Esophageal erosion by a PDA occluder device following MAPC closure in tetralogy of Fallot
Munaf J Yaseen, Wassan N Mohammed, Nabeeha N Akram, Mohanad K Shukur Al-Ghanimi

TL;DR
A young boy developed esophageal erosion after a device used to close a heart defect became lodged in his esophagus.
Contribution
Reports a rare case of esophageal erosion caused by a PDA occluder device following MAPC closure in TOF.
Findings
A PDA occluder device impacted in the esophagus caused dysphagia in a TOF patient.
The device was surgically removed, and the patient recovered well post-procedure.
This case highlights a previously unreported complication of transcatheter closure in TOF.
Abstract
Tetralogy of Fallot (TOF) is the commonest cyanotic congenital heart disease encountered in paediatrics. Major aortopulmonary collaterals (MAPCAs) often complicate TOF when surgical correction is delayed, and a transcatheter closure is commonly done prior to definitive surgery. Embolization of occluding devices is a known complication that typically occurs in the vessels or in cardiac chambers. We report a young boy who presented with 1-month dysphagia post-transcatheter closure of a large MAPCAs. Barium revealed a filling defect confirmed by endoscopy as an impacted occluding device in the oesophagus. It was surgically removed, and the boy was discharged well. This case highlights a rare but highly significant unreported complication.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
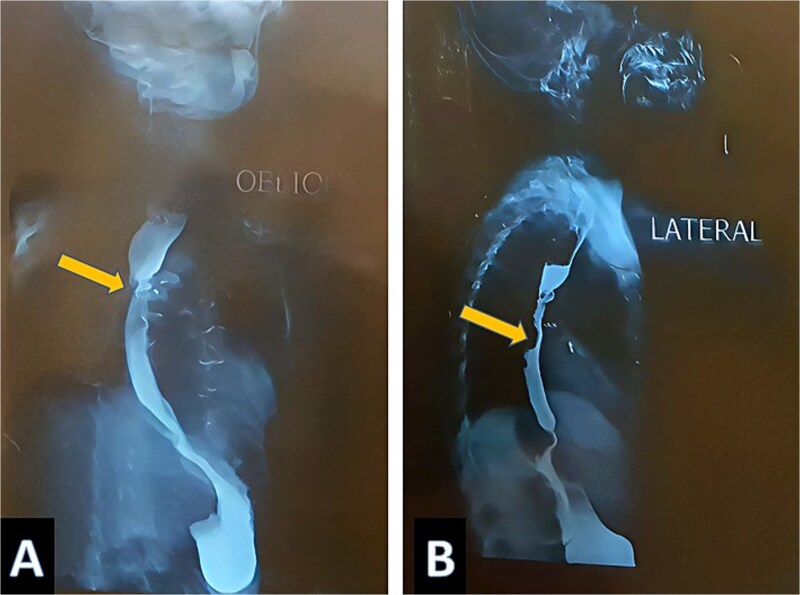 Figure 1
Figure 1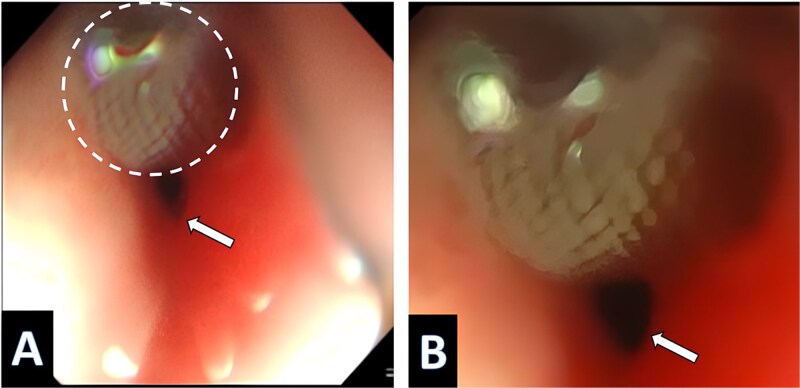 Figure 2
Figure 2| Authors Year | Age, sex | Type of occluder | Underlying Defect | Presenting symptom | Retrieval | Outcome/complication |
|---|---|---|---|---|---|---|
| Wiegand G et al. (2016) [ | 4.5 months, Female | Amplatzer vascular plug 4 occluder | AP shunt | severe gastrointestinal bleeding | Right lateral thoracotomy, the occluder was extracted surgically, the oesophageal injury sutured. | Uneventful, none |
| González et al. (2020) [ | 16 years male | ADO | scimitar syndrome with 2 large AP collaterals | Progressive dysphasia | endoscopic removal of the device with stent placement in the oesophagus | The esophageal stent was removed at 3 weeks, with no residual esophageal stenosis |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCongenital Heart Disease Studies · Aortic Disease and Treatment Approaches · Tracheal and airway disorders
Introduction
Major aortopulmonary collaterals (MAPCAs) often complicate Tetralogy of Fallot (TOF), which is one of the most common congenital cyanotic heart diseases that affects the paediatric age group [1]. MAPCAs tend to rise among cases when surgical repair is delayed. Aiming to reduce shunt and to improve postoperative complications, these MAPCs are usually closed transcatheter via coil or ductal occluder, which is considered the gold standard method [1]. Although coils can be effective in small PDAs, they are associated with a higher risk of embolization, particularly in moderate to large ducts. This limitation has led to the increased use of Amplatzer Duct Occluder (ADO) devices including: Amplatzer ductal occluder type 1(ADO1) and Amplatzer ductal occluder type 2 (ADO2), which provide more stable positioning and lower rates of residual shunting or device migration. Nevertheless, these occluders still carry risk of embolization into the pulmonary arteries, and the aorta [2]. Extracardiac erosion of these devices, particularly to the oesophagus, is exceptionally rare; we present a rare case of oesophageal erosion by a PDA occluder following a MAPCAs closure that was successfully retrieved by surgery with a favourable outcome.
