Parental postpartum depression directly and indirectly affects exclusive breastfeeding: a cross-sectional study
Yuefeng Tan, Xiaona Na, Lei Yu, Sitong Luo, Ai Zhao

TL;DR
This study shows that parental postpartum depression affects a mother's intention and ability to exclusively breastfeed, highlighting the need for mental health support for both parents.
Contribution
The study identifies both direct and indirect pathways linking parental depression to breastfeeding behavior using the ABC model of behavior theory.
Findings
Maternal depression is directly linked to a less positive intention to exclusively breastfeed.
Paternal depression indirectly affects maternal breastfeeding intention through maternal depression.
There is a significant gap between mothers' intention to breastfeed and actual practice.
Abstract
Exclusive breastfeeding (EBF) is essential for infant health. Parental postpartum depression (PPD) may play a crucial role in shaping maternal intention and behavior to breastfeeding. This study, grounded in the ABC model of behavior theory, aimed to examine the direct and indirect pathways linking maternal and paternal PPD with EBF intention and practice. A total of 273 couples attending postpartum health check-ups were invited to complete structured questionnaires with assistance from trained interviewers. Symptoms of PPD in both mothers and fathers were assessed using the Edinburgh Postnatal Depression Scale (EPDS). Logistic regression analyses were conducted to examine the associations between parental PPD and intention and practice related to EBF. Path analysis was further employed to identify potential pathways linking parental PPD, maternal intention to EBF, and EBF practice.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
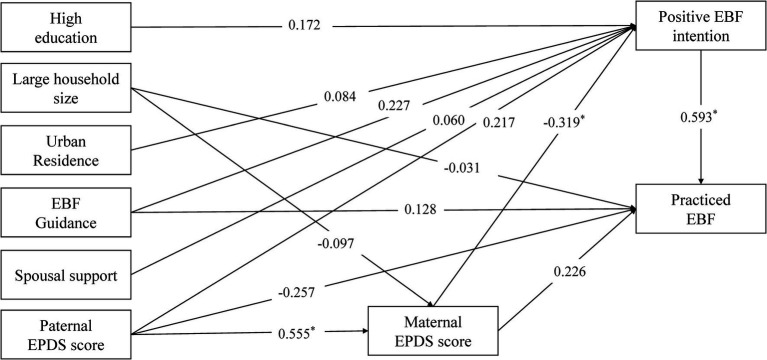 Figure 1
Figure 1| Factors | Intention to EBF |
| Practice of EBF |
| ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Negative | Positive | No | Yes | |||||||
|
| % |
| % |
| % |
| % | |||
| Overall | 18 | 6.6 | 255 | 93.4 | – | 143 | 47.6 | 130 | 52.4 | – |
| Age (y) | ||||||||||
| Under 30 | 12 | 66.7 | 141 | 55.3 | 0.488 | 63 | 48.5 | 90 | 62.9 | 0.022* |
| 30 and above | 6 | 33.3 | 114 | 44.7 | 67 | 51.5 | 53 | 37.1 | ||
| Residence | ||||||||||
| Rural | 12 | 66.7 | 86 | 33.7 | 0.010* | 51 | 39.2 | 47 | 32.9 | 0.351 |
| Urban | 6 | 33.3 | 169 | 66.3 | 79 | 60.8 | 96 | 67.1 | ||
| Education level | ||||||||||
| No bachelor’s degree | 13 | 72.2 | 105 | 41.2 | 0.020* | 63 | 48.5 | 55 | 38.5 | 0.123 |
| Bachelor’s degree | 5 | 27.8 | 150 | 58.8 | 67 | 51.5 | 88 | 61.5 | ||
