Stone-Dominant Renal Phenotype Without Nephrocalcinosis in FAM20A-Related Enamel Renal Syndrome
Neriman Sıla Koç

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
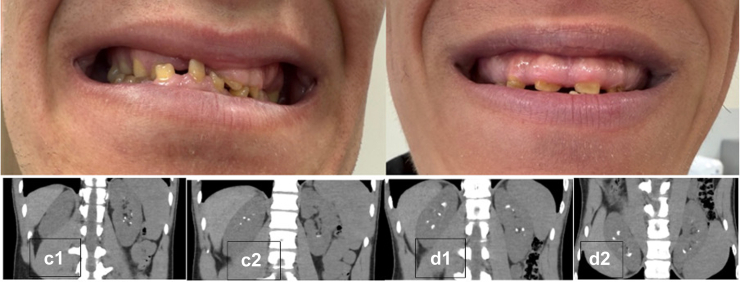 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsKidney Stones and Urolithiasis Treatments · Parathyroid Disorders and Treatments · Bone and Dental Protein Studies
To the Editor:
I read with great interest the article by Cogal et al.,1 in which the authors convincingly demonstrate that monogenic urinary stone disease is characterized by substantial genetic and phenotypic heterogeneity and that reliance on clinical or biochemical features alone may result in missed or delayed diagnoses. Their findings strongly support the use of broad targeted genetic screening in patients suspected of monogenic urinary stone disease or nephrocalcinosis.
I would like to extend this concept of phenotypic heterogeneity by describing a stone-dominant renal phenotype without nephrocalcinosis in patients with FAM20A-related enamel renal syndrome**,** a disorder classically associated with diffuse medullary nephrocalcinosis.
Enamel renal syndrome, caused by biallelic FAM20A mutations, is classically characterized by amelogenesis imperfecta and renal calcifications.2 From a nephrological standpoint, nephrocalcinosis has been considered the hallmark renal manifestation and has been reported in nearly all affected individuals in the largest cohorts.3 Nephrolithiasis, when described, usually coexists with medullary nephrocalcinosis rather than representing a dominant feature.2^,^4
In contrast, I evaluated 2 adult brothers with genetically confirmed enamel renal syndrome who presented with recurrent calcium-based nephrolithiasis in the absence of radiological nephrocalcinosis. Both patients had characteristic dental findings consistent with amelogenesis imperfecta (Figure 1). Genetic testing identified a homozygous pathogenic copy number deletion involving exon 4 of FAM20A (**NM_017565). Noncontrast abdominal computed tomography demonstrated multiple discrete calculi localized to the renal calyces, without diffuse or symmetric medullary calcification (Figure 1).Figure 1(a and b) Dental photographs demonstrating generalized enamel hypoplasia consistent with amelogenesis imperfecta in both siblings. (c_1-c_2, d_1_, and d_2_) Noncontrast abdominal computed tomography images showing bilateral renal calculi in both cases, with preserved renal parenchyma and absence of cortical or medullary nephrocalcinosis.
Metabolic evaluation showed hypocalciuria and marked hypocitraturia in both patients, with normal urinary oxalate and phosphate excretion. Serum calcium and phosphate levels were within reference ranges, and distal renal tubular acidosis was excluded (Supplementary Table S1). This biochemical profile suggests that impaired urinary crystal inhibition, rather than increased calcium load, may represent a key mechanism underlying stone formation in FAM20A-related disease.
Consistent with the observations of Cogal et al.,1 these findings illustrate that monogenic urinary stone disease represents a continuum of renal phenotypes. I propose that stone-dominant enamel renal syndrome without nephrocalcinosis constitutes an expanded renal phenotype, emphasizing that the absence of classical imaging features should not preclude consideration of monogenic disease. Moreover, my observations suggest that nephrolithiasis without nephrocalcinosis may represent an alternative or early renal manifestation of FAM20A-related disease, underscoring the importance of systematic renal imaging and metabolic evaluation in patients with enamel renal disorders, even in the absence of overt renal symptoms.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Cogal A.G.Arroyo J.Shah R.J.Comprehensive genetic analysis reveals complexity of monogenic urinary stone disease Kidney Int Rep 620212862288410.1016/j.ekir.2021.08.03334805638 PMC 8589729 · doi ↗ · pubmed ↗
- 2Jaureguiberry G.De la Dure-Molla M.Parry D.Nephrocalcinosis (enamel renal syndrome) caused by autosomal recessive FAM 20A mutations Nephron Physiol 12220131610.1159/000349989 PMC 378219423434854 · doi ↗ · pubmed ↗
- 3Roomaney I.A.Kabbashi S.Chetty M.The craniofacial, dental and systemic manifestations of Enamel Renal Syndrome: a Scoping review Eur J Med Genet 75202510500810.1016/j.ejmg.2025.10500840089179 · doi ↗ · pubmed ↗
- 4Koruyucu M.Seymen F.Gencay G.Nephrocalcinosis in amelogenesis imperfecta caused by the FAM 20A mutation Nephron 139201818919610.1159/00048660729439260 · doi ↗ · pubmed ↗