Traumatic Spinal Cord Infarction Associated With Elevated Intracranial and Intraspinal Pressure in a Pediatric Patient: A Case Report and Review of the Literature
Julianna L Barbaro, Priyanka Shah, Adam Donithan, Anthony Staples, Mandeep Rana

TL;DR
A rare case of spinal cord infarction in an 11-year-old girl is reported, highlighting the challenges in diagnosing and managing this condition in children.
Contribution
This case report documents a previously unrecorded association between elevated intracranial and intraspinal pressure and traumatic spinal cord infarction in a pediatric patient.
Findings
An 11-year-old girl presented with traumatic spinal cord infarction following a fall, confirmed by MRI.
Elevated opening pressure during lumbar puncture was observed, a finding not previously documented in the literature.
The case highlights the diagnostic challenges of distinguishing spinal cord infarction from myelitis in pediatric patients.
Abstract
Spinal cord ischemia (SCI) in the pediatric population is rare and not well characterized. Initial diagnosis is often delayed, and there are no standardized, evidence-based management strategies. Risk factors and etiologies vary and include trauma, thrombotic or embolic disease, infection, vasculitis, cerebellar herniation, arteriovenous malformation, cardiovascular interventions, scoliosis correction, sickle cell disease, and idiopathic causes. We present a case of an 11-year-old girl with anterior spinal artery (ASA) syndrome who presented four days after a fall with back pain, bilateral lower extremity weakness, and numbness. On examination, she demonstrated objective weakness and decreased pain and temperature sensation (worse on the left than the right) in her lower extremities. Diagnostic workup revealed a thoracic ASA infarction, thoracic transverse process fracture, lumbar…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2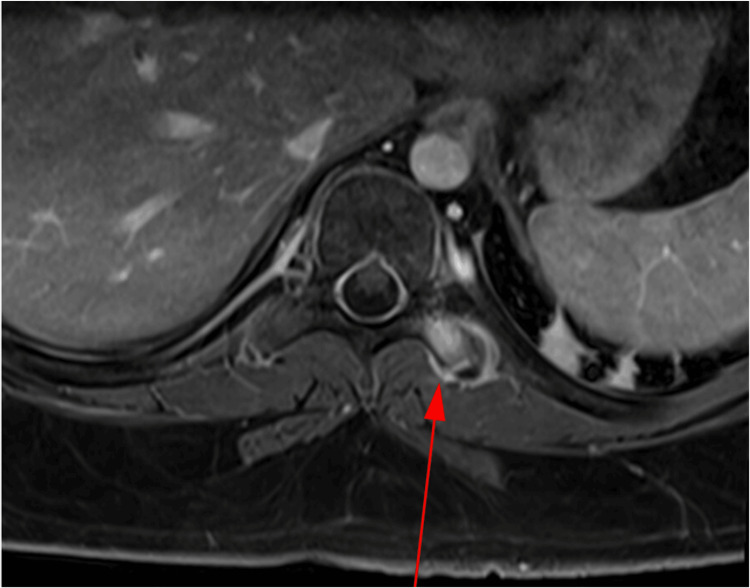 Figure 3
