Dose and normal tissue complication probability analysis of various radiotherapy regimens for thymomas
Wu Xiandong, Luo Haifeng, Zhichao Wang, Li Chao, Hu Yan, Li Jingjing

TL;DR
This study compares different radiotherapy techniques for thymomas and finds that non-coplanar VMAT offers better protection for normal tissues and balanced breast dose.
Contribution
The study introduces a detailed comparison of non-coplanar VMAT's dosimetric advantages and NTCP outcomes in thymoma radiotherapy.
Findings
VMAT techniques showed lower lung, heart, spinal cord, and esophagus doses compared to IMRT.
NONCO-VMAT provided better multi-organ protection and balanced breast dose compared to CO-VMAT.
CO-VMAT increased breast NTCP in female patients, while NONCO-VMAT reduced it.
Abstract
This study aimed to compare dosimetric differences and normal tissue complication probability (NTCP) among coplanar intensity-modulated radiation therapy (CO-IMRT), non-coplanar IMRT (NONCO-IMRT), coplanar volumetric-modulated arc therapy (CO-VMAT), and non-coplanar VMAT (NONCO-VMAT) in thymoma radiotherapy and clarify the value of non-coplanar plans. Forty-eight post-thymoma surgery patients were enrolled in this study. Four radiotherapy plans (50 Gy/25 fractions) were made for each patient. The target conformity index (CI), homogeneity index (HI), and organ-at-risk (OAR) (lungs, heart, etc.) dose parameters were then evaluated. NTCP was calculated using the Lyman–Kutcher–Burman (LKB) model. Statistical analysis was performed using the Student–Newman–Keuls (SNK-q) test (p < 0.05 for significance). There were no significant clinical differences in target volume coverage and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
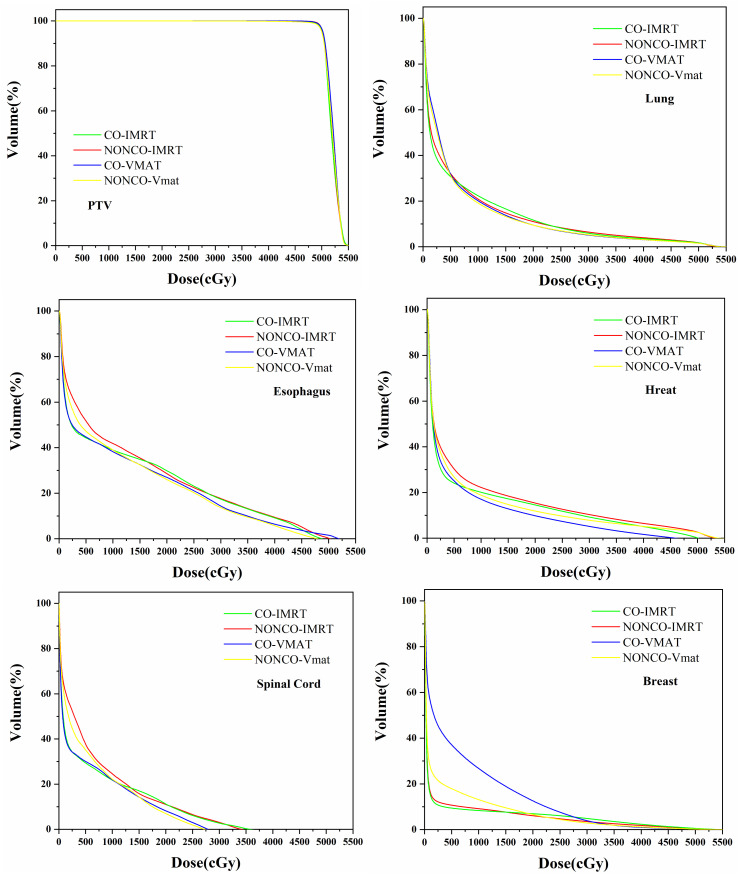 Figure 1
Figure 1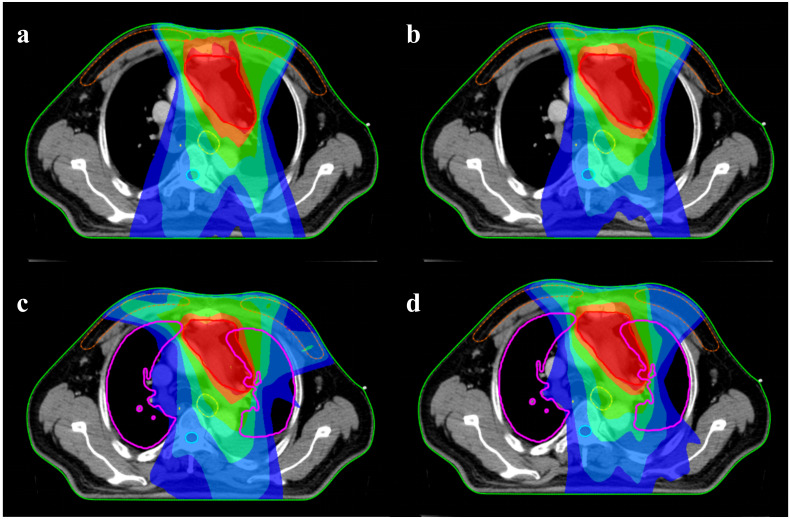 Figure 2
Figure 2| OAR | Dose constraint |
|---|---|
| Lung | V5 < 50% |
| V20 < 20% | |
| Vmean < 12 Gy | |
| Heart | V30 < 40% |
| Dmean < 26 Gy | |
| Spinal cord | Dmax < 40 Gy |
| Breast | Vmean < 5 Gy |
| Esophagus | Dmax < 50 Gy |
| OAR | n | m | D50 | Endpoint |
|---|---|---|---|---|
| Lung | 1 | 0.37 | 30.5 | Pneumonitis |
| Heart | 0.78 | 0.59 | 43.3 | Major adverse cardiac events |
| Spinal cord | 0.05 | 0.175 | 66.5 | Myelopathy |
| Esophagus | 0.29 | 0.15 | 46 | Grade 2 esophagitis |
| Breast | 0.36 | 0.19 | 60 | Fibrosis |
| OAR | Parameter | CO-IMRT | NON-IMRT | CO-VMAT | NON-VMAT |
