Prognostic value of systemic immune-inflammation index for colorectal cancer: a systematic review and meta-analysis
Pengfei Wang, Huiying Jiang

TL;DR
This study finds that a high systemic immune-inflammation index is linked to worse outcomes in colorectal cancer patients.
Contribution
The study clarifies the prognostic value of SII in CRC through a comprehensive meta-analysis.
Findings
Higher SII is associated with significantly poorer overall survival in CRC patients.
Elevated SII is also linked to worse progression-free survival in CRC patients.
The results are consistent across various subgroups and show no significant publication bias.
Abstract
Although the systemic immune-inflammation index (SII) has gained attention as a prognostic biomarker in colorectal cancer (CRC), existing studies report inconsistent findings due to methodological variability. This meta-analysis was conducted to clarify the prognostic value of SII in CRC. PubMed, Embase, the Cochrane Library and Web of Science were systematically searched for literature up to November 2025. The association between SII and clinical outcomes in CRC was identified. Studies that satisfying the inclusion and exclusion criteria were selected. Progression-free survival (PFS) and overall survival (OS) were the primary outcomes, which were presented by hazard ratios (HRs) with 95% confidence intervals (CIs). Heterogeneity and the stability of results were performed by subgroup and sensitivity analyses. Review Manager 5.4 and STATA 15.1 were conducted to analyze. Thirty-five…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
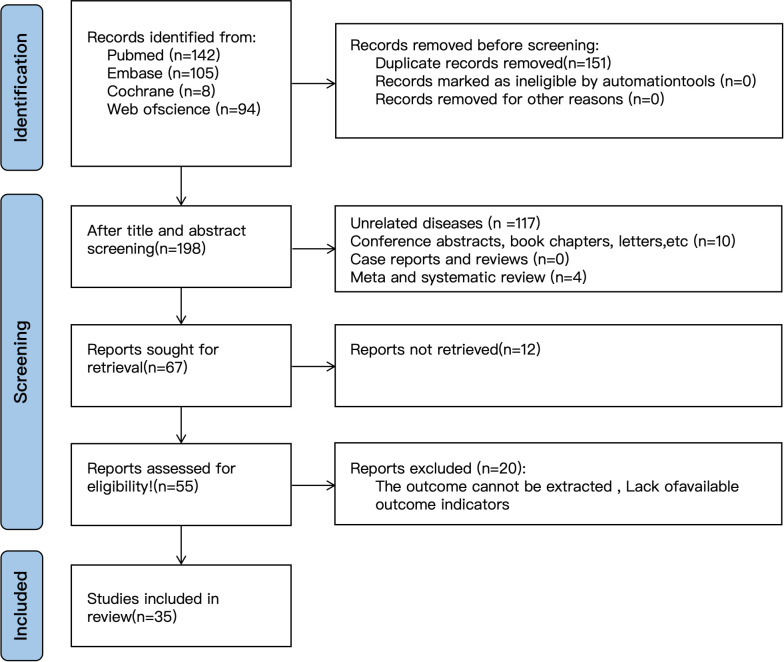 Figure 1
Figure 1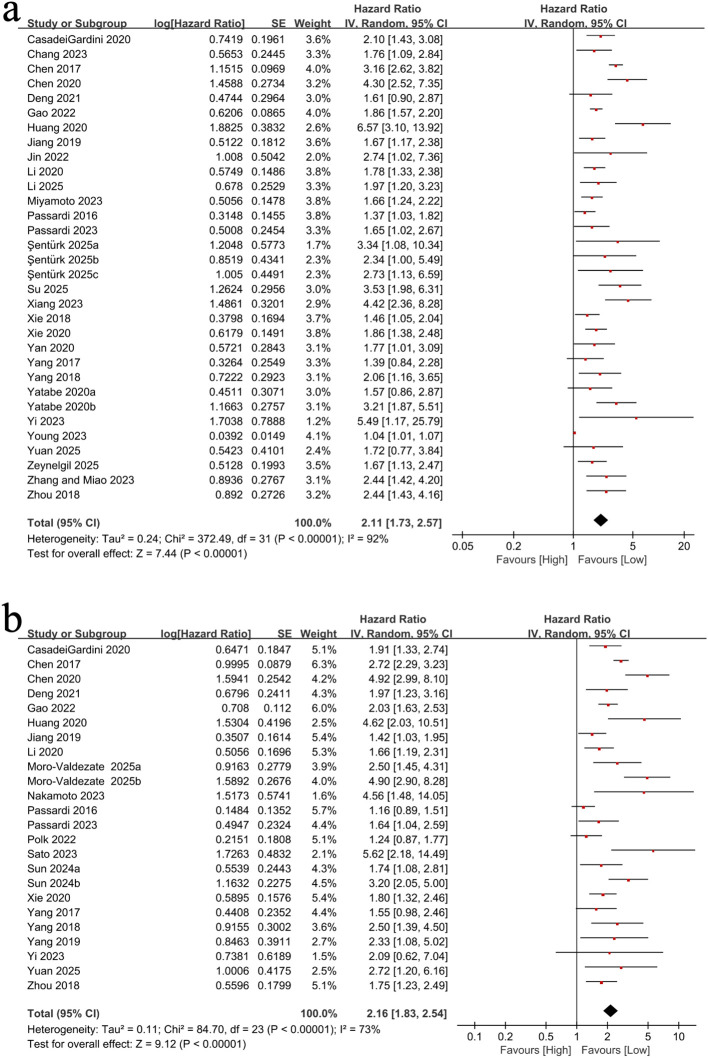 Figure 2
Figure 2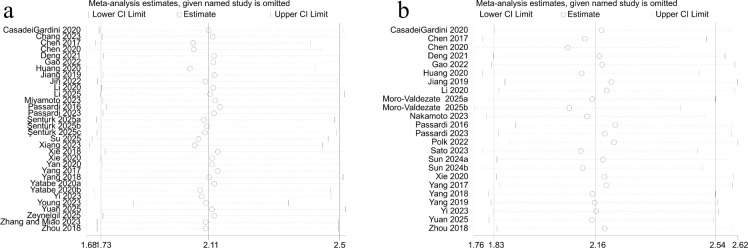 Figure 3
Figure 3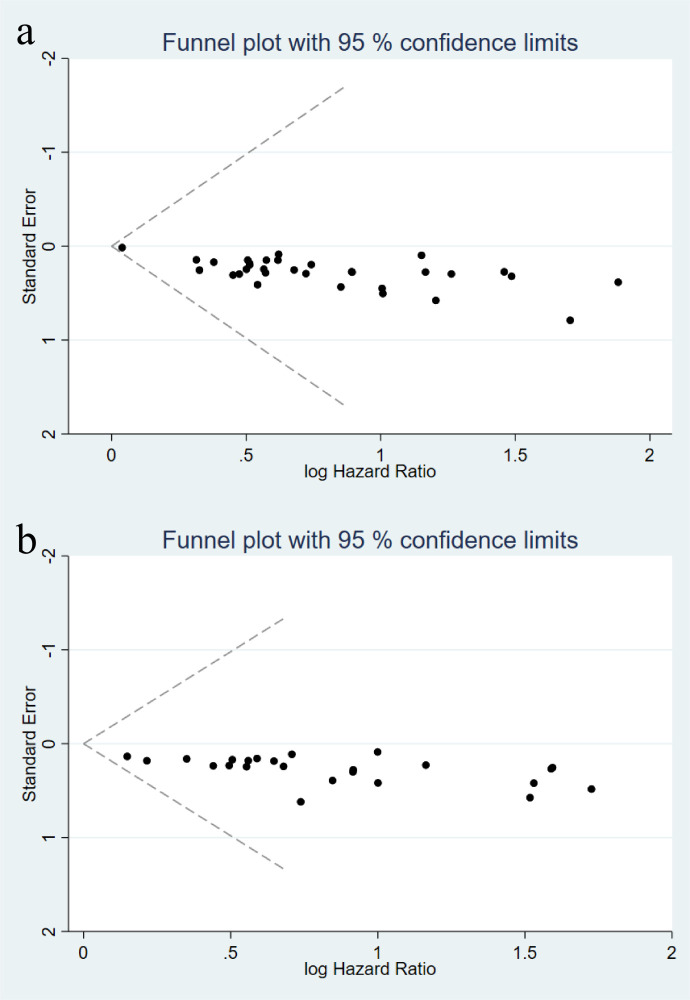 Figure 4
Figure 4| Author | Study period | Region | Study design | Population | Therapeutic approach | Test time | Sample size | Male | Female | Mean/Median age | Mean/Median BMI | Mean/Median tumor size | TNM stage | SII cut-off | Outcome | Quality score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CasadeiGardini 2020 | 2007-2012 | Italy | Retrospective | Metastatic colorectal cancer patients | First-line chemotherapy ± bevacizumab (CT ± B) | Baseline | 131 | 78 | 53 | 67 | NA | NA | IV | 6068 | OS,PFS | 8 |
| Chang 2023 | 2004-2014 | China | Retrospective | Patients who underwent colorectal cancer resection | Colorectal cancer resection ± adjuvant therapy | Within 14 days before surgery | 768 | 416 | 352 | 70 | NA | NA | II | 616 | OS | 8 |
| Chen 2017 | 1994-2010 | China | Retrospective | Colorectal cancer (CRC) patients | Colorectal cancer resection ± adjuvant chemotherapy | Before surgery | 1383 | 808 | 575 | 60 | NA | 5 | I-IV | 340 | OS,PFS | 7 |
| Chen 2020 | 2010-2015 | China | Retrospective | Colorectal cancer (CRC) patients | Surgical resection ± adjuvant treatment | 7 days before surgery | 206 | 108 | 98 | 56.8 | NA | NA | I-IV | 127.7 | OS,PFS | 7 |
| Deng 2021 | 2006-2016 | China | Retrospective | Colorectal liver metastasis (CRLM) patients | Radical resection ± perioperative chemotherapy | 7 days before surgery | 283 | 187 | 96 | 57 | NA | 2.4 | I-IV | 0.0135 | OS,PFS | 8 |
| Gao 2022 | 2014-2020 | China | Retrospective | Patients with digestive system tumors (including esophageal, gastric, and colorectal cancer) | Surgical resection | Before surgery | 8384 | 5844 | 2540 | NA | NA | NA | I-IV | 550 | OS,PFS | 7 |
| Huang 2020 | 2013-2017 | China | Retrospective | Patients with colorectal cancer who underwent radical surgery | Radical surgery | Before surgery | 1279 | 763 | 516 | 28-75 | NA | NA | I-III | 340 | OS,PFS | 9 |
| Jiang 2019 | 2010-2017 | China | Retrospective | Patients with metastatic colorectal cancer (mCRC) and RAS wild-type (WT) who received first-line cetuximab combined with chemotherapy | First-line chemotherapy + cetuximab | Within 3 days before treatment | 102 | 72 | 30 | NA | NA | NA | mCRC | 660.55 | OS,PFS | 8 |
