Oral amelanotic melanoma in a 73-year-old patient: A rare case report and literature review
José-Alcides-Almeida de Arruda, Victor-Zanetti Drumond, Lucas-Guimarães Abreu, Cinthia-Verónica-Bardález-López de Cáceres, Pablo-Agustin Vargas, Patrícia-Carlos Caldeira, Felipe-Paiva Fonseca, Ricardo-Alves Mesquita, Bruno-Augusto-Benevenuto de Andrade, Tarcília-Aparecida Silva

TL;DR
A rare case of non-pigmented oral melanoma in a 73-year-old woman is reported, highlighting diagnostic challenges and the importance of immunohistochemistry.
Contribution
This is the first report of TRP-2 immunoexpression in oral amelanotic melanoma and the sixth such case in Latin America.
Findings
Oral amelanotic melanoma in older adults is rare and often misdiagnosed due to lack of pigmentation.
Immunohistochemistry confirmed the diagnosis and revealed TRP-2 positivity, a first in this subtype.
The patient's case highlights the need for a detailed immunohistochemical panel to avoid diagnostic errors.
Abstract
Oral melanoma is an aggressive neoplasm that predominantly affects older adults. The amelanotic subtype is exceedingly rare, and its diagnosis is challenging due to the absence of pigmentation. Herein, we report a rare case of oral amelanotic melanoma in an older adult, discussed in light of the available literature. A 73-year-old Brazilian female patient presented with pain and discomfort in the left transverse palatal rugae. Clinically, the lesion appeared as a single, sessile, dome-shaped nodule with a coloration similar to the adjacent mucosa. Histopathological examination revealed a spindle-cell malignant neoplasm with epithelioid nests within a fibrous stroma, lacking melanin pigmentation. Immunohistochemistry was positive for pan-cytokeratin AE1/AE3, vimentin, S100 protein, Melan-A, SOX10, NSE, and TRP-2, with a high Ki-67 index. The patient died two months after diagnosis. A…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
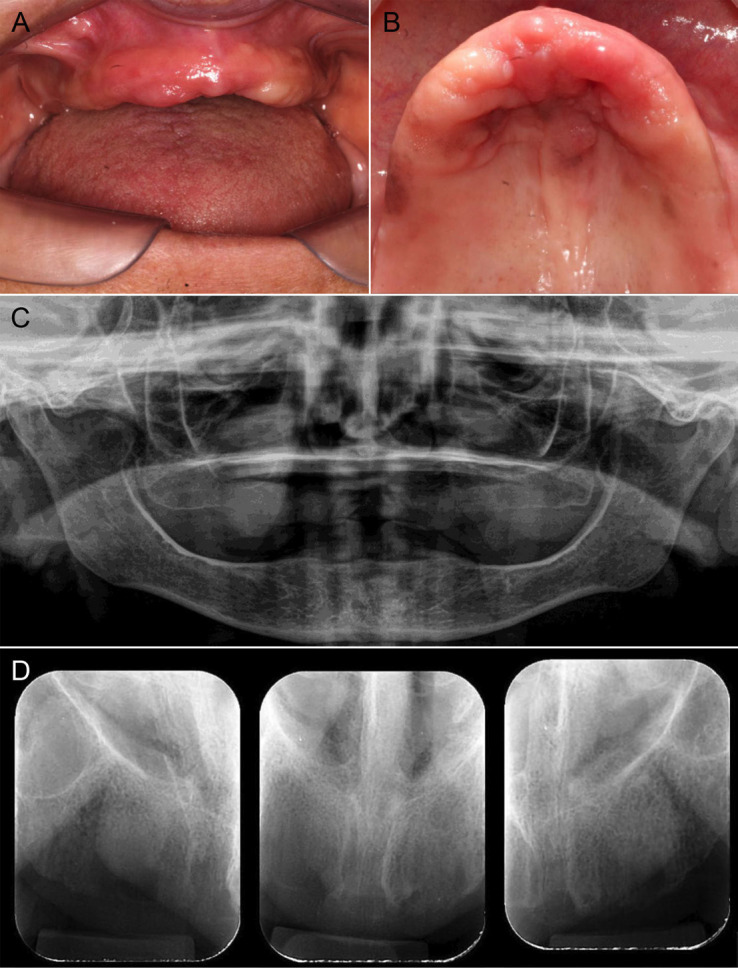 Figure 1
Figure 1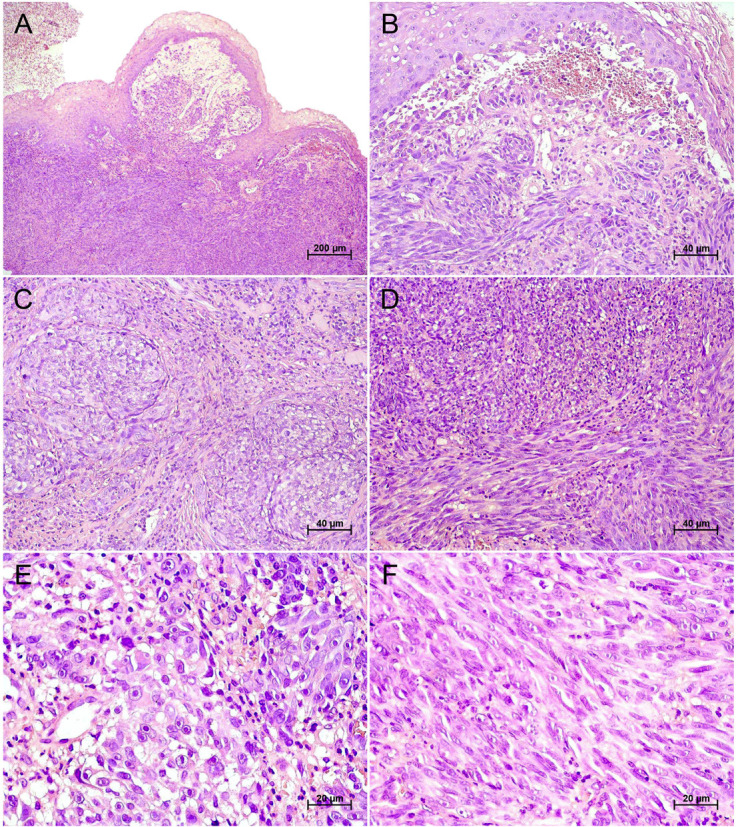 Figure 2
