Unveiling the Pernicious Truth: A Case Report on the Rare Presentation of Severe Vitamin B12 Deficiency
Olawale O Akinola, Anvitha Mandapati, Nathan Douthit

TL;DR
This case report highlights a rare presentation of severe vitamin B12 deficiency mimicking hemolytic anemia in a patient with Hashimoto’s thyroiditis.
Contribution
The paper presents a unique clinical case where pernicious anemia was misdiagnosed as hemolytic anemia due to overlapping symptoms and lab findings.
Findings
Severe vitamin B12 deficiency can present with hemolytic features, leading to confusion with autoimmune or microangiopathic processes.
Pernicious anemia was confirmed by positive anti-intrinsic factor antibodies and responded rapidly to vitamin B12 replacement therapy.
Abstract
Vitamin B₁₂ deficiency typically causes megaloblastic anemia but can rarely present with hemolytic features, leading to diagnostic confusion with autoimmune or microangiopathic processes. Pernicious anemia, an autoimmune cause of severe B₁₂ deficiency, is frequently underrecognized and may coexist with other autoimmune disorders. We report a 45-year-old woman with Hashimoto’s thyroiditis who presented with dizziness, profound fatigue, and symptomatic anemia. Laboratory evaluation revealed severe macrocytic anemia (hemoglobin 3.5 g/dL, mean corpuscular volume (MCV) 136.9 fL) with thrombocytopenia, elevated lactate dehydrogenase (LDH) (2905 U/L), indirect hyperbilirubinemia, and suppressed haptoglobin, findings suggestive of hemolysis. Peripheral smear showed macrocytosis and marked anisopoikilocytosis without schistocytes. Coombs testing was negative, and G6PD levels were normal.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
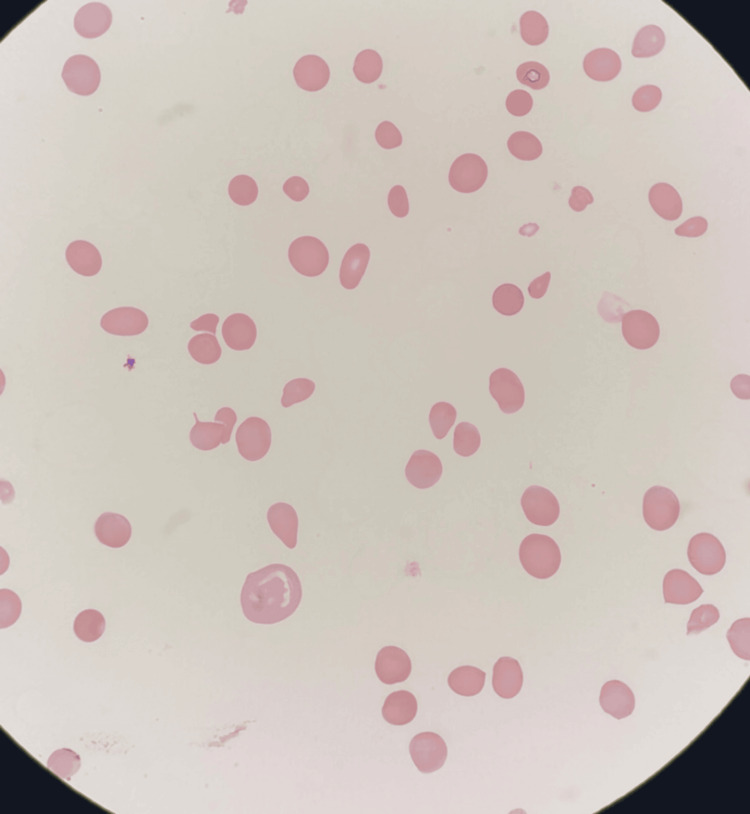 Figure 1
Figure 1| Test | Result | Reference Range | Interpretation |
| Hematology | |||
| Red blood cell count | 0.79 × 10^12/L | 3.4 – 5.0 × 10^12/L | ↓ Severe reduction |
| Hemoglobin | 3.5 g/dL | 11.7 – 15.5 g/dL | ↓ Severe anemia |
| Hematocrit | 0.108 | 36 – 46% | ↓ Low |
| Mean corpuscular volume (MCV) | 136.9 fL | 80 – 100 fL | ↑ Macrocytosis |
| Reticulocyte count | 0.026 | 0.5 – 2.5% | ↓When corrected |
| Platelets | 56 × 10^9/L | 150 – 450 × 10^9/L | ↓ Thrombocytopenia |
| White blood cells | 4.5 x 10^9/L | 4.0 – 11.0 × 10^9/L | Normal |
| Hemolysis Markers | |||
| Total bilirubin | 2.4 mg/dL | 0.3 – 1.1 mg/dL | ↑ Elevated |
| Indirect bilirubin | 1.6 mg/dL | <1.0 mg/dL | ↑ Elevated |
| LDH | 2905 U/L | 98 – 192 U/L | ↑ Markedly elevated |
| Haptoglobin | <30 mg/dL | 44 – 215 mg/dL | ↓ Reduced |
| Iron Studies | |||
| Serum iron | 256 µg/dL | 28 – 170 µg/dL | ↑ Elevated |
| Transferrin saturation | 0.92 | 18 – 48% | ↑ Elevated |
| Ferritin | 192.9 | 12 – 300 ng/mL | Within range |
| Vitamin / Endocrine | |||
| Vitamin B12 | 73 pg/mL | 180 – 914 pg/mL | ↓ Severe deficiency |
| Folate | 12 ng/mL | 3 – 17 ng/mL | Normal |
| TSH | 11.2 µIU/mL | 0.34 – 5.6 µIU/mL | ↑ Elevated |
| Free T4 | 0.94 ng/dL | 0.7 – 1.85 ng/dL | Normal |
| Other Tests | |||
| HIV serology | Negative | — | Negative |
| Hepatitis panel | Negative | — | Negative |