| Mode of delivery | ||||||||||
| Vaginal delivery | 13 | 72.2 | 182 | 71.4 | 1.000 | 87 | 66.9 | 108 | 75.5 | 0.151 |
| Cesarean section | 5 | 27.8 | 73 | 28.6 | 43 | 33.1 | 35 | 24.5 | ||
| Gravidity | ||||||||||
| Multigravida | 10 | 55.6 | 135 | 52.9 | 1.000 | 72 | 55.4 | 73 | 51.0 | 0.551 |
| Primigravida | 8 | 44.4 | 120 | 47.1 | 58 | 44.6 | 70 | 49.0 | ||
| Parity | ||||||||||
| Multiparous | 7 | 38.9 | 104 | 40.8 | 1.000 | 59 | 45.4 | 52 | 36.4 | 0.164 |
| Primiparous | 11 | 61.1 | 151 | 59.2 | 71 | 54.6 | 91 | 63.6 | ||
| Household size | ||||||||||
| Small household (2) | 3 | 16.7 | 69 | 27.1 | 0.417 | 24 | 18.5 | 48 | 33.6 | 0.007* |
| Large household (>2) | 15 | 83.3 | 186 | 72.9 | 106 | 81.5 | 95 | 66.4 | ||
| Guidance of breastfeeding | ||||||||||
| No | 14 | 77.8 | 114 | 44.7 | 0.013* | 78 | 60.0 | 50 | 35.0 | 0.001* |
| Yes | 4 | 22.2 | 141 | 55.3 | 52 | 40.0 | 93 | 65.0 | ||
| Spousal support | ||||||||||
| Low | 2 | 11.1 | 14 | 5.5 | 0.020* | 9 | 6.9 | 7 | 4.9 | 0.589 |
| Medium | 6 | 33.3 | 32 | 12.5 | 20 | 15.4 | 18 | 12.6 | ||
| High | 10 | 55.6 | 209 | 82.0 | 101 | 77.7 | 118 | 82.5 | ||
| Maternal PPD | ||||||||||
| Yes | 12 | 66.7 | 100 | 39.2 | 0.041* | 52 | 40.0 | 60 | 42.0 | 0.837 |
| No | 6 | 33.3 | 155 | 60.8 | 78 | 60.0 | 83 | 58.0 | ||
| Paternal PPD | ||||||||||
| Yes | 4 | 22.2 | 74 | 29.0 | 0.729 | 36 | 27.7 | 42 | 29.4 | 0.863 |
| No | 14 | 77.8 | 181 | 71.0 | 94 | 72.3 | 101 | 70.6 | ||
| Intention to EBF | ||||||||||
| Negative | – | – | – | – | – | 16 | 12.3 | 2 | 1.4 | 0.001* |
| Positive | – | – | – | – | 114 | 87.7 | 141 | 98.6 | ||
| Practice of EBF | ||||||||||
| No | 16 | 88.9 | 114 | 44.7 | <0.001* | – | – | – | – | – |
| Yes | 2 | 11.1 | 141 | 55.3 | – | – | – | – | ||
| Factors | Maternal PPD |
| Paternal PPD |
| ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| No | Yes | No | Yes | |||||||
|
| % |
| % |
| % |
| % | |||
| Overall | 161 | 59.0 | 112 | 41.0 | – | 195 | 71.5 | 78 | 28.5 | – |
| Age (y) | ||||||||||
| Under 30 | 95 | 59.0 | 58 | 51.8 | 0.290 | 106 | 54.4 | 47 | 60.3 | 0.452 |
| 30 and above | 66 | 41.0 | 54 | 48.2 | 89 | 45.6 | 31 | 39.7 | ||
| Residence | ||||||||||
| Rural | 60 | 37.3 | 38 | 33.9 | 0.662 | 64 | 32.8 | 34 | 43.6 | 0.125 |
| Urban | 101 | 62.7 | 74 | 66.1 | 131 | 67.2 | 44 | 56.4 | ||
| Education level | ||||||||||
| No bachelor’s degree | 73 | 45.3 | 45 | 40.2 | 0.470 | 89 | 45.6 | 29 | 37.2 | 0.254 |
| Bachelor’s degree | 88 | 54.7 | 67 | 59.8 | 106 | 54.4 | 49 | 62.8 | ||
| Mode of delivery | ||||||||||