|---|---|---|---|---|---|
| PTV | CI | 0.997 ± 0.004 | 0.999 ± 0.002 | 0.999 ± 0.002 | 0.999 ± 0.002 |
| HI | 0.090 ± 0.017 | 0.081 ± 0.008 | 0.081 ± 0.014 | 0.083 ± 0.011 | |
| Lung | V5 | 30.742 ± 10.790 | 31.999 ± 11.583 | 31.790 ± 9.89 | 31.328 ± 10.732 |
| V20 | 11.694 ± 6.490 | 11.018 ± 6.852 | 9.465 ± 5.252 | 9.461 ± 5.627 | |
| Vmean | 6.878 ± 2.819 | 6.93 ± 3.029 | 6.769 ± 2.377 | 6.694 ± 2.501 | |
| Heart | V30 | 11.550 ± 7.018 | 11.162 ± 6.693 | 7.897 ± 3.793 | 8.408 ± 4.304 |
| Vmean | 7.844 ± 3.942 | 8.305 ± 3.932 | 6.664 ± 2.642 | 7.041 ± 2.849 | |
| Spinal cord | Dmax | 28.909 ± 9.716 | 28.23 ± 9.764 | 24.073 ± 7.583 | 24.316 ± 7.556 |
| Breast | Dmean | 3.372 ± 2.022 | 3.162 ± 2.131 | 6.786 ± 3.559 | 3.587 ± 1.840 |
| V5 | 9.287 ± 4.998 | 10.361 ± 5.591 | 35.888 ± 16.120 | 16.690 ± 7.400 | |
| V10 | 8.321 ± 4.657 | 8.823 ± 5.126 | 24.729 ± 13.312 | 12.295 ± 6.097 | |
| Esophagus | Dmax | 39.990 ± 11.578 | 39.976 ± 11.653 | 37.246 ± 13.388 | 38.246 ± 12.731 |
| Dmean | 12.498 ± 5.960 | 13.207 ± 5.967 | 10.733 ± 5.850 | 11.114 ± 5.554 |
| p-Value | |||||||
|---|---|---|---|---|---|---|---|
| OAR | Parameter | CO-IMRT | CO-IMRT | CO-IMRT | NON-IMRT | NON-IMRT | CO-VMAT |
| PTV | CI | 0.006 | 0.066 | 0.173 | 0.298 | 0.167 | <0.001 |
| HI | 0.187 | 0.038 | 0.093 | 0.427 | 0.023 | <0.001 | |
| Lung | V5 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| V20 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | |
| Vmean | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | |
| Heart | V30 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| Vmean | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | |
| Spinal cord | Dmax | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| Breast | Dmean | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| V5 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | |
| V10 | <0.001 | 0.902 | <0.001 | 0.911 | <0.001 | 0.752 | |
| Esophagus | Dmax | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| Dmean | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | |
| NTCP (%) | |||||
|---|---|---|---|---|---|
| Technique | Lung | Heart | Spinal cord | Esophagus | Breast |
| CO-IMRT | 1.60 | 8.96 | 0.049 | 0.16 | 0.010 |
| NONCO-IMRT | 1.66 | 9.77 | 0.038 | 0.19 | 0.23 |
| CO-VMAT | 1.64 | 7.74 | 0.0079 | 0.10 | 1.75 |
| NONCO-VMAT | 1.58 | 8.84 | 0.0062 | 0.060 | 0.28 |
- —Natural Science Foundation of Hubei Province10.13039/501100003819
