Impact of Residents’ Mass Resignation in Cardiovascular Surgery: A System Sustainability Perspective
June Yeop Lee, Hyoung Woo Chang, Sang Yoon Kim, Joon Chul Jung, Jae Hang Lee, Sanghon Park, Jun Sung Kim, Kay-Hyun Park

TL;DR
A mass resignation of medical residents in South Korea led to significant disruptions in cardiovascular surgery, including longer waiting times and worse patient outcomes.
Contribution
This study reveals the systemic vulnerabilities in healthcare when resident labor is over-relied upon, using cardiovascular surgery as a case study.
Findings
Surgical volume dropped by 58% during resident absence and did not recover to pre-resignation levels.
Resident absence was an independent risk factor for failure-to-rescue complications and failure-to-rescue outcomes.
Median surgical waiting times increased significantly during the period of resident absence.
Abstract
In February 2024, a nationwide resident resignation occurred in South Korea that persisted for more than one and a half years and caused unprecedented disruptions in teaching hospitals. This study evaluated the clinical and socioeconomic impact of resident absence on cardiovascular surgery at a tertiary teaching hospital. We retrospectively reviewed 681 patients who underwent open-heart or aortic surgery between February 20 and November 30, 2023 (before resident absence) and in 2024 (resident absence). Each year was divided into 3 periods (Q1, Q2, and Q3) for temporal comparison. The primary outcomes were 30-day mortality, failure-to-rescue complications, and failure-to-rescue. Failure-to-rescue was defined as in-hospital mortality after one or more of the following failure-to-rescue complications: acute renal failure, respiratory complications (prolonged ventilation >24 h, pneumonia,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
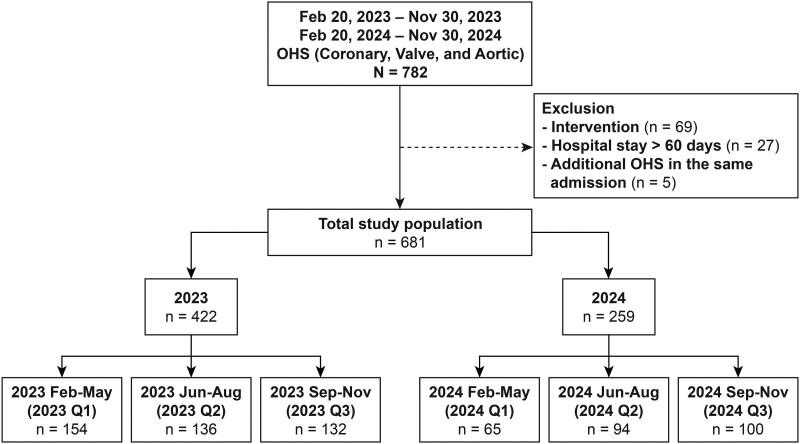 Figure 1
Figure 1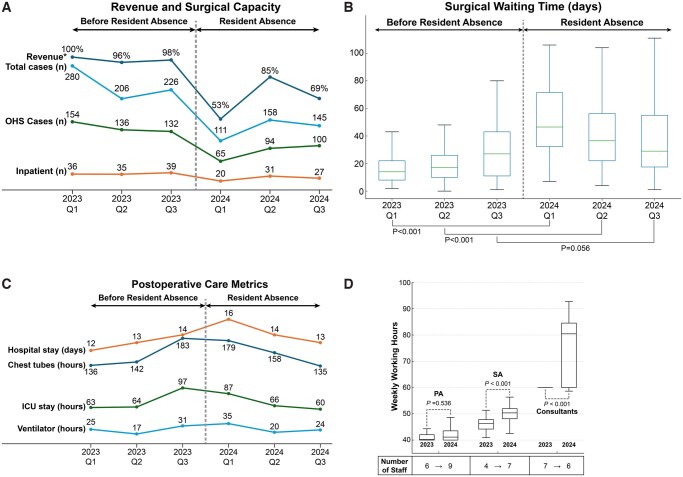 Figure 2
Figure 2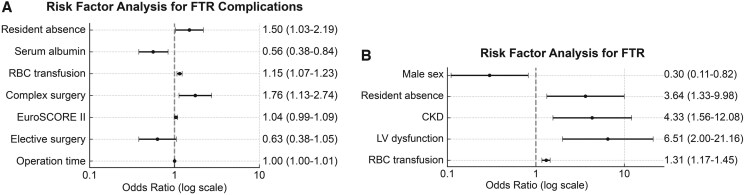 Figure 3
Figure 3| 2023 Q1 ( | 2024 Q1 ( |
| 2023 Q2 ( | 2024 Q2 ( |
| 2023 Q3 ( | 2024 Q3 ( |
| |
|---|---|---|---|---|---|---|---|---|---|
| Age, years | 66 (SD: 13) | 66 (SD: 14) | .876 | 67 (SD: 11) | 67 (SD: 12) | .892 | 66 (SD: 15) | 66 (SD: 11) | .866 |
| Sex, male | 106 (68.8) | 49 (75.4) | .330 | 91 (66.4) | 69 (73.4) | .259 | 98 (74.2) | 74 (74.0) | .967 |
| Body mass index, kg/m2 | 25 (SD: 4) | 24 (SD: 3) | .105 | 25 (SD: 4) | 24 (SD: 3) | .317 | 25 (SD: 4) | 25 (SD: 4) | .331 |
| Hypertension | 114 (74.0) | 50 (76.9) | .734 | 101 (73.7) | 66 (70.2) | .558 | 85 (64.4) | 69 (69.0) | .462 |
| Diabetes mellitus | 48 (31.2) | 22 (33.8) | .698 | 54 (39.4) | 25 (26.6) | .044 | 49 (37.1) | 35 (35.0) | .739 |
| Cerebrovascular accident | 27 (17.5) | 13 (20.0) | .666 | 22 (16.1) | 12 (12.8) | .488 | 21 (15.9) | 16 (16.0) | .985 |
| Chronic kidney disease | 20 (13.0) | 14 (21.5) | .110 | 19 (14.0) | 10 (10.6) | .454 | 19 (14.4) | 11 (11.0) | .445 |