Figure 3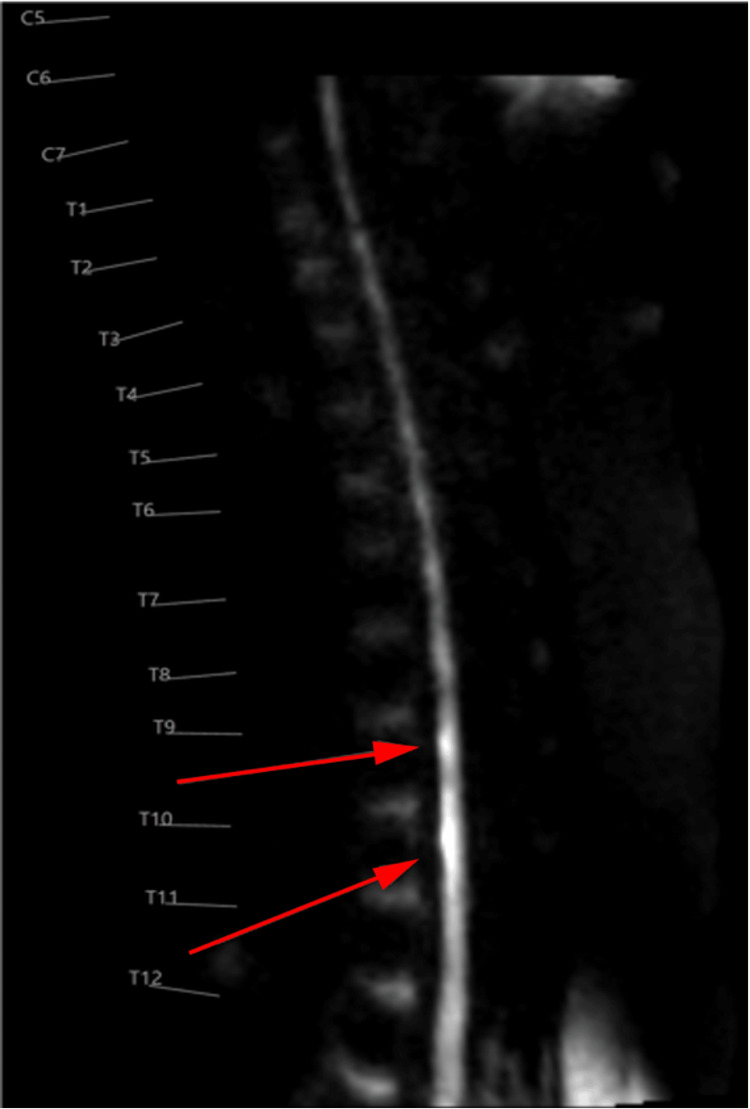 Figure 4
Figure 4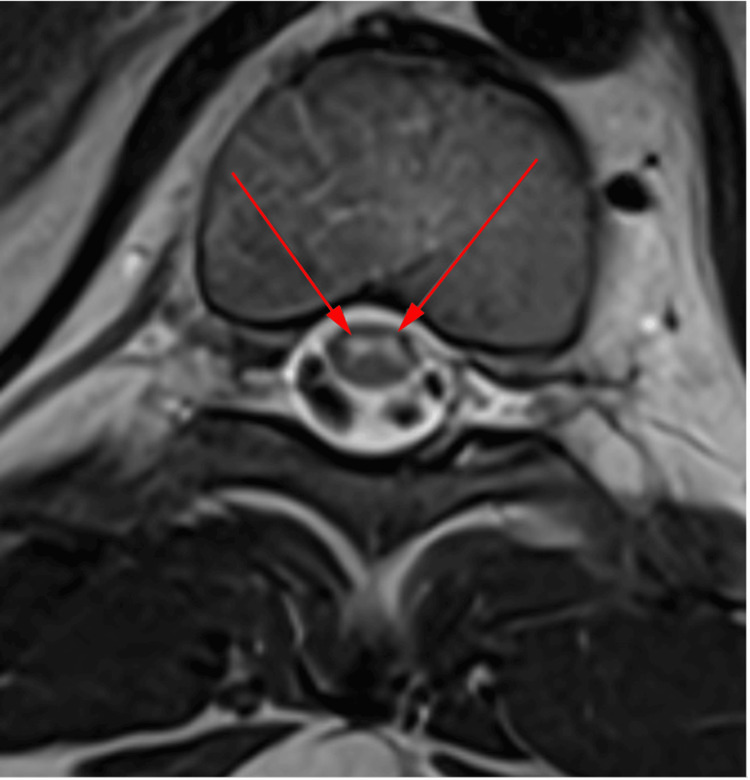 Figure 5
Figure 5| Variables | On admission | Reference range | Unit |
| White blood cells | 7.6 | 4.5-13.5 | K/µL |
| Hemoglobin | 12.2 | 11.5-15.5 | g/dL |
| Platelets | 301 | 130-400 | K/µL |
| Factor V (Leiden) mutation | Negative | Negative | N/A |
| Factor VIII | 91 | 60-200 | % |
| Fibrinogen | 324 | 175-425 | mg/dL |
| Protein S activity | 112 | 60-140 | % |
| D-dimer | 0.39 | <0.5 | µg FEU/mL |
| Antithrombin III | 116 | 80-135 | % |
| Total protein | 7.3 | 6.4-8.3 | g/dL |
| Albumin | 4.5 | 3.2-5.0 | g/dL |
| Aspartate aminotransferase | 22 | 15-37 | U/L |
| Alanine aminotransferase | 27 | 10-49 | U/L |
| HbA1c | 5.7 | <5.7 | % |
| Cholesterol | 143 | <170 | mg/dL |
| LDL | 91 | <110 | mg/dL |
| HDL | 34 | >45 | mg/dL |
| Glucose | 84 | 60-99 | mg/dL |
| CRP | <0.50 | <1.0 | mg/dL |
| TSH | 0.572 | 0.64-6.27 | µIU/mL |
| ANA | Negative | Negative | N/A |
| Serum MOG antibody | Negative | Negative | N/A |
| Serum aquaporin-4 antibody | Negative | Negative | N/A |
| CSF oligoclonal bands | Absent | Absent | N/A |
| CSF autoimmune encephalopathy panel | Negative | Negative | N/A |
| CSF meningoencephalitis panel | Negative | Negative | N/A |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAortic Disease and Treatment Approaches · Spinal Cord Injury Research · Spinal Hematomas and Complications
Introduction
Spinal cord ischemia (SCI) is a rare but serious condition that can cause long-lasting deficits requiring multidisciplinary care. In adults, it accounts for approximately 1% of all strokes, whereas in children, SCI is so uncommon that its incidence is unknown [1]. SCI is responsible for roughly 6% of acute myelopathies and 1-2% of vascular neurological pathologies [2].