Figure 2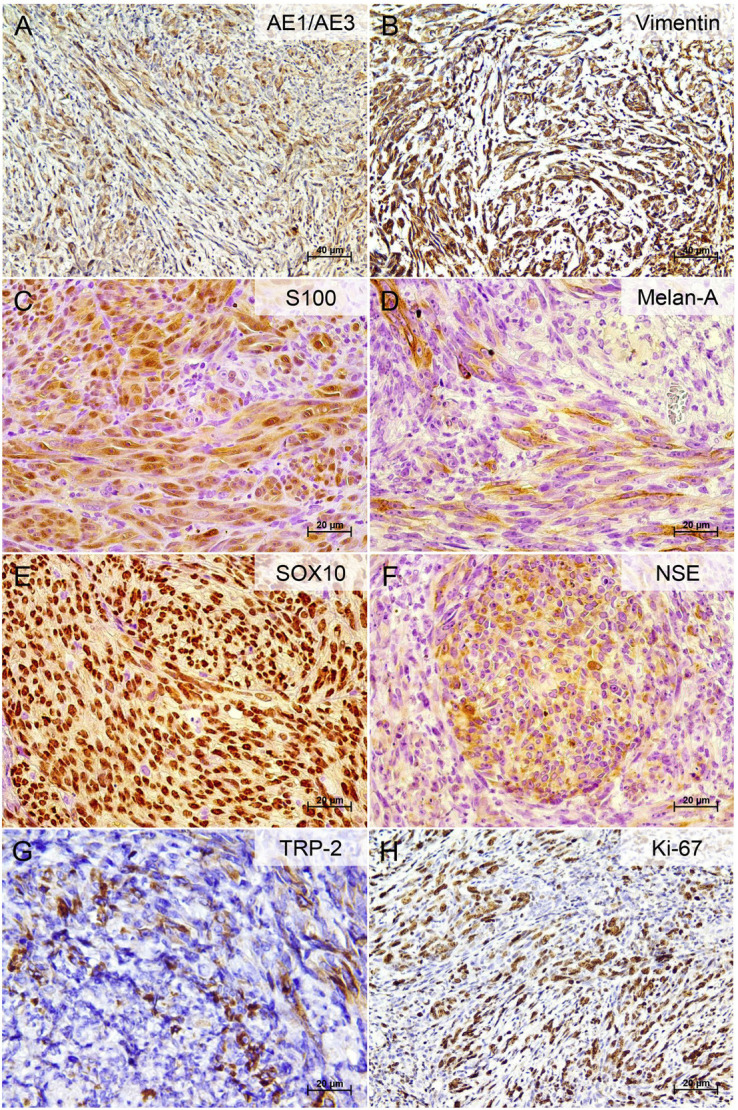 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCutaneous Melanoma Detection and Management · Oral and Maxillofacial Pathology · Laser Applications in Dentistry and Medicine
Introduction
Oral melanoma is an uncommon and highly aggressive malignant neoplasm originating from melanocytes within the ectoderm-derived mucosal epithelium (1 , 2). Epidemiologically, it accounts for 0.2%-0.8% of all melanomas, 31%-35.6% of mucosal melanomas, and approximately 0.03% of all malignant neoplasms (2 - 7). Historically, dark tumors described as melanosis were first reported as early as the 5th century B.C. by Hippocrates and later by Rufus of Ephesus. The first surgical description of melanoma is attributed to John Hunter in 1787, while William Norris provided the earliest account of amelanotic melanoma in 1857 (8). Amelanotic melanoma is a rare hypomelanotic variant, accounting for approximately 8% of all melanomas, with the head and neck affected in nearly 26% of cases (9 , 10). Oral amelanotic melanoma is exceedingly rare. In general, middle-aged men in their 50s, particularly with lesions involving the maxilla, are most frequently affected (11). At the molecular level, amelanotic melanoma is characterized by dysregulation of melanin synthesis, cell cycle regulation, and apoptotic pathways. Although tumor cells retain their melanocytic lineage and the inherent biological capacity to produce melanin, this ability is often absent or markedly diminished (12). Clinically, oral amelanotic melanoma is frequently misdiagnosed or detected at a late stage because it emulates non-neoplastic proliferative processes (11 , 13). For this reason, it has been termed "the great masquerader" (14). Histopathologically, most cases exhibit an epithelioid morphology, although spindle cell and desmoplastic patterns have also been described (12). Pigmentation is demonstrable microscopically in fewer than 5% of tumor cells yet remains clinically inapparent, further complicating diagnosis (15). Compared