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMyasthenia Gravis and Thymoma · Meningioma and schwannoma management · Advanced Radiotherapy Techniques
Introduction
1
Thymomas and thymic carcinomas are rare mediastinal tumors that arise from thymic epithelial cells and account for 0.2%–1.5% of all malignancies (1, 2). Thymic carcinoma is more aggressive, accounting for approximately 20% of thymic epithelial tumors (3, 4). Surgery remains the primary treatment for thymoma; however, radiotherapy (RT) also plays an important role, particularly in adjuvant and palliative settings (5), due to the intrinsic radiosensitivity of these tumors. Adjuvant RT has been shown to improve overall survival (OS) in patients with Masaoka–Koga stage IIB disease or those with aggressive histologic subtypes following resection (6, 7). In cases where complete surgical resection is not feasible, postoperative RT may delay or prevent recurrence and prolong patients’ survival (8, 9). For thymic carcinoma, postoperative RT is often recommended even after complete resection, with RT being optional for stage I, advised for stage II, and strongly recommended for stage III/IV disease (10).
Minimizing radiation exposure to surrounding normal tissues is a major challenge in thymoma radiotherapy. Due to its location in the anterior mediastinum, conventional radiation plans typically adopt anterior beam arrangements, resulting in unavoidable exposure of adjacent critical organs such as the lungs, heart, and esophagus to radiation (11, 12). Among these, the lungs and heart are particularly susceptible to radiation-induced toxicity, with previous studies such as those by Jalbout et al. identifying the lungs as the organ at the greatest risk (13).
In recent years, several strategies have been explored to mitigate radiation-related toxicity in thymoma treatment. Techniques such as intensity-modulated proton therapy (IMPT) (14–17) and deep inspiration breath-hold (DIBH) (18) have demonstrated efficacy in reducing radiation doses to intrathoracic organs, thereby lowering the risk of late complications and secondary malignancies. However, widespread adoption of these approaches is limited by the high cost of proton facilities and the technical demands of DIBH, which requires patient compliance and dedicated respiratory-gating systems. In numerous resource-limited centers, these technologies are not readily accessible.
