Current and emerging maintenance strategies after stem cell transplantation in children and adolescents with acute leukemias
Alexander W. Rankin, Amy K. Keating, Rolla F. Abu-Arja, Monica S. Thakar, Hemalatha G. Rangarajan

TL;DR
This paper reviews strategies to prevent leukemia relapse after stem cell transplants in children and adolescents, focusing on emerging targeted and immunotherapies.
Contribution
The paper provides a comprehensive review of post-HSCT maintenance strategies specifically for pediatric and adolescent patients with acute leukemias.
Findings
Post-HSCT relapse remains a significant challenge in pediatric acute leukemias.
Targeted and immunotherapeutic agents show promise in improving post-HSCT outcomes.
Early prophylactic intervention can improve survival in high-risk patients.
Abstract
Hematopoietic stem cell transplantation (HSCT) can promote durable long-term remissions for children and adolescents with high-risk acute leukemias. While many patients with acute lymphoblastic leukemia (ALL) and acute myeloid leukemia (AML) can achieve a cure, post-HSCT relapse remains a possibility for many. Recent therapeutic advances, particularly in the realm of targeted therapeutics, have revolutionized both first-line and relapsed/refractory management strategies, opening the door to more personalized and potentially less toxic approaches to treatment. Many of these agents have also either been proposed or have been actively investigated as having a role in the post-HSCT setting. Post-HSCT relapse often carries a dismal prognosis, and early prophylactic intervention has in many cases been shown to improve outcomes. Herein, we comprehensively review maintenance strategies for…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
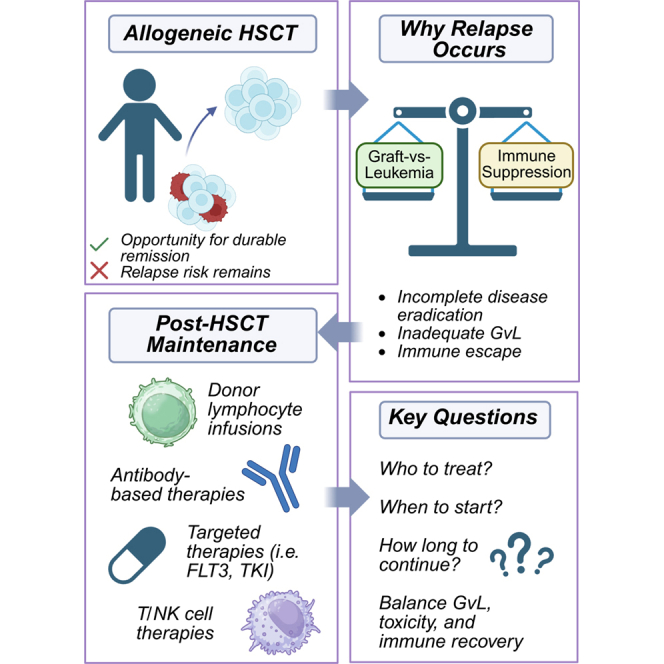 Figure 1
Figure 1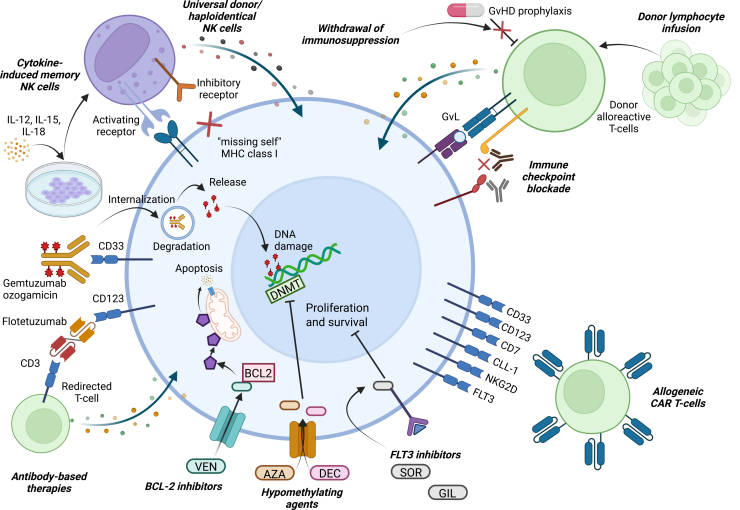 Figure 2
Figure 2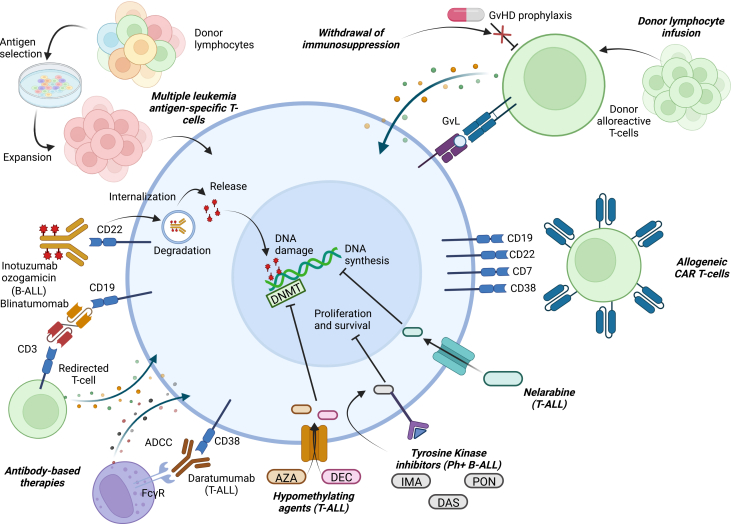 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAcute Lymphoblastic Leukemia research · Acute Myeloid Leukemia Research · Hematopoietic Stem Cell Transplantation
Introduction
Acute leukemias represent the most common cancer diagnoses in children and adolescents. According to recent data, from 2018 to 2022 the 5-year incidence of leukemia in individuals <20 years of age was 4.8 per 100,000, with acute lymphoblastic leukemia (ALL) (3.8 per 100,000) being more common than acute myeloid leukemia (AML) (0.8 per 100,000).1 Significant treatment advances over the past several decades have led to improvements in survival outcomes, with patients with B cell ALL (B-ALL) collectively having a 5-year overall survival (OS) rate of around 90% or higher,2^,^3^,^4^,^5^,^6^,^7 whereas those with AML have 5-year OS rates of 50%–70% or lower for higher risk patients.8^,^9^,^10^,^11 Patients with T cell ALL (T-ALL), while historically having outcomes below patients with B-ALL, have shown comparable outcomes in the modern era.12^,^13 Despite what are often good long-term outcomes, prospects for durable remission in those with relapsed disease are much lower, with 5-year OS rates dipping to around 50%–60% for those with first relapse of B-ALL according to a Children’s Oncology Group (COG) study of cases from 1996 to 2014,14 and even lower for relapsed AML15 or T-ALL.16
Allogeneic hematopoietic stem cell transplantation (HSCT) can lead to long-term survival for patients with relapsed disease or higher risk upfront disease, such as those with high-risk cytogenetic features or poor response to chemotherapy. HSCT involves the replacement of the host hematopoietic system, which in the case of leukemia is impacted by disease, with stem cells and other immune cells from a healthy donor after ablation or near-ablation of the host bone marrow with chemotherapy with or without radiation. For certain diseases, autologously collected stem cells from the host can be used to rescue hematopoietic function after administration of high doses of chemotherapy. In the case of leukemia, however, allogeneic stem cells collected from a related or unrelated donor are preferred due to both the possible contamination of an autologously collected graft with malignant cells and the beneficial effect of alloreactive surveillance mediated by donor immune cells commonly termed the graft-versus-leukemia (GvL) effect.17
While cure can be achieved, post-HSCT relapse rates remain high, and survival rates are still not optimal. A recent study reported 5-year leukemia-free survival (LFS) after HSCT ranging from 33%-68% for ALL and 25%–78% for AML, with 5-year relapse incidence of 16%–47% and 14%–58%, respectively.18 Therefore, strategies for remission maintenance after HSCT are greatly needed, particularly in higher risk populations.