| Vaginal delivery | 113 | 70.2 | 82 | 73.2 | 0.683 | 134 | 68.7 | 61 | 78.2 | 0.156 |
| Cesarean section | 48 | 29.8 | 30 | 26.8 | 61 | 31.3 | 17 | 21.8 | ||
| Gravidity | ||||||||||
| Multigravida | 81 | 50.3 | 64 | 57.1 | 0.322 | 102 | 52.3 | 43 | 55.1 | 0.774 |
| Primigravida | 80 | 49.7 | 48 | 42.9 | 93 | 47.7 | 35 | 44.9 | ||
| Parity | ||||||||||
| Multiparous | 61 | 37.9 | 50 | 44.6 | 0.321 | 84 | 43.1 | 27 | 34.6 | 0.250 |
| Primiparous | 100 | 62.1 | 62 | 55.4 | 111 | 56.9 | 51 | 65.4 | ||
| Household size | ||||||||||
| Small household (2) | 32 | 19.9 | 40 | 35.7 | 0.005* | 56 | 28.7 | 16 | 20.5 | 0.216 |
| Large household (>2) | 129 | 80.1 | 72 | 64.3 | 139 | 71.3 | 62 | 79.5 | ||
| Guidance of breastfeeding | ||||||||||
| No | 78 | 48.4 | 50 | 44.6 | 0.620 | 94 | 48.2 | 34 | 43.6 | 0.578 |
| Yes | 83 | 51.6 | 62 | 55.4 | 101 | 51.8 | 44 | 56.4 | ||
| Spousal support | ||||||||||
| Low | 10 | 6.2 | 6 | 5.4 | 0.074 | 11 | 5.6 | 5 | 6.4 | 0.967 |
| Medium | 16 | 9.9 | 22 | 19.6 | 27 | 13.8 | 11 | 14.1 | ||
| High | 135 | 83.9 | 84 | 75.0 | 157 | 80.5 | 62 | 79.5 | ||
| Intention to EBF | ||||||||||
| Negative | 6 | 3.7 | 12 | 10.7 | 0.041* | 14 | 7.2 | 4 | 5.1 | 0.729 |
| Positive | 155 | 96.3 | 100 | 89.3 | 181 | 92.8 | 74 | 94.9 | ||
| Practice of EBF | ||||||||||
| No | 78 | 48.4 | 52 | 46.4 | 0.837 | 94 | 48.2 | 36 | 46.2 | 0.863 |
| Yes | 83 | 51.6 | 60 | 53.6 | 101 | 51.8 | 42 | 53.8 | ||
| Maternal PPD | ||||||||||
| Yes | – | – | – | – | – | 61 | 31.3 | 51 | 65.4 | <0.001* |
| No | – | – | – | – | 134 | 68.7 | 27 | 34.6 | ||
| Paternal PPD | ||||||||||
| Yes | 27 | 16.8 | 51 | 45.5 | <0.001* | – | – | – | – | – |
| No | 134 | 83.2 | 61 | 54.5 | – | – | – | – | ||
| Variables | Intention to EBF (Positive) | Practice of EBF (Yes) | ||
|---|---|---|---|---|
| Crude OR (95%CI) | Adjusted OR (95%CI) | Crude OR (95%CI) | Adjusted OR (95%CI) | |
| Maternal PPD status | ||||
| Yes | 0.323* (0.117 ~ 0.887) | 0.201* (0.063 ~ 0.644) | 1.084 (0.669 ~ 1.758) | 0.957 (0.560 ~ 1.635) |
| No | Ref | Ref | Ref | Ref |
| Paternal PPD status | ||||
| Yes | 1.431 (0.456 ~ 4.490) | 1.378 (0.408 ~ 4.648) | 1.086 (0.641 ~ 1.838) | 1.044 (0.590 ~ 1.847) |
| No | Ref | Ref | Ref | Ref |
| Variables | Intention_ | Practice_ | Age_ | Residence_ | Education_ | Household size_ | Guidance_ | Spousal support_ | Maternal PPD_ | Paternal PPD_ |
|---|---|---|---|---|---|---|---|---|---|---|
| Intention_ | 1.000 | 0.220* | 0.060 | 0.170* | 0.160* | −0.060 | 0.160* | 0.167* | −0.140* | 0.040 |
| Practice_ | 0.220* | 1.000 | −0.150* | 0.070 | 0.100 | −0.170* | 0.250* | 0.062 | 0.020 | 0.020 |