| Jin 2022 | 2012-2015 | China | Retrospective | Patients with stage I colorectal cancer (CRC) who underwent radical surgery | Radical surgery | Within 1 week before surgery | 476 | 259 | 217 | 60.8 | NA | NA | I(pT1-2N0) | 540.262 | OS | 8 |
| Li 2020 | 2016-2019 | China | Retrospective | Colorectal cancer (CRC) patients | Surgery, neoadjuvant chemoradiotherapy, chemotherapy, or no surgery | Before treatment | 3919 | NA | NA | NA | NA | NA | NA | 340-1505 | OS,PFS | 8 |
| Li 2025 | 2010-2020 | Jingdezhen, Jiangxi Province, China | Retrospective | Colorectal cancer (CRC) patients | Radical resection | Within 7 days preoperatively | 324 | 183 cases (56.48%) | 141 cases (43.52%) | 62.60 ± 12.49 | NA | 5 | I-III | 532.985 | OS | 8 |
| Miyamoto 2023 | 2005-2019 | Japan | Retrospective | Patients with metastatic colorectal cancer who received first-line systemic chemotherapy | First-line systemic chemotherapy | 2 weeks before chemotherapy | 272 | 141 | 131 | 63 | 22.6 | NA | II-III | 640 | OS | 8 |
| Moro-Valdezate 2025a | 2011-2019 | Valencia, Spain | Observational | Stage I–III colorectal cancer patients undergoing curative resection (age ≥18) | Curative surgical resection (laparoscopic or open approach) | Preoperative peripheral blood sampled within 1 month before surgery | 764 | 465 (60.9%) | 299 (39.1%) | 65 | 27.68 kg/m² | NA | I-III | 919.48 | PFS | 8 |
| Moro-Valdezate 2025b | 2011-2019 | Valencia, Spain | Observational | Stage I–III colorectal cancer patients undergoing curative resection (age ≥18) | Curative surgical resection (laparoscopic or open approach) | Preoperative peripheral blood sampled within 1 month before surgery | 764 | 465 (60.9%) | 299 (39.1%) | 65 | 27.68 kg/m² | NA | I-III | 1401.01 | PFS | 8 |
| Nakamoto 2023 | 2012-2017 | Japan | Retrospective | CRC patients who underwent radical resection | Radical resection | Preoperative | 118 | 72 | 46 | 70(34-94) | 22.2 | NA | 0-III | 598 | PFS | 8 |
| Passardi 2016 | 2007-2012 | Italy | Prospective | Patients with metastatic colorectal cancer | First-line chemotherapy ± bevacizumab (FOLFIRI/FOLFOX4 ± B) | Baseline (before systemic treatment) | 289 | 103 | 65 | 65 | NA | NA | IV | 730 | OS,PFS | 8 |
| Passardi 2023 | 2016-2019 | Italy | Prospective | Patients with metastatic colorectal cancer (mCRC) who received first-line chemotherapy combined with bevacizumab | First-line chemotherapy + bevacizumab (FOLFIRI/FOLFOX4/CAPIRI/CAPOX + B) | At baseline and before each treatment cycle | 182 | 103 | 65 | 65 | NA | NA | IV | 730 | OS,PFS | 9 |
| Polk 2022 | 2001-2018 | Hungary | Retrospective | Colon cancer liver metastasis (CLM) patients | Surgery, CT, targeted therapy | 24–48 hours before surgery | 67 | 36 | 31 | 65(38-80) | NA | NA | NA | 535 | PFS | 8 |
| Sato 2023 | 2013-2020 | Japan | Retrospective | Obstructive CRC (OCRC) patients treated with self-expanding metal stents (SEMS) as palliative or bridge-to-surgery | Palliative treatment, bridge-to-surgery | Preoperative | 92 | 50 | 36 | 71 | 21.6 | NA | I-III | 597 | PFS | 8 |
| Şentürk 2025a | 2015-2023 | Turkey (Sakarya Training and Research Hospital) | Retrospective | Rectal cancer patients | Low anterior resection; Neoadjuvant therapy (34.22%); Adjuvant therapy (82.57%) with FOLFOX/FOLFIRI regimens | Preoperative (baseline) | 637 | 407 (63.9%) | 230 (36.1%) | 63.55 ± 12.49 | NA | 5 | T-stage: I -IV | 846.259 | OS | 8 |
| Şentürk 2025b | 2015-2023 | Turkey (Sakarya Training and Research Hospital) | Retrospective | Rectal cancer patients | Low anterior resection; Neoadjuvant therapy (34.22%); Adjuvant therapy (82.57%) with FOLFOX/FOLFIRI regimens | Preoperative (baseline) | 637 | 407 (63.9%) | 230 (36.1%) | 63.55 ± 12.49 | NA | 5 | T-stage: I -IV | 846.259 | OS | 8 |
| Şentürk 2025c | 2015-2023 | Turkey (Sakarya Training and Research Hospital) | Retrospective | Rectal cancer patients | Low anterior resection; Neoadjuvant therapy (34.22%); Adjuvant therapy (82.57%) with FOLFOX/FOLFIRI regimens | Preoperative (baseline) | 637 | 407 (63.9%) | 230 (36.1%) | 63.55 ± 12.49 | NA | 5 | T-stage: I -IV | 846.259 | OS | 8 |