To date, there is a lack of evidence-based strategies to promote durable remission in patients with acute leukemias after HSCT. This is particularly true in the pediatric and adolescent population, where there is a significant dearth of evidence. Herein, we will review the available evidence for post-HSCT remission maintenance strategies for AML (Figure 1) and ALL (Figure 2) in the pediatric and adolescent population and discuss some possible future directions. Due to the paucity of literature on post-HSCT maintenance in pediatric and adolescent patients, we will draw from evidence in adult patients where available, as well as preemptive approaches for the emergence of mixed chimerism or measurable residual disease (MRD), which often precede overt relapse.Figure 1. Post-HSCT therapeutic interventions for AMLOverview of the various current and potential strategies for post-HSCT maintenance for children and young adults with acute myeloid leukemia (AML). Large blue cell in the center represents an AML cell, with various categories of therapeutic interventions detailed circumferentially around the periphery. Abbreviations: AZA, azacitidine; BCL2, B cell lymphoma 2; DEC, decitabine; DNA, deoxyribonucleic acid; DNMT, DNA methyltransferase; FLT3, FMS-like tyrosine kinase 3; GIL, gilteritinib; GvHD, graft-versus-host disease; GvL, graft-versus-leukemia; IL, interleukin; MHC, major histocompatibility complex; NK, natural killer; SOR, sorafenib; VEN, venetoclax.Figure 2. Post-HSCT therapeutic interventions for ALLOverview of the various current and potential strategies for post-HSCT maintenance for children and young adults with acute lymphoblastic leukemia (ALL). Large blue cell in the center represents an ALL cell, with various categories of therapeutic interventions detailed circumferentially around the periphery. Abbreviations: ADCC, antibody-dependent cellular cytotoxicity; AZA, azacitidine; DAS, dasatinib; DEC, decitabine; DNA, deoxyribonucleic acid; DNMT, DNA methyltransferase; FcγR, Fc gamma receptor; GvHD, graft-versus-host disease; GvL, graft-versus-leukemia; IMA, imatinib; PON, ponatinib.
As the rationale for therapy initiation post HSCT varies between studies, we will employ the terms “prophylactic” or “maintenance” to refer to an agent initiated before the emergence of MRD, mixed chimerism, or overt relapse, while the term “preemptive” will be used to describe an agent initiated after the emergence of MRD or mixed chimerism but prior to overt relapse. Additionally, use of the term MRD is somewhat vague and has evolved greatly over the past two decades. Multiple methods with varying sensitivities for detection of disease exist,19^,^20^,^21 and different studies may employ variable thresholds for defining MRD positivity. A standardized approach to measuring and defining the presence of MRD is needed, especially when evaluating the efficacy of interventions guided by its presence or absence, such as post-HSCT maintenance.
Rationale for post-HSCT maintenance
While long-term durable remission after HSCT mediated by GvL is achievable in many patients with acute leukemias, the risk of relapse remains significant.22 The question as to which patients would benefit from maintenance therapy after HSCT remains debated. While some patients will relapse post-HSCT, others will achieve long-term remission, and whether the risk/benefit analysis would tilt toward all patients receiving some sort of maintenance post-HSCT or only those at highest risk of relapse remains unknown. Safety considerations regarding potential impacts on engraftment and immune reconstitution, along with how these effects may alter GvL, must be taken seriously. It is probable that maintenance approaches will provide the most benefit in higher risk populations, such as those with certain cytogenetic/molecular features,23 poor response to prior therapy,24 or pre-HSCT MRD.25 However, in the pediatric population, the calculus may favor more aggressive maintenance strategies given the general greater tolerability of therapy and longer remaining life expectancy as compared to older patients. This being said, care must be taken when extrapolating data from adults to children as toxicities may differ and data regarding late-onset side effects may not be available. The advent of targeted therapies will continue to expand the pool of patients who will have maintenance options available to them, but the populations that will benefit from each individual approach will be limited based on underlying disease characteristics, necessitating an increasingly personalized approach.
Certain biomarkers, such as the emergence of MRD26^,^27^,^28^,^29^,^30^,^31^,^32^,^33 or mixed chimerism,34^,^35^,^36^,^37^,^38 often herald overt relapse and can be acted upon through preemptive interventions; however, it is likely that maintenance approaches employed prior to the emergence of MRD or mixed chimerism may be more effective at exerting disease control. Many of the preemptive or maintenance strategies that have been reported in the literature have previously demonstrated efficacy in the upfront or relapse settings, and their use post HSCT has been extrapolated from these data. Additionally, there are several therapeutics that have shown promise in their potential to synergize with the GvL effect of HSCT, as discussed further, which may support their application in the post-HSCT setting.
AML
Withdrawal of immunosuppression
The GvL effect mediated through alloreactive donor T-cell recognition of minor histocompatibility antigens is crucial in maintaining AML remission after HSCT.39^,^40 Immune escape from GvL is thought to play a major role in AML relapse,41 and suppression of donor T-cell activity through prolonged use of immunomodulatory medications post-HSCT may augment this.42 Withdrawal of immunosuppression (WIS) is a frequent strategy for emergence of MRD and/or mixed chimerism, and there is some evidence that early tapering may improve outcomes,43^,^44 particularly with modern graft-versus-host disease (GvHD) prevention strategies. While preemptive WIS in isolation may be of limited efficacy, its use in combination with other approaches may provide benefit. Regardless, an important consideration is that early WIS carries the risk of eliciting GvHD, in which case the need for augmented immunosuppression may erase any benefits derived from early WIS. Though often employed in higher risk pediatric patients with AML, debate remains regarding the particular scenarios in which early prophylactic WIS is of benefit.
Donor lymphocyte infusions
Boosting the GvL effect through donor lymphocyte infusion (DLI) has been attempted both in the treatment of overt AML relapse post-HSCT and in the preemptive management of impending relapse. While DLI has been an effective strategy for treating relapsed chronic myeloid leukemia, experience in AML has been more muted.45^,^46 However, if used as a preemptive approach for the emergence of MRD or mixed chimerism as opposed to overt relapse, benefit may be more pronounced.47^,^48 For example, one study in pediatric patients with AML showed that those who developed mixed chimerism post-HSCT and received either WIS or DLI had significantly improved event-free survival (EFS).49 A similar study reported that 6 of 13 patients who developed mixed chimerism and were treated with either WIS or DLI reestablished complete chimerism and maintained long-term remission.50 However, all of those who did not receive an intervention relapsed. These studies suggest that, in certain cases, early immunologic intervention prior to overt relapse can be an effective preemptive strategy to maintain ongoing remission.
