Return to sport after arthroscopic rotator cuff repair: epidemiology and prognostic factors in a Swiss multicentre cohort
Madlaina Matter, Laurent Audigé, Thomas Stojanov, Andreas Mueller, Matthias A Zumstein, Annabel Hayoz, Michael Schär, Claudio Rosso, Philipp Moroder, Doruk Akgün, Isabella Weiss, Eduardo Samaniego, Thomas Suter, Sebastian A Müller, Markus Saner, Claudia Haag-Schumacher

TL;DR
This study examines how many patients return to sports after rotator cuff surgery and identifies factors that help predict successful recovery.
Contribution
The study provides new insights into prognostic factors for returning to sports after arthroscopic rotator cuff repair.
Findings
Over half of patients achieved full return to sports within 24 months after surgery.
Traumatic injury, high motivation, and higher sports activity levels were linked to better outcomes.
Delayed passive mobilisation was associated with incomplete return to sports.
Abstract
To investigate patients’ sports activities prior to and after arthroscopic rotator cuff repair (ARCR) and to better understand the relationship between patient, injury and sport-specific factors and return to sport (RTS) after ARCR. As a part of the ARCR_Pred multicentre cohort study, patients from 19 centres undergoing primary ARCR for partial or complete rotator cuff tears between June 2020 and November 2021 were prospectively enrolled. Only patients who participated in sports prior to the injury were included. Injury characteristics, sports activity, sociodemographic, psychological and rehabilitation-specific factors, including the ability to return to any sport, were recorded preoperatively and postoperatively at 6 weeks, 6, 12 and 24 months. Prognostic factors for full RTS were identified using univariable and multivariable logistic regression analysis. Of the 725 eligible…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
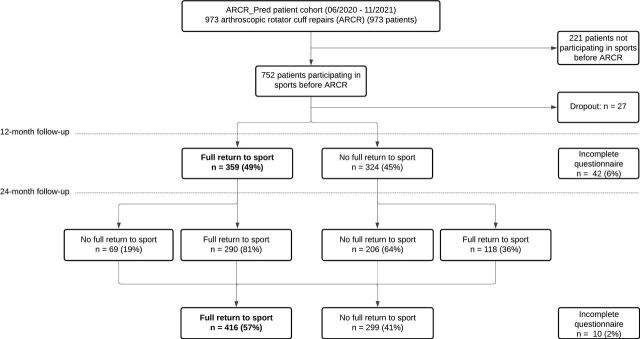 Figure 1
Figure 1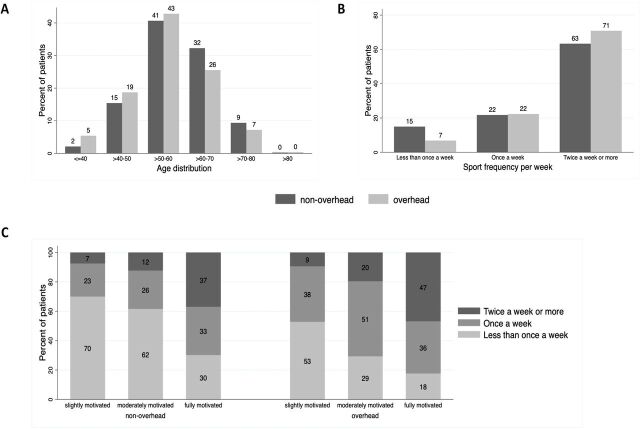 Figure 2
Figure 2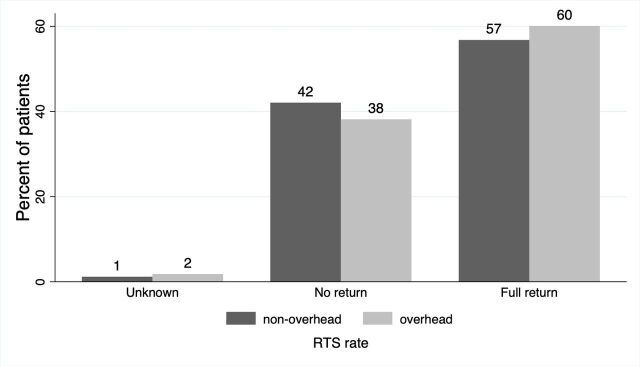 Figure 3
Figure 3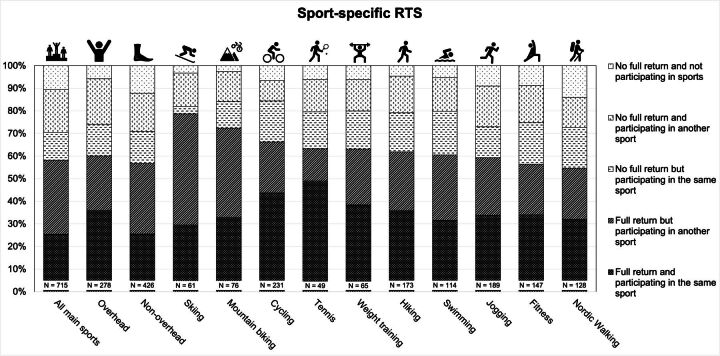 Figure 4
Figure 4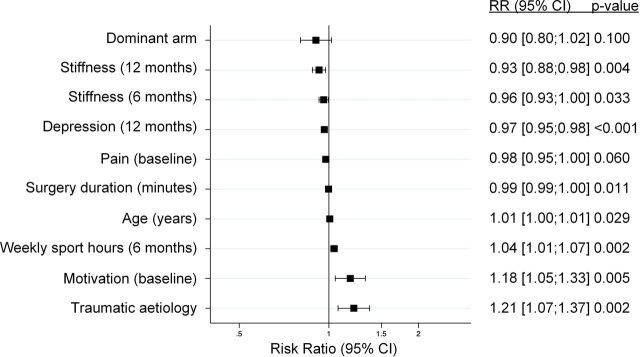 Figure 5
Figure 5| Parameter | Non-overhead (n=428) | Overhead (n=278) | |||||
| N (%) | Mean (SD) | N (%) | Mean (SD) | Standardised mean difference | Mean difference (95% CI) | P value | |
| Age at surgery (years) | 59 (9) | 56 (10) | 0.283 | −3 (−4 to −1) | <0.001 | ||
| Sex | |||||||
|
Female | 149 (35) | 116 (42) | 0.143 | 0.064 | |||
| BMI | 27 (4) | 26 (5) | 0.061 | −0 (−1 to 0) | 0.427 | ||
| ASA classification | |||||||
|
I | 186 (43) | 142 (51) | 0.153 | 0.139 | |||
| Surgery on the dominant arm | |||||||
|
No | 121 (28) | 80 (29) | 0.011 | 0.884 | |||
| Tear aetiology | |||||||
|
Degenerative | 198 (46) | 124 (45) | 0.033 | 0.666 | |||
| Tear severity (Gerber | |||||||
| Partial tear | 64 (15) | 40 (14) | 0.101 | 0.631 | |||
| Pain level NRS (0–10) | 5.4 (2.3) | 5.1 (2.2) | 0.149 | −0.3 (−0.7 to 0) | 0.054 | ||