with conventional melanoma, oral amelanotic melanoma demonstrates greater aggressiveness, higher recurrence rates, and significantly worse survival outcomes (9). Therefore, incorporating oral melanoma screening into routine geriatric dental care, supported by structured diagnostic algorithms, may substantially improve early detection and survival in this vulnerable population (2). Given the scarcity of reports on oral amelanotic melanoma, particularly among older adults, we present to literature an additional case involving a 73-year-old female patient. We also provide a review of the available data on oral amelanotic melanoma in the geriatric population (60 years).
Case Report
A 73-year-old female Brazilian patient was referred to the oral medicine service due to pain and discomfort while wearing a maxillary complete denture. The duration of the symptom was unknown. She reported no history of smoking, alcohol consumption, or trauma to the maxillofacial region. Her family history was notable for type II diabetes and unspecified cancer-related deaths. Her medical history included type II diabetes mellitus, systemic arterial hypertension, bilateral cataracts, and Alzheimer's disease. She was under pharmacological treatment with captopril (50 mg/day), hydrochlorothiazide (25 mg/day), metformin (500 mg twice daily), and donepezil (5 mg/day). Extraoral examination revealed no lymphadenopathy in the cervical lymph node chain. Intraorally, a single sessile, dome-shaped lesion was observed on the left transverse palatal rugae, measuring approximately 15×15×8 mm. The lesion had a smooth surface, firm consistency on palpation, and coloration similar to the adjacent mucosa, without signs of ulceration. On the anterior alveolar ridge, discrete erythematous areas were noted, whereas on the posterior alveolar ridge, multiple diffuse brownish macules of varying sizes were in place. These pigmented lesions were flat (macular) with irregular contours, smooth surfaces, and no evidence of ulceration erosion or induration (Fig. 1A,B).
