An unusual facial location for a meningioma. Case report
Emilia María Montoro-Serrano, María José Morán-Soto, Íñigo Aragón-Niño, José Luis del Castillo-Pardo de Vera, María Álvaro-Martínez, José Luis Cebrián-Carretero

TL;DR
A rare case of a meningioma tumor appearing on the face of a woman with a history of brain tumors is reported, highlighting the need to consider such tumors in facial mass diagnoses.
Contribution
This case adds to the limited literature on extracranial meningiomas by presenting a rare facial location example in a patient with prior intracranial tumors.
Findings
The patient had a subcutaneous facial lesion confirmed as an atypical meningioma (WHO grade II).
The case is classified as Type III cutaneous meningioma according to the López classification.
The report emphasizes the importance of considering extracranial meningiomas in facial mass differential diagnoses.
Abstract
Meningiomas are the most common primary tumors of the central nervous system (CNS), but their occurrence in extracranial locations such as soft tissue or skin is extremely rare. They may be congenital (Type I), ectopic soft tissue meningiomas (Type II), or secondary to an intracranial meningioma (Type III), according to the López classification. We report the case of a woman with a history of multiple intracranial atypical meningiomas (WHO grade II) who presented with a subcutaneous lesion in the left malar region. Histopathological examination confirmed the diagnosis of atypical meningioma (WHO grade II). This case represents a rare example of a Type III cutaneous meningioma according to the López classification. It underscores the importance of considering extracranial meningiomas in the differential diagnosis of facial subcutaneous masses, particularly in patients with a history of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
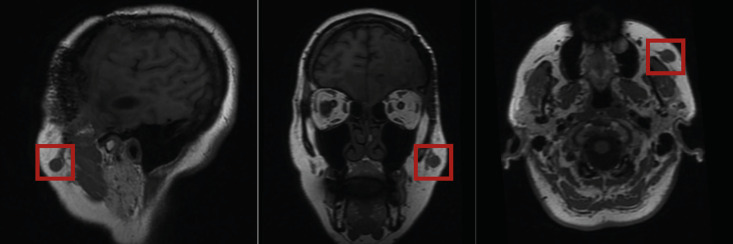 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMeningioma and schwannoma management · Neurofibromatosis and Schwannoma Cases · Facial Nerve Paralysis Treatment and Research
Introduction
Meningiomas are extra-axial tumors that arise from arachnoid cap cells of the meninges and represent the most common primary neoplasms of the central nervous system (CNS) (1). The term "meningioma" was first introduced by Harvey Cushing in 1922. They account for approximately 30% of all intracranial tumors. The incidence increases with age, with most cases diagnosed in adults, particularly after the age of 65, and shows a clear female predominance. About 98.6% of meningiomas are benign (WHO grade I), while the remainder are atypical (grade II) or, more rarely, malignant or anaplastic (grade III). Most meningiomas originate intracranially, and although rare, extracranial extension can occur. There are also reports of purely ectopic meningiomas (2). The most frequent locations include the convexity, parasagittal region, sphenoid wing, middle cranial fossa, spine, and olfactory groove (1). Primary meningiomas of the facial nerve are extremely rare. Gao et al. described a case of a meningioma intrinsic to the facial nerve extending from the porus acusticus internus to the geniculate ganglion (3), while Deep et al. reported one involving the entire intratemporal course of the facial nerve from the cerebellopontine angle to the stylomastoid foramen (2). The first case of a cutaneous meningioma was reported by Max Winkler in 1904, and the classification system proposed by López et al. in 1974 remains the basis for current categorization (4).
