Mycobacterial Infections in Patients With Hairy Cell Leukemia: A Systematic Review of Published Cases
Praveen Kumar Tirlangi, Venkata Swathi Kiran Pothumarthy, Adil Rashid Khan, Santosh Kumar Chellapuram, Martin Peter Grobusch, Nitin Gupta

TL;DR
This study reviews mycobacterial infections in patients with hairy cell leukemia, finding that these infections are often severe and widespread, with high mortality rates.
Contribution
The paper provides the first systematic review of mycobacterial infections in hairy cell leukemia, highlighting clinical patterns and outcomes.
Findings
Mycobacterial infections in HCL are frequently disseminated and associated with substantial mortality.
Nontuberculous mycobacteria, particularly M. kansasii and M. avium complex, are the most common causes of infection.
Pulmonary involvement is associated with significantly higher mortality rates in these patients.
Abstract
Hairy cell leukemia (HCL) is a rare B-cell lymphoproliferative disorder characterized by monocytopenia and profound defects in cellular immunity, predisposing patients to severe mycobacterial infections. Although numerous case reports exist, the clinical features and outcomes of these infections have not been systematically synthesized. We conducted a systematic review following PRISMA guidelines, searching PubMed, Embase, and Web of Science from inception to 31 January 2025, without language restrictions. Studies were eligible if they contained individual patient-level data on microbiologically confirmed mycobacterial infection in HCL. Data on demographics, clinical presentation, organ involvement, pathogen distribution, treatment timing, and outcomes were extracted and analyzed descriptively. Thirty-six articles describing 48 patients met the inclusion criteria. The mean age was…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
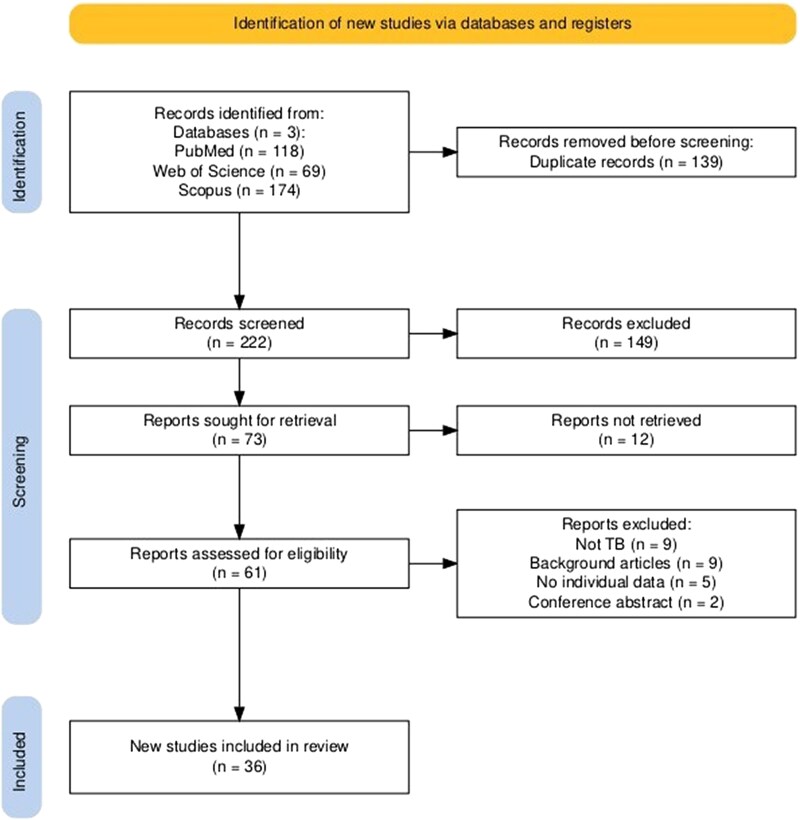 Figure 1
Figure 1| An | Author | Year | Country | Age | Sex | Mycobacteria spp. Diagnosis In Relation To HCL | Dissemination | Etiology | Mortality |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Cellini [ | 2022 | Italy | 59 | Male | Before treatment | Yes | Mtb | No |
| 2 | Castor [ | 1994 | Sweden | 57 | Female | Before treatment | Yes |
| Yes |
| 3 | Broady [ | 1999 | Australia | 57 | Male | Before treatment | Yes | MAC | No |
| 4 | Haefliger [ | 2023 | Switzerland | 74 | Male | Before treatment | No | MAC | Yes |
| 5 | Dugdale [ | 1989 | USA | 58 | Male | Before treatment | Yes | MAC | No |
| 6 | Bain [ | 1992 | UK | 67 | Male | Before treatment | No | Mtb | No |
| 7 | De Kruijf [ | 1997 | Netherlands | 72 | Female | Before treatment | Yes |
| Yes |
| 8 | Hulin [ | 1990 | France | 77 | Male | Before treatment | No | Mtb | No |
| 9 | Trizna [ | 2001 | USA | 60 | Female | After treatment | No | Mk | No |
| 10 | Fleisher | 2006 | Brazil | 44 | Female | Before treatment | Yes |
| No |
| 11 | Geller [ | 2015 | USA | 67 | Male | After treatment | Yes | Mtb | No |
| 12 | Thaker [ | 2001 | UK | 51 | Male | After treatment | Yes | MAC | No |
| 44 | Female | Before treatment | No | Mtb | No | ||||
| 13 | Green [ | 2008 | UK | 70 | Male | After treatment | Yes | Mk | Yes |
