Prolonged corrected QT interval and Torsades de pointes following electrical cardioversion of atrial fibrillation in a young woman
Hassan Elzain, Mohamed Elkalifa Elawad Elhassan, Karar Mahmoud Nadir Mohamed, Mohamed Adel Mostafa, Heba Fathy Ismail, Jasem H Redha, Anas Bedawi Babiker

TL;DR
A young woman developed a dangerous heart rhythm after a routine procedure to treat atrial fibrillation, highlighting the need for close monitoring.
Contribution
Reports a rare case of QT prolongation and torsades de pointes following cardioversion in a young patient with no prior repolarization issues.
Findings
QT interval prolonged to over 600 ms immediately after cardioversion.
Torsades de pointes occurred, requiring defibrillation and dopamine infusion for recovery.
Full recovery was achieved without arrhythmia recurrence after treatment.
Abstract
Electrical cardioversion is a widely used and generally safe procedure for restoring sinus rhythm in atrial fibrillation. However, it may rarely precipitate significant proarrhythmic complications. We report the case of a 35-year-old woman with a history of atrial septal defect closure who presented with persistent symptomatic atrial fibrillation. She underwent successful synchronized direct current cardioversion, but immediately developed marked prolongation of the corrected QT interval (>600 ms) followed by recurrent episodes of torsades de pointes, one requiring defibrillation. Intravenous magnesium was administered, but QT prolongation persisted in association