Consensus‐Based Recommendations on Pulp Therapies in Primary and Permanent Teeth: IAPD Porto Forum
Vineet Dhar, Ikhlas El‐Karim, James A. Coll, Ashraf F. Fouad, Anne C. O'Connell, Saeed Asgary, Lars Bjørndal, Zafer C. Cehreli, Yasmi O. Crystal, Manikandan Ekambaram, Brian D. Hodgson, Nicola P. Innes, Jonas Almeida Rodrigues, Nessrin A. Taha, Nitesh Tewari, Tugba Turk

TL;DR
This paper presents 38 evidence-based recommendations for pulp therapies in primary and permanent teeth, emphasizing minimally invasive approaches and calcium silicate cements.
Contribution
Provides updated, consensus-based clinical guidelines for pulp treatment using modern biological insights and materials.
Findings
Calcium silicate cements are preferred for vital pulp therapy over traditional materials.
Selective caries removal is recommended over complete excavation in deep caries cases.
Conservative approaches are prioritized for managing irreversible pulpitis and traumatic injuries.
Abstract
Recent understanding of pulp biology has shifted treatment paradigms toward preservation‐based approaches. Traditional diagnostic terminology and treatment protocols require updating to align with current evidence supporting the pulp's healing capacity. Sixteen international specialists in pediatric dentistry and endodontics convened at the 3rd IAPD Summit in Porto, Portugal (November 2024) to develop consensus‐based recommendations on pulp therapies in primary and permanent teeth. Following a structured three‐phase approach, experts conducted systematic literature reviews and participated in Delphi surveys using a 7‐point Likert scale. Recommendations achieving > 70% consensus were categorized as strong (based on RCTs/systematic reviews), conditional (observational studies), or consensus‐based statements (expert opinion). Thirty‐eight evidence‐based recommendations were developed…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 FIGURE 1
FIGURE 1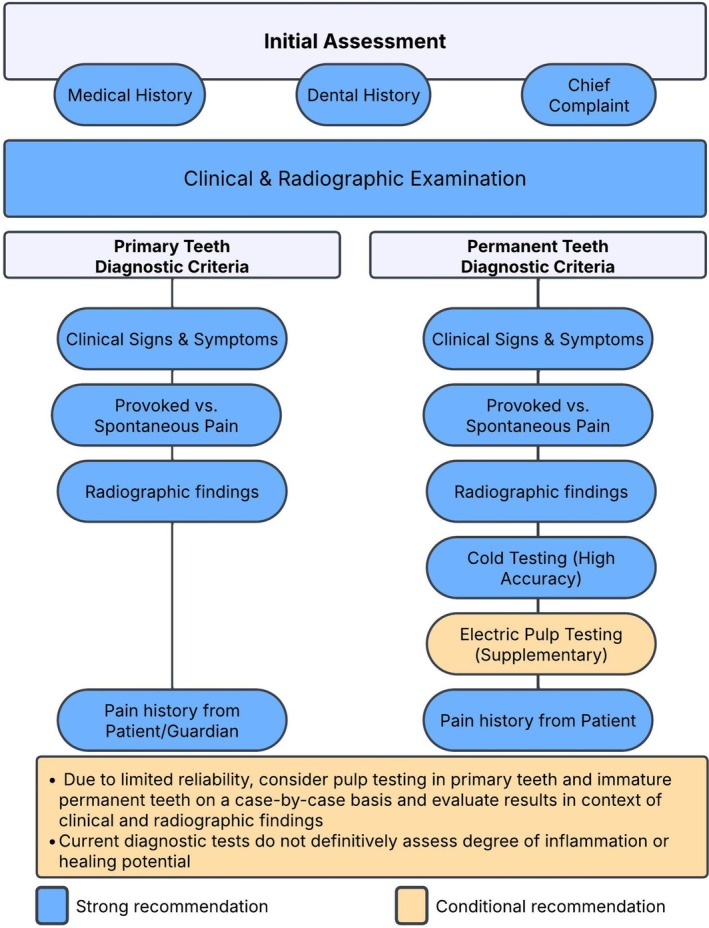 FIGURE 2
FIGURE 2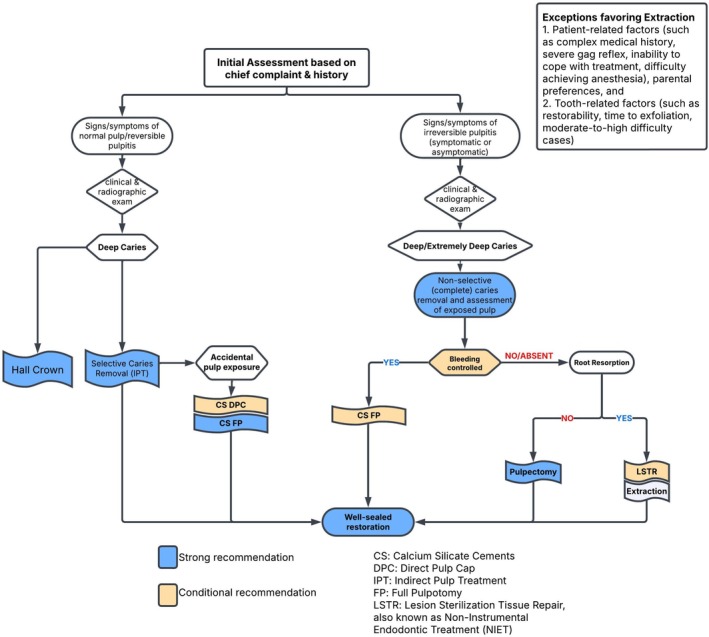 FIGURE 3
FIGURE 3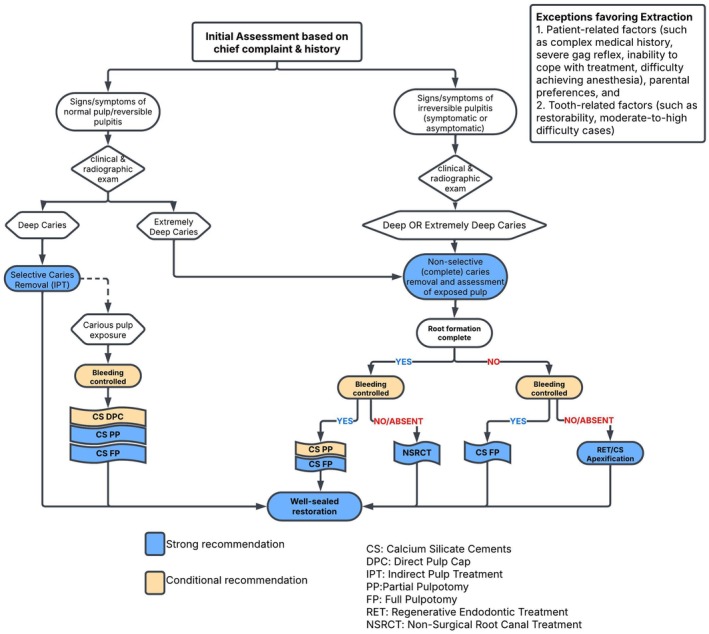 FIGURE 4
FIGURE 4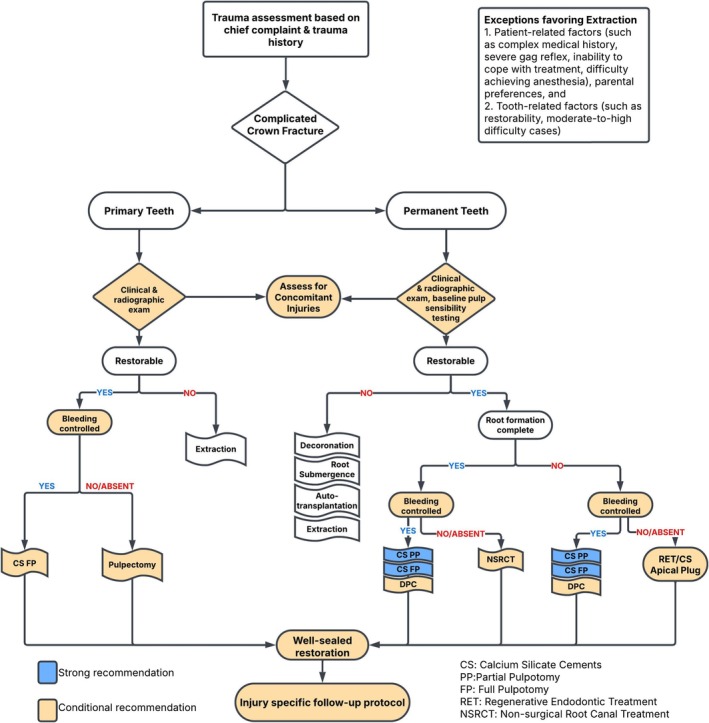 FIGURE 5
FIGURE 5|
|
|
|
| Members: Ikhlas El‐Karim (Chair), James A. Coll, Ashraf Fouad, Nicola Innes, Jonas A. Rodrigues |
|
|
| Members: James A. Coll (Chair), Yasmi Crystal, Zafer Çehreli, Vineet Dhar, Mani Ekambaram, Brian Hodgson |
|
|
| Members: Ashraf Fouad (Chair), Saeed Asgary, Lars Bjorndal, Nessrin Taha, Tugba Turk |
|
|
| Members: Anne O'Connell (Chair), Nitesh Tewari |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Statement | Type of statement | Strength of evidence (percent agreement) | |
|---|---|---|---|
|
| |||
| 1. | In primary and permanent teeth with deep caries diagnosed with reversible pulpitis, clinicians should attempt conservative treatment, as the inflamed dental pulp, if not exposed, can heal when provided with a favorable environment. In these cases, the inflammatory process stimulates odontoblasts to produce reactionary dentin. | Consensus‐based Recommendation | Conditional (> 70%) |
| 2. | In primary and permanent teeth with extremely deep caries and iatrogenic pulp exposure, severe injury causes odontoblast cell death and the inflammatory response triggers differentiation of the dental pulp stem cells to produce reparative dentin, if an environment favorable for healing can be created. | Consensus‐based Recommendation | Conditional (> 70%) |
| 3. | Pulpal diagnosis requires a comprehensive assessment and documentation of the patient's medical and, dental history, chief complaint, along with the results of diagnostic tests, and clinical and radiographic examinations. Key signs and symptoms to be considered include the onset, course, duration, intensity, aggravating and relieving factors, nocturnal pain, as well as evoked and persistent pain. For permanent teeth, the painful response and duration to cold stimuli should be assessed. For primary teeth, clinicians should primarily rely on clinical signs and symptoms of provoked versus spontaneous pain, along with radiographic findings. | Consensus‐based Recommendation | Conditional (> 70%) |