| 14 | Valizadeh [ | 2012 | Iran | 46 | Male | After treatment | Yes | Mtb | No |
| 15 | Papadopoulos [ | 2010 | Greece | 69 | Male | After treatment | Yes | AFB | No |
| 16 | Gogia [ | 2013 | India | 52 | Male | After treatment | No | Mtb | No |
| 17 | Weinstein [ | 1978 | USA | 28 | Male | Before treatment | Yes | Mk | Yes |
| 57 | Male | Before treatment | Yes | MAC | No | ||||
| 18 | Manes [ | 1976 | USA | 75 | Male | Before treatment | Yes | Mk | Yes |
| 19 | Raanani [ | 1996 | Israel | 62 | Female | After treatment | No | Mk | No |
| 20 | Dave [ | 1993 | UK | 55 | Male | Before treatment | Yes |
| No |
| 21 | Bennett [ | 1986 | USA | 65 | Male | Before treatment | Yes | Mtb | Yes |
| 30 | Male | After treatment | No | Mk | Yes | ||||
| 60 | Male | Before treatment | No | Mk | No | ||||
| 28 | Male | Before treatment | Yes | Mk | Yes | ||||
| 46 | Female | Before treatment | Yes | Mk | No | ||||
| 33 | Male | After treatment | Yes |
| Yes | ||||
| 57 | Male | Before treatment | Yes | Mk | No | ||||
| 49 | Male | After treatment | No | MAC | No | ||||
| 42 | Male | Before treatment | No | MAC | No | ||||
| 22 | Rice [ | 1982 | USA | 54 | Male | After treatment | Yes | Mk | No |
| 50 | Male | Before treatment | Yes | Mk | Yes | ||||
| 23 | Weinstein [ | 1981 | USA | 59 | Male | After treatment | Yes | Mk | Yes |
| 50 | Female | After treatment | Yes | Mk | No | ||||
| 24 | Mead [ | 1983 | UK | 48 | Female | Before treatment | Yes | Mk | Yes |
| 25 | Maziarz [ | 1988 | USA | 47 | Male | Before treatment | Yes | MAC | No |
| 26 | Hendrick [ | 1979 | USA | 55 | Male | Before treatment | Yes |
| Yes |
| 27 | Maurice [ | 1988 | Australia | 66 | Male | After treatment | Yes | MAC | No |
| 28 | Mummler [ | 2021 | Germany | 62 | Male | Before treatment | Yes | Mk | No |
| 29 | Fonseca [ | 2016 | Portugal | 67 | Male | After treatment | Yes | Mtb | No |
| 30 | Ramasamy [ | 2014 | India | 50 | Male | After treatment | No | AFB | Yes |
| 31 | Girardi [ | 2012 | Italy | 57 | Male | After treatment | No | Mtb | Yes |
| 32 | Filho [ | 2011 | Brazil | 35 | Male | Before treatment | Yes | AFB | No |
| 33 | Kramers [ | 1992 | Netherlands | 40 | Male | Before treatment | Yes | Mk | No |
| 34 | Nielsen [ | 1981 | Denmark | 39 | Male | Before treatment | No | MAC | Yes |
| 35 | Arslan [ | 2013 | Turkey | 56 | Male | Before treatment | Yes | Mtb | Yes |
| 36 | Stanton [ | 2024 | USA | 31 | Male | Before treatment | Yes | Mk | Yes |
| Feature | MTBC (n = 12) | MAC (n = 10) |
|
|
|---|---|---|---|---|
| Male gender | 11/12 (92%) | 8/10 (80%) | 16/18 (89%) | .692 |
| Fever | 10/12 (83%) | 10/10 (100%) | 13/18 (72%) | .179 |
| Mycobacterial infection diagnosed before HCL treatment | 7/12 (58%) | 7/10 (70%) | 11/18 (61%) | .842 |
| Dissemination | 7/12 (58%) | 6/9 (67%) | 14/18 (78%) | .518 |
| Lung involvement | 6/12 (50%) | 4/10 (40%) | 11/18 (61%) | .551 |
| CNS involvement | 4/12 (33%) | 0/10 (0%) | 0/18 (0%) | . |
| Blood culture positivity | 4/10 (40%) | 3/5 (60%) | 3/10 (30%) | .535 |
| Granulomas | 6/12 (50%) | 7/10 (70%) | 13/18 (72%) | .425 |
| Death | 4/12 (33%) | 2/10 (20%) | 9/18 (50%) | .273 |
| Variable | Death (n = 19) | No Death (n = 29) |
|