An alternative to using DLI as preemptive management or treatment of relapse would be to employ it prophylactically for maintenance of remission. Here, while extrapolated from data in adult patients with less robust data in children, efficacy has been demonstrated with certain caveats. Several studies have reported this to be a feasible approach and demonstrated the ability to improve the durability of post-HSCT remissions,47^,^51^,^52^,^53^,^54 often in patients with high-risk disease. While there is no adequate data to determine the optimal dosing regimen for prophylactic infusion, most reports have involved a single dose. Importantly, any potential benefit must be weighed against the not insignificant risk of triggering GvHD, which may occur in as high as 50%–80% of patients. This risk has been mitigated to some degree by certain groups who have delayed infusion until day 120 in those who are off immunosuppression53^,^55^,^56; however, toxicity has been a limiting factor to more broad application of this approach. Additionally, donor type may influence outcomes, although data do not exist to clearly inform the decision to pursue DLI based on donor type alone. Some studies have suggested lower risk of GvHD when using matched related donors compared to unrelated donors.53^,^56^,^57 However, related donors may also conceivably generate less alloreactivity and GvL, leading to higher relapse risk.52^,^53^,^56 While donor impact on survival outcomes is not proven, different dosing regimens are often employed for related and unrelated donors to account for expected differences in toxicity.50^,^52
Additional strategies to improve the efficacy of DLI may involve combinatorial approaches utilizing agents with known immunomodulatory properties, such as hypomethylating agents58^,^59^,^60^,^61 (discussed further), or cellular manipulation strategies to promote efficacy while limiting GvHD, such as TCRαβ+ T cell depletion.62^,^63 Studies specific to pediatric patients are needed to determine if data from adult patients can appropriately be extrapolated to a younger population.
Chimeric antigen receptor T cells
While chimeric antigen receptor (CAR) T cells have demonstrated remarkable efficacy in relapsed/refractory B-ALL, the same degree of success has not been seen in AML. CAR T cells directed at multiple targets are currently under preclinical or clinical investigation, including CD33,64^,^65^,^66^,^67 CD123,68^,^69 CD7,70^,^71 CLL-1,72^,^73^,^74 NKG2D,75 and FLT376^,^77; however, to date clinical efficacy is not proven. Allogeneic donor-derived CAR T cells are also under investigation for relapsed disease after HSCT.78^,^79 Future studies may consider donor-derived CAR T cells as a post-HSCT maintenance option.
Natural killer cells
Natural killer (NK) cells, which play a key role in promoting GvL without significantly driving GvHD, represent a promising cellular therapy approach to post-HSCT maintenance. Several studies have demonstrated the feasibility of using NK cells in the treatment of relapsed disease with mixed outcomes.80^,^81 The ongoing KARMA trial (NCT05503134) is a single-center phase 1/2 study evaluating universal donor NK cells combined with chemotherapy for the treatment of relapsed/refractory AML in young adult patients aged 18–25. Outside of the HSCT setting, Nguyen et al. evaluated the use of prophylactic haploidentical killer cell immunoglobulin-like receptor (KIR)-mismatched NK cells for consolidation of remission in pediatric patients.82 Twenty-one patients in first complete remission (CR) with a median age of 6.0 years received NK cell infusions following conditioning with no reported major toxicities, including GvHD. The majority displayed transient NK cell engraftment, but NK cells were not found to decrease the incidence of relapse or improve EFS or OS over chemotherapy alone. The ongoing EXCEL trial (NCT04836390) is a pilot phase 2 study evaluating the use of prophylactic ex-vivo-expanded haploidentical NK cells as consolidation of remission in the post-HSCT setting in pediatric and young adult patients. No results have been reported to date.
One limitation of NK cell therapy has been a lack of in vivo persistence. Cytokine-induced memory-like (CIML)-NK cells, generated through ex vivo culture with cytokines such as interleukin (IL)-12, IL-15, and IL-18, may further improve upon NK cell antileukemia efficacy and enhance persistence.83 There are several ongoing clinical trials utilizing this approach in pediatric patients, including for relapsed/refractory disease, post-HSCT relapse, and post-HSCT remission maintenance. Bednarski et al. have reported on the treatment of 9 pediatric/young adult patients with post-HSCT relapse using donor-derived CIML-NK cells in combination with DLI (NCT03068819).84 NK cells expanded and displayed persistent functional response without an increased incidence of GvHD, and 4/8 evaluable patients achieved a CR. Two of those patients maintained a durable remission for >3 months. Further data from ongoing efforts are anticipated to help inform the efficacy of post-HSCT NK cell approaches in the pediatric and adolescent population.
Other cellular therapies
Other modes of cellular therapy that may hold potential in the post-HSCT setting include T cell receptor (TCR) T cell therapies85^,^86 or cytokine-induced killer (CIK) cells. One group demonstrated that EBV-specific donor CD8^+^ T cells transduced with WT1-specific TCRs can be beneficial in maintaining GvL without inducing GvHD when employed prophylactically.87 Another group infused leukemia antigen-specific T cells (PRAME, WT1, survivin, and NY-ESO-1) prophylactically with a tolerable safety profile and encouraging efficacy.88 CD8^+^ T cells targeting the minor histocompatibility antigen HA-1 have also been proposed in the post-HSCT setting.89^,^90^,^91 Regarding CIK cells, a recent study reported on prophylactic infusion post HSCT for myeloid neoplasms but noted similar relapse and survival rates compared to historical controls.92
Antibody-based therapies
The CD33-targeted antibody-drug conjugate gemtuzumab ozogamicin (GO) has altered the landscape of pediatric AML treatment in recent years. Various studies have now been published regarding its utility in treating newly diagnosed AML93^,^94^,^95^,^96 as well as relapsed/refractory disease.97 Its use in the post-HSCT setting as both salvage combined with chemotherapy98 and prophylactically99^,^100^,^101 have been explored with limited data. Potential concerns with using GO in the post-HSCT setting include its association with sinusoidal obstructive syndrome (SOS) as well as concerns about toxicity to engrafting hematopoietic stem cells. As a novel approach to the latter problem, an ongoing clinical trial is investigating the use of GO prophylactically as post-HSCT maintenance following therapy with VOR33, an allogeneic CRISPR-Cas9-edited HSCT product lacking the CD33 protein (NCT04849910).102
Flotetuzumab is a dual-affinity re-targeting antibody that binds CD123 on AML cells and CD3^+^ T cells, working to redirect T cell cytotoxicity against AML. It has shown encouraging activity in adults with relapsed/refractory AML,103^,^104 and the COG PEPN1812 phase 1 study demonstrated safety and tolerability in children with an overall response rate of 20% at the recommended phase 2 dose.105 There is no data on its use in the post-HSCT setting, although a phase 1 trial for post-HSCT relapse (NCT05506956) has recently been completed. Pivekimab sunirine (IMGN632)106 and tagraxofusp107 are two additional CD123-targeting agents being investigated in the early-phase setting for AML that may hold future potential for post-HSCT application.
AML patients with the CBF2AT3-GLIS2 oncogenic fusion (“RAM” phenotype) have a particularly poor prognosis. STRO-002, an antibody-drug conjugate targeting FR-α expressed on RAM phenotype AML, has shown promising activity in relapsed/refractory disease and seems to be more effective in those with low tumor burden,108 again suggesting a potential application post-HSCT as preemptive or prophylactic therapy. Indeed, while published data are not yet available, given the extraordinarily high risk of relapse, many centers have unpublished experience safely utilizing STRO-002 prophylactically as post-HSCT maintenance therapy. Investigation of ELU001,109 a similar molecule targeting CBF2AT3-GLIS2 AML was also planned, but the trial was withdrawn prior to enrollment (NCT05622591).