| Age_ | 0.060 | −0.150* | 1.000 | 0.220* | 0.010 | −0.090 | 0.090 | 0.125 | 0.070 | −0.050 |
| Residence_ | 0.170* | 0.070 | 0.220* | 1.000 | 0.270* | −0.150* | 0.120 | 0.153* | 0.030 | −0.100 |
| Education level_ | 0.160* | 0.100 | 0.010 | 0.270* | 1.000 | −0.170* | 0.100 | 0.185* | 0.050 | 0.080 |
| Household size_ | −0.060 | −0.170* | −0.090 | −0.150* | −0.170* | 1.000 | −0.080 | 0.097 | −0.180* | 0.080 |
| Guidance_ | 0.160* | 0.250* | 0.090 | 0.120 | 0.100 | −0.080 | 1.000 | 0.135 | 0.040 | 0.040 |
| Spousal support_ | 0.167* | 0.062 | 0.125 | 0.153* | 0.185* | 0.097 | 0.135 | 1.000 | 0.138 | 0.016 |
| Maternal PPD_ | −0.140* | 0.020 | 0.070 | 0.030 | 0.050 | −0.180* | 0.040 | 0.138 | 1.000 | 0.310* |
| Paternal PPD_ | 0.040 | 0.020 | −0.050 | −0.100 | 0.080 | 0.080 | 0.040 | 0.016 | 0.310* | 1.000 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBreastfeeding Practices and Influences · Maternal Mental Health During Pregnancy and Postpartum · Infant Development and Preterm Care
Introduction
Extensive evidence has demonstrated the substantial benefits of breastfeeding for both mothers and infants. Breastfeeding contributes to lower maternal risks of cancers and mental disorders and reduces the likelihood of infectious diseases, obesity, diabetes, and other chronic conditions in children (1–3). Considered as the optimal feeding method, the WHO and UNICEF recommend that babies should be exclusively breastfed (EBF) for the first 6 months after birth, without adding any other food or liquids (4). Although the promotion of breastfeeding has been recognized as a global priority for improving child survival and health, only about 47% of infants under 6 months are exclusively breastfed worldwide, which remains far below the WHO’s target of at least 60% EBF within the first 6 months of life by 2030 (5).
In the exploration of factors associated with breastfeeding, postpartum depression (PPD) appears to be a potentially deleterious contributor (6–8). Approximately 17% of women experience PPD following childbirth (9). PPD usually occurs in women within 4–6 weeks of delivery, and has a long-lasting influence on maternal mental health. It may arise from a combination of hormonal changes, psychological adjustment to motherhood, less social support and unpleasant living conditions (10). Several studies have demonstrated that PPD is correlated with impairment of the mother–infant bond and less breastfeeding self-efficacy, which are considered as plausible reasons for the interruption of breastfeeding (11–13).