| Su 2025 | 2015-2023 | China (Suzhou/Changzhou, Jiangsu Province) | Retrospective | Patients with advanced left-sided CRC (initially unresectable or postoperative recurrent stage IV) receiving first-line CAPEOX ± bevacizumab | First-line chemotherapy: CAPEOX (capecitabine + oxaliplatin) ± bevacizumab | Blood samples obtained within 1 month prior to starting first-line chemotherapy | 231 | 162 (70.1%) | 69 (29.9%) | 65 | NA | NA | IV | 1,424.80 | OS | 8 |
| Sun 2024a | 2018-2020 | China | Retrospective | Rectal cancer patients undergoing radical surgery | Laparoscopic radical surgery | Within 7 days before surgery | 292 | 173 | 119 | 71 | 21.6 | NA | I-III | 449.325 | PFS | 8 |
| Sun 2024b | 2018-2020 | China | Retrospective | Rectal cancer patients undergoing radical surgery | Laparoscopic radical surgery | Within 21–56 days after surgery | 292 | 173 | 119 | 71 | 21.6 | NA | NA | 568.13 | PFS | 8 |
| Xiang 2023 | 2013-2017 | China | Retrospective | Patients under 50 years old diagnosed with colorectal cancer who underwent radical resection | Radical resection | Before surgery or within 1 week before surgery | 236 | 143 | 93 | 45 | 22.9 | NA | I-III | 637.6 | OS | 9 |
| Xie 2018 | 2009-2014 | China | Retrospective | Patients with stage IV metastatic colorectal cancer (mCRC) | Radical surgery | Before surgery | 240 | 157 | 83 | 59(18-90) | NA | NA | IV | 649.45 | OS | 8 |
| Xie 2020 | 2012-2014 | China | Retrospective | Colorectal cancer patients | Surgery ± adjuvant chemotherapy | Before surgery | 662 | 408 | 254 | 59 | NA | 5.0 ± 2.2 | TNM | 649.4 | OS,PFS | 8 |
| Yan 2020 | 1997-2013 | China | Retrospective | Patients with synchronous colorectal peritoneal cancer (SCRPC) who underwent cytoreductive surgery (CRS) and systemic chemotherapy (CT) | Cytoreductive surgery + systemic chemotherapy | Before surgery or within 1 week before surgery | 103 | 67 | 36 | NA | NA | NA | TNM | 410 | OS | 8 |
| Yang 2017 | 2009-2016 | China | Retrospective | Patients with wild-type RAS metastatic colorectal cancer (mCRC) who received cetuximab treatment | First-line chemotherapy + cetuximab | Within 10 days before cetuximab administration | 95 | 58 | 37 | 56 | NA | NA | M1a\M1b | 460.66 | OS,PFS | 8 |
| Yang 2018 | 2010-2017 | China | Retrospective | Patients with colorectal cancer who received neoadjuvant chemoradiotherapy (CRT) | Neoadjuvant chemoradiotherapy (CRT) | Within 4 weeks before CRT | 98 | 59 | 39 | 53 | NA | NA | TNM | 437.72 | OS,PFS | 8 |
| Yang 2019 | 2009-2015 | China | Retrospective | Stage III/IV CRC patients receiving adjuvant chemoradiotherapy | Adjuvant chemoradiotherapy (CRT) | Within 2 weeks before radiotherapy | 220 | 87 | 133 | 56 (23–78) | NA | NA | III-IV | 534.94 | PFS | 8 |
| Yatabe 2020a | 2010-2014 | Japan | Retrospective | Patients who underwent colorectal cancer resection | Surgical resection | Within 3 weeks before surgery | 733 | 463 | 270 | 66(58-74) | NA | NA | 0-IV | NA | OS | 8 |
| Yatabe 2020b | 2010-2014 | Japan | Retrospective | Patients with colorectal cancer (CRC) | Colorectal cancer resection ± preoperative radiotherapy/chemotherapy | Within 3 weeks before surgery | 733 | 463 | 270 | 66 | NA | NA | 0-IV | NA | OS | 8 |
| Yi 2023 | 2017-2022 | China | Retrospective | Patients with MSI-H metastatic colorectal cancer (mCRC) who received anti-PD-1 treatment | Anti-PD-1 treatment ± chemotherapy/anti-angiogenesis therapy | Within 1 week before surgery | 75 | 48 | 27 | 47(23-84) | NA | NA | IV | 409.6 | OS,PFS | 8 |
| Young 2023 | 2014-2019 | USA | Retrospective | Patients with metastatic colorectal cancer (mCRC) who received transarterial radioembolization (TARE) | Transarterial radioembolization (TARE) | 30 days after surgery | 41 | 21 | 20 | 61.4 ± 8.2 | NA | NA | NA | 409.6 | OS | 8 |
| Yuan 2025 | 2020-2022 | Chongqing, China (First Affiliated Hospital of Army Medical University) | Retrospective | pMMR advanced colorectal cancer patients (confirmed by immunohistochemistry, clinical stage IV) | Camrelizumab (anti-PD-1) combined with bevacizumab (anti-VEGF) targeted therapy | Baseline (before immunotherapy initiation) | 216 | 120 (55.6%) | 96 (44.4%) | 57(25-83) | 25 kg/m² | NA | IV | 663.9 | OS,PFS | 8 |