Hypomethylating agents
Agents such as azacitidine and decitabine have been studied extensively in the post-HSCT setting in adults as treatment of relapse110^,^111^,^112 as well as preemptive113 and maintenance51^,^114^,^115^,^116^,^117 therapies. Several studies have demonstrated an immunomodulatory role for hypomethylating agents in terms of increasing the expression of tumor antigens such as WT1118 and MAGE,119^,^120 promoting CD8^+^ cytotoxic T cell responses, and augmenting the expansion of regulatory T cells.121^,^122^,^123 In adult patients, most studies to date have demonstrated benefit in terms of improving survival and decreasing relapse rate when azacitidine or decitabine are used as prophylaxis post-HSCT,116^,^117^,^124^,^125^,^126 but some have failed to show improvement in outcomes.127^,^128^,^129
In the pediatric population, studies have begun to investigate the feasibility and efficacy of using hypomethylating agents in combination with other agents in relapsed patients.130^,^131^,^132^,^133 There are also several studies that have explored the use of azacitidine or decitabine prophylactically as post-HSCT maintenance in pediatric patients. Gao et al. conducted a phase 2 randomized controlled trial using the combination of prophylactic decitabine and granulocyte colony-stimulating factor (G-CSF) in patients with AML who were MRD negative after HSCT.134 While the study enrolled mostly adult patients, approximately 25% were <20 years of age. They found a 2-year cumulative incidence of relapse of 15% in the study arm vs. 38.3% in the control arm with incidence of chronic GvHD being 34.0% and 48.2%, respectively. They also noted increased proportions of NK cells, CD8^+^ T cells, and regulatory T cells in the study arm.
Tamura et al. presented a case series of 3 high-risk pediatric AML patients who were in remission post HSCT and received low-dose azacitidine prophylactically.135 The approach was feasible, and all remained in remission 13–41 months after HSCT with one developing acute GvHD. Recently, Booth et al. published their single-center experience using prophylactic low-dose azacitidine in combination with DLI as post-HSCT maintenance.59 Compared to historical controls, patients who received maintenance therapy had a 2-year LFS of 88.2% vs. 61.5% (p = 0.06), OS of 88.2% vs. 69.2% (p = 0.15), rate of grade II–IV acute GvHD of 38% vs. 30% (p = 0.51), and rate of moderate-severe chronic GvHD of 13% vs. 17% (p = 0.68). Given the experience in adult patients, application to pediatric patients is reasonable; however, larger prospective studies are needed.
B cell lymphoma 2 inhibitors
Venetoclax, a B cell lymphoma 2 (BCL-2) inhbitor, has been used effectively, particularly in combination with azacitidine, to target leukemia stem cells in adult patients with AML.136^,^137 There are also data to suggest that venetoclax is safe and tolerable as post-HSCT maintenance in adults.138^,^139 In pediatrics, the data are more limited, but available evidence is encouraging.140^,^141^,^142 Although no studies have been published on its use prophylactically as post-HSCT maintenance in pediatrics, the VIALE-T trial (NCT04161885) will evaluate the combination of venetoclax and azacitidine as maintenance in patients down to the age of 12 years.
FMS-like tyrosine kinase 3 inhibitors
Data suggest that in patients with FMS-like tyrosine kinase 3 (FLT3)-mutant AML, either with internal tandem duplication (ITD) or mutation in the tyrosine kinase domain (TKD), the addition of a targeted inhibitor is safe and improves outcomes in both adults and pediatrics.10^,^143^,^144 Indeed, in the post-HSCT setting, the ability of FLT3 inhibitors to induce alloimmune effects that may enhance GvL,145^,^146^,^147 which may be even more pronounced in combination with other immunotherapeutic approaches such as DLI,148 provides a strong rationale for their use.
Multiple studies in adult patients have suggested the potential of prophylactic post-HSCT maintenance with FLT3 inhibitors149^,^150^,^151^,^152^,^153^,^154 to improve remission duration. A recent randomized study showed that preemptive post-HSCT gilteritinib was beneficial in FLT3-ITD patients with either pre- or post-HSCT detectable MRD; however, no benefit was seen in those without detectable MRD.155 In pediatrics, the experience is less robust. Battipaglia et al. studied sorafenib prophylaxis in patients down to the age of 15 years, but the median age of subjects was 46 years.156 A retrospective study by Tarlock et al. analyzed the use of post-HSCT sorafenib in 15 pediatric patients, 6 of whom were treated as prophylaxis.157 All patients who received sorafenib preemptively either for pre-HSCT MRD or emergence of post-HSCT MRD were alive and in CR at 48 months. Pollard et al. also retrospectively examined the use of sorafenib post-HSCT in 13 patients, 8 of whom were treated prophylactically.158
Use in pediatrics as maintenance is often pursued and is reasonable given adult data and growing experience in children. It also remains unknown which FLT3 inhibitor, if any, is superior for use as maintenance and the optimal duration of maintenance is yet to be elucidated, although the European Society for Bone Marrow Transplantation (EBMT) recommendation is to continue for 2 years post-HSCT.159
Other targeted therapies
Several other targeted agents are being actively investigated or may have future potential as maintenance in the post-HSCT setting. Histone deacetylase inhibitors, such as hypomethylating agents and FLT3 inhibitors, may have some level of immunomodulatory effect via control of cytokine secretion and transcriptional modification of genes regulating immune checkpoint molecules.160 Post-HSCT, panobinostat maintenance has resulted in survival rates that compare favorably to historical data.161 A separate phase 3 trial in adult patients has completed accrual (NCT04326764), and a phase 1 trial of vorinostat in combination with azacitidine is currently recruiting (NCT03843528).
Isocitrate dehydrogenase (IDH) mutations can lead to epigenetic dysregulation and impairment of cellular differentiation in AML.162 IDH inhibitors have shown some efficacy for relapsed/refractory AML in adults,163 and both enasidenib164 and ivosidenib165 have been studied prophylactically as post-HSCT maintenance with some preliminary signals of efficacy. However, IDH1/2 mutations are rare in pediatric AML,166 making it doubtful they would have a large impact in younger populations.
The menin inhibitor revumenib received Food and Drug Administration (FDA) approval in 2024 for relapsed/refractory KMT2a-rearranged AML in children and adults,167^,^168 and Zucenka et al. reported on its prophylactic or preemptive use post-HSCT for patients enrolled in the pivotal AUGMENT-1 trial.169 Nine patients enrolled in the trial went on to receive revumenib after HSCT if in morphological CR, resuming between 59 and 180 days after. CR was maintained in 6 patients, with one patient who was MRD positive becoming MRD negative after initiating therapy. Its use post-HSCT warrants further study.170
Hedgehog pathway signaling is important for maintenance of leukemia stem cell populations, and pathway inhibition may mitigate leukemia development and sensitize leukemia stem cells to chemotherapy.171 However, the Hedgehog pathway inhibitor glasdegib to date has not shown efficacy as post-HSCT maintenance.172
CD47, an anti-phagocytic transmembrane protein, is highly expressed on AML leukemia stem cells, and increased expression is associated with worse prognosis.173 Magrolimab is an anti-CD47 monoclonal antibody that has not yet been studied in the post-HSCT setting but has shown some promise as part of combination therapy in early trials for de novo AML.174 However, results from more recent trials have been more muted.175^,^176
Checkpoint blockade
Targeting inhibitory checkpoint molecules, specifically programmed cell death protein (PD)-1/PD-ligand (L)1 and cytotoxic T lymphocyte-associated protein (CTLA)-4, may augment the antileukemia GvL effect after HSCT. Davids et al. showed that the administration of ipilimumab for patients with recurrent hematologic malignancies after HSCT led to some durable responses, including 2 patients with extramedullary AML.177 However, immune-mediated adverse events including acute GvHD occurred, and this has also been demonstrated with the use of nivolumab178^,^179^,^180 and pembrolizumab181 with only moderate antitumor activity. Whether checkpoint inhibition as maintenance in patients without significant tumor burden would be more efficacious and tolerable is unknown, and combination therapy with other agents to enhance GvL without promoting GvHD may provide theoretical benefit. Several trials are continuing to investigate the use of checkpoint inhibition for AML post-HSCT (NCT03286114, NCT03600155, and NCT02846376).