Case report
A three-year-old Iraqi boy with TOF diagnosed since birth, residing between Iraq and Turkey, was prepared for total surgical correction. As a preparatory step, a transcatheter study was conducted in Istanbul. The results showed three significant MAPCAs, two of them were embolized with 7 × 5 mm coils, while the largest one was occluded using an 8–6 mm PDA device in a smooth, uneventful surgery. One month after the surgery, the boy presented in Baghdad with progressive dysphagia for solid food with weight reduction from 11 kg (on the 5^th^ centile for age) to 10.2 kg (below the 5^th^ centile for age). Physical examination and lab tests were unremarkable, which led to a gastroesophageal regurgitation as a possible underlying cause. Imaging study: Bairam Meal revealed a mid-oesophageal filling with no mediastinum leakage, without suggestion of a filling defect nature, (Fig. 1A and B). Endoscopic examination of the oesophagus shows a PDA device protruding and impacting the upper part of the oesophagus, (Fig. 2A and B). This implies that the PDA occluder had eroded the collateral vessels into the oesophagus lumen to manifest as dysphagia. The case was referred to a cardiothoracic surgeon, where surgical retrieval was performed by open thoracotomy. The device was removed successfully without injury to the surrounding structures, the oesophagus was sutured but without residual defect and no stent was placed, and the postoperative course was uneventful.
Barium meal shows a filling defect marked by yellow arrow.
The endoscope picture shows the PDA device inside the oesophagus. Magnification by X20; (B) magnification by X40.
The operation and postoperative period went smoothly without complications, and the boy was discharged home three days later. There was complete resolution of dysphagia at follow-up visits with 1-week.
Discussion
All cyanotic congenital heart diseases, including TOF, may develop MAPCAs when surgical repair is delayed. The MAPCAs proliferate and inversely impact pulmonary vascular development, uneven pulmonary perfusion, and increase right ventricular workload, thus imposing long-term outcomes [1, 3]. Selective Transcatheter closure of these abnormal vessels can decrease the hemodynamic burden on the heart and improve preoperative haemodynamic and postoperative recovery after total surgical correction. It is worth noting that this patient’s procedure was performed at a different institution to where the complication was identified; at our institution practice consists of choosing the smallest effective closure device, placing the device as distally as possible to avoid erosion risks to adjacent structures (such as the oesophagus) and never using a device larger than the ADO1 5-4 mm. [4].