| Zeynelgil 2025 | 2020-2024 | Türkiye | Retrospective | Patients with metastatic colorectal cancer | Chemotherapy with or without biological agents; metastasectomy for selected patients | Pre-treatment, before the first chemotherapy | 155 | 99 | 56 | 60 (24-83) | NA | NA | IV | 835.96 | OS | 8 |
| Zhang and Miao 2023 | 2019-2023 | China | Retrospective | Patients who underwent colorectal cancer resection | Radical resection for colorectal cancer | Before surgery | 160 | 62 | 41 | 61.4 ± 8.2 | NA | NA | TNM | 513.53 | OS | 8 |
| Zhou 2018 | 2007-2015 | China | Retrospective | Patients who underwent colorectal cancer resection | Colorectal cancer resection ± preoperative/postoperative adjuvant treatment | Before surgery | 516 | 331 | 185 | 58.4 | NA | NA | I-IV | 568.69 | OS,PFS | 8 |
| Subgroup | Number of studies | Pooled HR (95% CI) | I² (%) | P-value |
|---|---|---|---|---|
| Overall | 32 | 2.11 (1.73–2.57) | 92 | <0.00001 |
| Study design | ||||
| Retrospective | 30 | 2.05 (1.67–2.52) | 92 | <0.00001 |
| Prospective | 2 | 1.89 (1.45–2.47) | 45 | <0.00001 |
| TNM stage | ||||
| Stage I–II | 8 | 2.31 (1.65–3.24) | 78 | <0.00001 |
| Stage III | 4 | 3.65 (1.98–6.91) | 85 | <0.00001 |
| Stage IV/Metastatic | 19 | 2.47 (1.34–4.84) | 93 | <0.00001 |
| Tumor location | ||||
| Colon | 12 | 2.18 (1.67–2.85) | 89 | <0.00001 |
| Rectal | 8 | 1.96 (1.45–2.65) | 85 | <0.00001 |
| Mixed/Colorectal | 12 | 2.05 (1.62–2.59) | 91 | <0.00001 |
| Treatment modality | ||||
| Chemotherapy alone | 14 | 2.01 (1.52–2.66) | 90 | <0.00001 |
| Chemo + Bevacizumab | 6 | 1.78 (1.23–2.58) | 85 | 0.002 |
| Surgical resection | 16 | 2.24 (1.78–2.82) | 93 | <0.00001 |
| Timing of measurement | ||||
| Baseline | 24 | 1.98 (1.62–2.43) | 91 | <0.00001 |
| Post-treatment | 8 | 2.44 (1.43–4.17) | 89 | 0.001 |
| Geographic region | ||||
| Asia | 26 | 2.12 (1.70–2.64) | 92 | <0.00001 |
| Europe/America | 6 | 1.87 (1.45–2.42) | 88 | <0.00001 |
| Age group | ||||
| ≥ro years | 12 | 2.34 (1.78–3.08) | 88 | <0.00001 |
| <65 years | 20 | 1.89 (1.52–2.35) | 92 | <0.00001 |
| Outcome | Moderator | β | 95% CI | P value | Studies(k) |
|---|---|---|---|---|---|
| OS | Cut-off (continuous) | –0.00001 | –0.00014–0.00013 | 0.94 | 28 |
| OS | ln(Cut-off) | 0.006 | –0.072–0.083 | 0.89 | 28 |
| PFS | Cut-off (continuous) | –0.00002 | –0.00017–0.00012 | 0.75 | 23 |
| PFS | ln(Cut-off) | –0.002 | –0.080–0.077 | 0.97 | 23 |
| Subgroup | Number of studies | Pooled HR (95% CI) | I² (%) | P-value |
|---|---|---|---|---|
| Overall | 24 | 2.16 (1.83–2.54) | 73 | <0.00001 |
| Study design | ||||
| Retrospective | 22 | 2.08 (1.74–2.49) | 74 | <0.00001 |
| Prospective | 2 | 1.28 (0.98–1.67) | 45 | 0.07 |
| TNM stage | ||||
| Stage III | 6 | 3.64 (1.65–8.60) | 89 | 0.002 |
| Stage IV/Metastatic | 12 | 2.23 (1.38–4.01) | 78 | 0.001 |
| Mixed stages | 6 | 1.97 (1.31–2.98) | 65 | 0.001 |
| Tumor location | ||||
| Colon | 10 | 2.24 (1.78–2.82) | 78 | <0.00001 |
| Rectal | 6 | 1.89 (1.42–2.52) | 69 | <0.00001 |
| Mixed/Colorectal | 8 | 2.08 (1.62–2.67) | 72 | <0.00001 |
| Treatment modality | ||||
| Chemotherapy alone | 10 | 2.01 (1.52–2.66) | 75 | <0.00001 |
| Chemo + Bevacizumab | 4 | 1.41 (0.97–2.06) | 68 | 0.07 |
| Surgical resection | 12 | 2.18 (1.74–2.73) | 74 | <0.00001 |
| Timing of measurement | ||||
| Baseline | 18 | 2.01 (1.65–2.45) | 74 | <0.00001 |
| Post-treatment | 6 | 2.18 (1.45–3.28) | 72 | <0.00001 |
| Geographic region | ||||
| Asia | 20 | 2.19 (1.82–2.63) | 74 | <0.00001 |
| Europe/America | 4 | 1.89 (1.42–2.52) | 68 | <0.00001 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInflammatory Biomarkers in Disease Prognosis · Cancer Immunotherapy and Biomarkers · Colorectal Cancer Surgical Treatments
Introduction
1