with hypotension and bradycardia. Dopamine infusion was initiated to increase heart rate, which contributed to gradual QT normalization. The patient recovered fully without recurrence of arrhythmia. This case highlights a rare…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
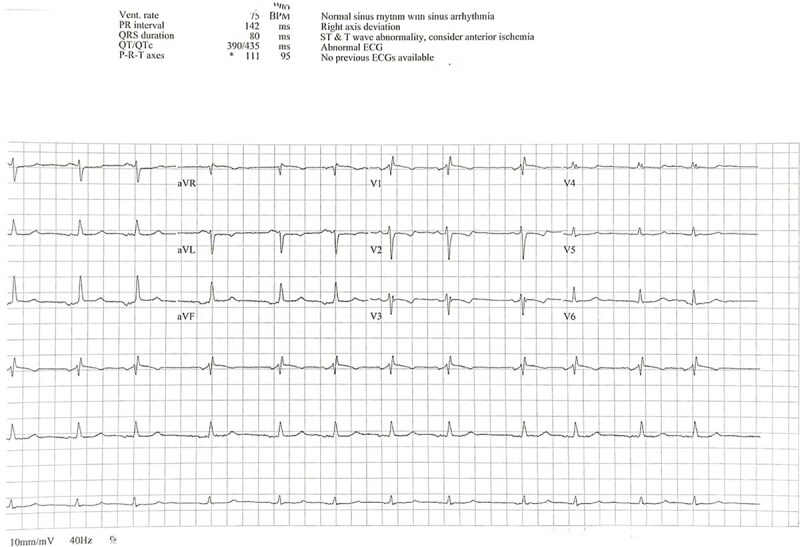 Figure 1
Figure 1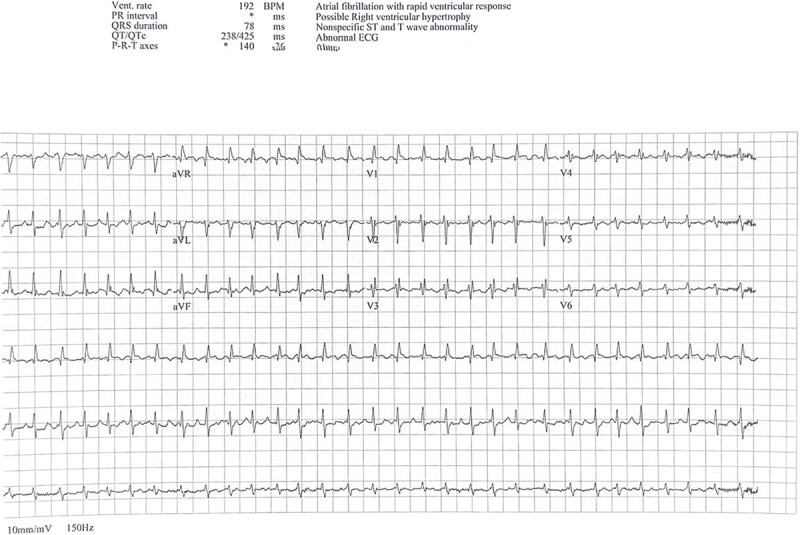 Figure 2
Figure 2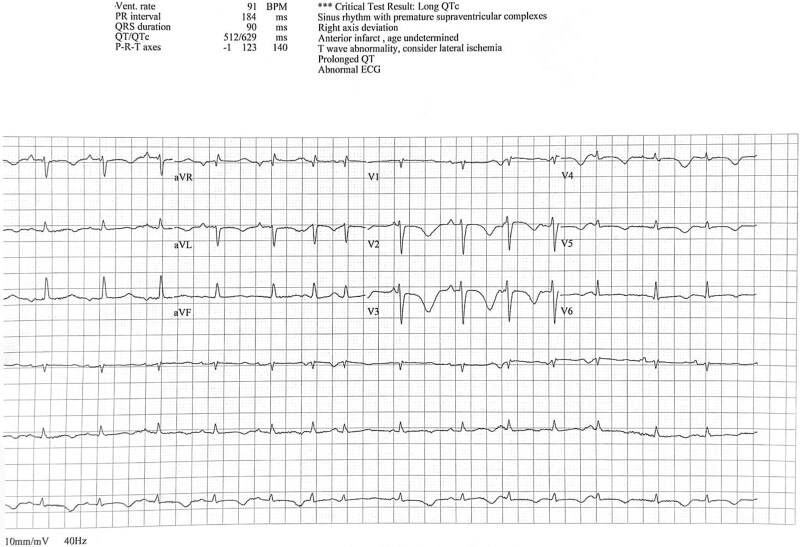 Figure 3
Figure 3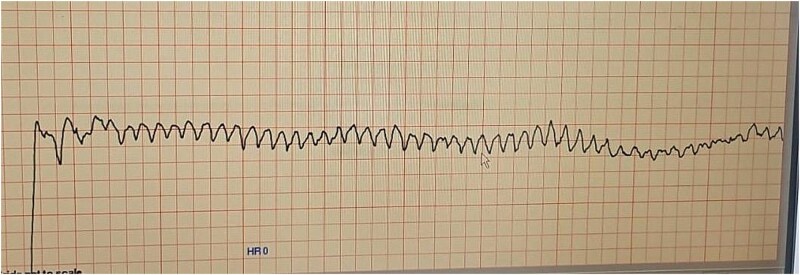 Figure 4
Figure 4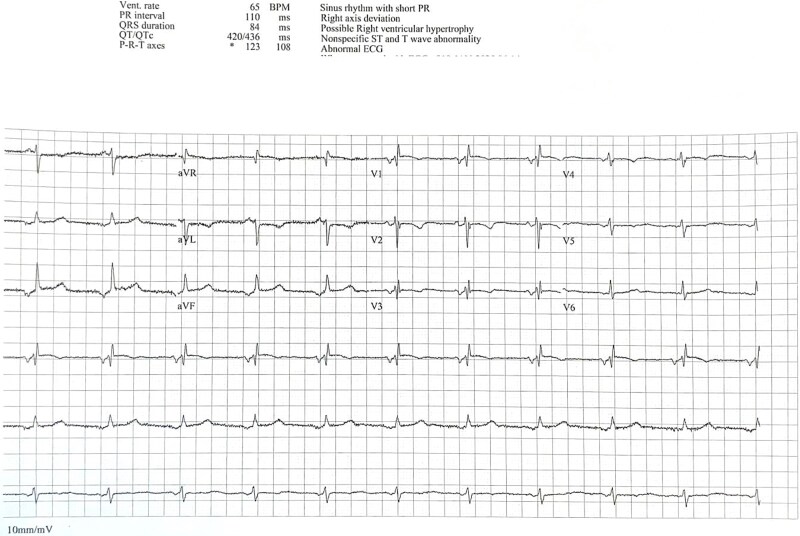 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac electrophysiology and arrhythmias · Magnesium in Health and Disease · Cardiac Arrhythmias and Treatments
Introduction
Electrical cardioversion is a well-established and widely utilized intervention for restoring sinus rhythm in patients with atrial fibrillation. While considered safe and effective, the procedure is not entirely without risk. Rare but serious complications, including proarrhythmic events such as QT interval prolongation and Torsades de Pointes, have been documented even in patients without prior repolarization abnormalities [1]. Prompt recognition of such adverse effects is crucial, as they may result in life-threatening arrhythmias if not managed appropriately. This report presents a unique case of post-cardioversion QT prolongation and Torsades de Pointes in a young woman with atrial fibrillation, underscoring the importance of close ECG monitoring following cardioversion.