| Sport frequency | |||||||
|
Less than once a week | 64 (15) | 19 (7) | 0.265 | 0.004 | |||
| Weekly hours of sport | 4 (2) | 4 (2) | 0.191 | 0 (0 to 1) | 0.014 | ||
| Motivation to return to sport after surgery | 10 (1) | 10 (1) | 0.030 | −0 (−0 to −0) | 0.695 | ||
| Confidence to resume sport at 100% of the capacity before the injury | 9 (2) | 9 (2) | 0.153 | 0.046 | |||
| PROMIS depression T score | 51 (8) | 51 (8) | 0.002 | 0 (−1 to 1) | 0.979 | ||
| PROMIS anxiety T score | 49 (9) | 49 (8) | 0.022 | −0 (−1 to 1) | 0.779 | ||
- —http://dx.doi.org/10.13039/501100007291SUVA
- —Swiss National Science Foundation
- —University Clinic Balgrist, Zurich, Switzerland
- —Endoclinic, Zurich, Switzerland
- —http://dx.doi.org/10.13039/100018402Schweizerische Gesellschaft für Orthopädie und Traumotologie
- —Inselspital, Bern, Switzerland
- —Hospital Solothurn, Solothurn, Switzerland
- —Charité Medicine University, Berlin, Germany
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsShoulder Injury and Treatment · Sports injuries and prevention · Shoulder and Clavicle Injuries
Introduction
Return to sport (RTS) is a key expectation for patients undergoing elective arthroscopic rotator cuff repair (ARCR).1 Various factors such as a higher preoperative sports activity level,2 fear of reinjury,3 participation in overhead and contact sports,4 or specific sports like baseball5 have been reported to impede a successful return to the patient’s previous sports activity level. RTS is a multifactorial process in which an athletically active patient advances from general rehabilitation activities to sport-specific movements following an injury.6 This progression depends on variables including training intensity, playing position, sport-specific biomechanics7 and psychological health and motivation.8 Notably, there is no consensus definition of the term RTS in the literature,9 with most studies relying on the patient’s subjective perception, primarily assessed using questionnaires.10–14
Previous studies analysing the outcome of RTS have focused on a narrow subgroup of patients (eg, only female tennis players,15 swimmers,16 partial tears,17 patients under 4518 or over 7019 years of age) and are therefore not generalisable. To our knowledge, limited epidemiological data and sports activity levels in a large population of patients with rotator cuff tear (RCT) have been described to date. In 2020, a Swiss-wide multicentre study for evaluation and prediction of core outcomes in ARCR (ARCR_Pred) was initiated.20 This study included sports activity levels. Grouping patients based on their RTS outcomes enables the assessment of not only functional recovery, but also outcomes within the complex context of sports participation. This approach could help identify patients who may face greater challenges in returning to their original performance level, allowing for individualised recommendations for those needing additional support during rehabilitation.
