Impact of a Structured Training Program on Medical Student Confidence and Behavior During Their First Radial Arterial Puncture: Comparative Study
Camille Rolland-Debord, Lucien Juret, Mathilde Simon, Abdallah El Mouhajer, Cécile Londner, Capucine Morélot-Panzini, Cécile Chenivesse, Thomas Similowski

TL;DR
A structured training program for medical students improved their confidence and reduced use of anesthesia during first radial artery punctures, despite similar anxiety levels.
Contribution
Demonstrates that structured simulation-based training alters student behavior during clinical procedures, even without changing self-reported confidence.
Findings
Students in the structured training group were significantly less likely to use local anesthesia during their first radial artery puncture.
Behavioral indicators suggested improved self-efficacy despite similar self-reported apprehension between groups.
First-attempt success rates were comparable between the trained and control groups.
Abstract
Radial artery puncture is a common clinical procedure essential for assessing gas exchange but is frequently perceived as stressful by inexperienced operators, who fear causing pain to their patients. Despite its practical relevance, formal training in this procedure is inconsistently integrated into medical curricula. This study evaluated whether a structured training program—combining theoretical instruction, simulation-based practice, and debriefing—could influence students’ procedural confidence and decision-making and patient experience during their first clinical arterial puncture. This study aimed to determine whether structured simulation-based training influences medical students’ anxiety, confidence, and technical performance and patient experience during their first arterial puncture. Third-year medical students who had never performed an arterial puncture were assigned to…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
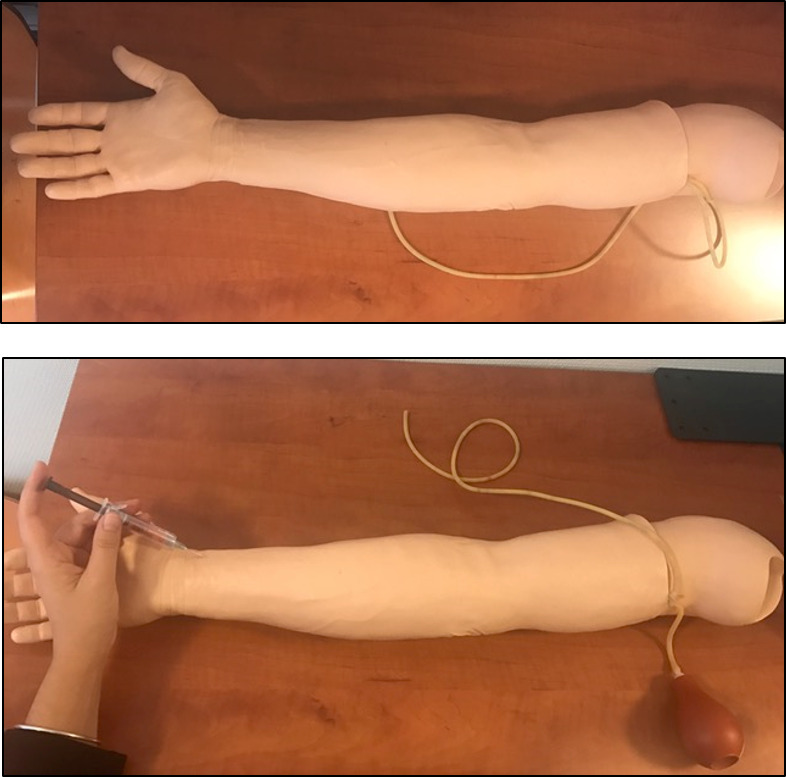 Figure 1
Figure 1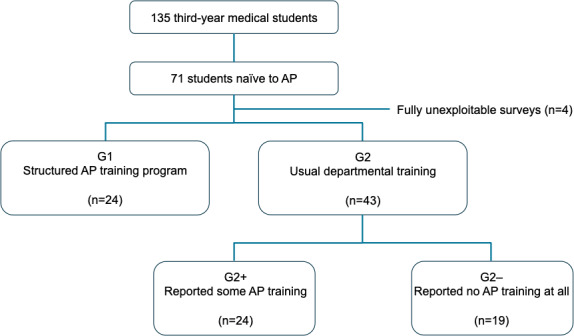 Figure 2
Figure 2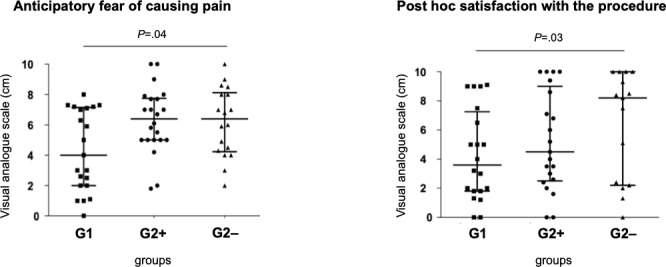 Figure 3
Figure 3| Group 1, median (IQR) | Group 2, median (IQR) | ||
|---|---|---|---|
| Global anticipatory apprehension | 4.1 (2.2-5.0) | 4.0 (2.0-5.6) | .67 |
| Apprehension about causing pain | 5.0 (2.3-7.2) | 5.0 (3.1-6.9) | .60 |
| Apprehension about procedure failure | 4.3 (2.3-6.2) | 4.4 (2.0-6.9) | .84 |
| Satisfaction with the procedure | 3.6 (1.8-7.3) | 5.6 (2.4-9.4) | .09 |
| Apprehension about repeating the procedure | 1.9 (0-4.6) | 2.3 (0.3-3.9) | .87 |