Currently, few reports exist in the pediatric literature regarding SCI diagnosis, etiology, prognosis, and treatment. Pediatric SCI risk factors include blood flow obstruction associated with cardiovascular malformations, cerebellar herniation, iatrogenic or traumatic vascular injury, infection, thrombosis or embolus, and vasculitis [3]. The presentation of SCI can be highly variable, ranging from minor weakness to tetraplegia, which makes accurate diagnosis challenging [4].
We present a pediatric case of anterior spinal artery (ASA) syndrome likely secondary to a fall. This case uniquely contributes to the literature because the patient demonstrated markedly elevated opening pressure (OP) on lumbar puncture (LP) despite the absence of inflammatory markers in CSF, traumatic brain injury, hydrocephalus, or mass lesion, an observation not previously described.
Case presentation
An 11-year-old girl with a medical history of asthma, attention deficit hyperactivity disorder, and prediabetes presented to an outside ED with sudden-onset bilateral lower extremity (BLE) numbness, weakness, and pain.
The patient reported falling from approximately six feet, landing on her feet, and then falling backward, hitting her head. At the time of injury, she denied loss of consciousness or back pain. Three days after the fall, her ambulation progressively worsened until she could no longer walk, prompting her initial ED visit. After a negative CT scan and X-ray, she was discharged but presented the following day to our ED and was subsequently admitted.
Neurological assessment revealed normal mental status, no papilledema, and intact strength and deep tendon reflexes in the bilateral upper extremities (BUE). Motor strength in the right lower extremity (RLE) ranged from 2/5 (hip flexion) to 4/5 (ankle mobility), whereas the left lower extremity (LLE) was predominantly 0/5. Reflexes were 2+ in the BLE patellar and LLE Achilles, but 1+ in the RLE Achilles, with a positive Babinski sign bilaterally. Sensory examination was intact to light touch and vibration in all four extremities. Pain and temperature sensation were normal in the BUE but decreased in the BLE, with complete loss of sharp and temperature sensation below the thoracic vertebrae T11-T12. Finger-to-nose testing was intact with no tremor.
The patient remained paraplegic on admission and for the first four days of hospitalization. The neurological differential diagnosis included acute myelitis, acute demyelinating process, and SCI.
MRI of the brain and cervical (C) spine revealed no abnormalities. MRI of the thoracic (T) spine demonstrated symmetric, ventral-predominant cord signal abnormality from T8 to T12 (Figure 1, Figure 2).
Sagittal T2-weighted MRI of the thoracic spine showing ventral-dominant cord signal abnormality from T8 to T9 through T11 to T12, indicated by red arrows
Sagittal post-contrast T1-weighted MRI of the thoracic spine showing no evidence of enhancement from T8 to T9 through T11 to T12, indicated by red arrows
Imaging of the thoracic spine revealed marrow edema and enhancement of the left T9-T10 transverse process and surrounding tissue, consistent with an acute fracture (Figure 3). MRI of the lumbar (L) spine demonstrated a left-sided L2-L4 paraspinal muscle strain. The radiological differential diagnosis included SCI versus transverse myelitis.
Axial T1-weighted MRI of the thoracic spineThe red arrow demonstrates a left transverse process fracture, corroborated on CT of the thoracic spine (not shown).
Cardiac evaluation and coagulation profile were normal, and other laboratory investigations were non-contributory (Table 1).
Neurosurgery evaluated the patient, and, in the absence of compressive pathology or spinal instability, no surgical intervention was indicated. The patient subsequently underwent a fluoroscopy-guided LP, with opening and closing pressures of 54 and 32 cm H₂O, respectively. CSF analysis was normal, without evidence of inflammation (Table 1), and fundoscopy revealed no papilledema despite the markedly elevated OP. Given concerns for transverse myelitis, she was treated with IV methylprednisolone (MPS) 1,000 mg daily for five days.