| Medical aid | 6 (3.9) | 1 (1.5) | .677 | 6 (4.4) | 1 (1.1) | .245 | 8 (6.1) | 4 (4.0) | .483 |
| Albumin, g/dl | 3.9 (SD: 0.5) | 3.9 (SD: 0.6) | .474 | 4.0 (SD: 0.5) | 4.0 (SD: 0.5) | .635 | 3.9 (SD: 0.6) | 4.1 (SD: 0.5) | .004 |
| EuroSCORE II | 1.9 [1-5] | 4.0 [2-8] | <.001 | 2.0 [1-4] | 2.2 [1-5] | .058 | 2.2 [1-5] | 2.0 [1-3] | .549 |
| LV dysfunction | 16 (10.7) | 6 (9.5) | .802 | 10 (7.5) | 8 (8.6) | .755 | 9 (7.0) | 9 (9.0) | .569 |
| Coronary, | 68 | 13 | .533 | 47 | 23 | .682 | 31 | 30 | .624 |
| 1-vessel disease | 1 (1.5) | 0 (0) | 1 (2.1) | 0 (0) | 1 (3.2) | 2 (6.7) | |||
| 2-vessel disease | 14 (20.6) | 1 (7.7) | 8 (17.0) | 6 (26.1) | 7 (22.6) | 4 (13.3) | |||
| 3-vessel disease | 53 (77.9) | 12 (92.3) | 38 (80.9) | 17 (73.9) | 23 (74.2) | 24 (80.0) | |||
| Valve, | 34 | 10 | .783 | 45 | 27 | .747 | 45 | 26 | .591 |
| Single valve surgery | 20 (58.8) | 7 (70.0) | 37 (82.2) | 24 (88.9) | 37 (82.2) | 19 (73.1) | |||
| Double valve surgery | 13 (38.2) | 3 (30.0) | 6 (13.3) | 3 (11.1) | 7 (15.6) | 6 (23.1) | |||
| Triple valve surgery | 1 (2.9) | 0 (0) | 2 (4.4) | 0 (0) | 1 (2.2) | 1 (3.8) | |||
| Infective endocarditis | 3 (8.8) | 3 (33.3) | .120 | 3 (6.7) | 1 (3.7) | >.999 | 4 (8.9) | 3 (11.5) | .701 |
| Aorta, | 52 | 42 | 44 | 44 | 56 | 44 | |||
| Aneurysm | 29 (55.8) | 20 (47.6) | .432 | 23 (52.3) | 31 (68.9) | .109 | 30 (53.6) | 27 (62.8) | .358 |
| Acute aortic syndrome | 18 (34.6) | 13 (41.9) | .707 | 15 (34.1) | 6 (13.3) | .021 | 22 (39.3) | 7 (16.3) | .013 |
| Complex surgery | 44 (28.6) | 10 (15.4) | .039 | 40 (29.2) | 22 (23.4) | .329 | 33 (25.0) | 17 (17.0) | .142 |
| Redo OHS | 12 (7.8) | 9 (13.8) | .165 | 9 (6.6) | 12 (12.8) | .112 | 14 (10.6) | 10 (10.0) | .881 |
| Emergency surgery | 23 (14.9) | 18 (27.7) | .027 | 18 (13.1) | 7 (7.4) | .171 | 22 (16.7) | 14 (14.0) | .579 |
| Operation time, min | 260 [220-310] | 260 [225-325] | .974 | 270 [225-315] | 228 [190-275] | <.001 | 265 [230-338] | 235 [185-285] | <.001 |
| 2023 Q1 ( | 2024 Q1 ( |
| 2023 Q2 ( | 2024 Q2 ( |
| 2023 Q3 ( | 2024 Q3 ( |
| |
|---|---|---|---|---|---|---|---|---|---|
| Bleeding control surgery | 18 (11.7) | 5 (7.7) | .474 | 10 (7.4) | 6 (6.4) | .801 | 10 (7.4) | 6 (6.0) | .497 |
| Reoperation | 9 (5.8) | 6 (9.2) | .387 | 11 (8.1) | 5 (5.3) | .447 | 11 (8.3) | 6 (6.0) | .614 |
| Stroke | 7 (4.5) | 1 (1.5) | .441 | 2 (1.5) | 4 (4.3) | .229 | 2 (1.5) | 4 (4.0) | .407 |
| Respiratory complication | 30 (19.5) | 17 (26.2) | .272 | 18 (13.2) | 20 (21.3) | .106 | 27 (20.5) | 14 (14.0) | .202 |
| Acute renal failure | 8 (5.2) | 6 (9.2) | .363 | 9 (6.6) | 3 (3.2) | .368 | 8 (6.1) | 7 (7.0) | .793 |
| Life-threatening arrhythmia | 8 (5.2) | 2 (3.1) | .727 | 5 (3.7) | 6 (6.4) | .363 | 5 (3.8) | 4 (4.0) | >.999 |
| Postoperative MI | 3 (1.9) | 1 (1.5) | >.999 | 1 (0.7) | 1 (1.1) | >.999 | 1 (0.8) | 2 (2.0) | .579 |
| Culture-positive sepsis | 0 (0) | 1 (1.5) | .297 | 2 (1.5) | 3 (3.2) | .401 | 2 (1.5) | 2 (2.0) | >.999 |