| Confidence in repeating the procedure | 7.0 (5.1-7.8) | 6.0 (4.4-8.0) | .80 |
| Group 1, median (IQR) | Group 2–, median (IQR) | ||
|---|---|---|---|
| Global anticipatory apprehension | 4.2 (1.0-6.1) | 4.7 (1.7-6.2) | .44 |
| Apprehension about causing pain | 4.0 (2.0-7.0) | 6.4 (4.2-8.5) | .04 |
| Apprehension about procedure failure | 5.0 (3.0-7.0) | 5.2 (3.0-7.2) | .56 |
| Satisfaction with the procedure | 3.6 (1.8-7.2) | 8.2 (2.3-10.0) | .03 |
| Apprehension about repeating the procedure | 1.8 (0-4.6) | 2.5 (1.0-3.8) | .58 |
| Confidence in repeating the procedure | 7.0 (5.0-7.7) | 6.0 (5.0-9.2) | .87 |
| Without prior anesthesia, median (IQR) | With prior anesthesia, median (IQR) | ||
|---|---|---|---|
| Patients | |||
| Anticipatory apprehension | 4 (2-6.2) | 3 (1.5-5.7) | .50 |
| Procedural pain | 4.8 (2.1-6.4) | 2.1 (1.2‐4) | .08 |
| Students | |||
| Global anticipatory apprehension | 3.8 (1.8-5.8) | 4.1 (2-5.1) | .89 |
| Apprehension about causing pain | 5 (2-7.3) | 5 (3.4-6.9) | .57 |
| Apprehension about procedure failure | 4.3 (2-7.2) | 4.4 (2-6.2) | .82 |
| Satisfaction with the procedure | 4 (2-9) | 5.1 (2‐8.8) | .61 |
| Apprehension about repeating the procedure | 1.9 (0-5) | 2.4 (0-4.1) | .93 |
| Confidence in repeating the procedure | 7.1 (5.3-8.6) | 5.4 (4.3-7.9) | .07 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSimulation-Based Education in Healthcare · Pediatric Pain Management Techniques · Intramuscular injections and effects
Introduction
Performing a radial arterial puncture to assess gas exchange can be challenging for medical and nursing students due to the risk of causing significant pain at a small puncture site densely packed with nociceptive C-fiber–containing structures, including the artery itself and nearby tissues such as the periosteum [12]. Several studies have explored strategies to improve patient tolerance. Topical anesthetics have shown limited effectiveness [34], and cryoanalgesia, though promising, is seldom used [5]. Local infiltration anesthesia offers the greatest pain reduction but is considered impractical and is infrequently applied [6-8]. Moreover, reducing needle gauge does not alleviate pain and may prolong the procedure [9]. Patout et al [9] demonstrated that preprocedural anxiety in patients significantly correlates with increased pain perception during radial arterial puncture. Importantly, patient anxiety is likely to be heightened by the anxiety of the operator, whose fear of causing discomfort can lead to anticipatory stress. This, in turn, may further complicate the procedure, creating a vicious circle that amplifies the risk of pain.