|---|---|---|---|
| Male gender | 16/19 (84.2%) | 23/29 (79.3%) | .671 |
| Fever | 18/19 (94.7%) | 25/29 (86.2%) | .344 |
| Mycobacterial infection diagnosis before HCL treatment | 13/19 (68.4%) | 17/29 (58.6%) | .493 |
| Monocytopenia | 11/11 (100%) | 11/12 (91.7%) | .328 |
| Lymphopenia | 5/8 (62.5%) | 10/14 (71.4%) | .665 |
| Dissemination | 14/19 (73.7%) | 20/28 (71.4%) | .865 |
| Lung involvement | 15/19 (78.9%) | 12/29 (41.4%) | .010 |
| Blood culture positive for Mycobacteria spp. | 5/14 (35.7%) | 7/19 (36.8%) | .947 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChronic Lymphocytic Leukemia Research · Immunodeficiency and Autoimmune Disorders · Cutaneous lymphoproliferative disorders research
Hairy cell leukemia (HCL) is a rare indolent B-cell neoplasm characterized by pancytopenia, splenomegaly, bone marrow fibrosis, and lymphocytes with distinctive cytoplasmic “hairy” projections [1–3]. Men and individuals of white ethnicity have a higher incidence, most common in middle-aged-to-older adults [1–3]. The neoplastic lymphocytes display aberrant expression of surface proteins that influence their tissue localization and interactions with the microenvironment. CD11c, an adhesion molecule typically found on monocytes and macrophages, mediates binding to complement-coated microbes [4–6]. In HCL, although the leukemic B cells express CD11c, they lack the antimicrobial effector functions of professional phagocytes, allowing intracellular pathogens such as Mycobacterium spp. to persist [7]. CD103 and CXCR4 further determine tissue homing and retention. CD103 binds E-cadherin, anchoring cells within the bone marrow and splenic red pulp, whereas CXCR4 guides migration toward these same niches in response to CXCL12. Once localized, adhesion is reinforced through VCAM-1 interactions, which are upregulated by TNF-α during the inflammatory process. These mechanisms promote the accumulation of leukemic cells in the marrow, liver, and spleen, while the absence of CXCR5 and CCR7 prevents lymph node homing [8, 9]. This unique trafficking pattern, coupled with impaired antimicrobial function, enables HCL cells to serve as permissive reservoirs for intracellular pathogens such as Mycobacterium spp. In addition, HCL creates a profoundly immunosuppressed milieu through monocytopenia, lymphopenia, NK-cell dysfunction, marrow infiltration, hypersplenism, and elevated TNF-α, resulting in pancytopenia and markedly reduced antimicrobial defenses [7, 10–12]. Severe fungal (Cryptococcus spp., Histoplasma spp.) and bacterial (Pseudomonas spp., Escherichia coli) infections occur in up to 40% of patients [11]. Mycobacterial infections are a particular concern, especially in endemic regions, where they may manifest as pulmonary, extrapulmonary, or disseminated disease. Notably, infection can occasionally precede the diagnosis of HCL, underscoring the interplay between disease biology and infection risk [12–14]. To better define this association, we conducted a systematic review of individual patient data to characterize the spectrum, timing, and outcomes of mycobacterial infections in HCL, and to explore their relationship with disease biology and therapy.