| 4. | In mature permanent teeth, cold testing exhibits high sensitivity, specificity, and accuracy, even in crowned teeth. It can be complemented by electric pulp testing when the results are inconclusive. Given its limited reliability, diagnostic pulp testing should be carried out on a case‐by‐case basis in primary teeth and immature permanent teeth, using clinical judgment to interpret results. | Consensus‐based Recommendation | Conditional (> 70%) |
| 5. | Current diagnostic tests cannot definitively assess the degree of inflammation or the healing potential of the dental pulp in both primary and permanent teeth. Although there are no commercially available devices for clinical use, the assessment of the pulp's microcirculation and vitality may be determined by measuring oxygen saturation. Currently, the biomarkers of inflammation have limited utility in clinical practice due to lack of established thresholds. | Consensus‐based Recommendation | Conditional (> 70%) |
| 6. | The duration of pulpal bleeding should be considered alongside other diagnostic indicators of pulpal health rather than in isolation. Although prolonged bleeding has not been definitively established as a predictor of outcomes of VPT, achieving hemostasis may be viewed to be of practical and pragmatic importance for the success of VPT. | Consensus‐based Recommendation | Conditional (> 70%) |
| 7. | In primary teeth with deep caries, clinicians may consider placing a temporary glass ionomer restoration without any caries tissue removal or after selective caries removal to soft dentin (interim therapeutic restoration) for a duration of 1–3 months as a diagnostic tool for pulp vitality before proceeding with definitive treatment. The interim restoration must provide an adequate seal to prevent bacterial ingress while monitoring pulpal response. | Consensus‐based Recommendation | Conditional (> 70%) |
| 8. | For the management of deep and extremely deep carious lesions, particularly in cases of pulp exposure, it is suggested to utilize magnification for direct visualization of the pulp, including pulpal bleeding, homogeneity of exposure, and to identify any areas of necrosis and degeneration. | Consensus‐based Statement | Strength—not determined (> 70%) |
|
| |||
| 9. | After confirming pulp vitality and considering the stage of tooth development, as well as the ability to place a well‐sealed restoration, clinicians should adopt a conservative approach to managing deep caries in both primary and permanent teeth. It is recommended to use selective caries removal or stepwise removal over non‐selective (complete) caries removal, except in cases of extremely deep caries. Selective caries removal offers an additional advantage as it is completed in a single visit. | Consensus‐based Recommendation | Strong (> 70%) |
| 10. | For vital primary teeth with multi‐surface or large single‐surface deep carious lesions, either no carious tissue removal with Hall Technique or selective caries removal to soft dentin followed by a preformed crown is recommended over non‐selective (complete) caries tissue removal. | Consensus‐based Recommendation | Strong (> 70%) |
| 11. | Considering the risk of pulp exposures, treatment of deep and extremely deep carious lesions should be performed using a dental dam to isolate the lesion and protect against bacterial contamination. Dental dam isolation is not needed when using Hall technique for management of deep caries in primary teeth. | Consensus‐based Statement | Strength—not determined (> 70%) |
| Statement | Type of statement | Strength of evidence (percent agreement) | |
|---|---|---|---|
| 12. | For vital primary teeth with deep caries, in the event of a pulp exposure, clinicians should utilize calcium silicate cement (CSC) as VPT medicament. These biomaterials promote pulp healing, stimulate the formation of reparative dentin, provide an effective seal, and thereby enhance the long‐term success of the treatment. | Consensus‐based Recommendation | Strong (> 70%) |
| 13. | When evaluating for VPT, selective caries removal (IPT) should be the preferred approach for primary teeth with deep caries and healthy pulp or reversible pulpitis due to its high success rate. | Consensus‐based Recommendation | Strong (> 70%) |