| Parameter | At Discharge | Two Weeks Post-Discharge | Interpretation / Trend |
| Red blood cell count | 2.40 × 10^12/L | 2.63 × 10^12/L | Improving, still low |
| Hemoglobin | 8.3 g/dL | 8.4 g/dL | Rising from nadir, remains anemic |
| Hematocrit | 0.248 | 0.265 | Improving |
| Mean corpuscular volume (MCV) | 103.3 fL | 100.7 fL | Trending toward normal |
| Platelet count | 39 × 10^9/L | 324 × 10^9/L | Recovered to normal |
| White blood cell count | 4.3 × 10^9/L | 7.6 × 10^9/L | Normal, improved |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFolate and B Vitamins Research · Porphyrin Metabolism and Disorders · Celiac Disease Research and Management
Introduction
Anemia is defined as a reduction in red blood cell mass, hemoglobin concentration, or hematocrit, resulting in impaired oxygen delivery to tissues. The World Health Organization (WHO) estimates that anemia affects around 500 million women of reproductive age and 269 million children worldwide [1]. In 2019, anemia was reported in 30% of non-pregnant and 37% of pregnant women aged 15-49 years [2]. According to WHO criteria, anemia is diagnosed when hemoglobin levels fall below 13 g/dL in men and below 12 g/dL in nonpregnant women [3]. Anemia is multifactorial and can be classified by red blood cell size (microcytic, normocytic, or macrocytic), onset (acute or chronic), etiology (nutritional deficiency, hemolysis, marrow failure, chronic inflammation, or inherited disorders), and severity (mild, moderate, or severe) [4,5]. Among global causes, nutritional deficiencies, particularly iron deficiency, remain predominant [2]. However, vitamin B₁₂ deficiency is a clinically significant but often overlooked cause, typically producing megaloblastic anemia due to defective DNA synthesis and ineffective erythropoiesis [5]. Efficient absorption of vitamin B₁₂ requires gastric intrinsic factor and formation of a B₁₂-intrinsic factor complex [6]. Severe deficiency caused by gastric bypass surgery, malabsorption, or autoimmune destruction of intrinsic factor (pernicious anemia) usually results in megaloblastic anemia but can, rarely, present with hemolytic anemia, as described in this case. Pernicious anemia is an autoimmune disorder characterized by antibodies against intrinsic factor or gastric parietal cells, impairing vitamin B₁₂ absorption [6]. It affects roughly 0.1% of the general population and up to 1.9% of those over 60 years, accounting for 20-50% of adult B₁₂ deficiency cases [7]. Historically, it was a fatal illness with patients typically surviving only one to three years after diagnosis until the discovery in the 1920s that liver ingestion improved survival and, subsequently, that vitamin B₁₂ was the curative factor [8]. These discoveries earned Minot and Murphy the Nobel Prize in 1934. With prompt recognition and lifelong supplementation, the prognosis is now excellent, though the condition remains underdiagnosed [6]. Definitive diagnosis depends on detecting parietal cell or intrinsic factor antibodies, and delayed treatment can lead to irreversible neurologic sequelae such as subacute combined degeneration of the spinal cord [9].