| Wound complication | 17 (11.0) | 5 (7.7) | .480 | 9 (6.6) | 9 (9.6) | .459 | 6 (4.5) | 7 (7.0) | .566 |
| Mediastinitis | 3 (1.9) | 0 (0) | .557 | 2 (1.5) | 3 (3.2) | .401 | 1 (0.8) | 3 (3.0) | .318 |
| Readmission | 12 (7.8) | 8 (12.3) | .310 | 8 (5.9) | 4 (4.3) | .766 | 11 (8.3) | 11 (11.0) | .506 |
| 30-day mortality | 6 (3.9) | 3 (4.6) | .727 | 4 (2.9) | 3 (3.2) | >.999 | 3 (2.3) | 5 (5.0) | .295 |
| FTR complication | 54 (35.1) | 27 (41.5) | .444 | 37 (27.2) | 34 (36.2) | .191 | 46 (34.8) | 32 (32.0) | .676 |
| FTR | 6 (11.1) | 6 (22.2) | .201 | 4 (10.8) | 6 (17.6) | .504 | 4 (8.7) | 6 (18.8) | .302 |
| RBC transfusion, units | 4 [1-8] | 6 [3-8] | .044 | 4 [1-7] | 4 [2-7] | .637 | 4 [2-8] | 3 [0-5] | <.001 |
| Ventilator use, h | 8 [5-18] | 10 [6-21] | .433 | 7 [4-15] | 5 [3-11] | .009 | 8 [4-16] | 4 [3-8] | <.001 |
| Intensive care unit stay, h | 44 [25-74] | 44 [25-70] | .909 | 50 [38-74] | 26 [21-50] | <.001 | 67 [28-99] | 27 [23-48] | <.001 |
| Hospital stay, days | 9 [7-14] | 11 [8-19] | .012 | 9 [7-13] | 10 [8-17] | .087 | 9 [7-15] | 9 [7-15] | .759 |
| Surgery waiting time, days | 14 [8-22] | 44 [21-71] | <.001 | 17 [10-27] | 37 [22-55] | <.001 | 27 [11-43] | 29 [15-55] | .056 |
| Chest tube drainage, h | 103 [68-162] | 118 [82-205] | .102 | 113 [71-162] | 101 [70-187] | .557 | 138 [93-208] | 98 [67-162] | <.001 |
| Vasopressors/inotropes, h | 52 [30-95] | 60 [28-110] | .686 | 67 [39-110] | 82 [23-140] | .340 | 80 [47-125] | 61 [26-134] | .118 |
| 2023 ( | 2024 ( |
| |
|---|---|---|---|
| Sex, male | 77 (73.3) | 47 (62.7) | .144 |
| Age | 66 (SD: 15) | 65 (SD: 13) | .498 |
| Admission route | .975 | ||
| Emergency room | 21 (19.8) | 15 (20.0) | |
| Transfer | 85 (80.2) | 60 (80.0) | |
| Treatment option | .299 | ||
| Medical | 37 (34.9) | 25 (33.3) | |
| Intervention | 2 (1.9) | 5 (6.7) | |
| Surgery | 67 (63.2) | 45 (60.0) | |
| Acute type A aortic dissection | 56 (52.8) | 30 (40.0) | .089 |
| Acute type B aortic dissection | 25 (23.6) | 27 (36.0) | .069 |
| Aortic aneurysm | 25 (23.6) | 18 (24.0) | .948 |
| 30-day mortality | 4 (4.2) | 6 (8.6) | .325 |
| Symptom-to-hospital, h | 6 [4-11] | 6 [4-18] | .502 |
| Transfer from tertiary hospital | 7 (8.4) | 12 (20.3) | .040 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSurgical Simulation and Training · Cardiac, Anesthesia and Surgical Outcomes · Hospital Admissions and Outcomes
INTRODUCTION
Residents hold a unique position, serving as both salaried employees and trainees.
In South Korea, 97% of the population is supported by the National Health Insurance Service, and the remaining 3% by medical aid. With low reimbursement rates, individuals pay approximately 3.5% of their income as insurance premiums while receiving high-quality, easily accessible healthcare. The avoidable mortality rate is 142 per 100 000 population (OECD 239; Germany 195; United States 336). The average number of annual outpatient visits per person is 15.7 (OECD 5.9; Germany 9.6; United States 3.4).1 Most patients can see a specialist on the same day.