In fact, not only maternal but also paternal PPD is a concerning mental disorder. It is reported that the prevalence of paternal depression is approximately 8% (14). Paternal PPD has a negative effect on communication among family members, especially parent–infant interactions, which may cause adverse emotion and behaviors in children (15). However, evidence on the association between paternal depression and breastfeeding is still scarce. In addition, according to the ABC Theory of Emotion proposed by Albert Ellis, a negative behavior is not directly caused by the activating event but the wrong beliefs generated by the individual’s incorrect cognition and evaluation about it (16). The intention to EBF, which was less mentioned in previous studies, may play a critical role in promoting EBF.
Therefore, this study aimed to investigate (i) association between maternal PPD and intention and practice of EBF; (ii) association between paternal PPD and intention and practice of EBF; and (iii) to perform a path analysis exploring the potential pathways linking paternal and maternal PPD, maternal intention to EBF, and breastfeeding practice.
Materials and methods
Participants
This cross-sectional study was conducted in Shenyang and Xuchang in China. In each city, one maternity and childcare hospital was selected by convenience. Infants’ parents who visited hospital for a postpartum health check-up during March to April 2021 were invited to participate in this study by local medical professionals. The eligible participants were women and their partners aged 18–45 years who had given birth to a single full-term infant within the past 3 months. The exclusion criteria included: (i) women not residing in the selected cities; (ii) women or infants with diseases requiring hospitalization or special medical care; (iii) parents with a history of psychological illness; and (iv) those with alcohol or drug addiction. A total of 530 mothers were invited to participate. After excluding cases with missing data, a total of 273 couples were included in the final analysis.
Ethics and consent statement
The research protocol was approved by the Ethics Committee of Tsinghua University (THUSM/PHREC/2020400-005). All procedures were conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants prior to the commencement of the study.
Data collection
With the assistance of trained surveyors, participants completed a structured questionnaire comprising four sections: (i) socio-demographic characteristics; (ii) maternity-related information and postpartum lifestyle; (iii) breastfeeding intention and practice; and (iv) mental health assessment. For socio-demographic characteristics, information such as age, residence, education and the household size were collected. Maternity information included pregnancy and delivery history, and the current delivery information. The definition of exclusive breastfeeding used in this study was consistent with the WHO criteria, as stated in the Introduction, and this definition was clearly stated in the questionnaire and explained to participants by trained field researchers at the study site. Regarding breastfeeding intention to EBF were investigated by the question “Would you like to exclusive breastfeeding?” and participants could respond Yes or No. Actual feeding practice were investigated by the question “How do you feed your baby now?” and participants could choose the appropriate option from exclusive breastfeeding (breastfeeding only), mixed feeding, and other feeding methods. Participants who chose “breastfeeding only” were classified as currently practicing exclusive breastfeeding. Questions such as “Have you ever received professional guidance of breastfeeding?” were also asked. For the measurement of depression, the Edinburgh Postnatal Depression Scale (EPDS) was applied for parents of infants. The EPDS is a 10-item 4-point Likert scale used as a PPD screen, with a higher total score indicating higher risk of PPD. In this study, the Cronbach alpha was 0.81 (wife) and 0.82 (husband) respectively. A cut-off score of 10 is recommended as a Chinese PPD diagnosis by researchers for both male and female population (17–19). Spousal support was measured using a single self-reported item that asked mothers: “How much support and care did you receive from your husband during the breastfeeding period?” Participants selected one of four response options: none, very little, moderate, or full support. We categorized spousal support into three levels: low (none or very little), medium (moderate), and high (full support). All items including those of a sensitive nature, were completed independently by participants in a private setting, with husbands and wives answering the survey separately to ensure comfort and confidentiality.