Structured training programs have been shown to reduce anxiety and build confidence in nursing [1011] and medical students [12-14] performing clinical procedures. In the particular case of radial arterial puncture, Collins et al [13] implemented a 5-step curriculum for respiratory care students combining theory, simulation, and peer assessment, which resulted in high interrater performance scores. Similarly, simulation-based training has been shown to enhance confidence and technical skills in core procedures among medical students, including those involving invasive techniques [1516].
In this context, we conducted a national survey of arterial puncture teaching practices in French pneumology departments and found that only a minority used structured programs to train medical students (Multimedia Appendix 1). At our own institution, a systematic observation of unsupervised arterial puncture attempts by third-year medical students on a simulator revealed a high frequency of procedural errors (Multimedia Appendix 1).
Building on these observations and the available literature, we designed a structured training program combining theoretical instruction, simulation-based practice, and supervised hands-on experience. The aim of this study was to evaluate whether adding a structured theoretical and simulation-based training session influenced medical students’ procedural confidence, preprocedural anxiety, and first-attempt performance during radial arterial puncture compared with usual heterogeneous bedside teaching. We hypothesized that structured preparation would be associated with increased confidence and reduced anxiety, as well as a possible improvement in performance.
Methods
Ethical Considerations
This study was approved by the institutional review board of the National Institute of Health and Medical Research (reference IRB00003888). All data were collected anonymously, and no personal identifiers were recorded at any stage. Informed consent was obtained from all participants prior to study participation. Participation was voluntary, and students could decline or withdraw at any time without any academic or clinical consequences. No financial or other compensation was provided for participation.
Recruitment Procedure
This study was conducted in hospitals affiliated with the Faculty of Health, Sorbonne University, one of the medical schools in the Paris area.
All third-year medical students (General Medical Sciences Diploma) completing a 3-month clinical rotation in pulmonology were eligible for inclusion if they performed their first arterial puncture on a patient and had not previously received simulation-based training for this procedure. Each eligible student was invited to complete the online questionnaire within 24 hours of performing the procedure (Multimedia Appendix 1). At the time of rotation assignment, students selecting a pulmonology placement were verbally informed that they would be invited to complete a short online questionnaire after performing their first arterial puncture. This information was reiterated at the beginning and end of the rotation and again during the end-of-semester pulmonology examination. At the start of each rotation, senior physicians in the participating departments were informed of the study via email and provided with a link to the questionnaire for distribution to their students. Data were collected using an online questionnaire specifically developed for this study and hosted on the SurveyMonkey platform (SurveyMonkey Inc; Multimedia Appendix 1). The initial draft was developed by the study investigators and reviewed for face and content validity by a panel of 5 academic pulmonologists and medical educators from Sorbonne University. The instrument was pilot-tested among medical students before implementation.
Student Groups
Overview
Students were assigned to groups based solely on their clinical placement independently of the study investigators. Both groups followed the usual teaching of their respective departments. These practices were heterogeneous and could involve bedside instruction by a nurse, a more senior medical student, a resident, or an attending physician. In some cases, students were verbally instructed before entering the patient’s room or performed the procedure after having observed it on another patient. No intervention was made to modify these existing teaching practices. Regarding the clinical procedure itself, the use of topical anesthesia was left up to the students in accordance with local departmental policies. The students were divided as follows:
Group 1—students rotating in the respiratory medicine department of Pitié-Salpêtrière Hospital, Sorbonne University, who received the usual teaching plus an additional structured training program before their first arterial punctureGroup 2—students rotating in other respiratory medicine departments of Sorbonne University who received usual teaching only
For sensitivity analysis, group 2 was then subdivided into students who had received bedside demonstration or guidance before their first arterial puncture (group 2+) and those who had not (group 2−). This subdivision allowed us to capture the full spectrum of existing informal learning situations within the “usual practice” group.
Structured Training Program (Group 1)
Overview
Students in group 1 participated in a structured theoretical and practical training session that had been routinely implemented in the department in previous years. The session was delivered by a single instructor and organized into 2 groups of approximately 7 students each. The total duration varied slightly between sessions but was at least 1 hour. The session began with a structured discussion of the indications and techniques for arterial puncture, followed by a briefing outlining the simulation objectives, procedural steps to be reproduced, and key safety principles.