Colorectal cancer (CRC) is a main global cause of cancer-related morbidity and mortality, exhibiting substantial prognostic variability even among patients classified within the same TNM stage. Although the TNM system forms the basis of survival assessment, its failure to account for inter-individual differences emphasizes the need for supplementary biomarkers to refine risk stratification. Systemic inflammation, a hallmark of tumor progression, plays a critical role in CRC pathogenesis. Inflammatory biomarkers such as the neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR) have shown prognostic value (13). The systemic immune-inflammation index (SII), calculated as platelet × neutrophil/lymphocyte, has emerged as a reliable indicator of immune-inflammatory status (1). Initially validated in hepatocellular carcinoma, its prognostic relevance in CRC has yet to be fully established.
Recent evidence underscores the prognostic significance of the SII in CRC. In metastatic CRC, a low SII is associated with prolonged progression-free and overall survival among patients receiving first-line chemotherapy (2, 3), whereas an elevated preoperative SII independently predicts inferior overall and disease-free survival following curative resection (1). Subgroup analyses indicate that the SII more accurately differentiates TNM stage-specific survival than the NLR or PLR and maintains prognostic relevance in stage II colorectal cancer when stratified by tumor sidedness (1, 4). Dynamic alterations in the systemic immune-inflammation index change (ΔSII) following resection offer superior prognostic precision compared to static measurements, with elevated ΔSII associated with a 4.3-fold increase in mortality risk (5). SII also retains prognostic relevance in distinct subgroups, including patients with liver metastases (7), obstructive colorectal cancer (14), and microsatellite instability-high tumors treated with immunotherapy (15).
Inconsistencies persist due to methodological heterogeneity. The prognostic significance of the SII varies by K-ras genotype, demonstrating relevance only in wild-type metastatic CRC (6), and its optimal cut-off values differ between colon (535) and rectal liver metastases (792) (7). Although meta-analyses report pooled HR for overall (HR = 1.86) and disease-free survival (HR = 2.03) (8) in digestive malignancies, CRC-specific evaluations remain limited. A recent meta-analysis by Tan et al. included 27 studies with a literature search updated to March 2024 (9). However, variations in study design, endpoint definitions, and patient characteristics—such as treatment strategies, geographic distribution, and inflammatory thresholds—continue to constrain clinical applicability.
This meta-analysis investigates the prognostic utility of the SII in CRC, addressing heterogeneity through comprehensive subgroup analyses stratified by disease stage, treatment modality, tumor location, TNM stage, and biomarker dynamics. Drawing on data from 35 studies comprising 26812 patients, it evaluates the role of SII in enhancing survival prediction and identifying high-risk subgroups to guide individualized treatment strategies.
Materials and methods
2
Literature search
2.1
This study was conducted in accordance with PRISMA 2020 guidelines and was prospectively registered in PROSPERO (CRD420251010606) (10). Two investigators (WPF and JHY) independently performed literature searching. Searching terms as following: “Colorectal, Neoplasm,” “Neoplasm, Colorectal,” “Colorectal Tumors,” “Colorectal Tumor,” “Tumor, Colorectal,” “Tumors, Colorectal,” “Neoplasms, Colorectal,” “Colorectal Cancer,” “Cancer, Colorectal,” “Cancers, Colorectal,” “Colorectal Cancers,” “Colorectal Carcinoma,” “Carcinoma, Colorectal,” “Carcinomas, Colorectal,” “Colorectal Carcinomas,” “Systemic Immune-Inflammation Index,” “systemic immune inflammation index.” The detailed literature searching strategy was depicted in Supplementary Table S1.
Study selection
2.2
Inclusion criteria: 1) CRC confirmed by pathological diagnosis; 2) treatment involving surgery, radiochemotherapy, neoadjuvant radiochemotherapy, or a combination thereof; 3) evaluation of the prognostic significance of the SII for PFS or OS; 4) availability of HRs with 95% confidence intervals (CIs), either reported or derivable from data; 5) stratification into high and low SII groups based on predefined cut-off values; 6) publication as a full-text article.
