of facelift surgery beyond traditional rejuvenation, encompassing reconstructive and identity-affirming dimensions. Further research is warranted to assess the long-term outcomes, patient satisfaction and psychological benefits of facelift procedures in transgender and non-binary individuals.
Overall, our findings highlight the evolving landscape of inpatient facelift surgery, shaped by geographical, socioeconomic, social media [34] and medical factors, underscoring the need for continued research and policy considerations to ensure equitable access and optimal patient outcomes.
Limitations
Several limitations must be acknowledged. First, the reliance on the HCUP-NIS database, while comprehensive, is restricted to inpatient procedures, potentially omitting outpatient and ambulatory facelift surgeries that may constitute a substantial proportion of cases. This limitation may skew findings toward more complex or medically necessary procedures rather than purely elective cosmetic surgeries. Moreover, specific coding incongruencies cannot be ruled out as common for studies employing multi-center, de-identified databases. Second, the database lacks in-depth details on surgical techniques, surgeon expertise and postoperative outcomes, limiting the ability to evaluate procedure-specific complications or success rates. There is a body of evidence that highlights the influence of different surgical techniques on postoperative outcomes and complications (35). Additionally, subgroup comparisons were exploratory, and statistical significance in some comparisons may be influenced by sample size constraints. Future prospective studies with more detailed patient and procedural data are necessary to validate and expand upon the presented findings. Moreover, procedures due to cosmetic and facial feminization indications may overlap, potentially leading to partial misclassification. Lastly, the lack of longitudinal follow-up prevents the assessment of long-term economic and clinical impacts, including revisions, complications, or patient-reported satisfaction. Integrating patient-reported outcomes and qualitative assessments in future research could provide a more holistic understanding of facelift surgery’s benefits and limitations. Of note, the recent HCUP-NIS database is structured by US ICD-10, including ICD-10-CM for diagnoses and ICD-10-PCS for procedures, which may differ from ICD-10 coding for other healthcare systems.
Conclusion
Inpatient facelift surgery is influenced by complex epidemiological and economic factors, with significant regional and socioeconomic disparities shaping patient access and procedural trends. Our analysis underscores the growing role of facial feminization procedures and highlights economic and geographic barriers that may limit equitable distribution. As technological advancements and social attitudes evolve, further research is warranted to assess long-term outcomes and the changing demographic landscape of inpatient facelift surgery.
The reference list from the paper itself. Each links out to its DOI / PubMed record.