Theoretical Component
A dedicated slide deck (Multimedia Appendix 1) was developed based on the New England Journal of Medicine resource on radial artery puncture [17] incorporating annotated screenshots from the procedural video. The content was reviewed for accuracy and pedagogical coherence by 5 academic pulmonologists. Each student received a printed copy of the material at the end of the session and was granted permanent online access.
Practical Component
The practical portion of the session consisted of individual hands-on training using an artificial arm simulator (Laerdal Medical; Figure 1), which allowed for palpation of a simulated pulse and visualization of arterial blood return. Each student repeated the procedure until they achieved self-reported confidence.
Procedural arm simulator with a pseudopulsatile artery and circulating red liquid (Laerdal Medical).
Procedural steps were practiced systematically, including patient communication, site preparation, needle positioning and insertion, troubleshooting in case of failure, and needle disposal. Students were encouraged to observe and discuss each other’s attempts to reinforce learning through peer observation.
Peer-to-peer exercises were also incorporated, including palpation of the radial artery groove, performance of the Allen test, patient communication, and patient positioning and preparation.
A standardized communication script (Multimedia Appendix 1) written and reviewed by the same 5 academic pulmonologists was introduced and read aloud by the instructor and then practiced in pairs by students. Each participant received a printed copy for review before performing the procedure in a clinical setting. The script included a standard introduction, an explanation of the procedure, information regarding expected discomfort, and clarification about the absence of unambiguously validated analgesic strategies.
Structured Debriefing
Each session concluded with a structured debriefing conducted according to the Haute Autorité de Santé simulation guidelines. Students were first invited to express their emotions and initial impressions (reaction); then analyze their actions and underlying reasoning (analysis); and, finally, summarize key learning points and objectives for improvement (synthesis). Incorrect decisions or technical errors were explored to identify their causes and were addressed through guided feedback, theoretical reinforcement, and targeted procedural adjustments. Throughout the session, the instructor fostered psychological safety; encouraged self-assessment; used open-ended questioning; and provided constructive, nonjudgmental feedback.
At the conclusion of the session, students were reminded that they would later be asked to complete an online questionnaire following their first arterial puncture on a patient.
Usual Teaching Only (Group 2)
Students in group 2 received the usual teaching routinely provided in the departments to which they had been assigned. Teaching practices varied and could include bedside instruction and/or verbal explanations given before entering the patient’s room. Instruction could be provided by a nurse, a senior medical student, a resident, or an attending physician. In some cases, students performed the procedure after first observing it on another patient. No intervention was introduced to modify these usual teaching practices.
Evaluation Criteria
Evaluation criteria included several dimensions of student and patient experience. For students, the following variables were assessed: global anticipatory apprehension, apprehension about causing pain, apprehension about procedural failure, satisfaction with the procedure, apprehension about repeating the procedure, and confidence in performing it again. The decision to use topical anesthesia was also recorded, as well as the success rate of the arterial puncture. For patients, perceptions of the procedure were evaluated through 2 measures: anticipatory apprehension and pain experienced during the puncture. Both students and patients rated their perceptions using a 10-cm visual analogue scale (VAS) ranging from 0 (“none at all”) to 10 (“maximum imaginable”).
Statistical Analysis
Statistical analyses were performed using Prism (GraphPad Software). Categorical variables were reported as counts and percentages, whereas continuous variables were presented as means and SDs or medians and IQRs depending on their distribution. Given the limited sample size and the ordinal nature of several variables, nonparametric statistics were used. The primary analysis compared group 1 and group 2. Group comparisons were conducted as follows: (1) categorical variables were compared using the Fisher exact test, and (2) continuous variables were compared using the Mann-Whitney U test. A sensitivity analysis was performed to compare group 1 with the group 2 subgroups: group 2+ (students who received prior training) and group 2− (students who did not receive prior training). All tests were 2 sided, with the type I error rate set at α=.05.
Results
Participants
During the study period, 135 third-year medical students were assigned to the participating departments. Of these 135 students, 71 (52.6%) were entirely naive to arterial puncture and performed their first procedure during their rotation (Figure 2). The cohort included 78.9% (56/71) women and 21.1% (15/71) men, with a median age of 21 (IQR 20‐21) years; 90.1% (64/71) were right-handed. A total of 83.1% (59/71) had previously observed an arterial puncture performed by a nurse or physician. All participants began completing the survey immediately after the procedure, but 21.1% (15/71) submitted incomplete responses. These included 16.7% (4/24) of the students from group 1, a total of 16.3% (7/43) from group 2, and 5.6% (4/71) whose group affiliation could not be determined. These cases were excluded from analysis, yielding a final sample of 67 students. Group 1 included 35.8% (24/67) of the students. Among the 43 students in group 2, a total of 19 (44.2%) reported having received no prior training (group 2−), and 24 (55.8%) reported some form of training (group 2+), which typically consisted of theoretical explanations and observation of procedures performed by nurses, senior students, or physicians.