METHODS
Study Design and Objective
This systematic review was conducted after registering in the PROSPERO database (CRD420250651278) in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (PRISMA checklist attached as supplementary file) [15]. The primary objective was to examine the relationship between HCL and mycobacterial infections, with a focus on clinical presentation, organ involvement, diagnostic methods, treatment strategies, and outcomes. Only reports with individual patient-level data were included to allow for detailed and granular analysis.
Search Strategy
A comprehensive search was conducted across PubMed, Embase, and Web of Science, spanning the databases’ inception to 31 January 2025. The following search string was used: (“hairy cell”) AND (leukaem* OR leukem*) AND (infect* OR TB OR tubercul* OR mycobact*). The reference lists of relevant articles were also manually screened to ensure completeness. No language restrictions were applied.
Eligibility Criteria
Studies were eligible if they were published case reports or case series describing patients with a confirmed diagnosis of HCL and providing individual-level data on concomitant or subsequent mycobacterial infection. Reports were required to include details on presentation, diagnosis, treatment, or outcomes. Review articles, editorials, conference abstracts, and studies without individual patient details were excluded, as were studies lacking microbiological confirmation of mycobacterial infection.
Study Selection and Data Extraction
Two reviewers (P. K. T. and V. S. K. P.) independently screened titles, abstracts, and full texts. Any disagreements were resolved through discussion or by consultation with a third reviewer (N. G.). A standardized data extraction form was developed a priori and used across all studies. Extracted data (entered by 1 reviewer and verified by another) included demographic details, hematological parameters at the time of diagnosis of mycobacterial infection, timing of mycobacterial infection in relation to HCL diagnosis and treatment, type of mycobacteria and diagnostic methods, clinical features and organ involvement, HCL-directed therapies, treatment of mycobacterial infection, and outcomes including remission, relapse, and mortality.
Definitions
Microbiological confirmation of mycobacterial infection was defined as culture or molecular test positivity from any clinical specimen. Organ involvement was attributed when microbiological confirmation was obtained from tissue or aspirate of the affected site. For organs where primary HCL involvement is uncommon, such as the lungs, lymph nodes, or central nervous system (CNS), involvement was inferred if compatible clinical or radiological findings were present alongside microbiological confirmation from another site. Disseminated mycobacterial infection was defined a priori as involvement of 2 or more noncontiguous organ systems (eg, lung, liver, spleen, lymph nodes, bone marrow, skin, and central nervous system), and/or the isolation of Mycobacterium spp. from a sterile site, including blood, bone marrow, liver, or spleen. This definition aligns with established criteria used in immunocompromised hosts and was applied uniformly to all cases. The temporal relationship between mycobacterial infections and HCL treatment was classified as either occurring before or after initiation of HCL-directed therapy. Monocytopenia was defined as an absolute monocyte count <200 cells/µL (0.2 × 10⁹/L), and lymphopenia as an absolute lymphocyte count <1000 cells/µL (1.0 × 10⁹/L) in adults. In instances where individual reports did not specify absolute counts but explicitly described the patient as having monocytopenia or lymphopenia, such cases were also recorded as fulfilling the respective definition.
Risk of Bias Assessment
All included case reports were critically appraised using the Joanna Briggs Institute (JBI) Critical Appraisal Checklist for Case Reports [16]. Each report was evaluated across key domains, demography, patient history, clinical presentation, diagnostic work-up, treatment, and follow-up, with items judged as adequately/comprehensively reported, inadequately reported, or absent. Patient history was considered adequate only if it included both relevant clinical details and lymphocyte or monocyte counts at the time of mycobacterial diagnosis. Adverse events, although part of the original JBI tool, were considered irrelevant to the objectives of this review and were not evaluated. Two reviewers (P. K. P. and V. S. K. P.) independently conducted the appraisal, and disagreements were resolved through discussion.