Statistical analysis
The RStudio (version 2023.09.1, Build 494; RStudio, PBC, Boston, MA, United States). and Mplus Version 7.4 (Muthén & Muthén Inc., Los Angeles, CA, United States) software were used for data analysis. The chi-square test and Fisher’s exact test were used to compare the distribution of EBF intention and practice among women with different characteristics, with the statistical significance level set at 0.05. Variables with significant results in the univariable analysis were considered as potential confounders and adjusted in the logistic regression analysis to examine the association between depression and EBF intention and practice. A path analysis model was established to explore the potential pathways linking parental PPD, maternal intention to EBF, and breastfeeding practice, using the weighted least squares mean and variance adjusted (WLSMV) estimator. Models with different pathways were established to test possible direct and indirect effects. Standardized path coefficients (β) were reported for all effects. The best-fitting model was selected based on comparative fit indices.
Results
Basic information of participants
The postpartum duration of participating mothers ranged from 0 to 72 days, with a mean of 15.9 ± 16.8 days. All newborns had an Apgar score of 10. None of the mothers smoked or consumed alcohol during pregnancy. Table 1 presents the socio-demographic characteristics and maternity history of the participating mothers, categorized by their intention and practice to EBF. Approximately 93.4% of mothers expressed a preference for EBF, while only 52.4% practiced it. Compared with mothers who had a negative intention to EBF, mothers with a positive intention to EBF had a higher proportion of urban residence, higher education levels, receipt of professional breastfeeding guidance, and stronger spousal support, as well as a lower prevalence of PPD and a higher prevalence of EBF practice. Among mothers who practiced EBF, a higher proportion lived in smaller households and had received feeding guidance from healthcare professionals compared with those who did not practice EBF. Table 2 displays the socio-demographic characteristics and maternity history of the participating mothers, categorized by levels of maternal and paternal PPD status. Using the EPDS, 41.0% of mothers and 28.5% of fathers were identified as having probable PPD. Mothers with PPD had a higher proportion living in smaller households and a higher prevalence of paternal PPD compared with mothers without PPD.
Associations between parental PPD and maternal intention and practice to EBF
Table 3 presents the associations of maternal and paternal PPD with intention and practice of EBF. Mothers experiencing PPD were significantly less likely to hold a positive intention to EBF compared with mothers without PPD (adjusted OR = 0.20, 95% CI: 0.06–0.64). In contrast, paternal PPD was not significantly associated with maternal intention to EBF. Furthermore, neither maternal nor paternal PPD demonstrated a significant association with actual EBF behavior.
Pathway analysis
Table 4 summarizes the correlations of the variables that were previously found to be significant predictors of EBF intentions and practice. In line with prior results, maternal depression was still linked to intention to EBF, but showed no significant relationship with actual practice. Paternal depression, on the other hand, showed no significant association with either EBF intention or practice. However, a significant positive correlation was observed between maternal intention to EBF and EBF practice. In addition, maternal PPD was significantly positively correlated with paternal PPD. Therefore, we further conducted a path analysis, as a form of structural equation modeling (SEM), to investigate whether parental depression indirectly influences EBF practice through its effect on maternal intention.
The proposed model, as shown in Figure 1, demonstrated an excellent fit to the data: root mean square error of approximation (RMSEA) = 0.013, comparative fit index (CFI) = 0.997, Tucker–Lewis index (TLI) = 0.993, and weighted root mean square residual (WRMR) = 0.567. Maternal PPD was significantly negatively associated with maternal intention to EBF (βtotal = −0.319, p = 0.001). Significant total effects were also observed between paternal PPD and maternal PPD (βtotal = 0.555, p < 0.001) and between maternal EBF intention and EBF practice (βtotal = 0.593, p = 0.001). In terms of indirect effects, paternal PPD significantly influenced maternal intention to EBF via maternal PPD (βindirect = −0.177, p = 0.001), and maternal PPD had a significant indirect effect on EBF practice through maternal intention (βindirect = −0.189, p = 0.038).
