Efficacy of NSAIDs and corticosteroids as premedication for post-endodontic pain management: A systematic review and meta-analysis
Radia Mrini, Marcela Salamanca-Ramos, Priscilla Ledezma, Alejandro R. Pérez, José Aranguren, Javier Montecinos, Elías Utreras, Nicolas Pinto-Pardo

TL;DR
This study finds that NSAIDs and corticosteroids both reduce post-dental pain, with NSAIDs acting quickly and corticosteroids providing longer-lasting relief.
Contribution
The study provides a systematic review and meta-analysis comparing preemptive NSAID and corticosteroid use for post-endodontic pain management.
Findings
NSAIDs and corticosteroids both significantly reduce postoperative pain compared to placebo.
NSAIDs offer rapid early pain relief, while corticosteroids provide sustained analgesia over 12-48 hours.
Both drug classes reduce rescue analgesic use, with corticosteroids showing slightly better long-term efficacy.
Abstract
Post-endodontic pain remains a common clinical challenge. This systematic review and meta-analysis evaluated the preemptive efficacy of NSAIDs and corticosteroids as premedication for managing postoperative pain in patients with symptomatic irreversible pulpitis undergoing non-surgical root canal treatment. Objectives: To compare the preemptive efficacy of NSAIDs and corticosteroids as single-dose premedication in reducing postoperative pain and rescue medication use after endodontic treatment. Following PRISMA 2020 guidelines, a systematic search was conducted in PubMed, Cochrane Library, and Embase up to April 2024. Eligibility criteria included randomized controlled trials comparing single-dose NSAIDs or corticosteroids with placebo. Primary outcomes were postoperative pain intensity measured by validated scales (VAS, NRS, HP-VAS) and need for rescue analgesics. Risk of bias was…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