Case report
A 35-year-old woman with a previous history of atrial septal defect (ASD) closure presented with symptomatic atrial fibrillation (AF). She had been diagnosed initially with paroxysmal AF in 2022, at which time her ECG showed sinus rhythm with a normal QT interval (Fig. 1). Bisoprolol was initiated, but she was subsequently lost to follow-up.
Baseline ECG showing normal sinus rhythm with normal QT interval.
From early 2025, she started experiencing increasingly frequent episodes of palpitations and fatigue. During the three months prior to presentation, her symptoms became persistent, and ECG confirmed progression to permanent AF (Fig. 2). She was initiated on apixaban 5 mg twice daily in addition to her ongoing bisoprolol. A transthoracic echocardiogram revealed mild left atrial dilation, mild mitral regurgitation, and preserved left ventricular systolic function without other significant abnormalities. Given her persistent symptoms, elective electrical cardioversion was planned.
ECG showing atrial fibrillation prior to cardioversion.
The patient underwent synchronized direct current cardioversion (DCCV) under sedation, successfully restoring sinus rhythm. Immediately following the procedure, a repeat ECG revealed profound QT interval prolongation (QTc > 600 ms) (Fig. 3). Within minutes, she developed recurrent episodes of polymorphic ventricular tachycardia (Torsades de Pointes), documented clearly on telemetry monitoring (Fig. 4). One sustained episode necessitated immediate defibrillation, successfully restoring sinus rhythm.
ECG immediately after cardioversion showing marked QT prolongation.
Telemetry recording of torsades de pointes following cardioversion.
In response, she was promptly managed with continuous intravenous magnesium infusion. Despite optimal magnesium supplementation, significant QT prolongation persisted, accompanied by hypotension (BP 90/50 mmHg) and relative bradycardia (heart rate approximately 60 bpm). Given the ongoing risk and the known association between bradycardia and QT prolongation, a dopamine infusion was initiated to elevate the heart rate and reduce the QT interval.
Over the subsequent 48 hours, there was gradual shortening of the QT interval. By the third day, repeat ECG confirmed normalization of QTc (Fig. 5). The patient remained hemodynamically stable thereafter, without recurrence of ventricular arrhythmias. Following normalization of the QT interval, genetic testing for congenital long QT syndrome was conducted and returned negative.
ECG on day 3 showing normalization of QT interval.
Discussion
This case highlights an uncommon but potentially life-threat-ening complication following cardioversion of atrial fibrillation—marked QT prolongation leading to Torsades de Pointes. Although direct current cardioversion (DCCV) is generally safe and widely used to restore sinus rhythm, it carries a small risk of adverse events, particularly in the immediate post-procedural period [1].
Atrial fibrillation induces both electrical and structural remodeling in the atria and ventricles. Restoration of sinus rhythm through cardioversion can unmask transient repolarization abnormalities and lead to QT interval prolongation. Several mechanisms have been proposed to explain this phenomenon, including abrupt shifts in heart rate and autonomic tone, which may expose latent repolarization defects. These changes in ventricular repolarization dynamics are typically transient, but in rare instances, they can trigger malignant arrhythmias such as Torsades de Pointes [2, 3].
Our patient had a normal QT interval prior to cardioversion but developed a markedly prolonged QT interval immediately after restoration of sinus rhythm, eventually resulting in TdP. The absence of QT-prolonging medications, electrolyte abnormalities, or structural heart disease further supports a primary cardioversion-related mechanism.