The pathway analysis model. p < 0.05 (). Model fit index: RMSEA = 0.013, CFI = 0.997, TFI = 0.993, WRMR = 0.567.*
Discussion
Our findings indicated a relatively higher prevalence of both willingness and practice of EBF. Notably, 93.4% of mothers expressed a positive intention to EBF, whereas only 52.4% practiced it, revealing a substantial gap between intention and behavior. This discrepancy may be explained by both family and professional factors. A higher proportion of mothers living in smaller households or those receiving professional breastfeeding guidance maintained EBF. Although larger households might provide emotional support and potentially reduce maternal depressive symptoms, excessive involvement from extended family members could interfere with consistent EBF practice. Meanwhile, guidance from healthcare professionals—such as home visiting and structured breastfeeding counseling—may help reinforce maternal confidence and promote adherence to EBF, which might partly explain why maternal PPD was not directly associated with breastfeeding practice in our sample (20, 21). These WHO-recommended approaches not only provide mothers with accessible channels for addressing breastfeeding difficulties but also support communities and healthcare systems in strengthening breastfeeding promotion and support.
While maternal PPD was not directly associated with EBF practice, our study identified a significant association between maternal PPD and negative intention to EBF. This finding is consistent with several previous studies (6, 7, 22, 23). Depressed mothers may experience sadness, hopelessness, and reduced confidence in infant care, which can lead to avoidance or reluctance to breastfeeding (11, 12, 24–26). In fact, a range of evidence-based interventions—such as home-visiting programs—has been shown to alleviate maternal emotional symptoms and improve the quality of feeding interaction, thereby promoting breastfeeding practice (21, 27). Moreover, recent studies have also indicated that breastfeeding may help alleviate postpartum depressive symptoms (28–30). Furthermore, the pathway analysis revealed a significant indirect effect, suggesting that maternal depression may influence breastfeeding behavior through its negative impact on mothers’ intention to EBF. According to the ABC behavioral theory, affective states (A) influence beliefs and cognitions (B), which in turn shape behavioral outcomes (C) (16). This framework has been widely applied to explain how emotional distress shapes health-related decision making and caregiving behaviors. In the context of breastfeeding, negative affective states such as sadness, hopelessness, and reduced self-efficacy may contribute to maladaptive cognitions about breastfeeding, thereby lowering motivation and consistency in maintaining EBF. Guided by this model, our findings suggest that maternal PPD (A) may undermine mothers’ intention to EBF (B), which may in turn affect their actual feeding practices (C). This finding emphasizing that improving mothers’ psychological well-being could help bridge the gap between breastfeeding intention and behavior.
Beyond maternal mental health, paternal psychological well-being also plays a crucial role in the family’s postpartum adjustment. New fathers may struggle to adapt to the transition to fatherhood and become vulnerable to depression due to factors such as negative life events, perceived stress, financial strain, and, notably, the presence of depressive symptoms in their partners (14, 31–34). Consistent with previous studies, our findings revealed a significant association between paternal and maternal PPD, underscoring the interdependence of parental mental health within families (32, 35–37). Building on this interdependence, paternal depression further indirectly affects maternal intention toward EBF by increasing maternal depressive symptoms. When fathers experience depression, their capacity to provide emotional support, childcare participation, and partner reassurance tends to decline. This reduction in paternal involvement may exacerbate maternal stress, decrease maternal confidence in breastfeeding, and, in severe cases, even impair lactation due to the mother’s heightened depressive symptoms (38–40). Moreover, fathers play a significant and independent role in shaping infants’ regulatory processes, including feeding (41). Evidence suggests that paternal depressive symptoms may interact with and exacerbate maternal emotional difficulties, resulting in greater mother–infant interaction conflict and heightened infant negative affectivity (42). These disruptions have been linked to an increased likelihood of non-breastfeeding feeding patterns, as emotionally strained triadic dynamics may reduce the feasibility of maintaining direct breastfeeding (43, 44). Such triadic dysregulation—spanning fathers, mothers, and infants—may ultimately create a less supportive emotional climate for breastfeeding, thereby undermining the establishment and maintenance of EBF. These findings highlight that PPD is not solely a maternal concern but a couple-level issue that can influence child-feeding outcomes. Routine PPD screening for both mothers and fathers should therefore be incorporated into standard postpartum follow-up and maternal–child health services. In addition, fathers may benefit from structured parenting support and psychological guidance to strengthen their ability to support breastfeeding. Actively involving fathers in postpartum mental health interventions and breastfeeding promotion programs may further contribute to successful exclusive breastfeeding.