| 14. | DPC is a viable treatment option for managing pulp exposures measuring less than 1 mm in vital primary teeth with deep caries diagnosed with healthy pulp or reversible pulpitis. However, DPC has a lower success rate compared to pulpotomy. | Consensus‐based Recommendation | Conditional (> 70%) |
| 15. | Clinicians should consider performing FP using CSCs in the event of pulp exposure in primary teeth with deep caries and diagnosed with healthy pulp or reversible pulpitis. | Consensus‐based Recommendation | Strong (> 70%) |
| 16. | Primary teeth that exhibit signs of irreversible pulpitis, based on history of spontaneous pain, can be managed successfully with a CSC pulpotomy for 12 months or possibly longer, provided the pulp upon access appears to be vital and there are no signs of necrosis or furcal radiolucency. Achieving hemostasis is considered important for the success of this CSC pulpotomy. | Consensus‐based Recommendation | Conditional (> 70%) |
| 17. | Pulpectomy can be considered as a non‐vital pulp treatment (NVPT) option for primary teeth without preoperative root resorption diagnosed with irreversible pulpitis or necrotic pulp with or without furcal radiolucency. This procedure can be effectively performed using either rotary or manual instrumentation, along with irrigation solutions such as sodium hypochlorite (1%–5%), saline, or chlorhexidine (2%). | Consensus‐based Recommendation | Strong (> 70%) |
| 18. | When obturating root canal(s) of a primary tooth undergoing pulpectomy, select either Zinc Oxide/Iodoform/Calcium Hydroxide or Zinc Oxide Eugenol (ZOE), over Calcium Hydroxide/Iodoform as filling materials based on 18‐month success rates. To avoid overfilling, utilize pluggers for ZOE and lentulo spirals for calcium hydroxide/Iodoform‐based materials. | Consensus‐based Recommendation | Conditional (> 70%) |
| 19. | Non‐Instrumental Endodontic Treatment (NIET), also referred to as Lesion Sterilization and Tissue Repair (LSTR), may be an alternative to pulpectomy for primary teeth with preoperative root resorption diagnosed with irreversible pulpitis or necrotic pulp knowing it has only shown short‐term success and has the potential for antibiotic resistance associated with the procedure. | Consensus‐based Recommendation | Conditional (> 70%) |
| 20. | Following a pulpotomy, NIET (LSTR), or pulpectomy, clinicians should restore the treated tooth with a preformed crown to protect against reinfection and enhance the tooth's long‐term survival. | Consensus‐based Recommendation | Conditional (> 70%) |
| Statement | Type of statement | Strength of evidence (percent agreement) | |
|---|---|---|---|
| 21. | For VPT in permanent teeth with deep caries, clinicians should utilize CSCs. These biomaterials promote pulp healing and stimulate the formation of reparative dentin, thereby enhancing the long‐term success of the treatment. Glass ionomer cement may be used in absence of pulp exposure. Placement of a well‐sealed coronal restoration enhances the long‐term success of the treatment. | Consensus‐based Recommendation | Strong (> 70%) |
| 22. | Selective caries removal (as known as IPT), should be considered as a viable option for managing deep caries, but not extremely deep caries, in permanent teeth diagnosed with healthy or reversible pulpitis. | Consensus‐based Recommendation | Strong (> 70%) |
| 23. | DPC is a viable treatment option for cases of pulp exposure while removing deep caries in permanent teeth, particularly when the pulp is diagnosed as healthy or reversibly inflamed. Notably, the long‐term success rate of DPC in permanent teeth is higher when calcium silicate cements are used as a medicament. | Consensus‐based Recommendation | Conditional (> 70%) |
| 24. | For the management of pulp exposure in permanent teeth with extremely deep caries and various degrees of pulpitis, clinicians can perform either a PP or FP using CSCs, as this approach has demonstrated a high success rate. If hemostasis cannot be achieved when attempting a partial pulpotomy, further tissue removal may be necessary by deepening the partial pulpotomy or progressing to a full pulpotomy. | Consensus‐based Recommendation | Conditional (> 70%) |