Data Analysis
Descriptive statistics were used to summarize patient characteristics, clinical features, organ involvement, treatment modalities, and outcomes. Categorical variables were expressed as absolute numbers and percentages, while continuous variables were reported as means with standard deviations. For comparative analysis, patients were stratified according to the type of mycobacterial infection: Mycobacterium tuberculosis complex (MTBC), Mycobacterium avium complex (MAC), and M. kansasii. Several stratified analyses were conducted to explore patterns of dissemination and organ involvement. Differences in categorical variables between groups were assessed using the χ^2^ test or Fisher's exact test, as appropriate. A P value of <.05 was considered statistically significant.
RESULTS
Study Selection
The initial database search yielded 361 records (PubMed: 118, Web of Science: 69, Scopus: 174). After removing 139 duplicates, 222 records remained for screening. Title and abstract screening excluded 149 records (67%), leaving 73 articles for full-text review. Of these, 37 were excluded (full text unavailable, n = 12; 32.4%, no microbiologically proven mycobacterial infection, n = 9; 24.3%, background articles, n = 9; 24.3%, no individual patient data, n = 5; 13.5%, conference abstracts, n = 2; 5.4%). Ultimately, 36 articles reporting 48 individual cases were included [13, 17–50] (Figure 1).
PRISMA flow diagram depicting the selection process for studies included in the systematic review.
Critical Appraisal of Included Studies
Of the 48 individual cases appraised, demographic details, treatment, and follow-up were consistently reported (100%) [13, 17–50] (Supplementary Table 1). Clinical presentation was adequately described in 47 reports (97.9%), and diagnostic methods were appropriately detailed in 44 (91.7%). Patient history was less comprehensive, with only 17 reports (35.4%) providing sufficient detail. Adverse events were not evaluated for this review. Overall, reporting quality was high, with the main limitation being incomplete patient histories.
Study and Patient Characteristics
The included studies were published between 1976 and 2024 [13, 17–50]. Over half (19/36, 53%) were published before 2000 [13, 17–19, 22–25, 33–42, 48, 49]. Geographically, most originated from the United States (11/36, 30.5%) and the United Kingdom (5/36, 14%) [13, 17, 22, 23, 26–29, 33–38, 40, 41]. Among the 48 cases, 81% (n = 39) were male (Table 1). The mean age at presentation was 53.7 ± 12.7 years. In all cases, mycobacterial infections were diagnosed after HCL. Fever was reported in 90% (n = 43). The median absolute lymphocyte and monocyte count at the time of diagnosis of mycobacterial infections was 10 (0–32)/mcL and 850 (260–1232)/mcL, respectively. Monocytopenia and lymphopenia were present in 95.6% (22/23) and 68.2% (15/22) patients, respectively. In 63% (30/48) of the patients, mycobacterial infections were identified before initiation of HCL-directed therapy. Reported HCL treatments included steroids (14/48, 29%), interferon-α (8/48, 17%), cladribine (12/48, 25%), rituximab (6/48, 13%), chlorambucil (5/48, 10%), and pentostatin (2/48, 4%). Splenectomy was performed in 46% (22/48) of cases (Table 1).
Clinical Profile of Mycobacterial Infections
Dissemination was reported in 71% (34/48) of patients (Table 1). The distribution of organ involvement was lymph nodes (29/48, 60%), lungs (27/48, 56%), liver (13/48, 27%), spleen (12/48, 25%), bone marrow (9/48, 19%), skin (7/48, 15%), pleura (6/48, 13%), and CNS (4/48, 8%). Blood cultures were positive for mycobacteria in 36% (12/33) of the tested patients. Granulomas were histopathologically demonstrated in 63% (30/48) of cases.
Microbiological Spectrum
Mycobacterial infections were attributed to MTBC in 12 cases (25%) and to nontuberculous mycobacteria (NTM) in 33 cases (69%); species distinction was not reported in 3 cases (6%). Among NTMs, the most frequent isolates were M. kansasii (18/33, 55%) and MAC (10/33, 30%) (Table 2).