The aims of this study were, first, to describe the sports activity levels and epidemiological data of patients undergoing arthroscopic surgical treatment for partial-thickness or full-thickness RCT; second, to determine their return-to-sport rates and to investigate prognostic factors for full RTS. We hypothesised that (1) patients who participate in overhead sports will have more difficulties in returning to the same sport and (2) patients who are more active prior to surgery will more likely RTS.
Methods
Items included in the present manuscript are reported according to the Strengthening the Reporting of Observational Studies in Epidemiology21 guidelines for cohort studies. No patient or public member was involved in the study design.
Equity, diversity and inclusion statement
Our study included a diverse cohort of patients who underwent ARCR, with no exclusion criteria in terms of age, gender or socioeconomic background. The author group comprised two women and four men with different professional backgrounds and levels of training. All surgeries were performed in clinics in Switzerland or Germany (ie, in wealthier countries), which is why patients from regions with limited access to medical care may not be represented. The influence of age, gender and body mass index on RTS is discussed. However, we did not consider ethnicity, race or socioeconomic status in our analysis.
ARCR_Pred study setting
Between June 2020 and November 2021, 973 patients undergoing primary ARCR were enrolled across 18 Swiss and 1 German orthopaedic centres and follow-up assessments were conducted up to 24 months postoperatively.22 Functional and structural outcomes, as well as patient-reported outcome measures and adverse events (AEs), were recorded. A detailed overview of all measures taken is provided in online esupplemental table 1.
10.1136/bjsports-2025-110358.supp1Supplementary data
Baseline documentation included patient demographics, psychological and clinical factors, RCT integrity (ultrasound examination at 12 months by radiologists with musculoskeletal specialty training, experienced rheumatologists or orthopaedic surgeons), concomitant local findings, assessment of the tear aetiology and RCT severity (partial tear | single full-thickness tear | involvement of two or three tendons (one full thickness, the rest partial) | massive tear) by the treating surgeon, surgical details and postoperative management factors. At 6 weeks, the duration of immobilisation, timing of passive and active mobilisation, and type of physiotherapy were recorded. Clinical follow-up at baseline, 6 and 12 months postoperatively included assessment of shoulder pain (patient’s highest pain level experienced in the affected shoulder during ordinary activities within the last 24 hours, documented on a Numerical Rating Scale (NRS) from 0 to 10, maximum pain), range of motion (ROM) (active shoulder flexion, abduction, external rotation at 0° abduction, internal rotation with the Apley’s test) and strength (mean strength in 90° abduction, measured in kg with a handheld dynamometer). Patient-reported questionnaires at baseline, 6, 12 and 24 months postoperatively assessed functional scores, anxiety and depression scores, and participation in sports.
All patients enrolled in the ARCR_Pred study were eligible for inclusion without further exclusion criteria. Patients with previous surgeries, a history of ipsilateral fractures or dislocations of the affected shoulder (n=19) were not excluded.22 However, for the assessment of RTS, only patients who reported participation in sport activities at baseline were included.