As an alternative, modifying beam geometry, specifically through non-coplanar radiotherapy techniques, offers a more practical means of reducing organ-at-risk (OAR) doses (19). Non-coplanar intensity-modulated radiation therapy (NONCO-IMRT) employs radiation beams delivered from multiple non-parallel planes, improving dose conformity by reducing the overlap of entrance and exit doses through critical structures (20). Dong et al. reported that in stereotactic body radiotherapy (SBRT) for lung tumors, NONCO-IMRT allowed for a 20-Gy increase in tumor dose compared to volumetric-modulated arc therapy (VMAT) while still respecting standard OAR dose constraints (21). Some studies have also suggested that non-coplanar planning may increase lung V_5_ but reduce lung V_10_ and V_20_, potentially offering better sparing of lung tissue compared to conventional coplanar IMRT (CO-IMRT) (22).
However, studies on non-coplanar VMAT (NONCO-VMAT) in thymomas are relatively scarce. This study aimed to explore the dosimetric differences between non-coplanar plans in IMRT and VMAT while analyzing the normal tissue complication probability (NTCP) of OARs in different plans. The aim of this study was to clarify the advantages and disadvantages of non-coplanar plans in radiation therapy for thymoma.
Methods
2
Patient selection and data collection
2.1
All procedures were conducted in accordance with relevant guidelines and institutional regulations. Overall, 48 patients diagnosed with thymoma or thymic carcinoma who received postoperative radiotherapy between 2019 and 2025 were retrospectively included in this study. The cohort comprised 24 male and 24 female patients, with a median age of 53 years (range, 27–70 years). Among them, 30 patients were diagnosed with thymomas, including 23 with Masaoka–Koga stage II and seven with stage III disease. The remaining 18 patients had thymic carcinoma, of whom nine were stage II, seven were stage III, and two were stage IV. All radiotherapy regimens for the enrolled patients were determined after evaluation by the multidisciplinary team for thymic tumors at our hospital.
This study was designed as a retrospective study and aimed to compare the dosimetric differences among various radiotherapy techniques. The study did not involve direct contact with the patients and was a non-interventional retrospective study. Therefore, it was approved by the Medical Ethics Committee of Jingzhou First People's Hospital (KY202405) and the need for obtaining informed consent from the participants was waived. The study was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki.
All patients underwent CT simulation with a slice thickness of 5 mm, and the images were transferred to the uRT-TPOIS treatment planning system for further planning.
Target volumes and OAR delineation
2.2
The gross tumor volume (GTV) was defined as the visible tumor bed or residual lesion on postoperative imaging. The clinical target volume (CTV) was generated by expanding the GTV by 0.5 cm to include areas of potential microscopic disease, such as adjacent thymic tissues or potentially involved structures. The planning target volume (PTV) was created by further expanding the CTV by 0.5 cm to account for setup and motion uncertainties. OARs delineated included the bilateral lungs, heart, esophagus, and spinal cord.
Treatment planning and beam configuration
2.3
Treatment plans were generated using the uRT-TPOIS system (United Imaging, Shanghai, China) and delivered on a uRT linac 506c linear accelerator (United Imaging, Shanghai, China). All plans utilized 6-MV photon beams, and dose calculations were performed using the Monte Carlo method. Forty-six patients received adjuvant radiotherapy, with no residual lesions. The prescribed dose was 50 Gy in 25 fractions. The remaining two patients with stage IV thymic carcinomas were initially planned to first receive 50 Gy in 25 fractions, with an intended subsequent cone-down boost to 66 Gy based on tumor response. However, after completing 50 Gy, radiation pneumonitis was observed on follow-up imaging, and further boosts were discontinued. These two cases were still included in the present dosimetric comparison, as they received the initial 50 Gy course.
Each patient underwent four treatment planning approaches: CO-IMRT, NONCO-IMRT, coplanar VMAT (CO-VMAT), and NONCO-VMAT. For all plans, the dose to 95% of the PTV (V95%) was required to cover at least 99% of the prescribed dose. Additionally, dose distributions to the lungs, heart, and spinal cord were evaluated for comparison. The dose constraint parameters for organs at risk are shown in Table 1.
CO-IMRT included five beam angles—330°, 345°, 0°, 15°, and 30°—all with a couch angle of 0°. For NONCO-IMRT, three fields (330°, 0°, and 30°) remained coplanar (couch angle 0°), while the other two fields used the same gantry angles (330° and 30°) but were delivered with a couch angle of 270°. CO-VMAT included a double arc, an angle of 275°–85°, and a couch angle of 0°. In NONCO-VMAT, two arc angles were 300°–60° with a bed angle of 0, two arc angles of 330°–30°, and a couch angle of 90°. All modalities involved avoiding mechanical collisions during delivery.