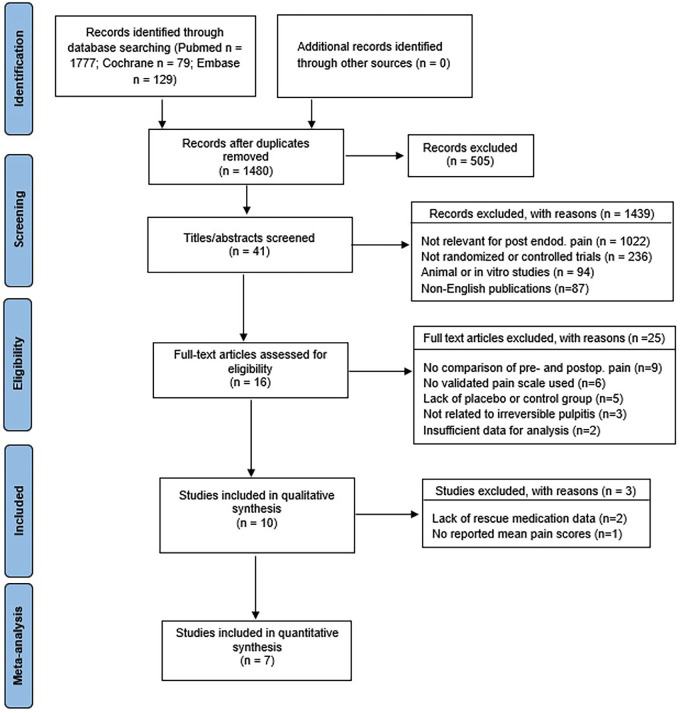 Figure 1
Figure 1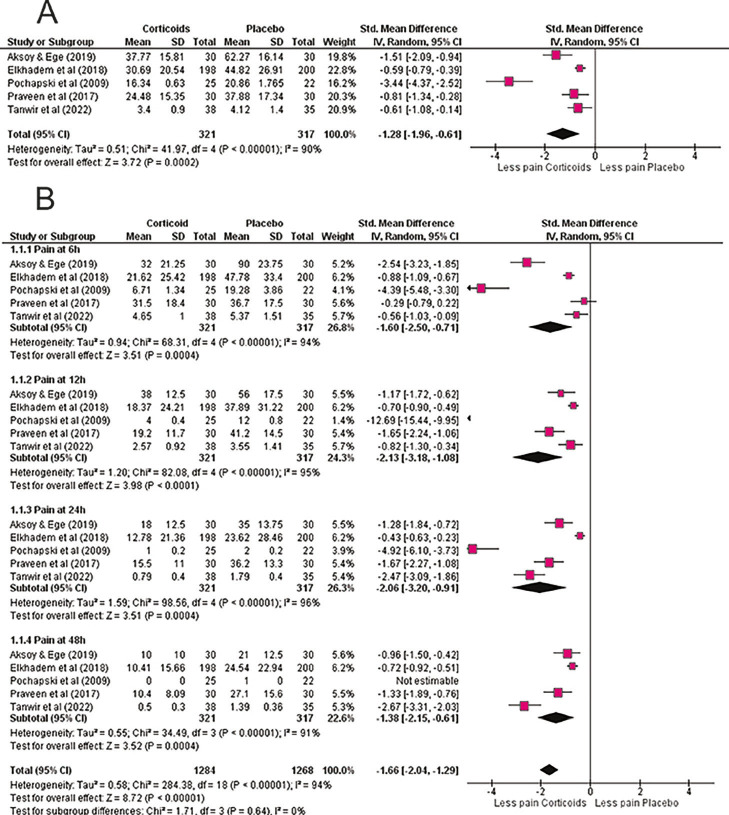 Figure 2
Figure 2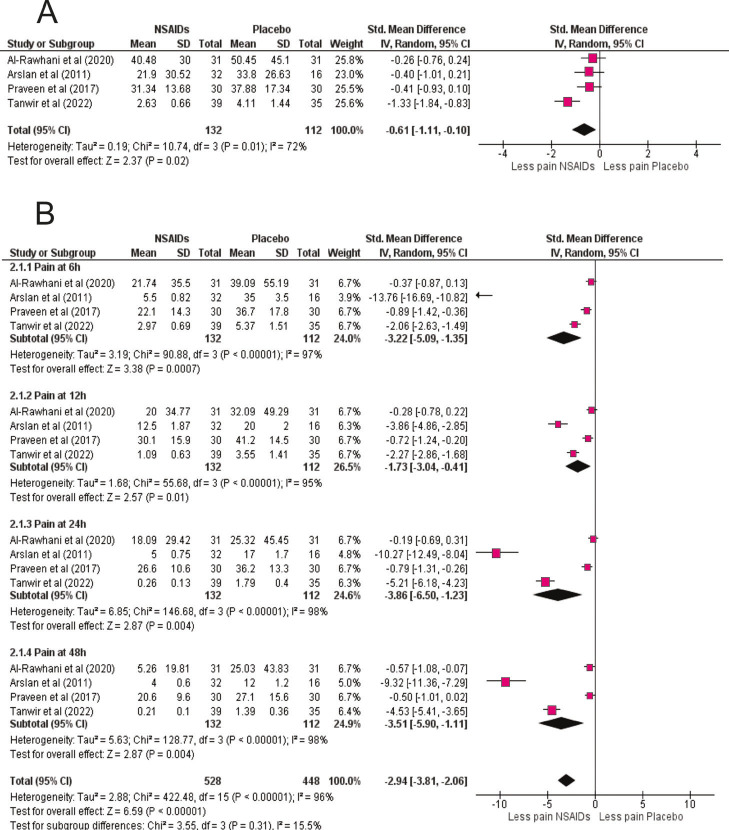 Figure 3
Figure 3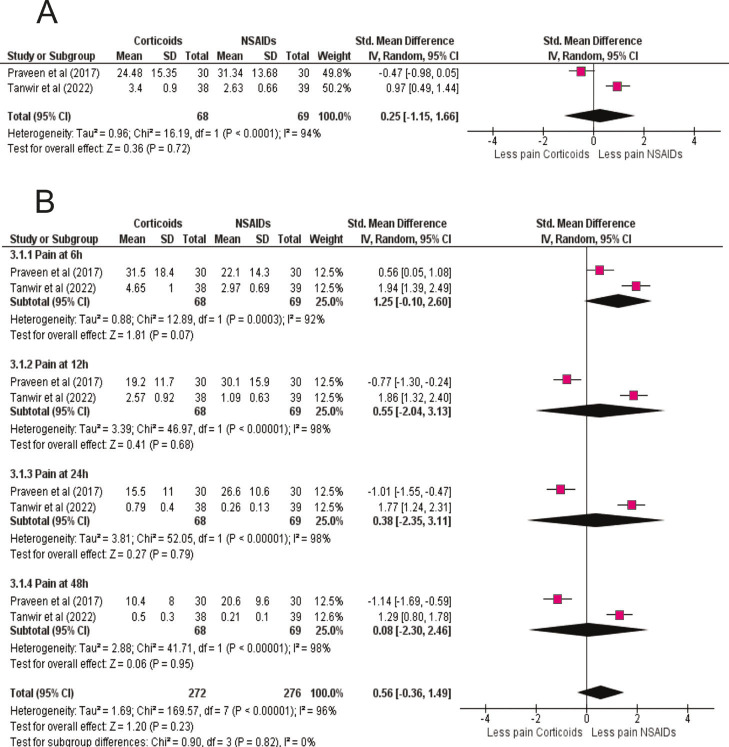 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEndodontics and Root Canal Treatments · Dental Anxiety and Anesthesia Techniques · Dental Erosion and Treatment
Introduction
Orofacial pain, prevalent in 5% to 57% of individuals across various regions (1), significantly impacts psychological, social, and economic well-being, with dental pain affecting 7% to 32% of the global population (2). Dental pain primarily arises from periapical or pulp conditions, often requiring endodontic therapy or extraction (3). Around 81% of these cases necessitate endodontic treatment (4), with the primary goal being the rapid relief of pain, particularly in cases of symptomatic irreversible pulpitis (5). Symptoms include persistent thermal discomfort, spontaneous pain, and referred pain, sometimes with no overt clinical signs despite underlying inflammation (6). Irreversible pulpitis is an inflammatory condition of the dental pulp, primarily triggered by bacterial infections (7). The immune response involves pro-inflammatory cytokines (such as IL-8 and TNF-) (8) and gene expression of IL-6 and MMP-9, driving inflammation and tissue degradation (9). Immune cell interactions, such as those involving calcitonin receptors, also contribute to pulp inflammation and pain (7 , 8). Non-surgical root canal therapy is the recommended treatment for irreversible pulpitis in mature permanent teeth, guided by clinical indicators and patient-reported experiences (10). Postoperative pain, affecting 3-58% of patients, requiring effective analgesic and anti-inflammatory strategies (2 , 11 , 12). Preemptive pain management is crucial, as preoperative medication can reduce postoperative pain by