Sports activities and overhead classification
At baseline, patients indicated via questionnaire whether they regularly participated in sport activities prior to their RCT. At 6, 12 and 24 months postoperatively, the patients were asked whether they were currently participating in sports. The response options were never, less than once a week, once a week or two times a week or more. Patients also indicated the number of hours spent per week on sports activities. Participants could specify up to three different sports (the most, second most and third most important) that they were currently engaged in. Sports could be selected from a predefined drop-down list with 44 sports, based on the classification system of the Swiss Office of Statistics for the documentation of sports.23
Motivation and confidence in RTS at baseline were assessed using a NRS from 0 (not at all) to 10 (fully). The same scale was used to assess motivation to participate in sports at 6, 12 and 24 months. All reported sports were classified as either overhead (eg, swimming, tennis, gymnastics) or non-overhead (eg, cycling, jogging, hiking) based on the most common type of movement, following consensus among the authors. If at least one of the sports specified by the patient at baseline was categorised as an overhead sport, the patient was classified as an overhead-sport patient.
Return to sport
RTS was defined based on a self-reported assessment provided in the patient questionnaire. At 12 and 24 months postoperatively, patients reported on a NRS from 0 to 10 how close they felt to returning to 100% of their original sport performance. Responses were dichotomised into ‘no full return’ (NRS values 0–8) and ‘full return’ (NRS values 9–10). If patients reported participating in sports at baseline but were not engaging in sports activities at 12 or 24 months, patients were classified as ‘no full return’.
RTS was primarily defined as a composite outcome based on the 24-month questionnaire value. If the 24-month questionnaire was not available (n=37), the value of the 12-month questionnaire was used. In addition, we documented whether patients were able to return to the same type of sport as reported at baseline.
Studied risk factors
In addition to sports activity parameters (frequency, quantity, sport, motivation and confidence) at baseline and at 6 months, a set of potential risk factors available in the ARCR_Pred study was investigated for associations with RTS. These included patient sociodemographic characteristics, surgical and injury-related factors, parameters related to the rehabilitation procedure, preoperative and postoperative scores up to 12 months and complications. Scores included: pain level, the Constant-Murley Score,24 abduction strength, a Shoulder Stiffness Scale (SSS) and psychological Patient Reported Outcomes Measurement Information System (PROMIS) depression and anxiety T-scores (calculated with the HealthMeasures PROMIS Scoring Manuals).25 26 The SSS is a monitoring tool for postoperative shoulder stiffness and ranges from 0 to 10 points (maximum stiffness). It is calculated from the parameters pain (sss1: 0–3 points), subjective ROM limitation in daily activities (sss2: 0–3 points), as well as side-to-side difference in passive external rotation in adduction and glenohumeral abduction (sss3: 0–4 points). Complications included events involving the operated shoulder, such as stiffness events within 6 months requiring treatment, and ipsilateral AEs within 12 and 24 months.
Data management and statistical analysis methods
Study data were managed using the REDCap Electronic Data Capture system27 and exported for variable transformation (including score calculations) and statistical analysis using Stata V.17 (StataCorp LP, College Station, Texas, USA).
Sports activities and baseline characteristics
Demographic characteristics, health status, intraoperative findings, sports activity levels and clinical shoulder parameters at baseline were analysed using descriptive statistics (mean and SD; frequency and percentages, as appropriate). Overhead and non-overhead sports patient groups were compared in terms of baseline characteristics using standardised mean differences (Std. Diff.).
Risk factors for RTS
An initial list of 36 candidate predictors for RTS was identified using expert-based knowledge from clinicians involved as a coauthor in the present study (AM, MAZ and MS). A univariable Poisson regression analysis was conducted to investigate the association (risk ratio (RR) and corresponding 95% CIs) between the aforementioned factors and the outcome of ‘full RTS’.28 For continuous and ordinal variables, we assessed non-linearity trends in univariable models using splines with one knot. The percentage of missing values for specific variables ranged from 0 to 14.8%. The proportion of patients with at least one missing predictor was 10%. Assuming that these missing values were missing at random, multiple imputation was performed using chained equations29 with 20 data sets. Missing values were imputed for risk factors only, not for the outcome ‘full RTS’.