Figure 1. Clinical and radiographic features of oral amelanotic melanoma. (A) Intraoral view showing a completely edentulous maxilla. (B) Occlusal view of the maxilla revealing a single sessile, dome-shaped lesion located on the left transverse palatal rugae, measuring approximately 15×15×8 mm. The lesion exhibits a smooth surface and coloration similar to the adjacent mucosa. Discrete erythematous areas are observed on the anterior alveolar ridge, while the posterior and lateral ridges display multiple diffuse brownish macules of varying sizes. (C) Panoramic and (D) periapical radiographs showing no evidence of bone alterations.
Panoramic and periapical radiographs revealed no evidence of underlying bone alterations (Fig. 1C,D). Based on the clinical characteristics, the primary diagnostic hypothesis for the dome-shaped lesion was inflammatory fibrous hyperplasia, whereas the differential diagnoses for the pigmented lesions included racial (physiological) pigmentation, drug-induced pigmentation, and post-traumatic or post-inflammatory hyperpigmentation. Blood tests revealed an HbA1c level of 8%, while the complete blood count and coagulation profile showed no significant abnormalities. Histopathological examination of the biopsy of the dome-shaped lesion revealed a malignant neoplasm composed predominantly of pleomorphic spindle cells arranged in interlacing fascicles, interspersed with ovoid and cuboidal epithelioid cells forming nests and solid cords within a dense and well-vascularized fibrous stroma. Focal areas of mixed inflammatory infiltrate were present, and no melanin pigment was observed in the neoplastic cells (Fig. 2).
Figure 2. Histopathological features of oral amelanotic melanoma. (A) Low-power view of an exophytic, nodular, non-pigmented mucosal lesion composed of an infiltrative malignant neoplasm extending from the epithelial–connective interface into the underlying lamina propria. (B) Interface region showing atypical epithelioid melanocytic cells arranged in nests immediately beneath the surface epithelium. (C) Tumor nests of atypical epithelioid cells with enlarged nuclei, prominent nucleoli, and moderate nuclear pleomorphism. (D) Solid sheets of neoplastic cells with high cellularity embedded in a desmoplastic stroma. (E) High-power view of epithelioid tumor cells with vesicular nuclei, amphophilic nucleoli, abundant eosinophilic cytoplasm, frequent mitotic figures (including atypical forms), and absence of melanin pigmentation. (F) Spindle-cell component composed of elongated nuclei, hyperchromasia, and fascicular arrangement (hematoxylin and eosin staining; 40×, 200×, and 400×).
Immunohistochemically, the tumor cells exhibited strong immunopositivity for pan-cytokeratin (AE1/AE3), vimentin, S100 protein, Melan-A, SOX10, and NSE, as well as diffuse cytoplasmic staining for TRP-2. The Ki-67 labeling index was approximately 70% (Fig. 3).
Figure 3. Immunohistochemical profile of the oral amelanotic melanoma. (A) Cytoplasmic immunoreactivity for pan-cytokeratin AE1/AE3 in spindle-shaped tumor cells (focal to moderate). (B) Strong cytoplasmic expression of vimentin in spindle cell areas. (C) Diffuse and intense nuclear and cytoplasmic positivity for S100 protein. (D) Focal cytoplasmic staining for Melan-A in tumor cells. (E) Strong and diffuse nuclear expression of SOX10 in tumor cells. (F) Cytoplasmic positivity for NSE in nodular aggregates of tumor cells. (G) Focal cytoplasmic expression of TRP-2 in scattered tumor cells. (H) Ki-67 nuclear staining indicating a proliferative index of 70% (immunohistochemistry with DAB (3,3′-diaminobenzidine) chromogen; 200× and 400×).
Tumor cells were negative for HMB45, LCA, -SMA, and GFAP. Table 1 depicts information on the antibodies used. Based on these findings, a diagnosis of amelanotic melanoma was established. The patient was referred to an oncology service but died two months after the diagnosis without receiving any treatment.