Behind these favourable statistics, however, lies a structural problem. To offset deficits from low reimbursement, teaching hospitals have reduced the number of board-certified specialists and relied heavily on residents. Residents work more than 80 h weekly for near-minimum wages and constitute more than 40% of the physicians in teaching hospitals.2^,^3 Moreover, even residents in South Korea may face criminal prosecution and actual penalties for adverse clinical outcomes, which has intensified the avoidance of high-risk specialties.4^,^5
Policymakers have linked this avoidance to a physician shortage, citing a density of 2.7 per 1000 population, below the OECD average of 3.7, and in February 2024, they announced a 65% increase in the medical school admission quota (3058-5058) and regulated non-reimbursable services to attract medical students to high-risk specialties.
Medical professionals warned that sudden expansion without sufficient faculty and infrastructure would compromise education quality and endanger public health. Nevertheless, government and university administrators proceeded. In protest, more than 95% of the residents resigned on February 20, 2024, and most medical students declared indefinite leave; both actions continued through August 2025. Without residents, teaching hospitals cannot sustain existing workloads, resulting in clinical and structural changes.
Resident strikes are rare but have increased since COVID-19, becoming a major social issue. Most studies have reported no short-term increase in mortality, but prolonged nationwide absences are exceptional and unstudied in CV surgery, where challenging surgeries and intensive care are frequently performed.6
In this study, the clinical, structural, and socioeconomic impacts of the nationwide mass resignation of residents on CV surgery in a tertiary teaching hospital were evaluated. In addition, the sustainability of a resident-independent system in South Korea was assessed.
PATIENTS AND METHODS
This study involved the collection and analysis of clinical data only and did not include the storage or use of any biological materials. The handling of collected data was conducted in a manner consistent with the requirements outlined in the WMA Declaration of Taipei. The study protocol was reviewed and approved by the Institutional Review Board of Seoul National University Bundang Hospital (SNUBH; B-2412-941-101). Given the retrospective nature of the study and the use of de-identified data, the requirement for informed consent was waived by the ethics committee.
Study design and patient selection
We reviewed patients who underwent open-heart surgery or open aortic surgery (collectively OHS) in the CV surgery department at SNUBH from February 20 to November 30 in both 2023 and 2024. February 20, the date of the nationwide residents’ resignation, was chosen as the starting point. Identical periods were selected to minimize seasonal variations.