Case presentation
A 45-year-old woman with a history of combined systolic and diastolic heart failure (automated implantable cardiac defibrillator in situ), essential hypertension, and hypothyroidism secondary to Hashimoto’s thyroiditis presented with dizziness and lightheadedness occurring during dinner. She reported nausea and transient blurring of vision without syncope or trauma. Over the preceding two weeks, she experienced increasing fatigue, which she attributed to her thyroid disease. She denied chest pain, palpitations, dyspnea, or seizures. No gastrointestinal or urinary symptoms were reported, though she noted intermenstrual bleeding for three months. Her medications included metoprolol, bumetanide, amiodarone, levothyroxine, and digoxin. On examination, she appeared pale and somnolent. Vitals were blood pressure of 109/62 mmHg, heart rate of 118 bpm, respiratory rate of 20/min, SpO₂ 100% (room air), and temperature 98.7°F. There was no cyanosis or jaundice. Cardiopulmonary, abdominal, and neurological examinations were unremarkable. Laboratory results (Table 1) revealed severe macrocytic anemia (hemoglobin 3.5 g/dL, mean corpuscular volume (MCV) 136.9 fL) with thrombocytopenia (56 × 10⁹/L). Hemolysis markers were deranged: lactate dehydrogenase (LDH) 2905 U/L, indirect bilirubin 1.6 mg/dL, and haptoglobin < 30 mg/dL. Iron and ferritin were normal, and thyroid testing confirmed uncontrolled hypothyroidism (thyroid-stimulating hormone (TSH) 11.2 µIU/mL). Serum vitamin B₁₂ was profoundly low (73 pg/mL).
CT of the abdomen revealed no mass lesions, and pelvic ultrasound identified a benign nabothian cyst. Peripheral smear (Figure 1) demonstrated macrocytosis, anisopoikilocytosis, ovalocytes, elliptocytes, teardrop cells, and nucleated red cells, without schistocytes.
Peripheral Blood Smear
She was transfused with three units of packed red cells and started on intramuscular cyanocobalamin 1000 μg daily for seven days, then weekly for four weeks, and monthly thereafter. Rapid hematologic improvement followed (Table 2). G6PD level was normal, and a negative Coombs test excluded autoimmune hemolytic anemia. Anti-intrinsic factor antibodies were positive, confirming pernicious anemia as the etiology of severe B₁₂ deficiency with secondary hemolysis and thrombocytopenia.
Clinical timeline
Over three months, the patient experienced progressive fatigue and exertional dyspnea, with dizziness worsening in the two weeks before presentation. Admission labs revealed severe macrocytic anemia (hemoglobin 3.5 g/dL, MCV 136.9 fL), thrombocytopenia, and biochemical evidence of hemolysis, with profoundly low vitamin B₁₂. She was promptly treated with packed red blood cell transfusions and intramuscular vitamin B₁₂, leading to rapid symptomatic improvement. By the third hospital day, the reticulocyte activity had improved. At discharge on day four, her hemoglobin had risen to 8.3 g/dL, and she transitioned to outpatient B₁₂ therapy. At her two-week follow-up, hemoglobin and macrocytosis continued to improve, and platelet counts normalized. Additionally, intrinsic factor antibodies confirmed the diagnosis of pernicious anemia. The patient reported feeling “dramatically better,” expressed full understanding of her diagnosis, and demonstrated clear commitment to lifelong B₁₂ replacement.
Discussion
This case highlights a rare manifestation of vitamin B₁₂ deficiency presenting as hemolytic anemia rather than the classic megaloblastic form. The patient exhibited profound anemia (hemoglobin 3.5 g/dL), elevated LDH, indirect hyperbilirubinemia, and low haptoglobin, all consistent with hemolysis. Yet, the reticulocyte index (0.3) indicated ineffective erythropoiesis rather than brisk peripheral destruction.
On physical examination, the patient appeared pale and markedly fatigued, with sinus tachycardia reflecting the severity of her anemia, though she remained normotensive and clinically stable. There was no scleral icterus or cutaneous jaundice despite biochemical evidence of hemolysis, and no petechiae or purpura to suggest consumptive or microangiopathic processes. Cardiopulmonary examination revealed regular rhythm without murmurs and clear lung fields. The abdomen was soft and non-tender, with no hepatosplenomegaly. Neurologic examination showed preserved mental status, motor strength, sensation, reflexes, and coordination, indicating absence of overt neurologic sequelae of vitamin B₁₂ deficiency at presentation.