Discussion
Data from a review in the electronic databases PubMed, Scopus, Embase, and Web of Science indicate that oral amelanotic melanoma in older adults is rare and has seldom been addressed in the literature, with only 35 cases documented hitherto (Table 2) (16 - 41).Table 2
Estimates of oral melanoma are largely derived from isolated case reports and small case series, with approximately 2,230 cases identified (1). This differs from oral amelanotic melanoma, for which only 55 cases have been reported thus far (11), and with cutaneous melanoma, which accounted for 325,000 new cases worldwide in 2020, with projections reaching 510,000 by 2040 (42). Previous research has indicated that 9% of oral melanoma cases correspond to the amelanotic variant (43). In the present review, Asia emerged as the leading continent (57.7%), with Japan accounting for 34.6% of all documented cases. It has been suggested that oral melanoma may occur more frequently in Asian populations, although the etiological basis remains elusive (1). In contrast, the relative proportion of oral melanoma among all mucosal melanomas in Caucasian populations is generally lower, although studies have reported comparable proportions of 30-50% in both Caucasian and Japanese cohorts (44 , 45). By comparison, the literature on cutaneous amelanotic melanoma is dominated by studies from Europe and North America (10). We herein contribute by describing a case of oral amelanotic melanoma in a 73-year-old patient, which likely represents the sixth reported case from Latin America.
Oral amelanotic melanoma shows a slight male predilection, similar to cutaneous forms, which affect men in approximately 55% of cases (9 , 11). Interestingly, our review demonstrated a female predominance (57.1%). Although sex distribution varies across studies (2), a systematic review reported a global male-to-female ratio of 1.2:1 (1). Age patterns were also distinctive. Most cases reported in the literature have occurred in the seventh decade of life, whereas a recent Brazilian series described a mean age of 53.6 years (38). Overall, the mean age at diagnosis of oral melanoma lies between 65 and 69 years, with incidence peaking at 70-79 years (2). Given this age profile, geriatricians and geriatric dentists should be particularly vigilant when non-pigmented or asymptomatic lesions arise. Integrating oral melanoma screening into whole-body skin examinations within geriatric care pathways is, therefore, strongly recommended (2).
Clinically, oral amelanotic melanoma presents as an insidious neoplasm with a broad spectrum of morphological appearances that are often deceptive and largely responsible for delayed diagnosis (11). In older adults, the mean time to detection was approximately six months. The nodular pattern was the most prevalent (34.3%), most commonly arising in the maxillary gingiva, while ulceroproliferative (25.7%), sessile, pedunculated, or erythematous forms were also noted. These findings reflect the clinical spectrum described by Bansal et al. (11) and Soares et al. (38), in which ulcerated/reddish masses of the palate and gingiva predominated. Only four oral amelanotic melanomas were reported in other locations, including the buccal mucosa (31 , 35), tongue (38), and lip (34). Most lesions measured between 10 and 60 mm, a range comparable to that of conventional oral melanoma (2). Approximately one-third of older adults reported pain (31.4%), whereas asymptomatic lesions were equally common (34.3%), illustrating the silent nature of the tumor in its early stages. Furthermore, the reviewed literature indicates that most patients (70%) presented with lymphadenopathy at the time of diagnosis.
The present case posed considerable diagnostic challenges, as the lesion clinically resembled a non-neoplastic proliferative process, i.e., an inflammatory fibrous hyperplasia. This presentation is reminiscent of a case reported by Soares et al. (38), involving a 33-year-old female with a small sessile nodule on the incisive papilla that was initially misdiagnosed as a pyogenic granuloma. Indeed, the literature emphasizes that oral amelanotic melanoma may atypically present as pyogenic granuloma-like lesions, with gingival cases frequently assigned a presumptive diagnosis of reactive processes (13). Such clinical overlaps are not a mere eventuality; they directly contribute to diagnostic delays and reinforce the principle that all lesions with a benign clinical appearance should undergo microscopic examination.
In our patient, additional contiguous mucosal alterations were also observed, including discrete erythematous macules and diffuse brownish macules on the alveolar ridge. At that stage, our differential diagnoses included physiological pigmentation, drug-induced pigmentation, and post-traumatic or post-inflammatory pigmentation. These considerations were supported by reports attesting that, in the skin, hydrochlorothiazide has been associated with hyperpigmentation, as has donepezil (commonly prescribed for dementia due to Alzheimer's disease), although no cases involving the oral mucosa have been documented (46). Likewise, drug-induced lichenoid reactions in the oral cavity are most often associated with nonsteroidal anti-inflammatory drugs and antihypertensive agents, including -blockers, angiotensin-converting enzyme inhibitors, and diuretics (e.g., hydrochlorothiazide) (47). However, these lesions are typically indistinguishable from oral lichen planus, and drug-related pigmentation can only be confirmed when a temporal association with medication use is established, along with resolution following drug withdrawal and exclusion of other etiologies (48). Another important aspect of the present report was the patient's diagnosis of Alzheimer's disease. To our knowledge, no prior studies have described oral amelanotic melanoma in an older adult with this condition. Of particular note, it has been demonstrated that melanoma cells require amyloid beta (A), a polypeptide involved in Alzheimer's disease, for survival and growth within the brain parenchyma (49). Although the primary tumor in our case was located in the palate, the possibility of distant metastasis cannot be entirely ruled out.