Data were extracted from a prospectively collected cardiac surgery database. Each year was divided into 3 intervals, that is February-May (Q1), June-August (Q2), and September-November (Q3), to assess temporal changes.
Coronary artery surgery included coronary artery bypass grafting with or without cardiopulmonary bypass. Valve surgery included replacement or repair of the aortic, mitral, or tricuspid valves. Aortic surgery included replacement of any segment from the root to the abdominal aorta, excluding peripheral arteries. Complex surgery involved 2 or more of these procedures during the same operation.
The exclusion criteria were as follows: (1) hospital stay >60 days, (2) percutaneous interventions, and (3) planned staged surgery at the same admission. These were predetermined through discussion among the coauthors, as such cases often have heterogeneous clinical courses.
Revenue data were obtained from the SNUBH information department and reported only as percentage changes due to institutional privacy policy.
Outcome variables
The primary outcomes were 30-day mortality, failure-to-rescue (FTR) complications and FTR. FTR was defined as in-hospital mortality after ≥1 of the following complications: acute renal failure (excluding preoperative dialysis); respiratory complications (prolonged ventilation >24 h, pneumonia, or tracheostomy); stroke; reoperation (including bleeding control); life-threatening arrhythmia; postoperative myocardial infarction; or culture-positive sepsis. Definitions followed the Society of Thoracic Surgeons Adult Cardiac Surgery Database (STS-ACSD; Supplementary Material 1).
Secondary outcomes were readmission, duration of mechanical ventilation, inotropic/vasopressor use, chest tube drainage, intensive care unit (ICU) and hospital stay, and surgical waiting time
Institutional changes following residents’ resignation
This section summarizes only measures directly related to clinical practice. The timeline and government’s actions are summarized in Supplementary Materials 2 and 3.
In 2023, at SNUBH, there were a total of 9 residents in the Department of Thoracic and Cardiovascular Surgery. Of these, 5 residents were assigned to CV surgery and 4 to general thoracic surgery, rotating every 2 months. They participate in surgical assistance, postoperative care, medical record documentation, emergency department coverage, and academic research. All the residents resigned on February 20, 2024, and the chief resident provided a 1-week handover to consultants to ensure continuity of patient care. On March 1, 2024, the contracts of the clinical fellows expired.
The faculty included 1 coronary specialist, 1 valve specialist, 2 aortic specialists, 2 intensivists, and 1 junior consultant; however, their surgical practice was not limited to their specialties. In August 2024, the valve specialist resigned, and the remaining 4 consultants shared valve surgeries. All surgeries, including emergency sternotomy and bleeding control surgery, were performed by faculty surgeons rather than residents in both 2023 and 2024.
In 2023, 5 physician assistants (PAs) and 4 surgical assistants (SAs) worked in CV surgery. After governmental approval to expand nurses’ roles, 3 PAs (August 2024) and 3 SAs (October 2024) were added.
The on-call system also changed. Before resident absence, 2 residents covered the ward and ICU separately, with a fellow or junior consultant on home call as a backup. After the residents’ resignation, one consultant covered both the ward and ICU. Standardized protocols for nonemergent conditions were provided to nurses, and PAs handled primary calls to reduce consultant workload. Three consultants rotated emergency aortic calls both before and after the residents’ absence.
Statistical analysis
Categorical variables were compared with the chi-square test or Fisher’s exact test, and continuous variables were compared with Student’s t test or the Mann-Whitney U test. Variables with a *P-*value ≤.1 in the univariable analysis were entered into the multivariable logistic regression. The backwards selection method was used, but variables of interest excluded during the process were nonetheless included in the final model. Multicollinearity was checked via the variance inflation factor (VIF), and variables with a VIF > 5 were excluded. Analyses were performed with SPSS 27.0 for Windows (IBM, Armonk, NY, United States).
RESULTS
Preoperative and operative characteristics
A total of 681 patients who underwent OHS between 20 February and 30 November in each of 2023 and 2024 were included and analysed according to the year of surgery: 2023 group (n = 422) and 2024 group (n = 259) (Figure 1). Each group was further subdivided into Q1, Q2, and Q3, and comparisons were drawn between corresponding quarters.
Patient Classification Flowchart of the Study Cohort. Abbreviation: OHS: open-heart surgery.
The preoperative and operative characteristics are summarized in Table 1, with the 2024 group (n = 259) representing a 38.6% reduction in case volume compared with 2023 group (n = 422) (Figure 2A). Most demographics and clinical parameters were comparable, but several differences were noted.