Comparative Analysis by Pathogen
Key clinical features and outcomes among patients with MTBC (n = 12), MAC (n = 10), and M. kansasii (n = 18) are summarized in Table 2. Central nervous system involvement was observed exclusively in MTBC cases (4/12, 33%; P = .006). Mortality was highest with M. kansasii (9/18, 50%) compared with MTBC (4/12, 33%) and MAC (2/10, 20%), though not statistically significant (P = .273).
Dissemination of Mycobacterial Infection
Dissemination was a dominant clinical pattern across the cohort, and stratified analyses were undertaken to characterize its timing, extent, and pathogen-specific behavior (Supplementary Tables 2–6). Disseminated infection was frequent in both groups, identified in 76.7% of cases diagnosed before HCL therapy and 61.1% of those diagnosed after therapy (P = .251). Similarly, mycobacteremia occurred at similar rates before and after therapy (38.1% vs 33.3%; P = .784) (Supplementary Table 2). A comparison of disseminated and nondisseminated infections revealed no significant differences in cytopenias, granulomatous inflammation, or mortality (all P > .05), indicating that dissemination reflects underlying host susceptibility rather than clinical severity markers (Supplementary Table 3). Species-level analyses showed that dissemination was common with both MTBC (58.3%) and NTM (75.0%; P = .281), with broadly overlapping involvement of lymph nodes, liver, spleen, bone marrow, and lungs (Supplementary Table 4). Restricting the analysis to disseminated cases alone yielded similar patterns of organ involvement between MTBC and NTM (all P > .05) (Supplementary Table 5). Pulmonary disease was rarely localized: among 25 pulmonary infections with identifiable species, all MTBC cases (100%) and most NTM cases (84.2%; P = .299) had concurrent extrapulmonary involvement (Supplementary Table 6). Together, these findings establish dissemination as the predominant presentation of mycobacterial disease in HCL across treatment groups and pathogen categories.
Factors Associated With Mortality
Nineteen patients (40%) died during follow-up. Most clinical and laboratory variables did not differ significantly between patients with and without mortality in HCL with concomitant mycobacterial infection (Table 3). Male gender, fever, timing of diagnosis of mycobacterial infection in relation to HCL treatment, monocytopenia, lymphopenia, dissemination, and blood culture positivity for mycobacteria were comparably distributed across both groups. However, pulmonary involvement was significantly more frequent among patients who died (78.9%) compared with those who survived (41.4%, P = .01).
DISCUSSION
This systematic review synthesizes nearly 5 decades of published reports on mycobacterial infections in HCL. Infections frequently occurred before the initiation of HCL therapy, were predominantly disseminated, and were most often caused by NTM, particularly M. kansasii and MAC. Central nervous system involvement was observed only in MTBC cases. Despite therapy, overall mortality remained high (40%), with the highest rates among M. kansasii cases (50%). These findings underscore that mycobacterial disease in HCL reflects not only environmental exposure but also the convergence of distinct host immune defects with microbial virulence strategies [13, 17–50].
The burden of mycobacterial infections in HCL varies markedly across geography and time, raising the possibility that some of the observed patterns may reflect regional background epidemiology rather than a disease-specific association. Early retrospective series from the United States in the 1980s reported prevalences ranging from 4.8% to over 20%, predominantly due to atypical mycobacteria such as M. kansasii and MAC [12, 13, 38, 51, 52], while Indian cohorts have documented similarly high rates, with 11%–13% of patients developing tuberculosis, including disseminated and multidrug-resistant forms [14, 53]. In contrast, recent large European multicenter cohorts describe mycobacterial infections as rare (<1%) [54, 55]. These geographic discrepancies raise a legitimate alternative explanation: some differences in MTBC versus NTM distribution may simply mirror local pathogen prevalence, and in high-burden regions, tuberculosis may occasionally lead to the incidental discovery of underlying HCL. Publication bias further contributes, as most reported cases originate from high-income nations, whereas under-reporting from TB-endemic regions in Asia, Africa, and Latin America is likely [13, 17, 22, 23, 26–29, 33–38, 40, 41]. However, even when considering these contextual factors, the uniformly high rates of dissemination across diverse settings suggest that environmental exposure alone cannot account for the clinical phenotype. Data on other opportunistic infections in HCL, such as invasive fungal or viral pathogens, remain sparse, limiting the ability to determine whether mycobacterial dissemination is unique or part of a broader pattern of susceptibility. Comparative studies across different pathogens and epidemiologic backgrounds will be critical to disentangling the contributions of exposure from the intrinsic immunologic vulnerabilities characteristic of HCL.