| 25. | Due to its minimally invasive nature and potential for pulp preservation, full pulpotomy using CSCs can be an alternative treatment to non‐surgical root canal treatment for mature permanent teeth with carious pulp exposure and clinical signs and symptoms of irreversible pulpitis, such as spontaneous or lingering pain, provided that there are no signs and symptoms of pulp necrosis. Achieving hemostasis may be viewed to be important for the success of VPT. The success rate of this full pulpotomy may be comparable to that of root canal treatment for vital permanent teeth. | Consensus‐based Recommendation | Strong (> 70%) |
| 26. | For immature permanent teeth with extremely deep caries diagnosed with irreversible pulpitis and there are no signs and symptoms of pulp necrosis, FP using CSCs is the recommended VPT due to its effectiveness in supporting root development and maintaining pulp vitality. | Consensus‐based Recommendation | Strong (> 70%) |
| 27. | Both apexification and Regenerative Endodontic Treatments (RETs) are viable options for managing immature, necrotic permanent teeth. The use of CSCs, which are supported by evidence, is preferred over calcium hydroxide (CH) apexification. | Consensus‐based Recommendation | Strong (> 70%) |
| Statement | Type of statement | Strength of evidence (percent agreement) | |
|---|---|---|---|
| 28. | Traumatic dental injuries affect the dental pulp either directly or indirectly due to infection, inflammation, and damage to the periodontium. Evidence supports that dental pulp tissue can heal after dental trauma; therefore clinicians should allow time for healing especially in cases of mild injury, immature teeth, and younger patients. | Consensus‐based Recommendation | Conditional (> 70%) |
| 29. | Traumatic dental injuries must be documented in a standardized manner and validated objective criteria must be used for interpreting the radiographic features for clearer prognostic evaluation. | Consensus‐based Recommendation | Conditional (> 70%) |
| 30. | Clinicians should evaluate for concomitant luxation injuries as these can cause disruption of the vascular supply to the pulp negatively impacting healing in immature permanent teeth with crown fractures. | Consensus‐based Recommendation | Conditional (> 70%) |
| 31. | Clinicians should use a combination of clinical and radiographic signs and symptoms such as pain, infection, discoloration, mobility, and pathological changes in the tooth or bone to assess the need for endodontic intervention in teeth with traumatic injuries. Discoloration in both dentitions may be transient and thereby not a reliable indicator of necrosis. In addition, responses to pulp sensibility tests (thermal, electric, and occasionally, cavity tests) may assist with diagnosis of necrotic pulp in permanent teeth. For primary teeth, pulp sensibility tests are not indicated. A positive response to sensibility tests shortly after trauma is a good predictor of vitality but lack of response is not always associated with subsequent necrosis, especially luxation injuries. | Consensus‐based Recommendation | Conditional (> 70%) |
| 32. | PP or FP has a high success rate in complicated crown fractures. Direct pulp capping has a lower success rate in permanent teeth with complicated crown fractures but may be suitable in select cases or as a temporary treatment in uncooperative children until pulpotomy can be performed. Clinicians should use non‐staining CSCs to prevent discoloration. | Consensus‐based Recommendation | Strong (Pulpotomy) Conditional (DPC) (> 70%) |
| 33. | Appropriate immediate management can limit the adverse complications of most traumatic injuries; however, avulsion and severe luxation (intrusive, extrusive, and lateral) injuries are associated with a higher incidence of complications. | Consensus‐based Recommendation | Conditional (> 70%) |
| 34. | Appropriate follow up of traumatic injuries is important due to the risk of late complications such as discoloration, pulp necrosis, arrest of root formation, apical periodontitis, external inflammatory root resorption, external replacement (ankylosis‐related) resorption, external invasive resorption, and internal resorption. The incidence and management of these complications differ between primary and permanent teeth. | Consensus‐based Recommendation | Conditional (> 70%) |