Histopathologically, the present case exhibited a spindle-cell predominance, which is the most frequent pattern in oral amelanotic melanomas. Nonetheless, the literature also documents epithelioid, round, and undifferentiated morphologies (38). In the absence of melanin, diagnosis becomes particularly challenging due to the highly variable sarcomatoid-like presentation of these lesions. Oral amelanotic melanoma may mimic other malignant neoplasms, including epithelial and mesenchymal tumors, lymphomas, and sarcomas. Consequently, immunohistochemical markers such as S100 protein, HMB45, and Melan-A are essential for establishing the diagnosis. When confronted with non-pigmented spindle or epithelioid tumors, a minimal diagnostic panel including S100 protein, SOX10, Melan-A, HMB45, and TRP-2 is recommended. SOX10, in particular, has proven to be a highly sensitive and specific nuclear marker, surpassing S100 in specificity and aiding the recognition of spindle-cell and desmoplastic variants often negative for Melan-A or MiTF (50 , 51). Interestingly, HMB45 was negative in our case. Two previous reports (29 , 51) have also described HMB45-negative oral amelanotic melanomas. Although HMB45 is widely used, it is less sensitive than S100 protein or Melan-A, and negativity should not preclude the diagnosis, particularly in spindle-cell and desmoplastic variants. Moreover, HMB45 and Melan-A may yield false negatives in amelanotic or desmoplastic melanomas and false positives in perivascular epithelioid cell or adrenocortical tumors, requiring interpretative caution (50).
Additionally, we demonstrated immunoexpression of TRP-2 in the present case. TRP-2 (dopachrome tautomerase/DCT) is a melanocyte differentiation enzyme involved in melanin synthesis and has been evaluated in human melanomas with variable sensitivity. Itakura et al. (54) reported TRP-2 positivity in 83% of primary and 100% of metastatic melanomas, while most nevi were negative, supporting its specificity. Strobel et al. (55) confirmed TRP-2 expression in approximately 50% of human melanomas and emphasized its association with a differentiated phenotype. Compared with conventional melanocytic markers, TRP-2 tends to be retained in certain amelanotic or desmoplastic variants in which HMB-45 or Melan-A may be absent, reinforcing its complementary diagnostic value (54 , 55). The inclusion of TRP-2 within "MDX-style" cocktails, combining HMB45, MART-1, and tyrosinase, has been shown to improve detection accuracy in diagnostically challenging lesions, particularly when integrated with SOX10 (50 , 56). To the authors' knowledge, this represents the first published report of TRP-2 immunoexpression in a human oral amelanotic melanoma.
The Ki-67 proliferation index in the present case was approximately 70%, consistent with evidence that oral amelanotic melanomas display higher proliferative indices (mean 64%) compared with their pigmented counterparts (mean 31%) (38). Such findings support the hypothesis that amelanotic tumors may represent a less differentiated, or even dedifferentiated, phenotype of conventional melanoma, associated with increased biological aggressiveness. Similar results have been reported in older patients, among whom spindle-cell morphology, variable HMB45 expression, and aggressive clinical outcomes were consistently reported (23 , 24 , 32).
Previous studies have shown that mutations in KIT, NRAS, and BRAF V600 are uncommon in oral melanomas, with reported frequencies around 10% or less (57 , 58). Ichimura et al. (59) further confirmed the absence of BRAF V600 mutations and identified amplifications in RICTOR, CDK4, MDM2, KDR, and NF1 as more frequent molecular events in oral melanomas. The literature addressing oral amelanotic melanoma is particularly scarce; nonetheless, a rare non-canonical BRAF double substitution (T599I/V600K) has been described in an amelanotic melanoma with oral metastases, underscoring the molecular heterogeneity of this phenotype (60). In our case, however, molecular testing was not performed, which represents a limitation of this report.
