Risk factors when considering heart transplants with donors aged 45 or above: Development of a Novel Mortality Risk Score using UNOS data
Anh Nguyen, Abbas Rana, Alexis Shafii, Gabriel Loor, Andrew Civitello, Todd Rosengart, Kenneth Liao

TL;DR
This study identifies risk factors for mortality in heart transplant recipients using donors aged 45 or older and creates a new risk score to help guide transplant decisions.
Contribution
A novel mortality risk score for heart transplants using donors aged ≥45, based on UNOS data.
Findings
1-, 5-, and 10-year survival rates were 87.0%, 73.3%, and 53.5% for transplants using donors aged ≥45.
Key risk factors included ischemic time ≥4 hours, CMV-positive donor status, and recipient factors like age >55 and diabetes.
The risk score model had moderate discrimination with a C-statistic of 0.58.
Abstract
Current International Society for Heart and Lung Transplantation guidelines support the use of donor hearts aged ≥45 if significant coronary artery disease is excluded and ischemic time remains <4 hours. This study aimed to identify additional risk factors affecting patient survival and develop a risk score for recipients of older donor hearts. We performed a retrospective cohort study of adult heart transplants using donors aged ≥45 from January 2000 to June 2024, using United Network for Organ Sharing data. Multivariable Cox regression identified risk factors for mortality, and the most significant variables were used to construct a risk score. Of 58,859 adult heart transplants, 9,843 (16.7%) involved donors aged ≥45. Recipient median age was 58 years (interquartile range, 51-64). One-, 5-, and 10-year patient survival rates were 87.0%, 73.3%, and 53.5%, respectively. Statistically…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
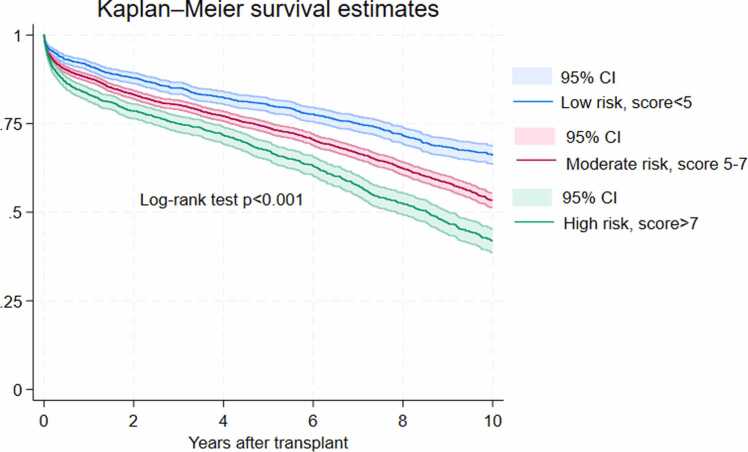 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTransplantation: Methods and Outcomes · Renal Transplantation Outcomes and Treatments · Organ Donation and Transplantation
Background
Heart failure continues to pose a significant global health challenge, affecting more than 64 million individuals worldwide and over 6.7 million adults annually in the United States.1 Heart transplantation remains the most effective therapy for patients with advanced heart failure, offering marked improvements in both survival and quality of life. However, the demand for donor hearts consistently surpasses the available supply.2 Alarmingly, more than 30% of patients on the transplant waiting list face mortality within 1 year if a suitable donor heart is not found.3 The use of extended donor criteria has included older donors in efforts to expand the donor pool. While some studies reported that older heart donors were associated with worse post-transplant survival,4, 5, 6, 7, 8, 9, 10 others showed that older donor hearts may achieve comparable perioperative outcomes and survival with careful selection.11, 12 The current International Society for Heart and Lung Transplantation (ISHLT) guidelines for donor heart selection stated that there was no established upper age limit and donors ≥45 years could be used after screening for significant coronary artery disease and short ischemic times could be expected.13 Our study aims to assess additional risk factors that may influence heart transplant patient survival with older donors and develop a corresponding mortality risk score to assist clinicians while considering heart donors aged ≥45 years.
Methods
Data source
It was a retrospective cohort study using data from the United Network for Organ Sharing Standard Transplant Analysis and Research dataset. We evaluated adult heart transplants with donors aged ≥45 years between January 2000 and June 2024. Donor information obtained from the database included age, gender, weight, body mass index, mechanism of death, hypertension, coronary artery disease, cigarette use, left ventricular ejection fraction, cytomegalovirus (CMV) status, and ischemic time. Recipient information obtained from the database included age, gender, ethnicity, weight, body mass index, diabetes, history of cardiac surgery, pretransplant dialysis, inotropic support, mechanical ventilation, extracorporeal membrane oxygenation (ECMO), or ventricular assist device (VAD), end listing status, and mortality. Transplant year was grouped into 5 transplant eras: 2000-2005, 2006-2010, 2011-2015, 2016-2020, and 2021-2024.