The thoracic cord signal abnormality and T9-T10 transverse process fracture prompted further imaging using thin axial slices via diffusion-weighted imaging (DWI). Symmetric, ventral-predominant T8-T12 cord signal abnormality in an “Owl’s eye” configuration with restricted diffusion, consistent with SCI, was observed (Figure 4, Figure 5). Differential diagnoses included ASA infarction versus neuromyelitis optica, the latter rarely producing an Owl’s eye sign.
Sagittal DWI of the thoracic spine demonstrating diffusion restriction at the site of the signal abnormality from T8 to T9 through T11 to T12, indicated by red arrowsDWI, diffusion-weighted imaging
Axial T2-weighted MRI of the thoracic spineThe red arrows demonstrate a hyperintense signal abnormality in the ventral spinal cord, representative of an Owl’s eye configuration.
Over the course of the week, the patient gradually improved in BLE motor strength and sensory function. She was fitted with bilateral pressure-relief ankle-foot orthoses, allowing ambulation using a walker and gait belt. After an eight-day hospital stay, she was discharged to inpatient rehabilitation for one week, followed by twice-weekly outpatient rehabilitation.
At follow-up with neurology at two and five months post-injury, she demonstrated progressive improvement, with a narrow-based, well-balanced gait. Weakness persisted but was significantly improved compared to hospitalization. She was advised to continue physical therapy and to return in four months, or sooner if neurological symptoms recurred.
Discussion
The ASA supplies the anterior two-thirds of the spinal cord. Although the spinal cord has robust vascularity, the mid-thoracic region is most vulnerable to infarction due to a smaller vessel diameter and weaker vascular supply from the unpaired artery of Adamkiewicz, which arises around T9-T12 and anastomoses with the ASA to supply the conus medullaris [4]. Approximately 75% of thoracolumbar spinal cord infarction cases present with an ASA infarction [5].
The mechanism of SCI following trauma is poorly understood, though three primary theories dominate. First, a more flexible vertebral column and less elastic spinal cord increase susceptibility to hyperflexion injuries, causing vascular spasm and cord insult [6]. Second, tearing of small spinal or radicular artery intimal linings can lead to dissection or thrombosis secondary to hematoma compression [4,7]. Third, fibrocartilaginous embolization of the nucleus pulposus can cause both traumatic and degenerative SCIs [8].
Compared to adults, extensive collateral blood flow in children renders their spinal cords less vulnerable to SCI [3]. The extent of disability in adulthood following pediatric SCI is evaluated using the American Spinal Injury Association impairment scale, which ranges from A (complete functional loss) to E (normal function). Approximately 50% of adults who experienced pediatric SCI are tetraplegic [9].
The median age of pediatric SCI is 14 years [9]. Traumatic ASA occlusion in pediatric SCI typically presents with acute back pain, followed by a symptom-free latent period, with neurological signs arising within 48 hours [1,7]. Three pediatric SCI case reports demonstrated normal BLE movement and sensation up to 48 hours prior to complete paraplegia [10]. In our patient, back pain and neurological symptoms began three days after the traumatic event. The literature describes eight cases of delayed symptom onset following SCI, ranging from two hours to four days, in children aged 1-10 years [7].
The gold standard for SCI diagnosis is MRI of the spine with axial thin-slice DWI [2]. Acute SCI on DWI demonstrates diffusion restriction, although imaging is often challenging due to the small spinal canal and cord diameter, respiratory motion, and CSF pulsation [4]. Spinal angiography can be useful for identifying occlusion of spinal cord vessels, particularly when MRI cannot resolve fine vascular details [7]. In this case, angiography was deemed unnecessary due to a patent artery of Adamkiewicz and a T9-T10 signal abnormality on MRI, indicating ASA occlusion. While smaller arterial occlusions could theoretically have been missed, this would not have altered treatment.
Our patient’s MRI of the thoracic spine with DWI demonstrated a classic Owl’s eye sign from T8 to T12. The Owl’s eye sign refers to bilateral symmetric T2 hyperintensities in the anterior horns of the spinal cord on axial MRI, indicating gray matter involvement. Spinal cord infarction is the most characteristic cause, particularly in the ASA territory. Acute flaccid myelitis, which typically presents with asymmetric flaccid weakness and is often associated with viral infections (not observed in this patient), also affects gray matter. The presence of a thoracic transverse process fracture favored trauma-related infarction. Neuromyelitis optica spectrum disorder less commonly shows the Owl’s eye sign compared to spinal cord infarction and typically presents with longitudinally extensive transverse myelitis affecting both gray and white matter [11]. Transverse myelitis may show central cord involvement, longitudinally extensive lesions, and variable enhancement, with or without the Owl’s eye pattern [12].