Findings from the present review revealed a mortality rate of 94.4%. These results reinforce the poor prognosis of oral melanoma and the limited effectiveness of conventional therapies, consistent with previous reports highlighting surgery as the mainstay, but rarely curative approach (1). Radiotherapy and chemotherapy, when used in isolation, were almost uniformly associated with poor survival, in line with the intrinsic radioresistance and chemoresistance of mucosal melanomas (61). Even multimodal regimens combining surgery, radiotherapy, and/or chemotherapy frequently resulted in disease progression, recurrence, or distant metastases. Immune checkpoint blockade and molecularly targeted therapies have shown promise in cutaneous melanoma and selected mucosal subtypes but remain underexplored in oral presentations (62). It is important to note that older adults with oral melanoma often face additional challenges related to treatment tolerability. Diagnostic delays further contribute to high mortality rates, as most cases are identified at stage III or IV, frequently with nodal or distant metastases (1). Survival rates for oral amelanotic melanoma are considerably lower than those for conventional oral melanoma, with 3-year and 5-year survival rates of 18.75% and 6.25%, respectively (11). We have previously emphasized the importance of a multidisciplinary team in delivering supportive care, addressing both physical and psychosocial needs, and ensuring comfort and dignity during the terminal phase of the disease (2).
In summary, this report describes the sixth documented case of oral amelanotic melanoma in an older adult from Latin America. Given its rarity and aggressive behavior, diagnosis is particularly challenging, as it often mimics non-neoplastic or reactive proliferations in clinical presentations. In the absence of melanin, a panel of immunohistochemical markers is indispensable to confirm the diagnosis.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Thuaire A Nicot R Boileau M Raoul G Descarpentries C Mouawad F Germain N Mortier L Schlund M Oral mucosal melanoma - A systematic review J Stomatol Oral Maxillofac Surg 20221235 e 425e 432.3513459010.1016/j.jormas.2022.02.002 · doi ↗ · pubmed ↗
- 2de Arruda JAA Drumond VZ Tenório JR Abreu LG Silva TA Mesquita R Ade Andrade BAB Oral Melanoma in Older Adults: Epidemiology, Molecular Landscape, and Treatment Strategies Pigment Cell Melanoma Res 2025383 e 70017.4022993710.1111/pcmr.70017 · doi ↗ · pubmed ↗
- 3Mehra T Grözinger G Mann S Guenova E Moos RRöcken M Claussen CD Dummer R Clasen S Naumann A Garbe C Primary localization and tumor thickness as prognostic factors of survival in patients with mucosal melanoma P Lo S One 2014911 e 112535.2538355310.1371/journal.pone.0112535 PMC 4226547 · doi ↗ · pubmed ↗
- 4Breik O Sim F Wong T Nastri A Iseli TA Wiesenfeld D Survival Outcomes of Mucosal Melanoma in the Head and Neck: Case Series and Review of Current Treatment Guidelines J Oral Maxillofac Surg 201674918591871.2706359010.1016/j.joms.2016.03.008 · doi ↗ · pubmed ↗
- 5Cohen Goldemberg Dde Melo A Cde Melo Pino LC Thuler LCS Epidemiological profile of mucosal melanoma in Brazil Sci Rep 2020101505.3194921010.1038/s 41598-019-57253-6PMC 6965610 · doi ↗ · pubmed ↗
- 6Oranges CM Sisti G Nasioudis D Tremp MDI Summa PG Kalbermatten DF Largo RD Schaefer DJ Hard Palate Melanoma: A Population-based Analysis of Epidemiology and Survival Outcomes Anticancer Res 2018381058115817.3027520410.21873/anticanres.12921 · doi ↗ · pubmed ↗
- 7Şendişçi Gök R TercanlıHA ten-year literature review of oral malignant melanoma cases: A meta-analysis study J Stomatol Oral Maxillofac Surg 2024125(4S)101922.3879591010.1016/j.jormas.2024.101922 · doi ↗ · pubmed ↗
- 8Rebecca VW Sondak VK Smalley KSA brief history of melanoma: from mummies to mutations Melanoma Res 2012222114122.2239541510.1097/CMR.0b 013e 328351 fa 4d PMC 3303163 · doi ↗ · pubmed ↗