The association between mycobacterial infection and HCL likely reflects the convergence of pathogen biology with the characteristic immune deficits of the disease. Pathogenic mycobacteria rely on specialized secretion systems to persist within host cells, while patients with HCL exhibit monocytopenia, lymphopenia, NK-cell dysfunction, and splenic sequestration, defects that collectively impair intracellular pathogen control [56, 57]. Consistent with this biology, more than 70% of infections in this review were disseminated, with frequent involvement of the lungs, liver, spleen, bone marrow, skin, and lymph nodes, and mycobacteremia documented in over one-third of cases. Granuloma formation remained intact in many patients, suggesting partial preservation of inflammatory containment despite impaired cell-mediated immunity. The consistently high rates of multiorgan involvement across subgroups, including cases with primary pulmonary presentation, further indicate that the immunologic milieu of HCL limits effective containment regardless of the mycobacterial species. That pulmonary MTBC and NTM infections were rarely isolated but instead almost universally accompanied by extrapulmonary involvement underscores that lung disease in HCL typically represents 1 manifestation of a broader systemic process. Together, these patterns provide a coherent mechanistic explanation for the extent of dissemination observed and reinforce the need for thorough systemic evaluation and a high index of suspicion for multiorgan involvement whenever mycobacterial infection is considered in patients with HCL.
Distinguishing HCL progression from infection remains a clinically challenging task. Fever and generalized lymphadenopathy are uncommon in untreated HCL and should instead raise suspicion for opportunistic infection, especially Mycobacterium spp. [4, 14]. Similarly, hepatic, splenic, skin, and marrow lesions should not be attributed to leukemia alone without considering infection [58]. In endemic regions, mycobacterial infections may even precede or unmask HCL, and the co-occurrence of mycobacterial disease with splenomegaly, lymphomonocytopenia, or autoinflammatory features (eg, Sweet's syndrome, vasculitis, arthralgias) should prompt evaluation for underlying HCL [58]. While cladribine and pentostatin have transformed HCL outcomes, both induce profound and durable CD4⁺ lymphopenia, compounding infection risk [59]. Splenectomy, performed in nearly half of the reviewed cases, may further impair clearance of disseminated pathogens [60]. Vigilant infection surveillance is therefore critical at all stages of the disease, including before treatment, during therapy, and in remission.
The predominance of NTMs, particularly M. kansasii and MAC, raises therapeutic challenges. Unlike MTBC, for which treatment guidelines are well established, NTM management is more heterogeneous, with species-specific regimens that often require prolonged multidrug therapy and may be limited by significant toxicity [61]. This is particularly problematic in HCL patients who often have marrow suppression, hepatic dysfunction, or are receiving immunosuppressive chemotherapy [58]. Future research into optimized treatment strategies for NTM in hematologic malignancies is urgently needed, including the role of newer antimycobacterial agents.
From a practical standpoint, the findings highlight the importance of vigilance for infection even before starting HCL-directed therapy. Baseline screening for mycobacterial infection, including chest imaging and targeted microbiologic evaluation in endemic settings, could be considered for selected patients with unexplained systemic symptoms. While the concept of pre-emptive therapy against mycobacterial infections is appealing, its practical implementation remains extremely challenging. Hence, heightened clinical vigilance, timely microbiological investigations, and context-specific empiric therapy remain the most pragmatic approaches in such patients. These measures, while not yet supported by formal guidelines, may mitigate some of the excess mortality observed in this population. Moving forward, systematic collection of prospective data through multicenter registries could address several knowledge gaps. These include the true incidence of mycobacterial disease in HCL, comparative outcomes between MTBC and NTM infections, the impact of HCL therapy on infection risk, and optimal antimicrobial regimens. Integration of molecular pathogen diagnostics with immunophenotypic monitoring of HCL may further clarify the interplay between host immunity and pathogen persistence. Finally, research into prophylactic or pre-emptive strategies, whether antimicrobial, immunologic, or a combination, represents an unmet need for reducing infection-related mortality in this highly susceptible group.