preventing central and peripheral sensitization (13 , 14). Effective premedication includes analgesia plans and patient education to minimize acute discomfort and prevent chronic pain (15). Analgesics are classified as opioids and non-opioids. While opioids like morphine or tramadol manage moderate to severe pain, they have significant side effects and dependency risks (16). Non-opioids, such as corticosteroids and NSAIDs, are essential due to their anti-inflammatory properties (17 , 18). Corticosteroids (dexamethasone or prednisolone) inhibit phospholipase A2, reducing inflammation (19). NSAIDs (ibuprofen or naproxen), act on cyclooxygenase enzymes, decreasing prostaglandin production and inflammation (20). However, NSAIDs may cause gastrointestinal issues, necessitating cautious prescribing (21). Continuous medication use raises risks of gastrointestinal bleeding and renal impairment, emphasizing the need for optimized medication strategies (22). A systematic review and meta-analysis are needed to develop clear clinical guidelines. Optimizing premedication with corticosteroids and NSAIDs may significantly enhance patient outcomes and satisfaction following endodontic treatments. Population, Intervention, Comparator, Outcomes (PICO): Adults with symptomatic irreversible pulpitis undergoing nonsurgical root canal treatment; single-dose premedication with NSAIDs or corticosteroids; comparator groups were placebo or the alternative drug class; primary outcomes were postoperative pain intensity at 6, 12, 24, and 48 h, and the use of rescue analgesics. Only randomized controlled trials were eligible. This review adds novelty by integrating a direct head-to-head quantitative comparison between corticosteroids and NSAIDs, accompanied by time-dependent (6-48 h) efficacy analysis and synthesis of rescue-medication use-an approach not addressed in previous meta-analyses.