Differential diagnosis
Given her age and menstrual history, iron deficiency anemia was considered but excluded by normal iron studies and macrocytosis. Autoimmune hemolytic anemia (AIHA) was considered due to elevated LDH, indirect hyperbilirubinemia, and low haptoglobin, but excluded by a negative Coombs test. Microangiopathic hemolytic anemia (MAHA), including thrombotic thrombocytopenic purpura (TTP) and hemolytic uremic syndrome (HUS), was ruled out by the absence of schistocytes, neurologic deficits, or renal impairment. None of her medications are typical triggers for drug-induced hemolysis, and G6PD deficiency was excluded. Ultimately, the combination of macrocytosis, autoimmune background (Hashimoto’s thyroiditis), markedly low B₁₂, and positive anti-intrinsic factor antibodies confirmed pernicious anemia. This careful diagnostic approach prevented misclassification as AIHA or TTP, avoiding unnecessary corticosteroids or plasma exchange.
Pathophysiology of hemolysis in vitamin B₁₂ deficiency
B₁₂ deficiency disrupts DNA synthesis in erythroid precursors, creating fragile megaloblasts that undergo apoptosis within the marrow (intramedullary hemolysis) [5,6]. These cells release LDH and bilirubin, mimicking hemolysis but lacking an immune mechanism, hence the negative Coombs test [10].
Autoimmune context
Pernicious anemia commonly coexists with other autoimmune diseases [6,11]. Autoimmune thyroid disease, particularly Hashimoto’s thyroiditis, is observed in 10-40% of patients with autoimmune gastritis or pernicious anemia, underscoring shared immunologic mechanisms [11]. This overlap provided an important diagnostic clue in our patient.
Response to treatment
Following transfusion and cyanocobalamin therapy, the patient’s platelet count normalized within two weeks, and hemoglobin rose from 3.5 g/dL to 8.4 g/dL, confirming marrow recovery [7]. Lifelong B₁₂ supplementation was emphasized to prevent relapse and irreversible neurologic damage.
Limitations
This case illustrates a rare hemolytic presentation of pernicious anemia and provides well-documented diagnostic evidence and treatment response. However, as a single case, its generalizability is limited, and the absence of longer-term follow-up is an additional constraint.
Conclusions
Vitamin B₁₂ deficiency, most often due to pernicious anemia, can occasionally manifest with hemolytic features instead of the classic megaloblastic presentation. In this case, the coexistence of Hashimoto’s thyroiditis provided a vital clue to an underlying autoimmune mechanism. Recognizing such atypical presentations prevents misclassification and avoids inappropriate therapy. Prompt diagnosis and lifelong vitamin B₁₂ supplementation can rapidly restore hematologic function and avert irreversible neurologic sequelae.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Trends and determinants of anemia in children 6-59 months and women of reproductive age in Chad from 2016 to 2021 BMC Nutr Zavala E Adler S Wabyona E Ahimbisibwe M Doocy S 117920233787263710.1186/s 40795-023-00777-y PMC 10594667 · doi ↗ · pubmed ↗
- 2Anaemia 9 2025 2025 https://www.who.int/news-room/fact-sheets/detail/anaemia
- 3Anemia in clinical practice-definition and classification: does hemoglobin change with aging?Semin Hematol Cappellini MD Motta I 2612695220152640443810.1053/j.seminhematol.2015.07.006 · doi ↗ · pubmed ↗
- 4Macrocytic anemia Stat Pearls Killeen RB Adil A Treasure Island Stat Pearls Publishing 2025 http://www.ncbi.nlm.nih.gov/books/NBK 459295/29083571 · pubmed ↗
- 5Megaloblastic anemia Stat Pearls Hariz A Bhattacharya PT Treasure Island Stat Pearls Publishing 2025 http://www.ncbi.nlm.nih.gov/books/NBK 537254/30725939 · pubmed ↗
- 6Pernicious anemia Stat Pearls Vaqar S Shackelford KB Treasure Island Stat Pearls Publishing 2025 https://pubmed.ncbi.nlm.nih.gov/31082033/31082033 · pubmed ↗
- 7Optimal management of pernicious anemia J Blood Med Andres E Serraj K 97103320122302823910.2147/JBM.S 25620 PMC 3441227 · doi ↗ · pubmed ↗
- 8One history of pernicious anaemia 9 2025 2025 https://pernicious-anaemia-society.org/pernicious-anaemia/one-history-of-pernicious-anaemia/