To examine the associations between multiple factors simultaneously and the RTS outcome, a multivariable Poisson regression analysis was performed. Given a fixed sample size (n=725), outcome prevalence of 42.6% and an anticipated c-statistic of 0.7 based on previous findings,30 we decided to restrict the model to a maximum of 10 factors (using the Stata package pmsampsize, following recommendations by Riley et al 31). The relationship between any factor pairs was analysed using correlation coefficient for continuous variables, χ² test for categorical variables (after checking statistical assumptions) and Spearman’s rank correlation coefficient for comparison of a continuous with a categorical variable.32 When two variables described similar constructs, variables that would lead to less loss of information (eg, number of hours of sport was preferred over the categorised sports frequency) were kept. Similarly, when correlation was observed between two factors (correlation coefficient >0.3,32 p value of χ² test <0.05,33 Spearman’s rank correlation coefficient >0.3),32 only one of the variables was retained prior to the variable selection procedures. A final exploratory RTS model was identified using backward elimination as the variable selection strategy with an alpha level of 0.157.34 Variable selection was performed on the complete case data. Model performance was assessed using Akaike’s Information Criterion (AIC),35 the generalised index of concordance (c-index)36 and Pearson goodness-of-fit.36 In the last step, when there were signs of non-linearity between continuous and/or ordinal variables and the outcome, we assessed whether non-linearity terms contributed to an improvement of model performance.35 36
Results
Patient cohort selection
Of the 973 patients enrolled in the ARCR_Pred study, 752 (77.3%) were participating in sport at baseline. Of these, 27 patients were lost to follow-up before the 12-month follow-up, leaving 725 patients (74.5%) available for analysis (figure 1). Among these, 37.2% were female, and the mean age was 57.7 years (range: 21–84 years).
Patient flow chart and follow-up. This figure presents patient selection, follow-up and RTS rates. RTS, return to sport.
The severity of the RCT was classified intraoperatively as follows: 15.0% had a partial tear, 26.2% a single full-thickness tear, 15.5% involvement of two or three tendons (one full thickness, the rest partial) and 43.3% a massive tear. The tear was associated with a traumatic event in 54.2% of cases. The dominant shoulder was injured in 71.5% of ARCR cases.
Sport participation and comparison of baseline characteristics
Overall, the three most frequently reported sports were cycling (n=231), jogging/running (n=189) and hiking/mountaineering (n=173) (online esupplemental table 2). Of the cohort, 278 (38.3%) were classified as overhead-sport patients and 428 (59.0%) as non-overhead-sport patients (2.6% of patients did not specify their sport). The most practised overhead sports were swimming (n=114), weight training (n=65) and tennis (n=49).
10.1136/bjsports-2025-110358.supp2Supplementary data
Patients in the non-overhead-sport group were older on average (59 vs 56 years, Std. Diff.=0.283) and exercised fewer times per week than those in the overhead-sport group (figure 2A,B). Tear aetiology (Std. Diff.=0.033) and severity (Std. Diff.=0.101) were similar between the groups. The preoperative motivation to RTS (mean 10 (SD=2), Std. Diff.=0.030) and confidence to resume sport at 100% of their original capacity (mean 9 (SD=2), Std. Diff=1.53) was high in both groups. Patients who exercised at least two times a week prior to surgery were more motivated to RTS than those who exercised less than once a week (Std. Diff.=0.716, figure 2C). A detailed overview of all baseline characteristics is provided in table 1.
Distribution of baseline characteristics. (A and B) Show the distribution of age (A) and sport frequency per week (B) among patients participating in overhead versus non-overhead sports. (C) Compares sport frequency per week with motivation to return to sport, grouped by overhead versus non-overhead-sport participation.
Return to sport
At 12 months, 49.5% (359/725) of patients had already reached full RTS; by 24 months, this proportion increased to 57.4% (416/725). Overall, 60.1% (167/278) of patients in the overhead-sport group achieved full RTS within 24 months, compared with 56.8% (243/428) in the non-overhead-sport group (figure 3).
RTS rates per sport group. This figure shows a comparison of RTS rates between patients participating in overhead and non-overhead sports. RTS, return to sport.
Among patients who achieved full RTS within 24 months, 90.1% (375/416) returned to at least one sport they had practised before the injury.
A full RTS to the same main sport was observed in 43.8% (182/416). Among overhead-sport patients, 36.0% (100/278) returned to their original overhead sport. Among non-overhead sport patients, 25.6% (50/123) returned to their original non-overhead sport. A detailed overview of all individual sports and their RTS outcomes is presented in figure 4 and online esupplemental table 2.
Sport-specific RTS rates. This figure shows RTS rates for the 10 most practised sports. It also indicates whether patients were able to return to the same sport as they reported at baseline. As patients could list up to three different sports, some may be included in multiple categories. RTS, return to sport.