Case Report
We present the case of a 55-year-old woman with a subcutaneous mass in the left malar region. She reported noticing the lesion approximately four months before presentation. The patient had a history of multiple surgical interventions for intracranial meningiomas. Seven years earlier, she underwent complete excision of a left pterional meningioma, which was histologically diagnosed as an atypical meningioma (WHO grade II), followed by adjuvant radiotherapy. Three years later, she experienced recurrence with several intracranial lesions and underwent reoperation and re-irradiation. One year afterward, radiological follow-up revealed two new lesions suggestive of meningioma recurrence. A conservative approach with continued imaging surveillance was initially chosen. However, due to progressive increase in size and number of lesions, a new surgical intervention was performed, confirming once again an atypical meningioma (WHO grade II). During the following year of surveillance, further intracranial progression was detected along with the development of a new subcutaneous lesion in the left malar region. This lesion measured approximately 2 × 2 cm, was firm on palpation, slightly mobile, and with unaffected overlying skin. The patient also exhibited left-sided facial paralysis with inability to raise her eyebrow. Because of these clinical findings, a parotid malignant lesion was initially suspected due to apparent facial nerve involvement. Upon review of her medical history, it was determined that the facial paralysis predated this lesion and resulted from previous surgical procedures. Magnetic resonance imaging (MRI) performed for evaluation of intracranial disease demonstrated a well-circumscribed, round lesion measuring 2 cm in diameter, isointense to gray matter on T1-weighted images, and embedded in the subcutaneous tissue of the left malar region. In the sagittal plane, a tail-like extension connecting the lesion to the underlying musculature was observed (Fig. 1).
Figure 1. Sagittal, coronal, and axial reconstruction planes in T1-weighted sequences. A well-circumscribed round lesion measuring approximately 2 cm arises from the soft tissues, is isointense to gray matter, and shows a tail-like extension toward the underlying musculature.
Fine-needle aspiration (FNA) of the subcutaneous mass was performed and suggested meningioma infiltration. During subsequent surgery for resection of recurrent intracranial meningiomas, the malar lesion was also excised through a transcutaneous approach, revealing a well-defined, rounded mass approximately 1.7 cm in diameter. Histopathological examination confirmed the diagnosis of atypical meningioma (WHO grade II).
Discussion
The presence of a subcutaneous meningioma may result either from metastasis or from a primary cutaneous meningioma. Regarding metastases, both benign and malignant meningiomas can disseminate, although this is extremely uncommon, with an overall probability of approximately 0.1%, rising to 30% in anaplastic meningiomas. Reported metastatic sites include bone, spinal cord, lung, liver, and subcutaneous tissue. Cutaneous meningiomas that develop de novo are even rarer. They typically arise in the skin of the head, face, or paraspinal regions. These lesions are usually slow-growing, well-circumscribed, and benign in nature, presenting clinically as asymptomatic subcutaneous nodules (4). Several theories have been proposed to explain their development: Head trauma leading to displacement of meningeal tissue with subsequent proliferation at the displaced site. Entrapment of heterotopic arachnoid cell rests within the soft tissues during embryogenesis. Migration of arachnoid cells along cranial or spinal nerves. Persistence of an atretic encephalocele with residual intracranial connections. Vascular turbulence causing detachment and embolization of arachnoid cell clusters (4 , 5). Magnetic resonance imaging (MRI) is the modality of choice for diagnosing and characterizing meningiomas. However, computed tomography (CT) is often the initial study, especially when lesions are incidentally detected. On non-contrast CT, meningiomas usually appear slightly hyperdense compared with normal brain tissue and may show calcifications and a variable degree of peritumoral edema. Correlations between age, sex, tumor size, growth rate, location, and histologic subtype have been suggested but not conclusively proven. Following contrast administration, homogeneous enhancement is typically observed. Hyperostosis, although uncommon, is a highly specific finding usually associated with skull base meningiomas. Increased heterogeneity on imaging has been linked to a higher probability of malignant histologic variants (6). As mentioned above, MRI remains the gold standard for detailed characterization. Meningiomas are extra-axial, usually homogeneous, and well-circumscribed lesions arising from a broad dural base. Certain features, such as the "dural tail sign," can help distinguish them from other extra-axial tumors; this finding is seen in about 72% of cases. Nonetheless, it is not specific to meningiomas, though it is most commonly associated with them. Signal characteristics in T2-weighted images may correlate with histologic subtypes: approximately half of meningiomas are isointense to gray matter, while the remainder appear hyperintense. T2 hyperintensity often corresponds to soft, hypervascular tumors such as microcystic, secretory, or angiomatous variants. On T1-weighted images, meningiomas are typically isointense. Some studies have suggested that higher histologic grades (II and III) may show increased diffusion restriction on DWI/ADC sequences, although evidence remains inconsistent (7). Based on their pathological and clinical characteristics, López et al. classified cutaneous meningiomas developing outside the CNS into three types (Table 1) (5 , 8).