Material and Methods
This systematic review and meta-analysis followed the PRISMA 2020 guidelines. The protocol was prospectively registered in PROSPERO (CRD42024499723). Eligibility criteria were defined according to the PICO framework described in the Introduction. This review included only randomized controlled trials (RCTs) enrolling adults diagnosed with symptomatic irreversible pulpitis (SIP), with or without symptomatic apical periodontitis, requiring nonsurgical root canal treatment under local anesthesia. Eligible studies met the following PICO-based criteria: Population (P): Adult patients (18 years) with a clinical and radiographic diagnosis of symptomatic irreversible pulpitis in permanent teeth. Intervention (I): Single-dose premedication with nonsteroidal anti-inflammatory drugs (NSAIDs) or corticosteroids administered orally, intramuscularly, or submucosally prior to endodontic treatment. Comparator (C): Placebo or an alternative drug class (NSAID vs corticosteroid). Outcomes (O): Primary outcome-postoperative pain intensity assessed at 6, 12, 24, and 48 h after treatment using validated scales (VAS, NRS, HP-VAS). Secondary outcome-the need for rescue analgesic medication. Only studies that clearly reported baseline and postoperative pain scores, drug dosage and administration route, and follow-up periods were included. Exclusion criteria were: (1) Non-randomized studies, quasi-experimental designs, case reports, or reviews; (2) Trials involving patients with systemic diseases, pregnant or lactating women, or those under chronic anti-inflammatory, analgesic, or corticosteroid therapy; (3) Studies without quantitative pain data or lacking mean and standard deviation values for each time point; (4) Trials where premedication was part of combination therapy with antibiotics or other analgesics; (5) Non-English publications or inaccessible full-text articles. Search strategy: A comprehensive search was conducted in PubMed, Cochrane Library, and Embase up to April 2024, combining controlled vocabulary (MeSH/Emtree) and free-text terms for "NSAIDs," "corticosteroids," "pulpitis," and "endodontic pain." Detailed strategies are provided in the (Supplement 1) http://www.medicinaoral.com/medoralfree01/aop/jced_63455_s01.pdf No language or publication status restrictions were applied. A list of excluded full-text studies with reasons is provided in (Supplement 2) http://www.medicinaoral.com/medoralfree01/aop/jced_63455_s02.pdf Certainty of evidence for each main outcome and comparison is summarized using the GRADE (Supplement 3) http://www.medicinaoral.com/medoralfree01/aop/jced_63455_s03.pdf For the head-to-head comparison (corticosteroids vs NSAIDs), we pooled only direct randomized evidence; no network meta-analysis was performed. Random-effects models were used throughout. Study selection: Three reviewers independently screened titles and abstracts, followed by full-text assessment. Disagreements were resolved by discussion and arbitration by a senior reviewer. Duplicates were removed with Mendeley software. The PRISMA 2020 flow diagram summarizes the process. Data extraction: Using a standardized Excel form, three reviewers independently extracted study characteristics (author, year, country, sample size, demographics, intervention, comparator, outcomes, and follow-up). The primary outcomes were postoperative pain intensity at 6, 12, 24, and 48 hours (measured by VAS, NRS, or HP-VAS) and need for rescue medication. Secondary outcomes included pain trajectories over time. Risk of bias and certainty: The Cochrane RoB2 tool was applied to assess risk of bias across domains: randomization, deviations from interventions, missing data, outcome measurement, and reporting. Certainty of evidence was graded with the GRADE approach, considering risk of bias, inconsistency, indirectness, imprecision, and publication bias. Statistical analysis: Meta-analyses were conducted using RevMan 5.4. Outcomes were pooled as standardized mean differences (SMD) with 95% confidence intervals (CI). Given substantial heterogeneity (I² = 90%), a random-effects model was applied. Subgroup analyses explored drug class (NSAIDs vs. corticosteroids), specific agent, dose, and administration route. To address concerns regarding imputed values from exponential decay modeling, a sensitivity analysis excluding imputed points was performed (Supplement 4) http://www.medicinaoral.com/medoralfree01/aop/jced_63455_s04.pdf Publication bias was assessed with funnel plots and Egger's test (p = 0.12).