Exclusion criteria were as follows: 1) reviews, commentaries, conference abstracts, case reports, or letters; 2) insufficient data to estimate HRs and CIs; 3) lack of survival outcomes; and 4) duplicate or overlapping datasets.
WPF and JHY screened titles and abstracts, reviewed full texts, and assessed study eligibility independently. Discrepancies were resolved through discussion.
Data extraction
2.3
WPF and JHY extracted the data independently, with discrepancies resolved through consensus. The first author, publication year, study location, study design, sample size, patient age, study duration, treatment modality, type of immune checkpoint inhibitor, timing of detection, cut-off value, follow-up period, and HRs with 95% CIs for OS and PFS were extracted. When studies simultaneously reported both univariate and multivariate analysis results, multivariate analysis results were preferentially extracted. For studies reporting “Low SII/High SII” comparisons, HRs and CIs were transformed by calculating reciprocals and inverting confidence limits to ensure consistent “High SII/Low SII” comparisons across analyses.
Quality assessment
2.4
Study quality was evaluated by Newcastle-Ottawa Scale (NOS), which assesses selection, comparability, and outcome domains, with a maximum score of nine. High quality studies score 7-9. Detailed scoring criteria and reasons for each assessment are provided in Supplementary Table S2.
Statistical analysis
2.5
Pooled HRs with 95% CIs were computed to estimate the prognostic significance of the SII in CRC. Cochran**’s Q test and Higgins’** I² statistic were used to evaluate the heterogeneity (11). Heterogeneity was deemed significant when the Q-test P-value was < 0.1 or I² exceeded 50%. Data synthesis was conducted using a random-effects model. Sensitivity and subgroup analyses were performed to assess result robustness and identify heterogeneity sources. Funnel plots, Egger**’**s tests were used to examine the publication bias. A two-sided P-value < 0.05 was considered statistically significant. All analyses were conducted using STATA 15.0 and Review Manager 5.4.
Results
3
Study characteristics
3.1
A total of 349 articles were retrieved: PubMed (n=142), Embase (n=105), Cochrane Library (n=8), and Web of Science (n=94). After removing 151 duplicates, 198 records remained. Screening of titles and abstracts excluded 131 records, comprising 117 unrelated diseases, 10 conference abstracts, book chapters, or letters, and 4 meta-analyses or systematic reviews. Sixty-seven articles were identified as potentially eligible and retrieved for full-text review. Twelve were unavailable, leaving 55 for further assessment. Twenty were excluded due to insufficient data or absence of outcome indicators. Ultimately, 35 studies comprising 26812 patients were included (Figure 1) (1–6, 8–40).
Flow chart of literature screening.
Studies were conducted across multiple countries, with the majority from Asia (China, Japan), followed by Europe (Italy, Hungary, Spain) and North America (USA). Four publications each included two cohorts, resulting in a total of 40 cohorts for analysis. Among these, 38 were retrospective and 2 were prospective. All cohort studies were published in English between 2016 and 2025. Study populations included patients with metastatic CRC, those undergoing surgical resection, and individuals receiving surgery, chemotherapy, targeted therapy, or immunotherapy. The SII was primarily measured at baseline or preoperatively, with some studies evaluating postoperative levels. Cut-off values varied substantially across studies, ranging from 340 to 1505. Detailed characteristics of studies are presented in Table 1.
Study quality
3.2
Study quality was evaluated using the NOS, with scores of 7–9 reflecting high methodological rigor (Supplementary Table S2). The mean NOS score was 7.8, indicating overall good quality of included studies.
Meta-analysis results
3.3
SII and OS
3.3.1
We evaluated the association between SII and OS using 32 cohort studies (25,366 participants). Given the substantial heterogeneity (I² = 92%, p < 0.00001; Figure 2A), a random-effects model was applied. Elevated SII was significantly associated with worse OS (HR = 2.11, 95% CI: 1.73–2.57; p < 0.00001; Figure 2A). Prespecified subgroup analyses showed broadly consistent associations across study design, population characteristics, tumor location, treatment modality, timing of SII measurement, geographic region, and sample size (Table 2). Notably, the association appeared strongest in stage III disease (HR = 3.65, 95% CI: 1.98–6.91), and post-treatment SII showed a numerically stronger association than baseline SII (post-treatment: HR = 2.44 vs baseline: HR = 1.98), suggesting potential prognostic value of dynamic inflammatory status during treatment.
Forest plots of the association between the systemic immune-inflammation index (SII) and survival outcomes: (a) overall survival (OS); (b) progression-free survival (PFS).
Meta-regression suggested a stronger prognostic effect in older populations (P = 0.041). Additionally, post-hoc meta-regression analyses indicated that the reported SII cut-off value was not a significant moderator of the pooled OS effect estimate (p = 0.938). The findings were consistent when using log-transformed cut-off values (p = 0.889) (Table 3).
SII and PFS
3.3.2
We investigated the association between SII and PFS across 24 cohort studies (19,402 participants). Substantial heterogeneity was observed (I² = 73%, p < 0.00001), and a random-effects model was used. Elevated SII was significantly associated with shorter PFS (HR = 2.16, 95% CI: 1.83–2.54; p < 0.00001; Figure 2B). Subgroup analyses demonstrated generally consistent findings across key strata, including metastatic status, TNM stage, tumor location, timing of measurement, and geographic region (Table 4). The association was robust in retrospective studies, whereas it did not reach statistical significance in the limited number of prospective cohorts, potentially reflecting smaller sample size and reduced power. Post-hoc meta-regression analyses similarly showed that the reported SII cut-off value did not significantly moderate the pooled PFS effect estimate (p = 0.746). Consistent results were obtained using log-transformed cut-off values (p = 0.968) (Table 3).
Sensitivity analysis
3.4
Sensitivity analysis confirmed the stability of the baseline SII findings, as effect sizes remained consistent when individual studies were sequentially excluded. No single study exerted a disproportionate influence on the results for OS (Figure 3A) or PFS (Figure 3B), supporting the overall reliability of the analysis.
Sensitivity analyses of the association between the systemic immune-inflammation index (SII) and survival outcomes: (a) overall survival (OS); (b) progression-free survival (PFS).