ALL
Withdrawal of immunosuppression
While the GvL effect is generally thought to be more potent in AML than ALL, WIS to enhance graft activity against the leukemia has been employed in ALL as well. Often used as a preemptive strategy for the management of mixed chimerism, it is employed alone or in combination with DLI to enhance GvL. Several studies in pediatrics have suggested that this can be an efficacious approach at restoring full donor chimerism and decreasing relapse.37^,^182^,^183 While there is little in the literature studying prophylactic early WIS in patients with ALL, relapse risk often informs clinicians’ decision to begin immunosuppression taper early in these patients, with higher risk patients often beginning withdrawal earlier.184 Ultimately, however, data are limited and not sufficient to determine the true efficacy of early WIS prior to the emergence of mixed chimerism or overt relapse.
Donor lymphocyte infusions
The utility of DLI has been limited in ALL. Multiple early studies in adults suggested that response rates were low in patients with relapse,45^,^185 and poor efficacy was linked in one study to the limited proliferative capacity of ALL-specific alloreactive T cells and was dependent on the HLA disparity between the donor and the patient.186 Additional early concerns had surrounded the high rates of GvHD associated with DLI; however, a recent study using a relatively large cohort of pediatric and young adult patients suggested rates comparable to the general HSCT population (acute: 19.4%, chronic: 9.2%).187 Further, while some studies have begun to investigate the utility of prophylactic DLI for post-HSCT ALL relapse prevention and have shown some benefit, many studies include both patients with AML and ALL, making it difficult to parse differential outcomes between the two different disease processes.188^,^189^,^190
In pediatrics, the outcomes using DLI for post-HSCT ALL relapse have been similarly underwhelming. Levine et al. reported outcomes of 49 children who received DLI for relapse after HSCT, including 18 with ALL.191 Prognosis was poor overall, especially in those who relapsed early (<6 months after HSCT) and in those with ALL, among whom 13/18 died of leukemia without achieving remission. Additionally, of the 4 who achieved remission, 2 later died from relapse and 1 from chronic GvHD. When all patients were compared to a matched cohort that did not receive DLI, no difference was found in survival between those who received DLI and those who did not. In contrast, a single-center retrospective study reported a 71% 5-year OS for children with ALL who received DLI post-HSCT, higher than the 32% for patients with AML.192 However, only 7 patients with ALL were included in this study.
In the preemptive setting, a retrospective study from Germany reported that there was no difference in relapse rates or survival when comparing pediatric patients with ALL who received DLI for mixed chimerism or emergence of MRD and those who did not.193 Gruhn et al. recently presented results of 34 pediatric patients (10 of whom had ALL), the majority of whom received preemptive or prophylactic DLI.194 While they did not separate response by underlying disease, 83% of those treated preemptively did not develop overt relapse, and none of the patients treated prophylactically relapsed. Interestingly, DLI was combined in several patients with blinatumomab, inotuzumab, and zoledronic acid to promote TCRγδ+ T cell cytotoxicity, all of which could be interesting avenues for future combinatorial studies.
In short, while efficacy for preemptive or salvage therapy appears to be minimal, the appropriate role for post-HSCT DLI as relapse prophylaxis remains to be elucidated.
Tyrosine kinase inhibitors
Maintenance with tyrosine kinase inhibitors (TKIs) is frequently pursued after HSCT for patients with Philadelphia chromosome-positive (Ph+) B-ALL, and many would now consider it to be standard of care. A study by the EBMT Acute Leukemia Working Party showed that the use of TKIs prophylactically after HSCT was associated with improved LFS and OS as well as a lower incidence of relapse.195 Interestingly, in multivariate analysis post-HSCT, TKI use was associated with a lower incidence of GvHD. First-,196 second-,197^,^198 and third-199^,^200 generation TKIs have all shown tolerability and efficacy in the post-HSCT setting; however, evidence on the best choice of TKI is mixed.201 A retrospective comparison of imatinib and dasatinib as post-HSCT prophylaxis did not show difference in outcomes but less tolerability of dasatinib.202 However, a randomized trial in children found dasatinib to be superior to imatinib when added to upfront chemotherapy.203 The EBMT has produced consensus guidelines on TKI use post-HSCT, recommending imatinib for most patients and dasatinib in cases of imatinib resistance, early molecular relapse, or significantly elevated BCR-ABL transcripts (>10^4^).204 Duration of therapy is generally at least 24 months, as this has been shown to reduce relapse risk.205
In pediatrics specifically, the COG AALL0031 and the intergroup EsPhALL2010 studies both demonstrated the utility of imatinib as part of upfront therapy for patients with Ph+ ALL, with the addition of a TKI to intensive chemotherapy resulting in outcomes similar to consolidative HSCT.206^,^207 Additionally, CA180-372/COG AALL1122 showed that dasatinib plus EsPhALL chemotherapy is effective for pediatric Ph+ ALL,208 and a retrospective study from the Japan Children’s Cancer Group suggested that ponatinib was safe and effective as well.209 However, when it comes to post-HSCT maintenance, there is a lack of pediatric-specific data, and usage is largely extrapolated from data in adults.
The use of sensitive molecular testing such as low-density microarray and reverse-transcription polymerase chain reaction (RT-PCR) has led to the increased recognition of B-ALL subtypes harboring kinase-activating mutations that result in a gene expression profile similar to Ph+ ALL but without the canonical BCR-ABL fusion protein.210 This “Ph-like” ALL may also be targetable with TKIs (as with ABL-class fusions) or other molecularly targeted therapies such as JAK inhibition. While these agents are increasingly used in the upfront or relapsed setting, only isolated case reports have been published on their use post HSCT,211^,^212 although unpublished experience is growing across a number of centers.
Blinatumomab
Blinatumomab is a bispecific T cell engager that targets CD19 and CD3 and works to engage and activate cytotoxic T cells and bridge them with CD19^+^ B cells to promote tumor killing. The efficacy of blinatumomab for both relapsed213^,^214 B-ALL and upfront management215^,^216 is well documented, and its inclusion in upfront chemotherapy regimens is becoming standard. In pediatrics, a recent study also suggested that post-HSCT outcomes are improved when blinatumomab is used as pre-HSCT remission consolidation as opposed to chemotherapy.217 In the post-HSCT relapse setting, there is evidence that blinatumomab can lead to meaningful responses through restoration of GvL in adult patients without apparent increase in GvHD risk.218^,^219 Combination with DLI may hold potential to enhance this further; however, evidence to date is limited and inconclusive.220^,^221
Regarding its use as prophylaxis for MRD-negative remission post-HSCT, several recent studies have suggested tolerability and efficacy in high-risk patients across a variety of dosing regimens.222^,^223 Two of these studies additionally demonstrated that those who were T cell deficient or had lower peripheral blood CD8:CD4 ratios and upregulation of inhibitory checkpoint molecules were associated with poorer response,224^,^225 suggesting that strategies to address these may enhance efficacy. While rates of GvHD were acceptable in these studies, care would need to be taken if considering addition of therapies such as checkpoint inhibitors given the risk of promoting T cell alloreactivity.