Flowchart of the study. AP: arterial puncture; G1: students assigned to the combined theoretical and practical structured AP training program; G2: students assigned to usual teaching; G2+: subgroup of G2 consisting of students who reported receiving some prior AP training; G2−: subgroup of G2 consisting of students who reported receiving no prior AP training at all.
Attendants
In total, 92.9% (52/56) of the students were accompanied during their first arterial puncture (19/19, 100% in the group 2− subgroup). Attendants were nurses in 52.2% (35/67) of cases, medical trainees in 31.3% (21/67) of cases (including fourth- to sixth-year medical students and residents more advanced in training than the study participants, who were all in their third year), and senior physicians in the remaining 16.4% (11/67) of cases.
Medical Students’ Perceptions
No statistically significant differences were observed between group 1 and group 2 in terms of global anticipatory apprehension, apprehension about causing pain, apprehension about procedural failure, satisfaction with the procedure, apprehension about repeating the procedure, or confidence in repeating the procedure (Table 1). However, anticipatory apprehension about causing pain was significantly lower in group 1 compared to group 2− (median 4.0, IQR 2.0‐7.0 vs median 6.4, IQR 4.2‐8.5; P=.04; Table 2 and Figure 3). Conversely, postprocedure satisfaction was significantly higher in group 2− than in group 1 (median 8.2, IQR 2.3‐10.0 vs median 3.6, IQR 1.8‐7.2; P=.03; Table 2 and Figure 3).
Sensitivity analysis. G1: students assigned to the combined theoretical and practical structured arterial puncture training program; G2+: subgroup of group 2 consisting of students who reported receiving some prior arterial puncture training; G2−: subgroup of group 2 consisting of students who reported receiving no prior arterial puncture training at all.
Use of Topical Anesthesia
Overall, 62.5% (35/56) of the students elected to use anesthesia before performing the arterial puncture. Among them, 45.7% (16/35) used an EMLA 5% patch, 51.4% (18/35) used EMLA 5% cream, and 2.9% (1/35) used subcutaneous lidocaine. Anesthesia use was significantly less frequent in group 1 compared to group 2 (7/20, 35% vs 28/36, 77.8%; P=.003). The use of anesthesia did not lead to statistically significant differences in students’ perceptions or patients’ reported experiences, although procedural pain and self-reported confidence showed nonsignificant trends (Table 3).
Arterial Puncture Success
The first-attempt success rate was 23.1% (3/13) in group 1 and 48.3% (14/29) in group 2 (P=.18). Within group 2, students with no prior training (group 2−) achieved a notably higher first-attempt success rate than those with some prior training (group 2+): 71.4% (10/14) vs 28.6% (4/14), respectively (P=.06). The overall success rate within the first 3 attempts was 65% (13/20) in group 1 and 80.6% (29/36) in group 2 (P=.20). The median number of attempts required for success was significantly higher in group 1 than in group 2 (median 1, IQR 0.5‐2 vs median 1, IQR 0‐1; P=.02). The number of procedures requiring supervisor intervention after 3 failed attempts was identical in both groups (7/20, 35% and 7/36, 19.4%).
Patient Description and Experiences
Arterial punctures were performed by students on 61 patients (median age 65, IQR 57‐76 years; n=38, 62.3% women and n=23, 37.7% men). The number of patients (n=61) was lower than the number of participating students because some students performed their first arterial puncture on the same patient for logistical reasons. A total of 26.2% (n=16) of the patients were receiving oral analgesics, primarily paracetamol. Most patients (n=41, 67.2%) had previously undergone multiple radial arterial punctures.