Results
Study selection: The initial search retrieved 1,327 records. After removal of duplicates and screening, 24 full-text articles were assessed. Finally, 7 randomized controlled trials (n = 820) published between 2009 and 2023 met the inclusion criteria. The PRISMA 2020 flow diagram summarizes the process (Fig. 1).
Figure 1PRISMA 2020 flow diagram illustrating the study selection process.
Flowchart of identification, screening, eligibility, and inclusion of randomized controlled trials evaluating single-dose premedication (NSAIDs or corticosteroids) for post-endodontic pain in symptomatic irreversible pulpitis. Reasons for exclusion are shown at each stage according to PRISMA 2020. Seven RCTs were included in the quantitative synthesis. Study characteristics: Included RCTs investigated different NSAIDs (ibuprofen, ketorolac, diclofenac) and corticosteroids (dexamethasone, prednisolone, betamethasone) administered as a single oral or intramuscular premedication before non-surgical root canal treatment in patients with symptomatic irreversible pulpitis. Placebo served as the comparator in all trials. Pain was measured using validated scales (VAS, NRS, HP-VAS) at 6, 12, 24, and 48 hours postoperatively. Rescue analgesic intake was recorded in most studies. Table 1 summarizes patient numbers, pre-medication used, and outcome verification methods.
Risk of Bias Assessment: The Revised Cochrane Risk of Bias Tool (RoB2) assessed study quality (Table 2).
Most studies were low risk of bias, though some had "some concerns" in randomization and missing outcome data. Summary of Included Studies: Primary outcomes measured were pain relief efficacy and duration of postoperative pain control. These studies provide insights into premedication strategies for managing postoperative pain during endodontic procedures. Meta-analysis Corticoids vs Placebo: Meta-analysis of seven RCTs demonstrated that premedication with corticosteroids significantly reduced postoperative endodontic pain compared with placebo (SMD = -1.28; 95% CI: -1.96 to -0.61; p = 0.0002), despite high heterogeneity (I² = 90%) (Fig. 2A).
Figure 2. Corticosteroid premedication versus placebo. (A) Overall random-effects meta-analysis comparing corticosteroids with placebo for postoperative pain after endodontic treatment. Effect sizes are standardized mean differences (SMD) with 95% confidence intervals (negative values favor corticosteroids). Across the included trials (corticosteroids n=321; placebo n=317), corticosteroid premedication significantly reduced pain (overall SMD = –1.28). Substantial heterogeneity likely reflects variation in drug type, dose, and route. (B) Time-course analysis (6, 12, 24, 48 h). Corticosteroids show rapid benefit that is most evident at 12–24 h and remains present at 48 h, consistent with their sustained anti-inflammatory action.
Prednisolone (20-40 mg), dexamethasone (4-8 mg, oral or intramuscular), and methylprednisolone were tested, all showing consistent analgesic benefit. Time-course analysis confirmed efficacy at all intervals. At 6 h, corticosteroids reduced pain substantially (SMD = -1.60; 95% CI: -2.50 to -0.71; p = 0.0004), with effects maintained at 12 h (SMD = -2.13; 95% CI: -3.18 to -1.08; p < 0.0001), 24 h (SMD = -2.06; 95% CI: -3.20 to -0.91; p = 0.0004), and 48 h (SMD = -1.38; 95% CI: -2.15 to -0.61; p = 0.001) (Fig. 2B). These findings highlight both rapid and sustained corticosteroid analgesia, supporting their role as an effective preemptive option in endodontic pain management. NSAIDs vs Placebo: NSAID premedication also significantly reduced postoperative pain compared with placebo (SMD = -0.61; 95% CI: -1.11 to -0.10; p = 0.02; I² = 72%) (Fig.3A).
Figure 3NSAID premedication versus placebo. (A) Overall random-effects meta-analysis comparing NSAIDs with placebo for postoperative pain. SMDs (95% CI) are shown; negative values favor NSAIDs. Pooled results (NSAIDs n=132; placebo n=112) demonstrate a significant reduction in pain (overall SMD ≈ –0.61), with moderate–high heterogeneity attributable to differences in drug and dosing regimens. B) Time-course analysis (6, 12, 24, 48 h). NSAIDs provide the greatest early analgesic effect at 6 h, with clinically meaningful reductions persisting through 24–48 h, consistent with their rapid onset via COX inhibition.