Huang et al. recently retrospectively reviewed their experience using prophylactic blinatumomab as post-HSCT maintenance in 21 patients, 6 of whom were under the age of 20.226 Blinatumomab was tolerable, with grade 1–2 GvHD occurring in 28.6% and grade 3–4 occurring in 4.8%. Five patients developed chronic GvHD. Relapse rate was only 6.4%, and 1-year OS, EFS, and GvHD/relapse-free survival (GRFS) were 81.6%, 82.1%, and 82.5%. Review of the data reveals that of the 6 patients <20 years of age, 1 with pre-HSCT MRD positivity relapsed and died while the others appeared to have remained in remission. Sakaguchi et al. are conducting a multi-center phase 1/2 study evaluating the use of blinatumomab as post-HSCT maintenance in children and young adults,227 which should help to clarify its role in the pediatric population.
As CD19-targeted therapies become more incorporated into the upfront and relapsed settings, both with increasing usage of blinatumomab and CD19 CAR T cells, it remains to be seen how this would impact the efficacy of further CD19 targeting post-HSCT, and consideration of additional antigenic targets may be necessary.
Inotuzumab
Little data are available on the application of the CD22-targeting antibody-drug conjugate inotuzumab ozogamicin for post-HSCT prophylaxis, and the association of inotuzumab with SOS may hamper enthusiasm for its use. However, a recent phase 1 study reported a tolerable safety profile for inotuzumab as maintenance with no episodes of SOS in a dose-escalation model across 18 patients.228 While an advantage of inotuzumab over blinatumomab may be that the latter requires endogenous cytotoxic T cells for efficacy (which may be rare or poorly functional in a post-HSCT reconstituting immune system) while the former does not, more data are needed to inform the safety and efficacy of inotuzumab in this setting.
Cellular therapy
The efficacy of autologous CD19 CAR T cells for relapsed/refractory B-ALL, including post-HSCT relapse,229^,^230 lends credence to the idea that they could be employed post-HSCT as a relapse prevention strategy. Allogeneic manufacturing platforms open the window for donor-derived infusions, although GvHD needs to be considered with this approach.231^,^232^,^233 Lu et al. treated 23 patients with what was termed prophylactic donor-derived CAR T cell infusion after HSCT, although 7 patients had active MRD.234 Notably, the infusions were tolerable with no severe cytokine release syndrome (CRS) or immune effector cell-associated neurotoxicity syndrome (ICANS), and only 3 patients developed acute GvHD, although hematotoxicity was prevalent. The 2-year incidence of relapse was 5.6%, compared to 28.8% in a contemporary control cohort. While further work is needed, these results are encouraging.
A plethora of additional targets for relapse prophylaxis, both for B and T cell ALL, could be envisioned, including but not limited to CD22,235^,^236 CD7,237^,^238 and CD38.239 Additionally, donor-derived leukemia-specific T cells targeting multiple antigens (PRAME, WT1, and survivin) may be a promising maintenance strategy after HSCT,240 while other TCR-, TCRγδ+-, or NK-based therapies remain to be explored.
T cell ALL
While less common than B-ALL, T-ALL also carries a high risk of relapse post-HSCT, and thus effective maintenance strategies are an area of unmet need. Although data are less robust, likely related to smaller patient numbers, several strategies deserve mention.
As in AML, hypomethylating agents have been studied as post-HSCT maintenance for patients with ALL. Two Chinese studies in adult patients suggested that decitabine after HSCT may provide benefit in reducing incidence of relapse, particularly in patients with T-ALL.241^,^242 The larger of the two studies reported a 3-year incidence of relapse of 19.6% vs. 36.1% in those who received decitabine vs. controls and was even lower in those with T-ALL who received decitabine (11.7%). BCL-2 inhibition may be another avenue for relapse prophylaxis in T-ALL, as BCL-2 is highly expressed in early T cell precursors and T-ALL cell lines do display sensitivity to BCL-2 inhibition.243 Hassan et al. described the prophylactic treatment of 4 T-ALL patients with post-HSCT venetoclax/azacitidine and noted that all four maintained remission with a median follow-up time of 15 months.244
Data on other strategies specifically for T-ALL are lacking, however. Nelarabine, which has been shown to improve upfront survival in pediatric patients with T-ALL,245 has also shown efficacy as salvage in the post-HSCT setting246 but has not been reported as a maintenance strategy. Bortezomib has also demonstrated efficacy in the upfront and relapse setting,247^,^248 and CD38 targeting with daratumumab has been investigated for relapsed/refractory disease as well.249^,^250 Data on post-HSCT use are currently absent; however, an ongoing clinical trial (NCT04972942) is investigating the use of daratumumab as post-HSCT maintenance in children and young adults with high-risk T cell leukemia and lymphoma. While CAR T cells for T-ALL may be complicated by fratricide and a risk of long-standing T cell lymphopenia, innovative engineering approaches have opened the door for targeting T lineage antigens, such as CD7.251 Donor-derived allogeneic approaches for relapse prevention should be subjects of future research.
Impact on post-HSCT immune reconstitution
Regardless of the post-HSCT intervention employed, careful consideration of the potential impacts on immune reconstitution is crucial. DLI can lead to the conversion of mixed donor chimerism to full chimerism and improve T cell reconstitution252^,^253 but may also drive increased alloreactivity and GvHD, especially at higher doses and when given earlier post HSCT,254 which may distort immune recovery. Prophylactic NK cell infusions have expectedly been associated with improved NK cell reconstitution255^,^256^,^257 and may specifically be advantageous in the context of post-transplant cyclophosphamide, which can ablate proliferating and alloreactive NK cell populations.258^,^259
Agents with myelosuppressive properties may conceivably lead to delays in immune reconstitution through suppression of hematopoiesis, and dosage holds and reductions are commonly needed to address hematotoxicity. However, to our knowledge, systematic evaluation of the impact of more commonly used agents such as hypomethylating agents, FLT3 inhibitors, and TKIs on immune recovery is not available. Similarly, how agents such as inotuzumab and blinatumomab impact immune reconstitution beyond inducing cytopenias is not well described, although in the case of blinatumomab, it has been shown that efficacy post HSCT may be constrained by the recovering T cell repertoire.224
Understanding of the impact of post-HSCT maintenance strategies on immune recovery would provide deeper mechanistic insights into effects on GvL and toxicity as well as shed light on potential concerns regarding post-HSCT infections and revaccination. As such, further study in this area is much needed.