A markedly elevated OP of 54 mmHg, in the absence of inflammatory markers, supports pediatric ASA SCI as the most likely diagnosis, a finding not previously reported. The spinal cord is contained within a rigid vertebral canal, so edema following SCI increases intraspinal pressure [13]. Intracranial pressure (ICP) and intraspinal pressure are directly connected and equilibrate via the CSF system, with lumbar CSF pressure accurately reflecting ICP when CSF pathways are patent [14]. This relationship is governed by the Monro-Kellie doctrine, which states that the intracranial and spinal compartments form a continuous, closed system, wherein volume changes in one component must be compensated by reciprocal changes in others [15,16].
Although laminectomy and CSF drainage were considered to relieve pressure, these interventions were not pursued due to ongoing motor improvement and neurosurgical assessment showing a patent artery of Adamkiewicz, no compressive pathology, and no spinal instability. Fehling’s guidelines for adults with acute SCI recommend early laminectomy for cord decompression; however, two pediatric exploratory laminectomy cases were ineffective [7]. Emerging preclinical evidence suggests aspirin may exert neuroprotective effects in SCI models by reducing neuronal apoptosis and inflammation via the Nrf2/HO-1 pathway, though this has not been validated in humans [17].
Given alternative differentials, IV MPS 1,000 mg was administered daily for five days. This therapy may confer short-term motor improvement as a neuroprotectant and reduce secondary injury, but long-term benefits beyond six months are unproven [18].
Our patient maintained activities of daily living, though residual motor deficits persisted despite intensive physical therapy.
Conclusions
Our case report highlights a thoracic ASA infarction diagnosed via axial thin-slice DWI, accompanied by elevated OP, a thoracic transverse process fracture, and lumbar paraspinal muscle strain, all managed conservatively with physical therapy. Although SCI is uncommon, its complications can be long-lasting and debilitating. A high index of suspicion for vascular insult to the spinal cord is warranted in any trauma, particularly involving the trunk, chest, or abdomen, to enable timely diagnosis and intervention. While spinal angiography was not performed in this patient, it may be useful in select cases to identify vasospasm, thrombus, vessel avulsion, or underlying vascular malformations. Further studies are needed to clarify optimal strategies for managing SCI.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Spinal cord ischemia revealed in the context of altered consciousness: a pediatric case report Brain Dev Case Rep Cellauro S Korff C Cipullo MB Vargas MI Polito A Corbisier T 10002622024
- 2Spinal cord ischemia: practical imaging tips, pearls, and pitfalls AJNR Am J Neuroradiol Vargas MI Gariani J Sztajzel R Barnaure-Nachbar I Delattre BM Lovblad KO Dietemann JL 8258303620152532449210.3174/ajnr.A 4118 PMC 7990611 · doi ↗ · pubmed ↗
- 3Ischemic spinal cord infarction in children without vertebral fracture Pediatr Neurol Nance JR Golomb MR 2092163620071743790210.1016/j.pediatrneurol.2007.01.006PMC 2001276 · doi ↗ · pubmed ↗
- 4Pediatric spinal cord infarction following a minor trauma: a case report Spinal Cord Ser Cases Morshid A Jadiry HA Chaudhry U Raghuram K 956202010.1038/s 41394-020-00344-8PMC 755058033046690 · doi ↗ · pubmed ↗
- 5Traumatic spinal cord infarction in a child: case report and review of literature Surg Neurol Robles LA 5295346720071744562710.1016/j.surneu.2006.07.016 · doi ↗ · pubmed ↗
- 6Spinal cord injury without radiographic abnormalities in children J Neurosurg Pang D Wilberger JE Jr 114129571982708648810.3171/jns.1982.57.1.0114 · doi ↗ · pubmed ↗
- 7Traumatic infarction of the spinal cord in children J Neurosurg Choi JU Hoffman HJ Hendrick EB Humphreys RP Keith WS 608610651986377244610.3171/jns.1986.65.5.0608 · doi ↗ · pubmed ↗
- 8Spinal cord infarction following minor trauma in children: fibrocartilaginous embolism as a putative cause J Neurosurg Pediatr Reisner A Gary MF Chern JJ Grattan-Smith JD 4454501120132341413310.3171/2013.1.PEDS 12382 · doi ↗ · pubmed ↗