Publication bias
3.5
Publication bias was assessed using funnel plots with pseudo 95% confidence limits and Egger’s regression test. Visual inspection of the funnel plots for OS and PFS suggested an approximately symmetric distribution of studies within the 95% confidence boundaries (Figures 4A, B), with no obvious small-study effects. Consistently, Egger’s test was not statistically significant for either OS (p = 0.669) or PFS (p = 0.261), indicating no evidence of publication bias.
Funnel plots for assessing publication bias in the meta-analysis of the systemic immune-inflammation index (SII) and survival outcomes: (a) overall survival (OS); (b) progression-free survival (PFS).
Discussion
4
Systemic inflammation contributes to tumor progression by promoting genetic mutations, genomic instability, epigenetic alterations, tumor metastasis, and cancer cell proliferation (12). Blood-derived markers, recognized for their accessibility and reproducibility, serve as robust indicators of systemic inflammation and patient prognosis (8, 13). The SII, defined as platelet count × neutrophil count/lymphocyte count, represents the interplay between host inflammatory status and tumor progression (1). However, studies evaluating its prognostic utility in CRC have yielded inconsistent results, likely due to variability in metastatic status (2, 3), treatment modalities (2, 3), timing of assessment (pre- vs. postoperative) (5), and divergent cut-off values (1, 9).
SII cut-off value variation and clinical implications
4.1
A critical challenge hindering the clinical application of SII is the substantial heterogeneity in cut-off values across studies, ranging from 340 to 1505 in our analysis (1, 9).Notably, despite the wide variation in cut-off thresholds across studies, our post-hoc meta-regression did not identify the SII cut-off value as a significant source of heterogeneity for either OS or PFS, suggesting that threshold variability alone may not explain the observed between-study heterogeneity (Table 3). This variability stems from multiple factors: 1) Population differences: Genetic backgrounds, environmental exposures, and baseline inflammatory states vary across geographic regions and ethnic groups; 2) Statistical methodologies: Different approaches for determining optimal thresholds, including receiver operating characteristic (ROC) curve analysis, median values, quartiles, or tertiles; 3) Treatment contexts: SII thresholds may differ between neoadjuvant, adjuvant, and palliative settings; 4) Disease characteristics: Optimal cut-offs may vary between colon and rectal cancers, as evidenced by the different thresholds reported for colon (535) versus rectal (792) liver metastases (7).
This heterogeneity poses significant challenges for clinical implementation and cross-study comparisons. We recommend that future research should: 1) Conduct large-scale prospective multicenter studies using standardized ROC analysis to establish and validate universally applicable optimal cut-off values; 2) Report SII both as continuous variables and categorical variables based on specific thresholds; 3) Consider population-specific reference ranges accounting for age, ethnicity, and geographic factors; 4) Develop dynamic monitoring protocols with standardized time points for SII assessment throughout the treatment trajectory.
Biological mechanisms underlying SII prognostic value
4.2
Elevated SII reflects a systemic inflammatory-immune imbalance characterized by: 1) Neutrophilia promoting tumor progression through VEGF and matrix metalloproteinases (MMPs) release, facilitating angiogenesis and metastasis; 2) Thrombocytosis enhancing tumor cell survival in circulation through platelet-tumor aggregate formation, protecting circulating tumor cells from immune surveillance and shear stress; 3) Lymphocytopenia impairing cytotoxic T cell-mediated antitumor immunity, reducing immunosurveillance capacity 4). This inflammatory-immune imbalance contributes to tumor progression by enhancing the infiltration of immunosuppressive cells, including myeloid-derived suppressor cells (MDSCs) and regulatory T cells (Tregs), within the tumor microenvironment.
TNM stage-specific prognostic value
4.3
Our comprehensive subgroup analysis by TNM stage revealed important insights: 1) Stage III patients showed the strongest association between elevated SII and poor prognosis (OS: HR = 3.65), suggesting SII may be particularly valuable for risk stratification in this intermediate-stage population where treatment intensification decisions are most critical; 2) Stage I-II patients demonstrated significant associations (OS: HR = 2.31), indicating SII**’s utility in identifying high-risk early-stage patients who might benefit from adjuvant therapy; 3) Stage IV/metastatic patients showed consistent prognostic value (OS: HR = 2.47), supporting SII’**s role in treatment monitoring and prognosis prediction in advanced disease.
These findings suggest that SII**’**s prognostic value varies across disease stages, likely reflecting different biological contexts: in early-stage disease, SII may indicate occult micrometastatic burden and systemic inflammatory response to tumor presence; in advanced disease, SII may reflect tumor burden, treatment response, and overall host inflammatory status.
Tumor location heterogeneity
4.4
Our analysis by tumor location revealed that SII**’**s prognostic value was consistent across colon, rectal, and mixed colorectal cancers, with HRs of 2.18, 1.96, and 2.05 respectively for OS. However, we acknowledge an important limitation: most original studies did not provide hazard ratios stratified by tumor location, preventing more granular analysis of potential differences between right-sided, left-sided, and rectal cancers. This represents a significant knowledge gap, as tumor location is increasingly recognized as a critical prognostic and predictive factor in CRC.
Future research should prioritize providing location-stratified analyses, as biological differences between proximal and distal CRC may influence SII**’**s prognostic value. Right-sided tumors are associated with different molecular features (higher rates of microsatellite instability, BRAF mutations, and CpG island methylator phenotype), distinct microbiome profiles, and different patterns of systemic inflammation compared to left-sided tumors (4).
Treatment modality and timing considerations
4.5
Our analysis revealed important differences based on treatment modality and timing: 1) Post-treatment SII measurements showed stronger associations with prognosis than baseline measurements, suggesting SII**’s potential as a treatment response biomarker; 2) The attenuated association in patients receiving bevacizumab combination therapy may reflect this agent’s anti-inflammatory properties; 3) SII’**s consistent prognostic value across different treatment modalities supports its broad applicability.
These findings suggest potential clinical applications: 1) Baseline SII assessment for initial risk stratification and treatment planning; 2) Serial SII monitoring during treatment to assess treatment response and detect early progression; 3) Integration with imaging and other biomarkers for comprehensive treatment monitoring. Recent studies suggest that dynamic SII changes (ΔSII) may offer superior prognostic precision compared to static measurements (5).
Geographic bias and generalizability
4.6
A significant limitation of our study is the geographic imbalance in included studies, with the majority originating from Asia (particularly China and Japan), limited representation from Europe, and minimal representation from North America, Africa, and other regions. This geographic bias raises important questions about the generalizability of our findings across different populations.