Trials tested ibuprofen (200 mg), diclofenac potassium (50 mg), and tenoxicam (20 mg), all demonstrating superiority over placebo. Time-course analysis revealed the strongest effect at 6 h (SMD = -3.22; 95% CI: -5.09 to -1.35; p = 0.0007), with continued benefit at 12 h (SMD = -1.73; 95% CI: -3.04 to -0.41; p = 0.01), 24 h (SMD = -3.86; 95% CI: -6.50 to -1.23; p = 0.004), and 48 h (SMD = -3.51; 95% CI: -5.90 to -1.11; p = 0.004) (Fig 3B). These results confirm NSAIDs' rapid onset of analgesia, consistent with their cyclooxygenase-inhibiting mechanism. Corticoids vs NSAIDs: Direct comparison between corticosteroids and NSAIDs revealed no statistically significant difference (SMD = 0.25; 95% CI: -1.15 to 1.66; p = 0.72; I² = 94%) (Fig. 4A).
Figure 4. Corticosteroids versus NSAIDs (head-to-head comparison). (A) Overall random-effects meta-analysis directly comparing corticosteroids and NSAIDs for postoperative pain reduction. SMDs (95% CI) are shown; negative values favor corticosteroids. No statistically significant difference was observed (corticosteroids n=68; NSAIDs n=69), indicating broadly comparable analgesic efficacy. (B) Time-course comparison (6, 12, 24, 48 h). NSAIDs tend to provide faster relief at 6 h, whereas corticosteroids maintain analgesia into the first two postoperative days, illustrating complementary onset–duration profiles relevant to individualized premedication.
Some trials slightly favored NSAIDs (Praveen et al.), while others favored corticosteroids (Tanwir et al.), reflecting heterogeneity in drug, dose, and administration. Time-course comparisons showed NSAIDs had a trend toward stronger pain reduction at 6 h (SMD = -1.25; 95% CI: -2.60 to 0.10; p = 0.07), while corticosteroids provided more sustained analgesia at later intervals, although differences were not statistically significant (Fig. 4B). These findings suggest both drug classes are effective, with NSAIDs better suited for early relief and corticosteroids for prolonged control. Use of Rescue Medication after Endodontic Treatment: Rescue medication use was consistently lower in premedicated arms than in placebo. Across trials, placebo groups showed the highest proportion of patients requiring additional analgesics (typically 30%), whereas both NSAID- and corticosteroid-premedicated groups were below 10%. These patterns were observed irrespective of drug, dose, and route, and remained robust in sensitivity analyses (Supplement 5) (http://www.medicinaoral.com/medoralfree01/aop/jced_63455_s05. Modeling of missing intermediate time points.). ANOVA and Tukey post-hoc analyses confirmed significant differences versus placebo (p < 0.05), but no difference between active treatments (p = 0.99). Individual studies echoed these results: Elkhadem et al. reported 48% of placebo patients versus 22% with prednisolone; Aksoy & Ege reported 56.7% with placebo versus 13.3% with dexamethasone; Al Rawhani et al. observed dose-dependent reductions with ketorolac (20% placebo vs 7.5% at 10 mg and 5% at 20 mg). Across all studies, both NSAIDs and corticosteroids substantially decreased reliance on supplementary analgesia (Table 3).