*Changes Before and After the Resident Resignation. (A) Line graphs showing changes in revenue and surgical capacity, (B) line graphs showing changes in postoperative care metrics, (C) box plots showing changes in surgical waiting time, and (D) box plots showing changes in weekly working hours of medical staff. Abbreviations: ICU: intensive care unit; OHS: open-heart surgery; PA: physician assistant; SA: surgical assistant. 2023 Q1 revenue = 100% (reference).
The EuroSCORE II was significantly higher in 2024 Q1 compared with 2023 Q1 (2023/2024 Q1: median 1.9 [IQR 1-5] vs 4.0 [2-8], P < .001). The proportion of acute aortic syndrome was lower in both 2024 Q2 and Q3 compared with the corresponding periods in 2023. In 2023 Q2, acute aortic syndrome occurred in 15 patients (34.1%) compared with 6 patients (13.3%) in 2024 Q2 (P = .021). Similarly, in 2023 Q3, the proportion was 22 patients (39.3%) compared with 7 patients (16.3%) in 2024 Q3 (P = .013). Complex surgery was less frequent in 2024 Q1 than in 2023 Q1 (2023/2024 Q1: 28.6% vs 15.4%, P = .039), whereas emergency surgery was more frequent in 2024 Q1 than in 2023 Q1 (2023/2024 Q1: 14.9% vs 27.7%, P = .027). Operation time was significantly shorter in 2024 Q2 and Q3 compared with the corresponding quarters in 2023 (2023/2024 Q2: 270 [225-315] vs 228 [190-275] min, P < .001; 2023/2024 Q3: 265 [230-338] vs 235 [185-285] min, P < .001).
Surgery-related outcomes
The surgery-related outcomes are summarized in Table 2, Figure 2B and C. Red blood cell (RBC) transfusion was higher in 2024 Q1 than in 2023 Q1 (2023/2024 Q1: 4 [1-8] vs 6 [3-8] units, P = .044), whereas it was lower in 2024 Q3 compared with 2023 Q3 (2023/2024 Q3: 4 [2-8] vs 3 [0-5] units, P < .001). Ventilator duration was significantly shorter in 2024 Q2 and Q3 than in the corresponding quarters of 2023 (2023/2024 Q2: 7 [4-15] vs 5 [3-11] h, P = .009; 2023/2024 Q3: 8 [4-16] vs 4 [3-8] h, P < .001). Similarly, ICU stay was shorter in 2024 Q2 and Q3 (2023/2024 Q2: 50 [38-74] vs 26 [21-50] h, P < .001; 2023/2024 Q3: 67 [28-99] vs 27 [23-48] h, P < .001). Hospital stay was longer in 2024 Q1 than in 2023 Q1 (2023/2024 Q1: 9 [7-14] vs 11 [8-19] days, P = .012) (Figure 2B).
Surgical waiting time was significantly prolonged in both 2024 Q1 and Q2 compared with the corresponding periods in 2023 (2023/2024 Q1: 14 [8-22] vs 44 [21-71] days, P < .001; 2023/2024 Q2: 17 [10-27] vs 37 [22-55] days, P < .001) (Figure 2C). Chest tube duration was shorter in 2024 Q3 than in 2023 Q3 (2023/2024 Q3: 138 [93-208] vs 98 [67-162] h, P < .001).
Cases of aortic emergencies
Among 181 emergency aortic cases, 106 occurred in 2023, and 75 occurred in 2024 representing a 29.2% reduction in case volume in 2024 (Table 3). Most clinical features were similar. However, transfers from other tertiary hospitals were significantly more common in 2024 than in 2023 (20.3% vs 8.4%, P = .040).
Risk factor analyses
Thirty-day mortality
On multivariable logistic regression analyses, independent predictors were valve surgery (OR 15.49, 95% CI 2.08-115.52; P = .008), diabetes mellitus (OR 3.33, 95% CI 1.11-9.98; P = .032), preoperative left ventricular dysfunction (OR 9.02, 95% CI 2.47-32.89; P < .001), and greater RBC transfusion (OR 1.44, 95% CI 1.28-1.62; P < .001). Resident absence was not a significant independent predictor of 30-day mortality (OR 1.62, 95% CI 0.56-4.69; P = .374) (Supplementary Material 4).
FTR complications
On multivariable logistic regression analyses, independent risk factors included resident absence (OR 1.50, 95% CI 1.03-2.19; P = .034), greater RBC transfusion (OR 1.15, 95% CI 1.07-1.23; P < .001), complex surgery (OR 1.76, 95% CI 1.13-2.74; P = .012), and longer operation time (OR 1.004, 95% CI 1.002-1.006; P < .001), whereas a higher preoperative serum albumin level was a protective factor (OR 0.56, 95% CI 0.38-0.84; P = .005) (Figure 3A and Supplementary Material 5).