These vascular occluders do have complications such as vascular injury, erosion, and migration. Migration of PDA occluder device is known complication, it can be early within hours- days (1%–3%) or late (<0.03%) years after their placement [5, 6]. Common sites for device migration reported in the literature are the descending thoracic aorta and the pulmonary vasculature [4]. However, device migration to oesophagus is very rarely reported and usually presented with upper gastrointestinal bleeding or dysphagia. Furthermore, the diagnosis is confirmed by Echo, fluoroscopy, or CT scan when the patient presents with unexplained decompensation or compromise [7]. The retrieval is either by percutaneous snare by Cath-based technique, or it is done by open surgery when the former method fails, with a good outcome even if device erosion was reported. We have summarized some of the reported cases in the last 5-years and the outcome.
The current case is unique in more than one aspect; device migration in TOF cases is rarely reported, and most of them occur during placement. The reported cases mention that the aorta and pulmonary vessels are the most common sites. To the best of our knowledge, there are only two previous reports of oesophageal erosion by PDA occluder after MAPCAs closure, which expands the spectrum of device-related complications in CHD, (Table 1).
There are many key points from this case. Device oversizing or proximal placing can cause migration and erosion to the adjacent mediastinal structure. The anatomical proximity of the oesophagus should be considered as a migration site, even though it has not previously been reported. The importance of close follow-up and clinical vigilance to CHD cases cannot be overestimated, and the appearance of unusual symptoms (such as dysphagia) should prompt investigation. Finally, imaging studies and endoscopy are important tools in unveiling the underlying cause and device migration site.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Edraki M, Naghshzan A, Amoozgar H. et al. Major Aortopulmonary collateral arteries and their effects on perioperative parameters and mortality of children with tetralogy of Fallot: a case-control study. Iran J Med Sci 2024;49:769–76. 10.30476/ijms.2024.100206.323739840301 PMC 11743443 · doi ↗ · pubmed ↗
- 2Karuru UD, Tummala SR, Naveen T. et al. Retrieval of patent ductus arteriosus device embolization using hybrid approach: a case report. Egypt Heart J 2024;76:160. 10.1186/s 43044-024-00595-y 39704986 PMC 11662123 · doi ↗ · pubmed ↗
- 3Al-Musawi M, Rubay D, Ohanisian L. et al. An unusual presentation of a cardiac foreign body in a Pediatric patient. Cureus. 2019;11:e 4829. 10.7759/cureus.482931404380 PMC 6682342 · doi ↗ · pubmed ↗
- 4Kouakou NYN, Song J, Huh J. et al. The experience of transcatheter closure of postoperative ventricular septal defect after total correction. J Cardiothorac Surg 2019;14.104 10.1186/s 13019-019-0933-8PMC 655891831186037 · doi ↗ · pubmed ↗
- 5Jaswal V, Singh Thingnam SK, Prasad Gourav K. et al. Delayed embolization of ductal occluder device into the aorta with near-complete obstruction of the aorta and critical cardiac decompensation. J Card Surg 2020;35:696–9. 10.1111/jocs.1443431971271 · doi ↗ · pubmed ↗
- 6Pan D, Yu A, Li C. et al. Delayed occluder displacement following patent ductus arteriosus closure successfully managed with thoracic endovascular aortic repair: a case report and literature review. J Cardiothorac Surg 2025;20:37. 10.1186/s 13019-024-03334-139762939 PMC 11705684 · doi ↗ · pubmed ↗
- 7Yaseen NJ, Akram NN, Nori W. Intravascular foreign bodies retrieval: navigating differences from childhood to adulthood. Scr Med 2025;56:69–76. 10.5937/scriptamed 56-53482 · doi ↗
- 8Wiegand G, Schlensak C, Hofbeck M. Esophageal perforation caused by an AMPLATZERTM vascular plug 4 occlusion device. Catheter Cardiovasc Interv 2016;88:E 113–6. 10.1002/ccd.2659527258845 · doi ↗ · pubmed ↗