Dosimetric evaluation and indices
2.4
Dosimetric assessment included both target conformity and dose to OARs. The conformity index (CI) was calculated as the ratio of the PTV covered by the 95% isodose line to the total PTV. A CI value close to 1 indicates optimal conformity. In this study, all plans achieved a CI exceeding 0.99. . D2% and D98% represent the high and low dose absorption regions of PTV, respectively (23). A lower HI value indicates a more uniform dose distribution within the target area.
For OARs, the following parameters were analyzed: whole lung V_20_, V_5_, and D_mean_; heart V_30_ and D_mean_; breast D_mean_; esophagus D_max_; and spinal cord D_max_.
Radiobiological parameters
2.5
The Lyman–Kutcher–Burman (LKB) NTCP model describes the NTCP as an organ or tumor sub-volume function that receives a uniform dose (24) of radiation. Because the dose distribution is heterogeneous in clinical treatment, a dose–volume histogram (DVH)-reduction method with the concept of Equivalent Uniform Dose (EUD) is typically employed (25). EUD represents a single uniform dose value equivalent to the biological effect of the non-uniform dose distribution delivered to an organ or tumor.
where v_i_ is the relative volume receiving the corresponding ith dose bin with the dose D_i_ of a differential DVH. The parameter D50 is the dose that corresponds to a 50% probability of complication, m is the slope of the NTCP curve, and n represents the volume dependency of the risk of complications (26). The parameters employed for calculating the NTCP of the lungs, heart, spinal cord, breast, and esophagus are shown in Table 2 (27–30).
Statistical analysis
2.6
The statistical analysis was performed using the SPSS version 17.0 software. Data were represented as (x ± s). Paired comparisons between different plans were conducted using the Student–Newman–Keuls (SNK-q) test. A two-sided p-value <0.05 was considered statistically significant.
Results
3
Planning dose parameters
3.1
Table 3 summarizes the dosimetric parameters, including the dose of CI and HI of the PTV, as well as a comparison with the doses of normal organs. Table 4 presents the statistical comparison of the target volumes and OAR doses among the four radiotherapy techniques for thymomas.
The differences in PTV dose parameters among the four plans were minimal, with statistical significance only observed between CO-VMAT and NONCO-VMAT. Regarding the breast V_10_, no statistical significance was found in the comparisons of CO-IMRT vs. CO-VMAT and CO-VMAT vs. NONCO-VMAT. For other comparisons between plans, the doses to OARs showed significant statistical differences (p < 0.001). The lung V_20_ values of CO-VMAT and NONCO-VMAT (9.465 and 9.461, respectively) were significantly lower than those of IMRT techniques (11.694 for CO-IMRT and 11.018 for NONCO-IMRT). The differences in lung V_5_ and lung V_mean_ among the four techniques were also small. VMAT showed a slight advantage in lung V_mean_, with the lowest value of 6.694 observed in NONCO-VMAT. IMRT showed a slight advantage in lung V_5_, with the lowest value of 30.742 observed in CO-IMRT.
The heart V_30_ values of CO-VMAT (7.897) and NONCO-VMAT (8.408) were significantly lower than those of IMRT techniques (11.550 for CO-IMRT and 11.162 for NONCO-IMRT). The heart D_mean_ of VMAT plans was also lower than that of IMRT plans. Among them, CO-VMAT (6.664) had the lowest heart D_mean_, outperforming other techniques.
The spinal cord D_max_ of VMAT techniques (24.073 for CO-VMAT and 24.316 for NONCO-VMAT) was lower than that of IMRT techniques (28.909 for CO-IMRT and 28.23 for NONCO-IMRT). Regarding the esophagus D_max_, VMAT techniques (37.246 for CO-VMAT and 38.246 for NONCO-VMAT) also showed lower values compared to IMRT techniques (≈39.99). Additionally, the esophagus D_mean_ of VMAT plans was lower, with CO-VMAT achieving the lowest value (10.733).