Forest Plots of Multivariable Logistic Regression Analyses for the Risk of Failure-to-Rescue (FTR) Complications and FTR. (A) Risk factor analysis of FTR complications, and (B) risk factor analysis of FTR. Abbreviations: CKD: chronic kidney disease; FTR: failure-to-rescue; LV: left ventricle; RBC: red blood cell.
Failure-to-rescue
On multivariable logistic regression analyses, independent risk factors included resident absence (OR 3.64, 95% CI 1.33-9.98; P = .012), chronic kidney disease (OR 4.33, 95% CI 1.56-12.08; P = .005), preoperative left ventricular dysfunction (OR 6.51, 95% CI 2.00-21.16; P = .002), and greater RBC transfusion (OR 1.31, 95% CI 1.17-1.45; P < .001). Male sex was a protective factor (OR 0.30, 95% CI 0.11-0.82; P = .018) (Figure 3B and Supplementary Material 6).
Medical staff workload
The workloads of PAs, SAs, and consultants are shown in Figure 2D, and detailed data by quarter are provided in Supplementary Material 7. The weekly working hours of SAs and consultants were significantly longer in 2024 than in 2023 (SA: 46 [44-48] vs 50 [48-53] h, P < .001; consultants: 60 [60-60] vs 80 [60-85] h, P < .001).
DISCUSSION
The main findings of this study are as follows:
The surgical volume decreased sharply early after resident absence, with higher EuroSCORE II and emergency rates. These changes likely reflected the prioritization of emergencies.The operation time, duration of ventilator support, and length of ICU stay decreased over time, whereas the complication rates and length of hospital stay remained unchanged. This finding indicates that improvements in operating room and ICU did not directly translate into better overall clinical outcomes.Thirty-day mortality did not change, and resident absence was not an independent risk factor.Resident absence independently increased FTR complications and FTR risk. This finding suggests that patients who might have survived with resident support were more likely to die.Transfers between tertiary centres increased, suggesting a structural vulnerability in the healthcare delivery system.
Changes in clinical practice
What had previously been conceivable only as a hypothetical scenario—the nationwide disappearance of residents—became reality in South Korea.
The first major change was the postponement of elective surgeries and a shift towards emergencies, with higher EuroSCORE II. This shift likely reflected the prioritization of limited workforce for life-saving care and a shortage of anaesthesiologists.
Operation time decreased, likely because surgeons no longer needed to spend time on education in the operating room. However, this alteration does not reflect changes in surgery type or complexity and should be interpreted with caution. In 2024 Q3, the durations of ventilation, ICU stay decreased, possibly because of faster decision-making by consultants and reduced surgical volume, which facilitated timely ICU-to-ward transfers. However, complication rates and hospital stay duration did not change, likely because other variables may have offset this effect, and patients could be discharged without time pressure, allowing longer recovery in the ward.
Surgical waiting times were prolonged throughout the period of resident absence. As noted in previous studies, the impact of surgical delay is difficult to predict and may pose long-term risks, highlighting the need for long-term follow-up.
Mortality and failure-to-rescue
The year of surgery was used as a surrogate because CV surgery policy remained stable. Although unmeasured factors may exist, they were regarded as part of the natural adaptation to residents’ resignation.
Failure-to-rescue, defined as death after a postoperative complication, was first introduced by Silber et al7 and has since been validated as a quality metric for postoperative care in numerous studies.8–10 FTR complications vary by surgery type, but the inclusion criteria should follow certain principles: (1) severe enough to potentially result in death, (2) not present preoperatively, and (3) potentially preventable or amenable to rescue.11
Consistent with the findings of previous studies, 30-day mortality did not increase, and resident absence was not an independent risk factor.6^,^12^,^13 Although the crude comparison of FTR complications and FTR showed no significant differences when comparing by quarter, but after controlling for confounding variables in the multivariable analysis, the resident absence independently predicted FTR complications and FTR, suggesting possibility of failures in early detection and timely intervention. Providing standardized care protocols and replacing residents with other medical staff may have been insufficient to compensate for resident absence.
Other independent risk factors for FTR were male, chronic kidney disease, preoperative left ventricular dysfunction, and greater RBC transfusion, which were generally consistent with previous reports.14^,^15
Possible explanations may account for our less favourable results compared with previous studies. CV surgery involves high-risk patients who require close monitoring and immediate intervention. According to the Korean Intern Resident Association Survey 2022, CV surgery residents worked an average of 102 h weekly, indicating the system’s high dependency on their labour. Moreover, most previous studies have assessed short-term absences and may not reflect the impact of prolonged absences. Finally, negative outcomes may have been underreported, particularly in single-centre studies.