| 35. | Traumatized immature permanent teeth with pulp necrosis can be managed either by RET or by apical plug using CSC barrier. Both methods have demonstrated comparable clinical, radiographic, and overall success and survival rates. However, RET may be preferred for necrotic teeth in very early stages of root development and for teeth with developmental dental anomalies. | Consensus‐based Recommendation | Conditional (> 70%) |
| 36. | External inflammatory root resorption can be arrested by careful removal of causative factors by endodontic debridement, irrigation, and use of intracanal medicament (Calcium Hydroxide, Triple Antibiotic Paste, Double Antibiotic Paste). External replacement resorption is progressive in nature and cannot be stopped or reversed. In permanent teeth, decoronation or root submergence or autotransplantation and extraction are acceptable treatments in suitable patients. | Consensus‐based Recommendation | Conditional (> 70%) |
| 37. | Pulp canal obliteration in primary and permanent teeth is a healing response and yellow discoloration is due to the internal layers of dentin formed in response to injury. Clinicians should monitor these teeth without any intervention unless pulp necrosis and apical periodontitis develop. | Consensus‐based Recommendation | Conditional (> 70%) |
| 38. | In traumatized permanent incisors, the use of non‐surgical endodontic protocols for teeth with symptomatic or asymptomatic apical periodontitis or acute abscess with varying grades of periapical radiolucency is indicated in cases that fail to respond to RET. | Consensus‐based Recommendation | Conditional (> 70%) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEndodontics and Root Canal Treatments · Surgical Sutures and Adhesives · Dental materials and restorations
Introduction
1
Managing pulpal and apical diseases in primary and permanent teeth is a critical aspect of dental care. Recent advances have transformed our understanding of pulp biology. Current research recognizes pulp's healing capacity and defensive mechanisms, which have shifted treatment paradigms for both primary and permanent dentitions [1, 2]. Traditional perspectives viewed pulpal inflammation as a largely progressive condition often culminating in pulp death. This led to treatment approaches that favored complete pulp removal, even when pulp was partially involved.
Contemporary research reveals that dental pulp possesses remarkable defensive and reparative capabilities, which may be leveraged through minimally invasive interventions [3, 4, 5]. The inflammatory process, once viewed primarily as destructive, is now recognized as a complex biological response that can facilitate healing and repair when appropriately managed [4]. The pulp responds to injury, whether from caries or trauma, through complex cellular and molecular mechanisms.
These mechanisms include recruiting immune cells, releasing inflammatory mediators, and activating dental pulp stem cells (DPSCs). In slowly progressing carious lesions, bacterial products diffuse through dentinal tubules. This triggers a controlled inflammatory response associated with increased odontoblast activity and reactionary dentin formation [5]. More severe injury causes odontoblast cell death. This results in an inflammatory response that, if properly managed, can lead to DPSC activation and differentiation into odontoblast‐like cells, producing reparative dentin [6].
The traditional diagnostic terminology (reversible/irreversible pulpitis) is becoming increasingly inadequate [7], with alternative classifications proposed [8, 9, 10] and consensus efforts underway to align terminology with current evidence. Additionally, there is a lack of consensus on the pulpal diagnostic terminology used by pediatric dentists and endodontists [10, 11, 12]. Clinical evidence suggests that the Wolters classification system may offer a prognostic advantage over traditional American Association of Endodontics (AAE) terminology, especially within the subdivisions of irreversible pulpitis [13].