A major strength of this study lies in identifying maternal intention as a key pathway linking parental depression to EBF practice. By emphasizing the pivotal role of intention in bridging intention and behavior, and by incorporating the mental health of both parents, this study offers a more comprehensive understanding of the psychological determinants of EBF. However, several limitations should be acknowledged. First, the cross-sectional design precludes causal inferences between PPD and EBF. Second, PPD was assessed using the EPDS rather than clinical diagnostic criteria, which may have led to an overestimation of its prevalence. Third, the analytic sample consisted of mothers with relatively higher education levels and better breastfeeding practices, which may introduce selection bias and limit the generalizability of our results; specifically, 56.8% of participants had attained a bachelor’s degree or higher, and 52.4% practiced exclusive breastfeeding. Future studies involving more diverse participants and improved data completeness are warranted. Finally, breastfeeding behavior is influenced by multiple unmeasured factors, such as parental knowledge of EBF, human resource and social welfare policies, and environmental or workplace support.
Conclusion
This study revealed a substantial gap between mothers’ intention and actual practice of EBF. Maternal PPD was associated with intention to EBF but not with its practice, while paternal PPD showed an indirect association with EBF intention. These findings highlight the importance of assessing and addressing both maternal and paternal PPD to promote EBF. Future research and interventions should take a holistic approach, integrating individual, environmental, and policy factors to foster a breastfeeding-friendly society.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Victora CG Bahl R Barros AJ Franca GV Horton S Krasevec J . Breastfeeding in the 21st century: epidemiology, mechanisms, and lifelong effect. Lancet. (2016) 387:475–90. doi: 10.1016/S 0140-6736(15)01024-7, 26869575 · doi ↗ · pubmed ↗
- 2Lubis PN Saputra M Rabbani MW. A systematic review of the benefits of breastfeeding against postpartum depression in low-middle-income countries. J Ment Health. (2025) 34:305–17. doi: 10.1080/09638237.2024.2361232, 38869015 · doi ↗ · pubmed ↗
- 3Masi AC Stewart CJ. Role of breastfeeding in disease prevention. Microb Biotechnol. (2024) 17:e 14520. doi: 10.1111/1751-7915.14520, 38946112 PMC 11214977 · doi ↗ · pubmed ↗
- 4UNICEF. Breastfeeding: A mother’s gift, for every child. New York: (2018).
- 5UNICEF. Global breastfeeding scorecard, 2025. New York: (2025).
- 6Silva CS Lima MC Sequeira-de-Andrade LAS Oliveira JS Monteiro JS Lima NS . Association between postpartum depression and the practice of exclusive breastfeeding in the first three months of life. J Pediatr. (2017) 93:356–64. doi: 10.1016/j.jped.2016.08.00528034730 · doi ↗ · pubmed ↗
- 7Woldeyohannes D Tekalegn Y Sahiledengle B Ermias D Ejajo T Mwanri L. Effect of postpartum depression on exclusive breast-feeding practices in sub-Saharan Africa countries: a systematic review and meta-analysis. BMC Pregnancy Childbirth. (2021) 21:113. doi: 10.1186/s 12884-020-03535-1, 33557766 PMC 7869485 · doi ↗ · pubmed ↗
- 8Henshaw EJ. Breastfeeding and postpartum depression: a review of relationships and potential mechanisms. Curr Psychiatry Rep. (2023) 25:803–8. doi: 10.1007/s 11920-023-01471-3, 37906349 · doi ↗ · pubmed ↗