The breast D_mean_ (6.786), V_5_ (35.888), and V_10_ (24.729) of CO-VMAT were significantly higher than those of other techniques. The breast parameters of NONCO-VMAT (D_mean_ of 3.587, V_5_ of 16.690, and V_10_ of 12.295) were superior to those of CO-VMAT and even close to those of IMRT techniques.
Figure 1 shows the mean DVHs of the PTV and the mean DVH of key organs for patients in the CO-IMRT, NONCO-IMRT, CO-VMAT, and NONCO-VMAT. Figure 2 presents the typical dose distributions around the target volume when female thymoma patients receive different radiotherapy techniques.
DVH average of 48 patients for PTV and critical organs in CO-IMRT, NONCO-IMRT, CO-VMAT, and NONCO-VMAT plans. DVH, dose–volume histogram; PTV, planning target volume; IMRT, intensity-modulated radiation therapy; CO-IMRT, coplanar IMRT; NONCO-IMRT, non-coplanar IMRT; VMAT, volumetric-modulated arc therapy; CO-VMAT, coplanar VMAT; NONCO-VMAT, non-coplanar VMAT.
Typical dose distributions around the target volume when female thymoma patients receive different radiotherapy techniques: (a) CO-IMRT, (b) NONCO-IMRT, (c) CO-VMAT, and (d) NONCO-VMAT. The red, orange, green, yellow, light blue, and dark blue colors represent the isodose lines of 50, 45, 30, 20, 10, and 5 Gy, respectively. IMRT, intensity-modulated radiation therapy; CO-IMRT, coplanar IMRT; NONCO-IMRT, non-coplanar IMRT; VMAT, volumetric-modulated arc therapy; CO-VMAT, coplanar VMAT; NONCO-VMAT, non-coplanar VMAT.
Radiobiological parameters
3.2
Using the mean DVH of the four plans, the NTCP of OARs for the four different radiotherapy techniques was calculated, as shown in Table 5. Among the four plans, the lung NTCP of CO-VMAT was the lowest (1.58%); however, the overall difference was small (ranging from 1.58% to 1.66%). The heart NTCP of VMAT plans (7.74% for CO-VMAT and 8.84% for NONCO-VMAT) was lower than that of IMRT plans (8.96% for CO-IMRT and 9.77% for NONCO-IMRT). The spinal cord NTCP of VMAT plans (0.0079% for CO-VMAT and 0.0062% for NONCO-VMAT) was significantly lower than that of IMRT plans (0.049% for CO-IMRT and 0.038% for NONCO-IMRT); however, all values were far below the clinical warning threshold. The esophagus NTCP of VMAT plans (0.10% for CO-VMAT and 0.06% for NONCO-VMAT) was lower than that of IMRT plans (0.16% for CO-IMRT and 0.19% for NONCO-IMRT). The breast NTCP of CO-VMAT (1.75%) was significantly higher than that of other plans. The breast NTCP of CO-IMRT (0.01%) was much lower than that of other plans, while the breast NTCPs of NONCO-IMRT (0.23%) and NONCO-VMAT (0.28%) were similar.
Discussion
4
This study compared four radiotherapy planning schemes for the treatment of thymomas, including CO-IMRT, NONCO-IMRT, CO-VMAT, and NONCO-VMAT, for administering the same prescribed dose of 50 Gy/25 f. All plans were formulated with priority given to meeting the prescribed dose. The optimization criteria for OARs were consistent across the four plans for the same patient.
All four plans achieved excellent conformity (CI > 0.99) and satisfactory uniformity (HI 0.081–0.090) for the PTV, indicating that each technique can effectively deliver the prescribed dose to the target. This aligns with the primary goal of radiotherapy, ensuring adequate tumor control, while confirming that both IMRT and VMAT, whether coplanar or non-coplanar, are capable of meeting clinical target dose requirements for thymomas.