Statistical analysis
Donor and recipient characteristics were reported as frequencies and proportions for categorical variables and as median and interquartile range (IQR) for continuous variables. Multivariable Cox proportional hazards regression was used to identify risk factors associated with mortality. The model was adjusted for ischemic time, CMV mismatch, gender mismatch, donor/recipient weight ratio, donor hypertension, donor left ventricular ejection fraction, donor diabetes, donor cigarette and cocaine use, donor cause of death, recipient age, recipient gender, recipient race, recipient obesity, recipient pretransplant dialysis/cardiac surgery/mechanical ventilation/ECMO/VAD/IV inotropes, recipient end listing status, and transplant era. Statistically significant and clinically relevant variables were kept optimizing the model performance with C-statistics of 0.58. To develop a clinically friendly risk score, we ran a Cox regression model with the significant variables in addition to recipient ECMO and converted their beta-coefficients in the model to integer risk scores according to a well-established methodology.14 The total risk score of each patient was calculated based on these 9 risk factors and then classified as low (<25% percentile), moderate (25%-75% percentile), and high risk (>75% percentile). Kaplan-Meier graphs were used to present patient survival by these 3 risk categories and the log-rank test to compare overall survival. All tests were 2-tailed with an alpha level of 0.05. Analyses were performed on Stata version 18.0 (Stata Corp LLC, College Station, TX).
This study was approved with a waiver of patient consent and Health Insurance Portability and Accountability Act authorization by the Institutional Review Board for Human Subject Research for Baylor College of Medicine and Affiliated Hospitals (H-51123, approved on November 29, 2022).
Results
Donor and recipient characteristics
Of the 58,859 adult heart transplants performed during the study period, 9,843 (16.7%) involved donors aged 45 years or older. The median donor age was 49 years (IQR, 47-53). Gender mismatch between donor and recipient occurred in 27.8% of cases, and 11.9% of donors had a weight less than 80% of the recipients. A history of hypertension was present in 35.5% of donors. Most donors had preserved left ventricular function, with 99.1% exhibiting an ejection fraction >50%. Coronary artery stenosis >50% was observed in 9.8% of donors. Additionally, 6.8% of donors had a history of diabetes. Substance use was notable, with 32.3% reporting cigarette use and 17.5% reporting cocaine use. The most common causes of donor death were stroke (47.1%), head trauma (29.6%), and anoxia (21.0%), with other causes accounting for 2.3%. The median ischemic time was 3.3 hours (IQR, 2.5-3.9) and 2,499 transplants (25.4%) had ischemic time ≥4 hours. CMV serostatus combinations included donor(−)/recipient(−) in 16.0%, donor(−)/recipient(+) in 21.0%, donor(+)/recipient(+) in 38.9%, and donor(+)/recipient(−) in 24.1% of cases.