Overall, anticipatory apprehension was rated at a median of 3.5 (IQR 2.0‐6.0) on the VAS, with no statistically significant difference between patients who did not receive anesthesia and those who did (median 4.0, IQR 2.0‐6.2 vs median 3.0, IQR 1.5‐5.7; P=.50). Overall procedural pain was rated at a median of 2.7 (IQR 1.2‐5.4). Pain scores were higher in the group without anesthesia than in the group with anesthesia (median 4.8, IQR 2.1‐6.4 vs median 2.1, IQR 1.2‐4.0), although the difference did not reach statistical significance (P=.08).
Discussion
Principal Findings
In a context where the training provided to French medical students for arterial puncture appears highly variable and generally brief—typically lasting less than 30 minutes—and where unsupervised students without specific training demonstrate frequent procedural errors (Multimedia Appendix 1), our results show that a structured training program can meaningfully influence behavior. Specifically, students who completed the structured program (group 1) were significantly less likely to choose local anesthesia before the procedure compared to those who received only informal or no training (group 2; 7/20, 35% vs 28/36, 77.8%; P=.003) despite having similar levels of self-reported anticipatory apprehension. This occurred even though the rate of successful punctures did not differ significantly between groups. From the patients’ perspective, no statistically significant differences were found in anticipatory apprehension or procedural pain based on anesthesia use. Nonetheless, the difference in pain ratings exceeded the minimal clinically important difference on a VAS—typically estimated at 13 mm (1.3 cm) [18]—suggesting a clinically meaningful effect even in the absence of statistical significance. These findings are consistent with those of prior studies that report limited impact of topical anesthetics and highlight the role of operator anxiety in shaping patient experience [459].
Recent reviews in respiratory care education highlight that simulation—whether of low or high fidelity—enhances clinical reasoning, adherence to safety standards, and learner engagement [14]. To our knowledge, this study is among the first to examine the impact of structured training on medical students performing their first arterial puncture. While no direct parallels exist in this population, similar findings have been reported in other health care student groups. For example, Collins et al [13] implemented a 5-step curriculum for respiratory care students combining theory, simulation, and peer assessment, which resulted in high interrater performance scores. In nursing education, structured programs using artificial arm simulators have improved procedural success rates and reduced errors [11], and a competency-based model allowed nurses to reach proficiency levels typically associated with physicians [19]. Given these precedents—and the findings from our preliminary observations (Multimedia Appendix 1)—our study focused not on procedural skill acquisition but on the impact of structured training on students’ apprehension and confidence. In other domains, simulation-based training and structured debriefing have been shown to reduce anxiety and enhance self-confidence. For instance, Schmidt et al [20] demonstrated reduced anxiety in students presenting clinical cases after receiving video-based feedback, and Toy et al [21] reported improved confidence and competence following simulation-based training in core invasive procedures. Similar outcomes have been reported with academic detailing, an approach that typically refers to individualized educational outreach for practicing clinicians [22] that can influence clinical decision-making and has also been shown to improve confidence, competence, and critical thinking [23]. In our study, students who completed the structured training program (group 1) reported levels of apprehension and confidence similar to those of students with informal or no training (group 2) both before and after the procedure. While these results might initially appear less favorable, group 1 students were significantly less likely to use local anesthesia (7/20, 35% vs 28/36, 77.8%; P=.003), revealing a notable divergence between self-reported perception and actual behavior. This suggests that the training influenced confidence in ways not fully captured by subjective ratings. Choosing to perform a first arterial puncture without anesthesia may reflect a stronger sense of preparedness despite lingering concerns about causing pain. Supporting this interpretation, group 1 students showed significantly less apprehension about causing pain than students with no prior training (group 2−). Group 1 students also reported lower postprocedure satisfaction than group 2− students, which may reflect more realistic expectations shaped by the training and a narrower gap between anticipation and experience. The lower use of local anesthesia by group 1 students may also be due to the educational content of the program, which did mention the limited effectiveness of topical anesthetics for arterial puncture according to the literature. However, group 1 students were not advised against their use and were taught how to administer them. This leads us to believe that increased self-confidence did play a role in the observed difference, possibly in addition to or in synergy with adherence to the course content.