Risk factors for RTS
The analysis of 36 risk factors for RTS is summarised in online esupplemental table 3. At the univariable analysis level, several sociodemographic, surgical and injury-related factors showed a significant association with full RTS (p<0.05). These included, for example, dominance of the operated side (RR 0.87 (95% CI 0.76 to 0.99); p=0.031), age at surgery (RR 1.01 (95% CI 1.01 to 1.02); p<0.001) and traumatic injury (RR 1.20 (95% CI 1.06 to 1.37); p=0.005).
10.1136/bjsports-2025-110358.supp3Supplementary data
The time of onset of passive movements in weeks (RR 0.94 (95% CI 0.89 to 0.99); p=0.017), a higher baseline level of sports activity, all preoperative and postoperative scores and psychological factors at almost all follow-up points, particularly the motivation to RTS at baseline (RR 1.29, (95% CI 1.15 to 1.44), p<0.001), were significantly associated with full RTS. Practising an overhead sport (RR 1.06 (95% CI 0.94 to 1.21); p=0.325) was not significantly associated with RTS outcome.
From the initial list of 36 candidate predictors, 8 were dropped because of high correlation and redundant information. The final model resulting from the backward elimination procedure was composed of 10 factors (figure 5, online esupplemental table 4a). Inclusion of non-linear spline terms did not improve the performance of the final multivariable model. The model performance was AIC=1130.708, Pearson goodness-of-fit = 244.082 and c-index=0.762 (online esupplemental table 4b).
10.1136/bjsports-2025-110358.supp4Supplementary data
Multivariable logistic regression model. This figure shows the forest plot of the multivariable model including 10 factors. Squares represent the RR, and horizontal lines indicate 95% CIs of the specific factor. RR, risk ratio.
Discussion
We investigated the ability of patients in Switzerland to RTS after undergoing an ARCR. Overall, 57.4% were able to RTS following ARCR. While RTS rates did not differ between overhead and non-overhead sports, we observed variation at the level of individual sports. Patients were more likely to RTS in sports such as tennis and cycling, and less likely in swimming and skiing. We also only noted minor differences in baseline characteristics between patients participating in overhead versus non-overhead sports. Therefore, differences in RTS between these two sports groups may not be biased by confounding baseline conditions, aside from age and level of sports activity.
The baseline distributions of sports participation in our investigation were similar to those among the Swiss population in 2020 reported by the Swiss Federal Office for Sport.23 A direct comparison of RTS rates with the literature is challenging because the studies differ greatly in terms of patient selection, injury characteristics and definitions of RTS. Yet, meta-analyses have reported higher rates of return to the same or better level (65.9%2 and 70.2%,37 respectively). In our study, participation in a specific sport group such as overhead sports had no clear influence on RTS rates. Therefore, our first hypothesis was rejected. This finding may appear unexpected, given the high precision and function required of the shoulder in overhead sports,38 and contrasts with previous studies2 37 that identified participation in overhead sports as a potential negative predictor of RTS. A large part (90%) of patients returned to at least one sport that they had practised prior to injury, but only 25% returned to their primary sport. High RTS rates were achieved by patients participating in golf, tennis or cycling, consistent with findings from previous studies.39 40 Regardless of sport type, patients who exercised more frequently prior to surgery were associated with higher RTS rates, confirming our second hypothesis.
In the univariable analysis, early passive mobilisation was significantly associated with full RTS. The start of passive mobilisation is a balancing act between early functional activity to prevent stiffness and enhance shoulder mobility and impairing tendon healing.41 Its absence from the multivariable model may be due to the multiple interrelationships among the various risk factors assessed.42 The SSS itself showed a significant correlation with complete RTS both in the univariable analysis and multivariable model, suggesting its prognostic value in orthopaedic shoulder surgery. A shorter duration of surgery, also found to be a predictor in other studies,43 44 appears to serve as a proxy for disease complexity. This may be due to factors such as the surgeon’s experience or the complexity of the rupture.45 46
All psychological factors assessed in our study had a significant impact on RTS similar to previous studies.47 48 This emphasises the importance of the patient’s attitude towards surgery and mindset in the subsequent recovery period and may encourage the integration of mental health considerations into preoperative and postoperative assessments. However, high motivation may also carry the risk of premature return to training, potentially resulting in relapse or a new injury.