Pain Perception Over Time: Two-way ANOVA demonstrated that time accounted for most variation in pain scores (78.1%, p < 0.0001), with a significant effect of treatment type (p = 0.0019) but no significant interaction (p = 0.47). ídák's test showed NSAIDs significantly reduced pain versus placebo at 6 h (p = 0.0106). Corticosteroids also lowered pain scores at this interval but without statistical significance (p = 0.12). At 12, 24, and 48 h, pain scores declined similarly across groups, with no significant differences between active treatments. This pattern reinforces NSAIDs' role in early postoperative relief and corticosteroids' contribution to longer-term control (Supplement 5) http://www.medicinaoral.com/medoralfree01/aop/jced_63455_s05.pdf
Discussion
This systematic review and meta-analysis evaluated the preemptive use of corticosteroids and NSAIDs for managing postoperative endodontic pain in symptomatic irreversible pulpitis. Unlike prior reviews that examined each drug class separately, this study provides the first integrated quantitative comparison encompassing temporal efficacy (6-48 h) and rescue-medication outcomes. This unified framework clarifies the time-dependent analgesic profiles of both drug classes and supports evidence-based, opioid-sparing strategies. The findings confirm that both corticosteroids and NSAIDs significantly reduce pain intensity and the need for additional analgesics compared with placebo, underscoring their clinical relevance in acute dental pain management (23 - 25). This work advances previous evidence by offering a head-to-head synthesis that enhances clinical decision-making through a comprehensive appraisal of onset, duration, and overall analgesic effectiveness. The finding that NSAIDs produced rapid pain relief within 6 h, while corticosteroids exerted more sustained effects up to 48 h, reflects the pharmacodynamic differences between these drug classes. NSAIDs inhibit cyclooxygenase enzymes, thereby suppressing prostaglandin synthesis and reducing peripheral nociceptor sensitization (26). This mechanism explains their superior early performance, particularly with agents such as ibuprofen and diclofenac, which have short plasma half-lives but rapid onset of action (27). In contrast, corticosteroids act through glucocorticoid receptor activation, leading to downregulation of pro-inflammatory cytokines such as IL-6 and TNF-, and upregulation of IL-10 (28). These genomic effects suppress NF-B pathways, reduce vascular permeability, and dampen neurogenic inflammation, resulting in delayed but prolonged analgesia (29 , 30). The distinct temporal patterns observed in our analysis therefore have a clear biological rationale and support the potential role of multimodal regimens that combine both drug classes to maximize early and sustained pain relief (31). This mechanistic complementarity may explain why both drug classes ultimately converge in analgesic efficacy but differ in onset and duration, informing clinical decisions for individualized premedication strategies. Our findings align with several previous systematic reviews and randomized controlled trials. Shamszadeh et al. reported consistent reductions in postoperative endodontic pain with corticosteroid premedication, particularly at 12 and 24 hours (32). Similarly, Jose et al. demonstrated in a systematic review that both NSAIDs and corticosteroids administered orally are effective in reducing post-endodontic pain, with comparable efficacy across most time intervals (25). Hegde et al. confirmed the benefit of preoperative corticosteroids in single-visit root canal treatment, reinforcing their role in difficult-to-manage pulpitis cases (24). However, individual trials have shown conflicting results. Zanjir et al. observed that NSAIDs maintained superior pain reduction at later intervals (33), whereas Konagala et al. found no significant difference beyond 12 hours (34). Tanwir et al. reported that both piroxicam and prednisolone were effective without major differences (35). These inconsistencies highlight the variability in drug type, dosage, administration routes, and study methodology, which were reflected in the high heterogeneity (I² > 70%) of our pooled results. The clinical implications of these findings are significant. The 2024 American Dental Association (ADA) guideline strongly recommends NSAIDs, alone or in combination with acetaminophen, as first-line therapy for acute dental pain and discourages opioid prescribing (23). Our results confirm the rapid analgesic benefits of NSAIDs, particularly important in acute cases where immediate relief is needed. However, the sustained analgesic profile of corticosteroids suggests an additional role in situations where prolonged control is desirable or where NSAIDs are contraindicated due to gastrointestinal or renal risks (36). These insights support individualized prescribing decisions in endodontic practice and encourage consideration of multimodal strategies. Rescue medication use provided further confirmation of the effectiveness of both drug classes. Placebo groups consistently showed the highest rates of supplemental analgesic intake, often exceeding 30%, whereas premedication with either NSAIDs or corticosteroids reduced this to below 10% (24 , 35 , 37). For example, Elkhadem et al. demonstrated that preoperative prednisolone halved the number of patients requiring additional analgesics after root canal treatment (37). These findings illustrate not only improved patient comfort but also an important opioid-sparing effect. In the context of the ongoing opioid crisis, the capacity of NSAIDs and corticosteroids to reduce the need for supplementary pain medication strengthens the case for their routine use in endodontic protocols (23). It is also important to recognize that pain perception is influenced not only by pharmacological interventions but also by psychosocial factors. Placebo responses in dental pain can reach up to 30% and are mediated by endogenous opioid activity and anticipatory mechanisms (38 , 39). Anxiety, prior dental experiences, and patient expectations strongly modulate perceived pain intensity (40). These considerations emphasize the value of combining pharmacological approaches with effective communication and reassurance to optimize outcomes, particularly in anxious patients. Although this review adhered to PRISMA standards and applied RoB2 and GRADE, certainty is tempered by small sample sizes, single-center designs, and heterogeneity in drug type, dose, route, and outcome measurement. According to the GRADE assessment (Supplement 3) (http://www.medicinaoral.com/medoralfree01/aop/jced_63455_s03), the certainty of evidence ranged from moderate to low, mainly due to heterogeneity and sample size limitations, yet the consistency of effect direction supports clinical applicability. These limitations underscore the need for larger, multicenter randomized controlled trials with standardized protocols to strengthen the evidence base.