The most striking findings lie in the differential sparing of OARs across techniques, with VMAT (both CO-VMAT and NONCO-VMAT) generally outperforming IMRT in protecting critical structures, including the heart, spinal cord, and esophagus, while showing mixed results for the lungs and breasts.
VMAT techniques (CO-VMAT and NONCO-VMAT) significantly reduced lung V_20_ compared to IMRT techniques (9.46 vs. 11.02–11.69), a parameter strongly associated with radiation-induced pneumonitis risk (13, 26). Although lung V_5_ and V_mean_ showed smaller differences, the reduction in V_20_ was clinically meaningful, as V_20_ > 30% is a well-established predictor of pneumonitis. This aligns with the findings of previous studies suggesting that arc-based techniques (VMAT) can reduce high-dose lung exposure by optimizing beam angles to avoid overlapping with lung tissue (21).
VMAT plans (especially CO-VMAT) achieved lower heart V_30_ and D_mean_ than IMRT, with CO-VMAT reducing V_30_ by 30% (7.90 vs. 11.16–11.55). Given that heart V_30_ is linked to major adverse cardiac events (MACEs) (27), this reduction could translate to lower long-term cardiac toxicity, a critical consideration for patients with thymomas who often have prolonged survival.
VMAT techniques consistently reduced maximum doses to the spinal cord (24.07–24.32 vs. 28.23–28.91 Gy) and esophagus (37.25–38.25 vs. ~39.99 Gy) compared to IMRT. These findings support the utility of VMAT in sparing posterior (spinal cord) and central (esophagus) structures; moreover, more irradiation angles of VMAT technology make the medium- and high-dose curves wrap more closely.
A key exception was the breast, where CO-VMAT showed significantly higher D_mean_, V_5_, and V_10_ compared to other techniques. This likely stems from the arc angles used in CO-VMAT (275°–85° with 0°couch), which may irradiate more breast tissue in anterior mediastinal targets, particularly in female patients. Figure 2 shows that the 5-Gy dose range of the CO-VMAT program covers more of the breast. In contrast, NONCO-VMAT (incorporating 90°couch angles) mitigated this effect, with breast parameters comparable to those of IMRT, highlighting the value of non-coplanar beam geometry in reducing unnecessary breast exposure, which is an important consideration for younger female patients at risk of breast fibrosis (29).
To assess the specific impact of dose differences on patients’ side effects, it was also necessary to combine the measurement of radiobiological indices. This study calculated the NTCP caused by thymoma radiotherapy to the lungs, heart, spinal cord, esophagus, and breasts, which correspond to pneumonia, major adverse cardiac events, myelopathy, grade 2 esophagitis, and fibrosis, respectively. The NTCP results were consistent with the dosimetric results. The VMAT plans also showed a lower complication risk for most OARs. Lung NTCP was the lowest in NONCO-VMAT (1.58%), consistent with its favorable V_20_. Heart NTCP was reduced in VMAT (7.74%–8.84% vs. 8.96%–9.77% in IMRT), aligning with lower V_30_ and D_mean_. Spinal cord NTCP was negligible across all plans but significantly lower in VMAT (0.0062%–0.0079% vs. 0.038%–0.049% in IMRT), confirming effective sparing. Esophagus NTCP was the lowest in NONCO-VMAT (0.06%), reflecting reduced D_max_ and D_mean_. The elevated breast NTCP in CO-VMAT (1.75%), compared to values of 0.01%–0.28% in other plans, further underscores the need to avoid excessive breast irradiation in clinical practice, particularly for female patients.
Our findings build on prior research on non-coplanar techniques and VMAT in thoracic malignancies. Dong et al. reported that non-coplanar IMRT (NONCO-IMRT) improved the protection of OARs in lung SBRT (21). This study extends this application to thymomas, showing that NONCO-VMAT is superior to CO-VMAT in balancing target volume coverage and breast protection. Furthermore, the advantage of VMAT in reducing the doses to the heart and spinal cord was consistent with the findings of studies on lung cancer and esophageal cancer, which reported that arc-based techniques can minimize the radiation dose received by adjacent structures (19, 22). He et al. (31) found that CO-VMAT plans increased the radiation dose to the breasts, which is consistent with the results of our study. However, our study further demonstrates that NONCO-VMAT can significantly reduce the breast dose in VMAT plans while maintaining other dosimetric advantages of VMAT plans.