Several factors may contribute to geographic differences in SII prognostic value: 1) Genetic and ethnic variations in inflammatory responses and immune function; 2) Environmental factors including diet, microbiome composition, and exposure to infectious agents; 3) Healthcare system differences affecting cancer screening, diagnosis timing, and treatment protocols; 4) Population-specific baseline inflammatory marker ranges.
We strongly recommend that future research should prioritize inclusion of more diverse, globally representative populations. Multi-center international collaborations are essential to validate SII**’**s prognostic value across different ethnic groups and healthcare systems. Only through such efforts can SII be established as a truly universal prognostic biomarker suitable for global clinical implementation.
Comparison with previous meta-analyses
4.7
Our study provides significant incremental value compared to previous meta-analyses, particularly the recent analysis by Tan et al.: 1) Larger sample size: 35 studies with 26812 patients vs. 27 studies with 18,420 patients; 2) More recent literature: search updated to November 2025 vs. March 2024; 3) More comprehensive subgroup analyses: including TNM stage and tumor location analyses not performed in previous studies; 4) More detailed methodological reporting: comprehensive sensitivity analyses and quality assessment.
These enhancements provide stronger evidence for SII**’**s prognostic value and more nuanced understanding of its clinical applications across different patient subgroups.
Limitations and future directions
4.8
This study has several limitations requiring cautious interpretation. First, the marked heterogeneity in SII cut-off values across studies may compromise result comparability and clinical applicability. Second, the predominance of retrospective designs (38 of 40 cohorts) introduces potential confounders and selection bias. Third, the geographic imbalance limits generalizability to non-Asian populations. Fourth, insufficient reporting of tumor location-specific data prevented more granular analysis of potential anatomical heterogeneity.
Future research should address these limitations through: 1) Large-scale prospective multicenter studies with standardized protocols; 2) Development and validation of universally applicable SII cut-off values using ROC analysis; 3) Integration of SII with molecular subtyping and other biomarkers for enhanced prognostic accuracy; 4) Investigation of SII**’**s role in treatment selection and monitoring; 5) Exploration of dynamic SII monitoring protocols; 6) Expansion to more geographically diverse populations.
Clinical implementation recommendations
4.9
Based on our findings, we propose the following clinical implementation framework: 1) Baseline SII assessment at diagnosis for initial risk stratification; 2) Serial SII monitoring during treatment (e.g., every 3 months) to assess treatment response; 3) Integration with TNM staging to refine prognostic assessment, particularly in Stage III disease; 4) Consideration of treatment intensification for patients with persistently elevated SII; 5) Development of nomograms incorporating SII with other clinical and molecular variables for personalized prognostication.
Conclusion
5
This meta-analysis of 35 studies involving 26812 patients demonstrates that elevated pretreatment SII is significantly associated with inferior overall and progression-free survival in colorectal cancer, supporting its utility as a robust prognostic biomarker. The prognostic value is consistent across diverse clinical subgroups, with particularly strong associations in Stage III disease and elderly patients. However, substantial heterogeneity in cut-off values and geographic bias limit immediate clinical implementation.
Large-scale, prospective, multicenter investigations with standardized methodologies are warranted to validate these findings, establish optimal threshold values, and develop evidence-based clinical implementation guidelines. Integrating SII with other biomarkers and molecular subtyping may enhance prognostic accuracy and inform individualized therapeutic strategies in colorectal cancer.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chen JH Zhai ET Yuan YJ Wu KM Xu JB Peng JJ . Systemic immune-inflammation index for predicting prognosis of colorectal cancer. World J Gastroenterol. (2017) 23:6261. doi: 10.3748/wjg.v 23.i 34.6261, PMID: 28974892 PMC 5603492 · doi ↗ · pubmed ↗
- 2Passardi A Scarpi E Cavanna L Dall'Agata M Tassinari D Leo S . Inflammatory indexes as predictors of prognosis and bevacizumab efficacy in patients with metastatic colorectal cancer. Oncotarget. (2016) 7:33210–9. doi: 10.18632/oncotarget.8901, PMID: 27120807 PMC 5078087 · doi ↗ · pubmed ↗
- 3Casadei Gardini A Scarpi E Valgiusti M Monti M Ruscelli S Matteucci L . Prognostic role of a new index (multi inflammatory index) in patients with metastatic colorectal cancer: results from the randomized ITA Ca trial. Ther Adv Med Oncol. (2020) 12:1758835920958363. doi: 10.1177/1758835920958363, PMID: 33062063 PMC 7534088 · doi ↗ · pubmed ↗
- 4Chang J Cheng H Huang S Lin H Chang S Lin C . The impact of inflammatory markers on prognosis of stage II colon cancers depends on tumour sidedness. ANZ J Surg. (2023) 93:182–95. doi: 10.1111/ans.18014, PMID: 36097407 · doi ↗ · pubmed ↗
- 5Chen Q Wu H Guo X Gu K Wang W Chen X . The change of systemic immune-inflammation index independently predicts survival of colorectal cancer patients after curative resection. Mediators Inflamm. (2020) 2020:1–8. doi: 10.1155/2020/4105809, PMID: 33293896 PMC 7718069 · doi ↗ · pubmed ↗
- 6Jin Z Wu Q Deng X Wang Z . The clinic factors in evaluating long-term outcomes of patients with stage I colorectal cancer. Asian J Surg. (2022) 45:2231–8. doi: 10.1016/j.asjsur.2021.11.055, PMID: 35012854 · doi ↗ · pubmed ↗
- 7Page MJ Mc Kenzie JE Bossuyt PM Boutron I Hoffmann TC Mulrow CD . The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 372:n 71. doi: 10.1136/bmj.n 71, PMID: 33782057 PMC 8005924 · doi ↗ · pubmed ↗
- 8Deng Y Zhao Y Qin J Huang X Wu R Zhou C . Prognostic value of the C-reactive protein/albumin ratio and systemic immune-inflammation index for patients with colorectal liver metastasis undergoing curative resection. Pathol Oncol Res. (2021) 27:633480. doi: 10.3389/pore.2021.633480, PMID: 34257601 PMC 8262228 · doi ↗ · pubmed ↗