Our case corresponds to an atypical meningioma (WHO grade II) and a Type III cutaneous meningioma according to the López classification, due to its association with a known intracranial meningioma in an adult patient. This behavior of intracranial meningiomas is not uncommon. It has been estimated that up to 20% of intracranial meningiomas may develop synchronous extracranial extension, most frequently in the head and neck region (8). Surgical seeding of tumor cells is a recognized complication of meningioma surgery, first reported by Cushing in 1938. In our case, although the lesion was not located directly within the surgical field, it was situated near the most caudal aspect of a previous coronal approach, suggesting a possible relation to surgical seeding, consistent with the tail-like extension observed on imaging (9). Avecillas-Chasin et al. described several risk factors associated with scalp metastases of meningiomas, including reoperations, immunosuppression, radiotherapy, cerebrospinal fluid fistula, and delayed wound healing. Although our lesion was located outside the scalp, some of these risk factors-such as multiple surgical procedures and repeated radiotherapy-were also present in our patient (9 , 10).
Conclusions
Cutaneous meningiomas are extremely rare lesions that may arise de novo or as secondary extensions of intracranial tumors. This case illustrates a Type III cutaneous meningioma, according to the López classification, located in the unusual malar region and associated with a history of multiple intracranial atypical meningiomas. Awareness of this entity is essential for clinicians, as extracranial meningiomas should be considered in the differential diagnosis of facial subcutaneous masses, particularly in patients with a history of meningioma surgery or radiotherapy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Casas Parera IBáez A Banfi N Blumenkrantz Y Halfon MJ Barros M Meningiomas en neurooncología Neurol Argent 20168321026.
- 2Deep NL Gnagi SH Carpentieri DF Adelson PD Weisskopf PA Facial nerve meningioma: A cause of pediatric facial weakness Otol Neurotol 2017383 e 812.2789860610.1097/MAO.0000000000001293 · doi ↗ · pubmed ↗
- 3Gao W Zi D Lu L Facial nerve meningioma: A case mimicking facial nerve schwannoma Ear Nose Throat J 202210164024.3302334110.1177/0145561320962582 · doi ↗ · pubmed ↗
- 4Porumb-Andrese E Grigore T Popa University of Medicine and Pharmacy, Iaşi, Romania, Costea CF, Macovei G, Dumitrescu GF, Blaj LA, et al Humps and bumps of head: review of meningiomas of the scalp. Rom J Morphol Embryol 202464446773.10.47162/RJME.64.4.02PMC 1086369238184826 · doi ↗ · pubmed ↗
- 5Cheng MF Cheung LK Dodoo EA Po YCA case of giant cutaneous Lopez type III meningioma of the scalp J Neurol Surg Rep 20238401 e 215.3687463210.1055/s-0043-1764322 PMC 9984268 · doi ↗ · pubmed ↗
- 6Gaillard F Mahmoud Q Vargas Carvajal D Meningioma Radiopaedia org 2008
- 7Fotakopoulos G Tsolaki V Aravantinou-Fatorou A Georgakopoulou VE Spandidos DA Papalexis P Tarantinos K Trakas N Sklapani P Mathioudakis N Chlapoutakis S Lavdas E Uncommon and atypical meningiomas and imaging variants: A report of 7 cases Med Int (Lond)202226353669915310.3892/mi.2022.60PMC 9829240 · doi ↗ · pubmed ↗
- 8Lopez DA Silvers DN Helwig EB Cutaneous meningiomas--a clinicopathologic study Cancer 197434372844.485123110.1002/1097-0142(197409)34:3<728::aid-cncr 2820340332>3.0.co;2-u · doi ↗ · pubmed ↗