The strengths of this study include the large sample size with a total of 725 rotator cuff repairs and the minimal exclusion criteria, limited only to the absence of sports activity at baseline. As a result, findings can be generalised to physically active patients with RCT. Additionally, the 24-month follow-up period provides an overview of a longer period during which functional improvements or also deteriorations can be observed.
Our definition of RTS was based on the patient’s subjective assessment of their ability to participate in sport. Therefore, it may also have been influenced by individual levels of motivation or psychological burden. Patients with lower motivation or more pronounced depressive symptoms may have perceived their condition less positively.49 In addition, RTS was assessed as a general outcome, limiting the precision of our analysis for specific sport types. This assessment may also explain the relatively low rate (43.8%) of full return to the same main sport: a change in ranking (eg, from first to second priority) may not be indicative of a poor outcome but may rather reflect changes in personal preferences. Also, we did not collect data on the exact time point at which patients returned to sport, which limits time-based outcome analyses. We acknowledge that measurements like, for example, strength in other motions than abduction are lacking. These additional strength measures were not documented in our database. Some potential confounding factors, such as surgeon’s experience, differences in rehabilitation adherence or structural tendon healing, were not considered in our analysis.
We developed an exploratory model with 10 predictors aiming at identifying factors associated with full RTS after ARCR.36 The model showed a sound predictive accuracy compared with other recent orthopaedic models.30 50 However, we must acknowledge that the selection of the 10 predictors in this model was data-driven and therefore prone to testimation bias35 and could lead to overfitting. If the aim was to develop and validate a proper prediction model for RTS, there would remain room to improve model specification and performance by making use of expert knowledge (eg, using Delphi surveys) and/or advanced variable selection procedure methods.51
Conclusion
This study examined the relationship between epidemiological factors and sports activity in physically active patients who underwent ARCR. Over half of ARCR patients achieved full RTS, with nearly all returning to a sport they had already practised before surgery. Traumatic injury aetiology, high motivation to RTS, higher sports activity levels and a low depression score were associated with full RTS within 2 years after ARCR. Based on these findings, a multivariable model for full RTS after ARCR was established, contributing to the evolving field of prognostic modelling for ARCR outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Warth RJ , Briggs KK , Dornan GJ , et al . Patient expectations before arthroscopic shoulder surgery: correlation with patients’ reasons for seeking treatment. J Shoulder Elbow Surg 2013;22:1676–81. 10.1016/j.jse.2013.05.003 23850307 · doi ↗ · pubmed ↗
- 2Klouche S , Lefevre N , Herman S , et al . Return to Sport After Rotator Cuff Tear Repair: A Systematic Review and Meta-analysis. Am J Sports Med 2016;44:1877–87. 10.1177/0363546515598995 26316611 · doi ↗ · pubmed ↗
- 3Burns JP , Snyder SJ . Arthroscopic rotator cuff repair in patients younger than fifty years of age. J Shoulder Elbow Surg 2008;17:90–6. 10.1016/j.jse.2007.05.006 18069008 · doi ↗ · pubmed ↗
- 4Plate JF , Haubruck P , Walters J , et al . Rotator cuff injuries in professional and recreational athletes. J Surg Orthop Adv 2013;22:134–42. 10.3113/jsoa.2013.0134 23628566 · doi ↗ · pubmed ↗
- 5Dines JS , Jones K , Maher P , et al . Arthroscopic Management of Full-Thickness Rotator Cuff Tears in Major League Baseball Pitchers: The Lateralized Footprint Repair Technique. Am J Orthop (Belle Mead NJ) 2016;45:128–33.26991564 · pubmed ↗
- 6Unfallversicherung V Ig . Return-to-competition: testmanual zur beurteilung der spielfähigkeit nach akuter verletzung der schulter. 2022. Available: https://www.vbg.de/cms/sport/return-to-competition/rtc-schulter [Accessed 26 Apr 2024].
- 7Schwank A , Blazey P , Asker M , et al . 2022 Bern Consensus Statement on Shoulder Injury Prevention, Rehabilitation, and Return to Sport for Athletes at All Participation Levels. J Orthop Sports Phys Ther 2022;52:11–28. 10.2519/jospt.2022.10952 34972489 · doi ↗ · pubmed ↗
- 8Shrier I . Strategic Assessment of Risk and Risk Tolerance (St ARRT) framework for return-to-play decision-making. Br J Sports Med 2015;49:1311–5. 10.1136/bjsports-2014-094569 26036678 · doi ↗ · pubmed ↗