Conclusions
According to the findings of the present systematic review and meta-analysis, both NSAIDs and corticosteroids are effective preemptive medications for reducing postoperative pain in symptomatic irreversible pulpitis. NSAIDs provide rapid early relief, while corticosteroids sustain analgesia into the first two postoperative days. Both significantly reduce the need for rescue analgesics, making them valuable tools in opioid-sparing pain management strategies. Clinicians should tailor drug selection based on patient needs, contraindications, and desired timing of pain control. By integrating pharmacological evidence with guideline recommendations and psychosocial strategies, endodontic practice can further optimize patient-centered pain management. Clinicians should consider NSAID premedication for immediate pain control and corticosteroids when extended postoperative relief is desirable, particularly in cases where NSAIDs are contraindicated. Future multicenter RCTs should aim to define optimal dosing and combined regimens to balance efficacy and safety in endodontic pain management. These findings reinforce the evidence base for incorporating preemptive anti-inflammatory strategies into routine endodontic protocols.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Macfarlane TV Glenny AM Worthington HV Systematic review of population-based epidemiological studies of oro-facial pain J Dent 200129745167.1180932310.1016/s 0300-5712(01)00041-0 · doi ↗ · pubmed ↗
- 2Alhilou AM Al-Moraissi EA Bakhsh A Christidis NNäsman P Pain after emergency treatments of symptomatic irreversible pulpitis and symptomatic apical periodontitis in the permanent dentition: a systematic review of randomized clinical trials Front Oral Health 202341147884.3792059210.3389/froh.2023.1147884 PMC 10618681 · doi ↗ · pubmed ↗
- 3Yang SE Park YG Han K Min JA Kim SY Dental pain related to quality of life and mental health in South Korean adults Psychol Health Med 201621898192.2645632410.1080/13548506.2015.1098781 · doi ↗ · pubmed ↗
- 4Virdee SS Effective Pain Management Strategies in Endodontic Therapy Dent Update 20164365756,82914865410.12968/denu.2016.43.6.575 · doi ↗ · pubmed ↗
- 5Mc Gillivray A Dutta A The influence of laser-activated irrigation on post-operative pain following root canal treatment: A systematic review J Dent 2024144104928.3848486710.1016/j.jdent.2024.104928 · doi ↗ · pubmed ↗
- 6Azim AA Merdad K Peters OA Diagnosis consensus among endodontic specialists and general practitioners: An international survey and a proposed modification to the current diagnostic terminology Int Endod J 20225511120211.3598473010.1111/iej.13816 PMC 9826047 · doi ↗ · pubmed ↗
- 7Abraham D Singh A Goyal A Symptomatic Irreversible Pulpitis Induces Increased Levels of Human NLRP 3 in Gingival Crevicular Fluid Compared to Saliva: A Case Control Observational Study J Endod 2023491114806.3763457810.1016/j.joen.2023.08.013 · doi ↗ · pubmed ↗
- 8Barbero-Navarro I Irigoyen-Camacho ME Zepeda-Zepeda MA Ribas-Perez D Castaño-Seiquer A Sofian-Pauliuc I Understanding the Dynamics of Inflammatory Cytokines in Endodontic Diagnosis: A Systematic Review Diagnostics (Basel)202414111099.3889362610.3390/diagnostics 14111099 PMC 11171959 · doi ↗ · pubmed ↗