Conclusions and future directions
The curative potential of allogeneic HSCT for children and adolescents with acute leukemias continues to be limited by relapse. The use of post-HSCT maintenance has made strides in promoting durable remissions in patients with “druggable” targets, such as FLT3-mutated AML or Ph+ ALL. However, this still leaves most patients without evidence-based options for post-HSCT remission prophylaxis. A select list of active clinical trials is shown in Table 1. Approaches to enhance GvL, such as WIS ± DLI, have generated only modest efficacy at best and can be limited by the development of GvHD. Allogeneic cellular therapy approaches, such as CAR T cells or NK cells, are promising, but the current focus for these and many other therapies is on salvage potential for patients with active disease as opposed to relapse prevention. Additionally, even for interventions that have shown efficacy in adults, data in pediatrics specifically can be quite hard to come by, a problem often faced by pediatric hematologists/oncologists when providing evidence-based counseling to families. While extrapolating from data in adult patients may provide insight, it is not clear that this is always appropriate, and trials specifically targeted at the pediatric and adolescent population are needed.Table 1. Select clinical trials for post-HSCT maintenance currently recruitingClinicalTrials.gov IDStudy nameDiseaseAgeSponsorNCT06158828Pilot Study of Memory-like Natural Killer (ML NK) Cells After TCRαβ T cell Depleted Haploidentical Transplant in AML (ABCD-NK)AML<30 yearsWashington University School of MedicineNCT05686538Innate Donor Effector Allogeneic Lymphocyte Infusion After Stem Cell Transplantation: the IDEAL Trial (IDEAL)AML, MDS≥18 yearsRigshospitalet, DenmarkNCT06765915Avapritinib Maintenance for AML With KIT MutationsAML≥14 yearsRuijin HospitalNCT03286530Ruxolitinib + Allogeneic Stem Cell Transplantation in AMLAML60–80 yearsMassachusetts General HospitalNCT05858814RC1012 Injection (Allo-DNT Cells) for the Prevention of Relapse in AML Patients After Allo-HSCTAML18–70 yearsGuangdong Ruishun Biotech Co., Ltd.NCT06707493Ivosidenib as Post-HSCT Maintenance for AMLAML18–75 yearsMassachusetts General HospitalNCT06754540Azacitidine Combined with Donor Lymphocyte Infusion for Acute Myeloid Leukemia Post-transplant Relapse PreventionAML18–70 yearsShanghai General Hospital, Shanghai Jiao Tong University School of MedicineNCT06765928Selinexor Combined With Venetoclax Maintenance Therapy After Allo-HSCTAML18–75 yearsRuijin HospitalNCT05768035Safety and Efficacy of SMART101 in Adult Patients With Hematological Malignancies After Haploidentical HSCT With Post-transplant CyclophosphamideAML, ALL, MDS≥18 yearsSmart Immune SASNCT06783478NK Cell Infusion for Remission Consolidation in AML: A Phase II Trial (NKLMA)AML18–75 yearsHospital de Clinicas de Porto AlegreNCT06717958Prospective Evaluation of Ivosidenib Maintenance Following Allogeneic Stem Cell Transplantation in Patients With Acute Myeloid Leukemia or High-risk Myelodysplastic Neoplasia With IDH1 (Isocitrate Dehydrogenase 1) Mutation (PIVOT)AML, MDS18–75 yearsTechnische Universität DresdenNCT06704152BSB-1001 in Patients Undergoing HLA-Matched Allogenic Hematopoietic Stem Cell Transplant for AML, ALL or MDSAML, ALL, MDS18–70 yearsBlueSphere Bio, Inc.NCT05528354Venetoclax and Decitabine Based Conditioning Regimen Followed With Post-HSCT Decitabine Maintenance Therapy in TP53 Mutant AML/MDS PatientsAML, MDS12–70 yearsZhejiang UniversityNCT06598384VA as Maintenance Therapy Post Allo-HSCT in MDS and AMLAML, MDS≥18 yearsNavy General Hospital, BeijingNCT03300492Expanded Natural Killer Cells Following Haploidentical HSCT for AML/MDSAML, MDS≥18 yearsUniversity Hospital, Basel, SwitzerlandNCT05796570A Pilot Study to Evaluate the Feasibility of Post-Hematopoietic Stem Cell Transplant Prophylaxis with Decitabine Combined with Filgrastim for Children and Young Adults with AML, MDS and Related Myeloid Malignancies (MORE)AML, MDS1–39 yearsFranziska WachterNCT03597321Early Prophylactic Donor Lymphocyte Infusion After Allo-HSCT for Patients With AML (ELIT-AML01)AML18–70 yearsInstitut Paoli-CalmettesNCT06441084A Trial to Evaluate the Safety and Efficacy of NCR300 in Preventing Recurrence of Acute Myeloid Leukemia (AML) After TransplantationAML18–65 yearsNuwacell Biotechnologies Co., Ltd.NCT02494167Administration of Donor Multi TAA-Specific T Cells for AML or MDS (ADSPAM)AML, MDSchild, adultBaylor College of MedicineNCT04849910Allogeneic Engineered Hematopoietic Stem Cell Transplant (HCT) Lacking the CD33 Protein, and Post-HCT Treatment With Mylotarg, for Patients With CD33+ AML or MDSAML, MDS18–70 yearsVor BiopharmaNCT04128501Venetoclax and Azacitidine for the Treatment of Acute Myeloid Leukemia in the Post-Transplant SettingAML, ALL18–75 yearsM.D. Anderson Cancer CenterNCT06543381Olutasidenib for the Treatment of Patients with IDH1 Mutated AML, MDS or CMML After Donor Hematopoietic Cell TransplantAML, MDS, CML≥18 yearsCity of Hope Medical CenterNCT05945849CD33KO-HSPC Infusion Followed by CART-33 Infusion(s) for Refractory/Relapsed AML (CART33)AML≥18 yearsUniversity of PennsylvaniaNCT05233618Study of Tagraxofusp for Post-Transplant Maintenance for Patients With CD 123+ AML, MF and CMML (HSCT 002)AML, CML, MF18–75 yearsKaren Ballen, MDNCT05682755Chidamide Prevents Recurrence of High-risk AML After Allo-HSCTAML18–65 yearsSichuan UniversityNCT06158100Venetoclax in Combination With Azacitidine (VEN/AZA) Followed by Donor Lymphocyte Infusion (DLI) for Patients With Very High-Risk Acute Myeloid Leukemia (AML) Undergoing Allogeneic Hematopoietic Cell Transplant (HCT)AML18–75 yearsAntonio M Jimenez JimenezNCT06138587Preemptive CIML NK Cell Therapy After Hematopoietic Stem Cell TransplantationAML≥18 yearsDana-Farber Cancer InstituteNCT06129734Decitabine and Venetoclax Treatment as Maintenance Therapy in Patients Post Allograft Stem Cell TransplantAML, MDS≥18 yearsBenjamin TomlinsonNCT03533816Expanded/Activated Gamma Delta T cell Infusion Following Hematopoietic Stem Cell Transplantation and Post-transplant CyclophosphamideAML, ALL, MDS, CML19–65 yearsUniversity of Kansas Medical CenterNCT06498973Tagraxofusp and Azacitidine for Maintenance Treatment in Patients With CD123 Positive AML and MDS Following Donor Hematopoietic Cell TransplantAML, MDS18–75 yearsCity of Hope Medical CenterNCT06575296Revumenib for the Treatment of Acute Leukemia in Patients Post-Allogeneic Stem Cell TransplantAML≥2 yearsCity of Hope Medical CenterNCT03728335Enasidenib as Maintenance Therapy in Treating Patients With Acute Myeloid Leukemia With IDH2 Mutation After Donor Stem Cell TransplantAML≥18 yearsCity of Hope Medical CenterNCT06532084Sorafenib Relapse Prophylaxis After HCT With PTBCy Regimen (SoraGVL)AML, MDS18–75 yearsSt. Petersburg State Pavlov Medical UniversityNCT06440135Ziftomenib Maintenance Post Allo-HCTAML≥18 yearsMassachusetts