This study has several limitations. The study’s retrospective design and small cohort of only 48 patients may introduce selection bias; therefore, larger prospective cohorts are needed to validate clinical outcomes (e.g., pneumonitis and cardiac events). NTCP calculations relied on the Lyman model with parameters from other tumor types (26–29); therefore, thymoma-specific NTCP parameters were lacking and warrant further investigation. The findings of this study inspire us to explore new techniques that could be extended to patients with locally advanced, non-surgical thymoma or thymic carcinoma. In such cases, the target volumes are typically larger and more irregular in shape and may have more complex relationships with adjacent OARs. Evaluating whether different radiotherapy techniques, particularly non-coplanar VMAT, can retain their superior protective capacity for OARs while ensuring target dose coverage in these more complex clinical scenarios would be of significant clinical value.
Conclusion
5
In summary, all four radiotherapy techniques achieved adequate target coverage for thymomas; however, VMAT, particularly NONCO-VMAT, offered superior OAR sparing for the heart, spinal cord, esophagus, and lungs, with balanced breast protection. These findings support the use of NONCO-VMAT as a treatment option for most patients with thymoma, especially those requiring heart and spinal cord sparing, while CO-VMAT may be avoided in female patients due to the associated higher breast dose.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Carter BW Marom EM Detterbeck FC . Approaching the patient with an anterior mediastinal mass: a guide for clinicians. J Thorac Oncol. (2014) 9:S 102–S 9. doi: 10.1097/JTO.0000000000000294, PMID: 25396306 · doi ↗ · pubmed ↗
- 2Rich AL . Epidemiology of thymoma. J Thorac Dis. (2020) 12:7531–5. doi: 10.21037/jtd-2019-thym-02, PMID: 33447443 PMC 7797839 · doi ↗ · pubmed ↗
- 3Ahmad U Yao X Detterbeck F Huang J Antonicelli A Filosso PL . Thymic carcinoma outcomes and prognosis: results of an international analysis. J Thorac Cardiovasc Surg. (2014) 149:95–101.e 2. doi: 10.1016/j.jtcvs.2014.09.124, PMID: 25524678 · doi ↗ · pubmed ↗
- 4Ruffini E Detterbeck F Van Raemdonck D Rocco G Thomas P Weder W . Thymic carcinoma: a cohort study of patients from the European Society of Thoracic Surgeons database. J Thorac Oncol. (2014) 9:541–8. doi: 10.1097/JTO.0000000000000128, PMID: 24736078 · doi ↗ · pubmed ↗
- 5Komaki R Gomez DR . Radiotherapy for thymic carcinoma: adjuvant, inductive, and definitive. Front Oncol. (2013) 3:330. doi: 10.3389/fonc.2013.00330, PMID: 24455488 PMC 3887269 · doi ↗ · pubmed ↗
- 6Tateishi Y Horita N Namkoong H Enomoto T Takeda A Kaneko T . Postoperative radiotherapy for completely resected Masaoka/Masaoka-Koga stage II/III thymoma improves overall survival: an updated meta-analysis of 4746 patients. J Thorac Oncol. (2021) 16:677–85. doi: 10.1016/j.jtho.2020.12.023, PMID: 33515812 · doi ↗ · pubmed ↗
- 7Zhang C Wang Q Hu L Cong Z Qiang Y Xu F . The prognostic value of postoperative radiotherapy for thymoma and thymic carcinoma: a propensity-matched study based on SEER database. Cancers (Basel). (2022) 14:4938. doi: 10.3390/cancers 14194938, PMID: 36230861 PMC 9563976 · doi ↗ · pubmed ↗
- 8Jackson MW Palma DA Camidge DR Jones BL Robin TP Sher DJ . The impact of postoperative radiotherapy for thymoma and thymic carcinoma. J Thorac Oncol. (2017) 12:734–44. doi: 10.1016/j.jtho.2017.01.002, PMID: 28126540 · doi ↗ · pubmed ↗