Accurate diagnosis of pulp status remains a significant challenge. Clinical symptoms and traditional testing methods may not reliably reflect the histological status of the pulp. The limitations of current diagnostic tools for pulpitis, particularly in assessing the inflammatory status of the pulp, have prompted investigation into biomarkers for pulpal diagnosis and prognosis [14, 15]. While the evidence is emerging, no established thresholds yet support the routine use of biomarkers in clinical practice [16].
Recent evidence has challenged traditional treatment paradigms, particularly regarding the management of deep caries, pulp exposures, and pulp injury following dental traumatic injuries. The concept of “irreversible pulpitis” is being reconsidered as evidence emerges that inflamed pulp tissue, once considered irreversibly damaged, may have healing potential under appropriate conditions [17]. Consequently, there is a growing emphasis on pulp preservation using minimally invasive pulp therapies such as partial pulpotomy (PP), which consider pulpal inflammation as existing on a continuum and aim to preserve pulp vitality and function [18].
The development of bioactive materials, particularly calcium silicate‐based cements, has significantly influenced treatment outcomes in vital pulp therapy (VPT) procedures [19, 20]. These materials demonstrate superior biocompatibility and the ability to stimulate reparative dentinogenesis compared to traditional materials [21, 22]. However, questions remain regarding optimal clinical protocols, case selection criteria, and long‐term outcomes. Treatment approaches must be adapted for different patient populations and tooth types.
Pulp therapy in primary teeth presents unique challenges due to their limited lifespan and the presence of a developing permanent successor [2]. The management of immature permanent teeth requires special consideration due to their thin dentinal walls and open apices, necessitating approaches that can promote continued root development [23].
Scope and Purpose
1.1
This research paper formulates consensus‐based recommendations for managing pulp therapies in primary and permanent teeth. Specifically, this paper:
- Synthesizes the current evidence regarding the biological basis for VPT.
- Provides evidence‐based guidelines for diagnosis and appropriate selection for various pulp therapy procedures in primary and permanent teeth.
- Identifies research gaps and future directions for advancing evidence‐based care.
Target Users
1.2
The target users are dental professionals including general practitioners, pediatric dentists, and endodontists.
Target Population
1.3
The target population includes children and adolescents requiring pulp treatment due to caries or trauma in primary and permanent teeth.
Exceptions
1.4
Clinicians may need to modify these recommendations due to various factors. These include the patient's cooperation level, complex medical conditions, difficulty achieving local anesthesia, limited mouth opening, severe gag reflex, facial swelling, undiagnosed oral pain, complications from previous pulp therapy, or concurrent periodontal issues. Individual considerations such as parent and patient preferences, patient's age, and treatment costs may necessitate alternate treatment approaches including extraction of the tooth.
Materials and Methods
2
These consensus‐based recommendations were derived from 16 international specialists in pediatric dentistry (10 experts) and endodontics (6 experts). Some of these experts also had internationally recognized expertise in cariology. The experts convened at the 3rd IAPD Summit in Porto, Portugal, in November 2024. They followed a structured approach comprising three phases: pre‐summit preparation, summit meeting, and post‐summit activities (Figure 1).
Methods.
Pre‐Summit Activities
2.1
First, the working groups (WG) comprised 16 experts, was established and assigned to focus on four key areas in pulp therapy (Table 1). Each expert panelist systematically searched the literature of their area of expertise. They submitted draft recommendations 2 months before the summit. From these drafts, 38 recommendation statements were created that underwent a Delphi process using a 7‐point Likert Scale.
The Delphi process is a structured method that uses multiple rounds of anonymous surveys with a panel of experts, where participants refine their opinions based on feedback from previous rounds until consensus emerges. It is designed to harness collective expert judgment while avoiding the biases of face‐to‐face group dynamics [24].
Summit Activities
2.2
During the meeting, the WGs made minor editorial edits to recommendations with over 70% agreement and revised the recommendations that received under 70% agreement in the initial Delphi round. The WGs created: consensus‐based recommendations and consensus‐based statements, both developed with Delphi agreement. The recommendations were categorized based on the strength of supporting evidence. Strong recommendations were based on randomized controlled trials (RCTs), systematic reviews, or clinical practice guidelines. Conditional recommendations were based on lower‐quality studies such as observational studies, while consensus‐based statements reflected expert opinion.
Consensus‐based recommendations drawn from clinical practice guidelines were evaluated for strength according to their original source and were not automatically elevated to the “strong” category.
Post‐Summit Activities
2.3
After a second Delphi survey, all recommendations received over 70% consensus from the 16‐member workgroup. This resulted in 38 recommendations that were reviewed and approved by the WGs in the final survey. The glossary of terms is presented in Table 2.
Understanding the Recommendations/Statements
2.4
The recommendations are intended to assist clinicians in making informed decisions regarding pulp therapies. They do not replace clinical judgment.
Strong recommendations for specific interventions indicate that the WGs have determined that the benefits substantially outweigh potential risks. In these cases, clinicians should consider implementing the recommended intervention as a standard approach.
Conditional recommendations reflect that the WG felt less certain in the benefit–risk assessment. These recommendations may change with new evidence. A conditional recommendation suggests that while an intervention may be appropriate for some patients, clinicians should carefully evaluate individual circumstances and consider alternative approaches.
Consensus‐based statements represent expert‐derived best practices in areas where high‐quality research evidence is currently limited or unavailable.