This study has several limitations. First, the structured training was not delivered by certified simulation instructors as recommended by the French National Authority for Health. This may have affected its quality—particularly the debriefing, widely regarded as the most critical element of simulation-based learning. Second, the educational interventions received by students in both groups were inherently heterogeneous. Teaching practices varied across hospital sites, ranging from bedside instruction by a nurse, senior medical student, resident, or attending physician to situations in which students performed the procedure with minimal prior observation. This design intentionally reflected the authentic diversity of clinical training conditions rather than an artificially standardized environment to assess the added value of a structured program under real-world conditions. Such heterogeneity may have introduced uncontrolled differences in baseline exposure. Future studies could address this by comparing structured training with a standardized “usual practice” curriculum to more precisely isolate the effects of the structured training. Third, we relied on nonvalidated VASs to assess students’ apprehension and confidence. While these were practical and easy to administer, their psychometric properties are uncertain, limiting the reliability and generalizability of the findings. Future studies should consider using validated instruments for anxiety and procedural self-efficacy, as well as integrating frameworks such as entrustable professional activities to better capture learners’ readiness for unsupervised clinical practice. Fourth, contextual and patient-related factors could not be controlled across hospital sites. Differences in patient characteristics or case complexity may have influenced the technical difficulty of arterial puncture and contributed to variations in first-attempt success rates. Additional limitations include the potential demotivating effect of a lengthy questionnaire, which may have contributed to incomplete responses and the absence of data on the time interval between training and the procedure. Although students had continuous access to theoretical materials, we cannot confirm that they reviewed them prior to performing the puncture, which may have attenuated the effects of the training.
Conclusions
Structured training for arterial puncture influences students’ behavior in meaningful ways even when self-reported confidence and apprehension appear unchanged. The reduced reliance on local anesthesia among trained students may reflect greater readiness to take responsibility for a potentially painful procedure. These findings support the value of formalized training and highlight the need for validated tools and long-term evaluation to fully capture its educational and clinical impact. Although exploratory and limited by methodological constraints, this study provides initial evidence that such pedagogical frameworks could be meaningfully integrated into undergraduate medical curricula in pulmonology and related disciplines.
Supplementary material
10.2196/78086Multimedia Appendix 1Survey, teaching slide, and script.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Dubey R Singh V Khetarpal M Singha SK Sharma K Neema P A comparative study of the ease of radial artery cannulation using the palpation method in patients undergoing surgery under general anaesthesia: pre-induction versus post-induction Cureus Feb 162025172 e 79115 doi 10.7759/cureus.79115 Medline 40109821 PMC 11919643 · doi ↗ · pubmed ↗
- 2Gibbons RC Zanaboni A Saravitz SM Costantino TG Ultrasound guidance versus landmark-guided palpation for radial arterial line placement by novice emergency medicine interns: a randomized controlled trial J Emerg Med Dec 2020596911917 doi 10.1016/j.jemermed.2020.07.029Medline 32917440 · doi ↗ · pubmed ↗
- 3Aaron SD Vandemheen KL Naftel SA Lewis MJ Rodger MA Topical tetracaine prior to arterial puncture: a randomized, placebo-controlled clinical trial Respir Med Nov 2003971111951199 doi 10.1016/s 0954-6111(03)00226-9Medline 14635973 · doi ↗ · pubmed ↗
- 4Tran NQ Pretto JJ Worsnop CJ A randomized controlled trial of the effectiveness of topical amethocaine in reducing pain during arterial puncture Chest Oct 2002122413571360 doi 10.1378/chest.122.4.1357 Medline 12377864 · doi ↗ · pubmed ↗
- 5Haynes JM Randomized controlled trial of cryoanalgesia (ice bag) to reduce pain associated with arterial puncture Respir Care 01201560115 doi 10.4187/respcare.03312 Medline 25516991 · doi ↗ · pubmed ↗
- 6Beaumont M Goret M Orione C et al Effect of local anesthesia on pain during arterial puncture: the GAEL randomized placebo-controlled trial Respir Care Jun 2021666976982 doi 10.4187/respcare.08328 Medline 33758058 · doi ↗ · pubmed ↗
- 7Lightowler JV Elliott MW Local anaesthetic infiltration prior to arterial puncture for blood gas analysis: a survey of current practice and a randomised double blind placebo controlled trial J R Coll Physicians Lond 1997316645646 Medline 9409498 PMC 5421072 · pubmed ↗
- 8Valero Marco AV Martínez Castillo C Maciá Soler L Local anesthesia in arterial puncture: nurses’ knowledge and attitudes Arch Bronconeumol 072008447360363 doi 10.1016/s 1579-2129(08)60062-2Medline 18727888 · doi ↗ · pubmed ↗