Emergency healthcare delivery system
The increase in transfers between tertiary centres is undesirable and reveals structural vulnerabilities in the healthcare delivery system, as longer travel may adversely affect outcomes.16 It is concerning that tertiary hospitals, which should serve as the final destination for emergency patients, failed to fulfil this role. The lower proportion of acute type A dissections and unchanged symptom-to-hospital arrival time may suggest the presence of survivor bias in 2024. Further studies with nationwide data are needed for validation.
Financial and workload changes
In 2024 Q1, revenue dropped to 53% of 2023 Q1 levels and has not returned to baseline (Figure 2A). The workloads of SAs and consultants increased, raising concerns about burnout and financial sustainability (Figure 2D), as their hourly wages are substantially higher than those of residents. These increased costs were covered by public funds based on taxation (Supplementary Material 3).
Limitations
First, the single-centre, retrospective design and the relatively small number of FTR events relative to the number of covariates may have limited the statistical power of our analyses. Second, since reliance on residents varies internationally, these findings may not be generalizable. Further studies with nationwide data are needed for validation. Nevertheless, discrepancy between documented working hours and actual working hours is not unique to South Korea and has been reported in resident training systems in other countries as well. For this reason, we believe our observations in the setting of resident overwork may provide meaningful insights for the healthcare system.
CONCLUSION
The nationwide mass resignation of residents revealed the structural vulnerability of South Korea’s healthcare system, which has relied heavily on residents. In their absence, teaching hospitals experienced difficulties in maintaining prior surgical volumes, raising concerns about possible downstream effects on postoperative care quality and the healthcare delivery system. The remaining staff appeared to face heavier workloads, and patients experienced longer waiting times for surgery, which may threaten the sustainability of the healthcare system. These findings suggest that careful reform of this resident-dependent system may be warranted, and teaching hospitals should continue to emphasize their role as educational institutions, ensuring that residents are regarded primarily as trainees rather than as a low-cost workforce.
Supplementary Material
ivag037_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1OECD. OECD Health Statistics 2023. OECD indicators. Accessed June 4, 2024. 10.1787/7a 7afb 35-en · doi ↗
- 2Sohn S , Seo Y, Jeong Y, Lee S, Lee J, Lee KJ. Changes in the working conditions and learning environment of medical residents after the enactment of the Medical Resident Act in Korea in 2015: a national 4-year longitudinal study. J Educ Eval Health Prof. 2021;18:7.33873263 10.3352/jeehp.2021.18.7PMC 8118751 · doi ↗ · pubmed ↗
- 3Park J , Shin CH, Lee JY. Why did all the residents resign? Key takeaways from the junior physicians’ mass walkout in South Korea. J Grad Med Educ. 2024;16:402-406.39148889 10.4300/JGME-D-24-00227.1PMC 11324171 · doi ↗ · pubmed ↗
- 4Chang YS. Moving forward to improve safety and quality of neonatal intensive care in Korea. J Korean Med Sci. 2018;33:e 89.29441743 10.3346/jkms.2018.33.e 89PMC 5811665 · doi ↗ · pubmed ↗
- 5Jung JY , Kim SY, Kim DG, et al Analysis of lawsuit cases in the Department of Surgery in Korea. Ann Surg Treat Res. 2018;94:113-117.29520344 10.4174/astr.2018.94.3.113PMC 5842082 · doi ↗ · pubmed ↗
- 6Cunningham SA , Mitchell K, Narayan KM, Yusuf S. Doctors’ strikes and mortality: a review. Soc Sci Med. 2008;67:1784-1788.18849101 10.1016/j.socscimed.2008.09.044 · doi ↗ · pubmed ↗
- 7Silber JH , Williams SV, Krakauer H, Schwartz JS. Hospital and patient characteristics associated with death after surgery. A study of adverse occurrence and failure to rescue. Med Care. 1992;30:615-629.1614231 10.1097/00005650-199207000-00004 · doi ↗ · pubmed ↗
- 8Reddy HG , Shih T, Englesbe MJ, et al Analyzing "failure to rescue": is this an opportunity for outcome improvement in cardiac surgery? Ann Thorac Surg. 2013;95:1976-1981; discussion 1981.23642682 10.1016/j.athoracsur.2013.03.027PMC 4398337 · doi ↗ · pubmed ↗