Our analysis is limited by reliance on case reports and small case series, which are subject to publication bias, incomplete reporting, and heterogeneity in diagnostic and therapeutic approaches. Many cases predate modern microbiologic methods and current therapeutic standards, restricting direct applicability to contemporary practice. Nonetheless, pooling these data provides valuable insight into patterns of susceptibility, clinical presentation, and outcomes that would otherwise remain anecdotal.
CONCLUSION
Patients with HCL demonstrate a clear predisposition to disseminated mycobacterial infections, reflected in the high proportion of cases presenting with multiorgan involvement. This susceptibility is consistent with the characteristic immune deficits of HCL, particularly monocytopenia, which compromises the host's defense against intracellular pathogens. Clinically, when patients with HCL develop fever, lymphadenopathy, or otherwise unexplained systemic inflammation, mycobacterial infection should be considered early, as presentations are frequently disseminated and atypical. The diversity of species identified, encompassing both MTB and multiple NTM pathogens, reinforces the importance of timely, species-level microbiological diagnosis to guide therapy. Collectively, our findings underscore several key takeaways: clinicians should maintain heightened awareness for mycobacterial disease in HCL; diagnostic evaluation should be prompt and thorough when compatible symptoms arise; and future research is needed to define incidence, understand comparative risks with other indolent hematologic malignancies, and improve early recognition and management strategies in this vulnerable population.
Supplementary Material
ofag063_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Maćkowiak K, Jankowiak M, Szewczyk-Golec K, Hołyńska-Iwan I. Hairy cell leukemia—etiopathogenesis, diagnosis and modern therapeutic approach. Biochem Medica 2024; 34:020502.10.11613/BM.2024.020502 PMC 1117765838882583 · doi ↗ · pubmed ↗
- 2Tadmor T, Polliack A. Epidemiology and environmental risk in hairy cell leukemia. Best Pract Res Clin Haematol 2015; 28:175–9.26614895 10.1016/j.beha.2015.10.014 · doi ↗ · pubmed ↗
- 3Staines A, Cartwright RA. Hairy cell leukaemia: descriptive epidemiology and a case-control study. Br J Haematol 1993; 85:714–7.7918034 10.1111/j.1365-2141.1993.tb 03213.x · doi ↗ · pubmed ↗
- 4Gupta AK, Sachdeva MUS, Ahluwalia J, et al Haematological profile of 21 patients with hairy cell leukaemia in a tertiary care centre of north India. Indian J Med Res 2015; 142:426–9.26609034 10.4103/0971-5916.169204 PMC 4683827 · doi ↗ · pubmed ↗
- 5Lukácsi S, Nagy-Baló Z, Erdei A, Sándor N, Bajtay Z. The role of CR 3 (CD 11b/CD 18) and CR 4 (CD 11c/CD 18) in complement-mediated phagocytosis and podosome formation by human phagocytes. Immunol Lett 2017; 189:64–72.28554712 10.1016/j.imlet.2017.05.014 · doi ↗ · pubmed ↗
- 6Ben Nasr A, Haithcoat J, Masterson JE, Gunn JS, Eaves-Pyles T, Klimpel GR. Critical role for serum opsonins and complement receptors CR 3 (CD 11b/CD 18) and CR 4 (CD 11c/CD 18) in phagocytosis of Francisella tularensis by human dendritic cells (DC): uptake of Francisella leads to activation of immature DC and intracellular survival of the bacteria. J Leukoc Biol 2006; 80:774–86.16857732 10.1189/jlb.1205755 · doi ↗ · pubmed ↗
- 7Mackowiak PA, Demian SE, Sutker WL, et al Infections of hairy cell leukemia. Clinical evidence of a pronounced defect in cell-mediated immunity. Am J Med 1980; 68:718–24.7377223 10.1016/0002-9343(80)90259-4 · doi ↗ · pubmed ↗
- 8Sivina M, Kreitman RJ, Peled A, Ravandi F, Burger JA. Adhesion of hairy cells leukemia (HCL) cells to stromal cells can be inhibited by blocking VLA-4 integrins and CXCR 4 chemokine receptors. Blood 2011; 118:1760.