QT prolongation and Torsades de Pointes (TdP) are medical emergencies that require immediate intervention. Intravenous magnesium sulfate is considered the first-line therapy for TdP, regardless of the serum magnesium level, due to its stabilizing effect on myocardial repolarization and ability to suppress early afterdepolarizations [4, 5]. In cases of hemodynamically unstable or sustained TdP, immediate direct current (DC) cardioversion is the treatment of choice. Delay in defibrillation may lead to degeneration into ventricular fibrillation and sudden cardiac death [6, 7]. In our patient, one sustained episode of TdP required prompt defibrillation, successfully restoring sinus rhythm.
In cases where QT prolongation persists despite magnesium therapy, especially when associated with bradycardia, increasing the heart rate becomes a critical strategy to prevent further episodes of TdP. Elevating the heart rate reduces the repolarization interval, thereby minimizing the risk of early afterdepolarizations that precipitate TdP. This can be achieved pharmacologically using agents such as isoproterenol or dopamine, or by temporary pacing in more severe or recurrent cases. In our patient, dopamine infusion was initiated to maintain a heart rate above 80 bpm, which contributed to QT interval normalization and arrhythmia suppression over the following days [7, 8].
This case underscores the critical need for vigilant ECG monitoring following electrical cardioversion, even in patients without prior repolarization abnormalities. While QT prolongation after cardioversion is often transient and benign, it may, in rare cases, precipitate life-threatening arrhythmias such as Torsades de Pointes. Early identification and timely intervention are essential, particularly when QT prolongation persists or arrhythmias recur despite appropriate therapy [7]. Although this is a single case and its findings cannot be generalized, it highlights a potentially underrecognized complication. Further studies are warranted to assess the prevalence, predictors, and optimal monitoring strategies for QT prolongation and arrhythmic events post-cardioversion.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Guédon-Moreau L, Gayet JL, Galinier M. et al. Incidence of early adverse events surrounding direct current cardioversion of persistent atrial fibrillation. Therapie. 2007;62:45–8. 10.2515/therapie:200700917374347 · doi ↗ · pubmed ↗
- 2Tan HL, Smits JP, Loef A. et al. Electrocardiographic evidence of ventricular repolarization remodelling during atrial fibrillation. Europace. 2008;10:99–104. 10.1093/europace/eum 27018094018 · doi ↗ · pubmed ↗
- 3Omondi A, Sirinvaravong N, Spears J. et al. Marked Q Tc reduction immediately following direct current cardioversion of atrial fibrillation: clinical implications and mechanisms. JACC Clin Electrophysiol 2023;9:543–54. 10.1016/j.jacep.2022.10.03136752461 · doi ↗ · pubmed ↗
- 4Drew BJ, Ackerman MJ, Funk M. et al. Prevention of torsade de pointes in hospital settings: a scientific statement from the American Heart Association and the American College of Cardiology Foundation. Circulation. 2010;121:1047–60. 10.1161/CIRCULATIONAHA.109.19270420142454 PMC 3056123 · doi ↗ · pubmed ↗
- 5Al-Khatib SM, Stevenson WG, Ackerman MJ. et al. 2017 AHA/ACC/HRS guideline for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: a report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines and the Heart Rhythm Society. J Am Coll Cardiol 2018;72:e 91–220. 10.1016/j.jacc.2017.10.05429097296 · doi ↗ · pubmed ↗
- 6Tisdale JE . Drug-induced QT interval prolongation and torsades de pointes: role of the pharmacist in risk assessment, prevention and management. Can Pharm J (Ott) 2016;149:139–52. 10.1177/171516351664113627212965 PMC 4860751 · doi ↗ · pubmed ↗
- 7Zeppenfeld K, Tfelt-Hansen J, de Riva M. et al. 2022 ESC guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Eur Heart J 2022;43:3997–4126. 10.1093/eurheartj/ehac 26236017572 · doi ↗ · pubmed ↗
- 8Cohagan B, Brandis D. Torsade de pointes. In: Stat Pearls [Internet]. Treasure Island (FL): Stat Pearls Publishing ed. 2023.29083738 · pubmed ↗