Results
3
The 38 recommendations regarding pulp therapies in primary and permanent teeth, along with their strength and percent agreement, are presented (Tables 3, 4, 5, 6). The WGs have also developed evidence‐based decision trees on pulp diagnosis and treatment to support clinicians in their chairside decision‐making (see Figures 2, 3, 4, 5).
Diagnostic approach to pulpal status assessment.
Management of pulpitis in carious primary teeth.
Management of pulpitis in carious permanent teeth.
Management of complicated crown fracture.
A summary of the supporting evidence along with justification for the assigned strength of evidence is outlined in the Appendix S1.
Discussion
4
Conducting high quality research on pulp therapies in children presents several methodological challenges. These include navigating Institutional Review Board approval processes for studies involving minors, collecting long‐term follow‐up data, and working with small sample sizes due to the infrequency of severe pediatric dental trauma cases. This highlights the need for multi‐institutional collaboration, innovative study designs that make optimal use of limited cases, and sustained funding to support the long follow‐up times necessary to confirm outcomes of pediatric dental trauma.
Despite these obstacles, ongoing efforts to develop creative methodologies and strengthen research networks remain important for advancing evidence‐based care. The review of current evidence has identified research gaps and future directions:
Evidence suggests that current categories of reversible and irreversible pulpitis are inadequate to reflect the capacity of the pulp to heal and should be modified [7, 10]. A critical research priority remains the development of reliable, objective diagnostic tools for assessing pulpal status. While current diagnostic methods rely heavily on clinical symptoms and sensibility testing, there is a pressing need for chairside diagnostic tests and biomarkers that can accurately reflect the inflammatory status of the pulp [14, 16]. Future research should focus on establishing clearer correlations between clinical symptoms and histological status of the pulp, as current evidence shows significant discrepancies between these parameters [25]. Research is also needed to better understand the optimal endpoints for caries removal in deep lesions, particularly regarding the biological markers that indicate successful conservative treatment. Long‐term studies comparing outcomes between selective and complete caries removal approaches are essential, especially given the paradigm shift toward more conservative techniques [16, 26].
Research in primary tooth pulp therapy faces unique challenges requiring specific attention. There is a pressing need for age‐appropriate diagnostic methods, as current pulp testing approaches in caries and trauma show limited reliability in young children largely due to difficulty in performing and interpreting children's responses [2, 27]. Future studies should focus on developing diagnostic criteria specifically tailored to primary teeth, considering their unique anatomical and physiological characteristics. Long‐term outcome studies comparing different VPT techniques are crucial, particularly regarding the efficacy of newer bioactive materials in primary teeth. Research should also investigate the impact of child‐specific factors such as age, behavior, and compliance on treatment outcomes. The development of biocompatible materials specifically designed for primary teeth represents another important research direction, as current materials are often adaptations of those developed for permanent teeth.
Research priorities for VPT in permanent teeth should focus on generating high‐quality evidence to improve clinical outcomes. Extended longitudinal studies (5–10 years) comparing VPT outcomes with conventional root canal treatment are critically needed in children and adolescents, where maintaining tooth vitality for decades is essential [28]. While current evidence supports using vital pulp therapies in cases previously considered irreversible, robust long‐term comparative data would help establish definitive clinical protocols [18, 29, 30]. Standardized, evidence‐based protocols addressing specific indications for each VPT technique, optimal irrigation solutions, hemostasis protocols, and restoration techniques would enhance clinical predictability [31, 32]. More studies directly comparing different VPT approaches (IPT, DPC, PP, and FP) with standardized methodologies, outcomes, and outcome measures would help establish a hierarchy of treatment options based on tooth type, patient age, extent and location of caries, and preoperative symptoms [16, 33]. Given these limitations, permanent teeth that have undergone VPT, which includes IPT, should have long‐term monitoring during recall visits and routine radiographic examinations to facilitate timely intervention or referral when indicated. Research should investigate materials and medications that are specifically anti‐inflammatory and therapeutic to the inflamed pulp, beyond current CSCs [34]. This includes exploration of pharmacological agents that can effectively modulate pulpal inflammation, bioactive materials that promote pulp healing and dentinogenesis, and novel delivery systems that optimize therapeutic effects at the pulp‐dentin interface [35, 36].
The identification and validation of reliable biomarkers for pulpal inflammation would significantly improve diagnostic accuracy and treatment planning [37]. Investigation into pulp regeneration strategies incorporating tissue engineering principles could potentially transform management of deeply carious permanent teeth [1]. This includes research on stem cell applications, growth factors that promote pulpal healing, and biomimetic scaffolds that support tissue regeneration [23, 38, 39]. By addressing these research priorities, the profession can continue to advance toward more predictable, biologically based approaches to managing pulpal disease in permanent teeth, potentially reducing the need for more invasive procedures while maintaining pulp vitality for improved long‐term outcomes [40].