General HospitalNCT04764513Safety and Efficiency of γδ T cell Against Hematological Malignancies After Allo-HSCTAML, ALL18–65 yearsChinese PLA General HospitalNCT03843528Vorinostat Dose-escalation After Allogeneic Hematopoietic Cell TransplantationAML, MDS, JMML1–21 yearsJohns Hopkins All Children’s HospitalNCT02782546Cytokine Induced Memory-like NK Cell Adoptive Therapy After Haploidentical Donor Hematopoietic Cell TransplantationAML≥18 yearsWashington University School of MedicineNCT03856216Inotuzumab Ozogamicin and Chemotherapy in Treating Patients With Leukemia or Lymphoma Undergoing Stem Cell TransplantationALL, lymphoma12–70 yearsM.D. Anderson Cancer CenterNCT06735690Allogeneic CMV-Specific CD19-CAR T Cells Plus CMV-MVA Triplex Vaccine After Matched Related Donor Hematopoietic Cell Transplant for the Treatment of Patients With High-Risk Acute Lymphoblastic LeukemiaALL≥18 yearsCity of Hope Medical CenterNCT06438796Blinatumomab Maintenance After Allo-HSCTALL16–65 yearsRuijin HospitalNCT05991973Low-dose Chidamide Maintenance Therapy After Allo-HSCT for T cell Acute Lymphoblastic Leukemia or T cell LymphomasT-ALL/LL14–70 yearsZhejiang UniversityNCT06686108Demethylating Agents Combined with Venetoclax for High-risk T cell Lymphoma/Leukemia Post-Transplant Relapse PreventionT-ALL/LL14–55 yearsShanghai General Hospital, Shanghai Jiao Tong University School of MedicineNCT06393985Decitabine, Venetoclax and Blinatumomab for Maintenance Following HSCT in Patients With Ph-Negative B-ALLALL18–65 yearsThe First Affiliated Hospital of Soochow UniversityNCT06658938Blinatumomab as Maintenance Therapy in Patients With High-risk B-lineage Acute Lymphoblastic Leukemia Post Allogeneic Hematopoietic Cell TransplantationALL≥14 yearsInstitute of Hematology & Blood Diseases Hospital, ChinaNCT06658925Olverembatinib as Maintenance Therapy or Preemptive Therapy After Allo-HSCT in Ph+ALLALL≥18 yearsInstitute of Hematology & Blood Diseases Hospital, ChinaNCT03622788Cytokine-Treated Veto Cells in Treating Patients With Hematologic Malignancies Following Stem Cell Transplantany heme malignancy12–75 yearsM.D. Anderson Cancer CenterNCT06075238Blinatumomab Prevents Recurrence of R/R ALL After Allo-HSCTALL16–65 yearsSichuan UniversityNCT04972942Targeted Immunotherapy After Myeloablative TBI-Based Conditioning & AlloHCT in CAYA With High Risk T cell ALL & Lymphoma (ALLO-T-DART)T-ALL≤39 yearsNew York Medical CollegeNCT04746209Blinatumomab After TCR Alpha Beta/CD19 Depleted HCTALL≤25 yearsMedical College of Wisconsin
In addition to the “what” of post-HSCT maintenance, questions still abound as to “who” ought to receive additional therapy and “how” this therapy should be administered (i.e., timing of initiation and duration of therapy) to appropriately balance the potential benefits of better disease control with toxicity concerns and impacts on immune reconstitution. Challenges will remain, including a lack of consensus regarding the duration of maintenance for many of the agents discussed as well as considering if and how different post-HSCT agents may affect decisions about the HSCT platform, such as conditioning regimen and graft selection. Additionally, as the field evolves to incorporate more targeted therapies in the upfront and relapsed settings, issues of antigen downregulation or escape will continue to necessitate a personalized approach. While much work is still to be done, recent advances in molecular and cellular-/immunotherapies provide hope that HSCT along with thoughtful maintenance therapy can one day be a means toward durable cure for all children and young adults with acute leukemias.
Acknowledgments
The authors thank all of the investigators who have committed time and effort to performing the studies that comprise this review. The figures were generated using BioRender (https://biorender.com).
Author contributions
A.W.R. developed the outline for the manuscript, performed the literature review, and wrote the first draft of the manuscript. A.K.K., R.F.A.-A., and M.S.T. reviewed and edited the manuscript. H.G.R. supervised the writing of the manuscript and reviewed the final version.
Declaration of interests
The authors declare no competing interests.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1SEER∗Explorer An interactive website for SEER cancer statistics [Internet]https://seer.cancer.gov/statistics-network/explorer/2025
- 2Möricke A.Zimmermann M.Valsecchi M.G.Stanulla M.Biondi A.Mann G.Locatelli F.Cazzaniga G.Niggli F.AricòM.Dexamethasone vs prednisone in induction treatment of pediatric ALL: results of the randomized trial AIEOP-BFM ALL 2000 Blood 12720162101211210.1182/blood-2015-09-67072926888258 · doi ↗ · pubmed ↗
- 3Vora A.Goulden N.Wade R.Mitchell C.Hancock J.Hough R.Rowntree C.Richards S.Treatment reduction for children and young adults with low-risk acute lymphoblastic leukaemia defined by minimal residual disease (UKALL 2003): a randomised controlled trial Lancet Oncol.14201319920910.1016/s 1470-2045(12)70600-923395119 · doi ↗ · pubmed ↗
- 4Place A.E.Stevenson K.E.Vrooman L.M.Harris M.H.Hunt S.K.O'Brien J.E.Supko J.G.Asselin B.L.Athale U.H.Clavell L.A.Intravenous pegylated asparaginase versus intramuscular native Escherichia coli L-asparaginase in newly diagnosed childhood acute lymphoblastic leukaemia (DFCI 05-001): a randomised, open-label phase 3 trial Lancet Oncol.1620151677169010.1016/s 1470-2045(15)00363-026549586 · doi ↗ · pubmed ↗
- 5Pieters R.de Groot-Kruseman H.Van der Velden V.Fiocco M.van den Berg H.de Bont E.Egeler R.M.Hoogerbrugge P.Kaspers G.Van der Schoot E.Successful Therapy Reduction and Intensification for Childhood Acute Lymphoblastic Leukemia Based on Minimal Residual Disease Monitoring: Study ALL 10 From the Dutch Childhood Oncology Group J. Clin. Oncol.3420162591260110.1200/jco.2015.64.636427269950 · doi ↗ · pubmed ↗
- 6Salzer W.L.Burke M.J.Devidas M.Dai Y.Hardy K.K.Kairalla J.A.Gore L.Hilden J.M.Larsen E.Rabin K.R.Impact of Intrathecal Triple Therapy Versus Intrathecal Methotrexate on Disease-Free Survival for High-Risk B-Lymphoblastic Leukemia: Children's Oncology Group Study AALL 1131 J. Clin. Oncol.3820202628263810.1200/jco.19.0289232496902 PMC 7402996 · doi ↗ · pubmed ↗
- 7Angiolillo A.L.Schore R.J.Kairalla J.A.Devidas M.Rabin K.R.Zweidler-Mc Kay P.Borowitz M.J.Wood B.Carroll A.J.Heerema N.A.Excellent Outcomes With Reduced Frequency of Vincristine and Dexamethasone Pulses in Standard-Risk B-Lymphoblastic Leukemia: Results From Children's Oncology Group AALL 0932 J. Clin. Oncol.3920211437144710.1200/jco.20.0049433411585 PMC 8274746 · doi ↗ · pubmed ↗
- 8Lange B.J.Smith F.O.Feusner J.Barnard D.R.Dinndorf P.Feig S.Heerema N.A.Arndt C.Arceci R.J.Seibel N.Outcomes in CCG-2961, a children's oncology group phase 3 trial for untreated pediatric acute myeloid leukemia: a report from the children's oncology group Blood 11120081044105310.1182/blood-2007-04-08429318000167 PMC 2214754 · doi ↗ · pubmed ↗