Future research in dental trauma should prioritize the development of improved methods for assessing pulp status following injury in both primary and permanent teeth. This is particularly important in the immediate post‐trauma period when current diagnostic tools may be unreliable. Studies are needed to identify early indicators of pulp necrosis and better understand healing patterns in different types of traumatic injuries. Age‐related differences in healing responses require further investigation, especially in determining the optimal timing of intervention after trauma. Research into regenerative approaches for traumatized immature permanent teeth is particularly important, as these cases present unique challenges and opportunities for promoting continued root development [23]. Several research priorities span across all areas of pulp therapy. The development of standardized outcome measures and uniform reporting criteria for clinical studies is essential for advancing the field. The need for a well‐sealed restoration following vital pulp therapy is universally recognized; however, there is a critical need to deepen our understanding of the molecular and cellular mechanisms underlying pulp‐dentin complex responses to injury and treatment. Integrating new technologies, such as advanced imaging techniques and artificial intelligence applications into diagnostic practices offers promising directions for future research. The benefit of cone beam computed tomography (CBCT) should be assessed and referral to a specialist made when appropriate. Investigation into cost‐effectiveness and long‐term outcomes of conservative versus invasive approaches is needed to inform clinical decision‐making. Future studies should also focus on developing minimally invasive treatment approaches and novel delivery systems for therapeutic agents, while further advancing our understanding of regenerative techniques and biomaterial development [4, 5]. These research priorities highlight the need for a multi‐faceted approach to advancing the field of pulp therapy, combining basic science research with clinical investigations to develop more predictable and less invasive treatment approaches in both primary and permanent teeth. Success will require collaboration across disciplines and continued investment in both laboratory and clinical research infrastructure.
In summary, clinicians often encounter uncertainty in diagnosing the condition of pulp, as definitive histological confirmation of pulpitis is not feasible. While clinical symptoms, radiographic signs, and pulp sensibility tests offer guidance, they do not consistently reflect the healing potential of the inflamed pulp. Pulpal inflammation should be considered a continuum rather than a binary condition. In cases where teeth exhibit clinical signs and symptoms of pulpitis, treatment should be initiated using a tiered approach, with conservative methods as the first‐line treatment. Advancing our understanding of pulp biology, refining diagnostic tools, and developing more conservative and regenerative therapies are essential to improving long‐term outcomes and preserving natural dentition. The IAPD Porto Forum has outlined key research priorities to address the current challenges and unmet needs in managing pulp inflammation and trauma in primary and permanent teeth. By addressing these identified research priorities, the dental community can work toward a future where the inflamed or traumatized pulp is managed with greater precision, reliability, and biological compatibility. This will ultimately lead to better quality of life for patients of all ages.
Author Contributions
Dr. Vineet Dhar led the expert panel. Dr. Ikhlas El‐Karim, Dr. James A. Coll, Dr. Ashraf F. Fouad, and Dr. Anne C. O'Connell led workgroups on specific domains. All authors contributed equally to concept, writing, and revisions.
Funding
The authors have nothing to report.
Conflicts of Interest
The authors declare no conflicts of interest.
Supporting information
Data S1: ipd70068‐sup‐0001‐AppendixS1.pdf.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1I. El Karim , P. Cooper , I. About , et al., “Deciphering Reparative Processes in the Inflamed Dental Pulp,” Frontiers in Dental Medicine 2, no. 651219 (2021): 1–10.
- 2J. Coll , V. Dhar , and C. Chen , “Use of Vital Pulp Therapies in Primary Teeth 2024,” Pediatric Dentistry 46, no. 1 (2024): 13–26.38449041 · pubmed ↗
- 3N. Philip , X. Li , and H. Hu , “Treatment Outcomes of Pulpotomy Versus Pulpectomy in Vital Primary Molars Diagnosed With Symptomatic Irreversible Pulpitis: Protocol for a Non‐Inferiority Randomised Controlled Trial,” BMC Oral Health 24 (2024): 626.38807160 10.1186/s 12903-024-04411-6PMC 11134690 · doi ↗ · pubmed ↗
- 4J. Farges , B. Alliot‐Licht , C. Baudouin , et al., “Odontoblast Control of Dental Pulp Inflammation Triggered by Cariogenic Bacteria,” Frontiers in Physiology 4 (2013): 326.24273514 10.3389/fphys.2013.00326 PMC 3823031 · doi ↗ · pubmed ↗
- 5A. Smith , N. Cassidy , H. Perry , C. Bègue‐Kirn , J. V. Ruch , and H. Lesot , “Reactionary Dentinogenesis,” International Journal of Developmental Biology 39, no. 1 (1995): 273–280.7626417 · pubmed ↗
- 6A. Smith , R. Tobias , N. Cassidy , et al., “Influence of Substrate Nature and Immobilization of Implanted Dentin Matrix Components During Induction of Reparative Dentinogenesis,” Connective Tissue Research 32, no. 1–4 (1995): 291–296.7554930 10.3109/03008209509013736 · doi ↗ · pubmed ↗
- 7I. Mejare , S. Axelsson , T. Davidson , et al., “Diagnosis of the Condition of the Dental Pulp: A Systematic Review,” International Endodontic Journal 45, no. 7 (2012): 597–613.22329525 10.1111/j.1365-2591.2012.02016.x · doi ↗ · pubmed ↗
- 8J. Galicia and O. Peters , “Proposal for a New Diagnostic Terminology to Describe the Status of the Dental Pulp,” International Endodontic Journal 54, no. 8 (2021): 1415–1416.34271591 10.1111/iej.13545 · doi ↗ · pubmed ↗