Recipients had a median age of 58 years (IQR, 51-64), and 26.7% were female. The majority were White (68.6%), followed by Black (19.5%), Hispanic (7.9%), Asian (3.0%), American Indian (0.2%), Pacific Islander (0.4%), and Multiracial (0.3%). Comorbid conditions included obesity in 29.1%, diabetes in 28.6%, and pretransplant dialysis in 4.8%. A history of pretransplant cardiac surgery was present in 39.6% of recipients, while 40.5% required inotropic support, 25.8% had a VAD, 2.3% were on mechanical ventilation, and 1.8% received ECMO. At the time of listing, 62.0% were status 1, followed by status 2 (22.9%), status 3 (5.7%), status 4 (6.8%), status 5 (0.4%), and status 6 (2.1%). Detailed recipient characteristics are presented in Table 1.Table 1. Baseline Characteristics of Donors Aged ≥45 Years and Their Heart RecipientsTable 1CharacteristicSummary StatisticDonorsAge (years), median (IQR)49 (47-53)Gender mismatch, N (%)2,736 (27.8)Donor/recipient weight <80%, N (%)1,167 (11.9)Hypertension, N (%)3,451 (35.5)Left ventricular ejection fraction >50%9,614 (99.1)Coronary artery stenosis >50%, N (%)65 (9.8)Ischemic time (hours), median (IQR)3.3 (2.5-3.9)CMV status, N (%) Donor (−)/recipient (−)1,471 (16.0) Donor (−)/recipient (+)1,940 (21.0) Donor (+)/recipient (+)3,582 (38.9) Donor (+)/recipient (−)2,223 (24.1)Diabetes665 (6.8)Cigarette use3,105 (32.3)Cocaine use1,588 (17.5)Cause of death Anoxia2,061 (21.0) Stroke4,637 (47.1) Head trauma2,908 (29.6) Others232 (2.3) RecipientsAge (years), median (IQR)58 (51-64)Female, N (%)2,625 (26.7)Ethnicity, N (%) White6,756 (68.6) Black1,914 (19.5) Hispanic778 (7.9) Asian298 (3.0) American Indian25 (0.2) Pacific Islander40 (0.4) Multiracial30 (0.3)Obesity, N (%)2,863 (29.1)Diabetes, N (%)2,796 (28.6)Pretransplant dialysis, N (%)461 (4.8)Pretransplant cardiac surgery, N (%)3,151 (39.6)Pretransplant mechanical ventilator, N (%)229 (2.3)Pretransplant ECMO, N (%)117 (1.8)Pretransplant inotropic support, N (%)3,989 (40.5)Pretransplant ventricular assist device, N (%)2,538 (25.8)End listing status, N (%) 16,105 (62.0) 22,259 (22.9) 3562 (5.7) 4667 (6.8) 539 (0.4) 6209 (2.1)Transplant era 2000-20052,162 (22.0) 2006-20101,714 (17.4) 2011-20151,920 (19.5) 2016-20202,254 (22.9) 2021-20241,793 (18.2)Abbreviations: CMV, cytomegalovirus; ECMO, extracorporeal membrane oxygenation; IQR, interquartile range.
Mortality predictors of heart transplants with donors aged ≥45 years
One-, 5-, and 10-year survival rates were 87.0% (95% confidence interval [CI] 86.3-87.7), 73.3% (95% CI 72.4-74.3), and 53.5% (95% CI 52.2-54.7), respectively.
Donor coronary artery stenosis >50% was associated with a nonstatistically significant risk of post-transplant mortality (hazard ratio [HR] = 1.35, 95% CI 0.98-1.86, p = 0.06). Due to the limited availability of angiographic data present in only 662 donors (6.7%), this variable was not included in the multivariable analysis.
In the multivariable Cox proportional hazards model evaluating heart transplant outcomes with donors aged ≥45 years, several donor and recipient factors were significantly associated with post-transplant survival. Among donor characteristics, ischemic time ≥4 hours was associated with increased mortality risk (HR = 1.12; 95% CI, 1.03-1.23; p = 0.011). CMV serostatus mismatch also influenced outcomes: compared to donor(−)/recipient(−) pairs, donor(+)/recipient(+) combinations were associated with higher mortality (HR = 1.8; 95% CI, 1.05-1.32; p = 0.007), as were donor(+)/recipient(−) pairs (HR = 1.14; 95% CI, 1.00-1.29; p = 0.044). Additionally, donor cigarette use was associated with a 10% increase in mortality risk (HR = 1.10; 95% CI, 1.01-1.19; p = 0.028).
Recipient characteristics showed stronger associations with post-transplant outcomes. Increasing age was a significant predictor of mortality, with recipients aged 56 to 65 (HR = 1.35; 95% CI, 1.19-1.53; p = < 0.001) and >65 years (HR = 1.61; 95% CI, 1.41-1.85; p < 0.001) having elevated risk compared to those ≤35 years. Black race (HR = 1.1; 95% CI, 1.10-1.4; p < 0.001), obesity (HR = 1.21; 95% CI, 1.1-1.32; p < 0.001), and diabetes (HR = 1.26; 95% CI, 1.17-1.38; p < 0.001) were also independently associated with worse survival. Pretransplant dialysis (HR = 1.46; 95% CI, 1.25-1.71; p < 0.001), cardiac surgery (HR = 1.26; 95% CI, 1.17-1.37; p < 0.001), and mechanical ventilator support (HR = 1.45; 95% CI, 1.09-1.93; p < 0.011) were significant risk factors. Other donor and recipient factors, including gender mismatch, donor hypertension, donor diabetes, donor cocaine use, donor cause of death, and use of inotropes, VADs, or ECMO, were not significantly associated with survival. The final model demonstrated moderate discriminatory ability, with a C-statistic of 0.58 (95% CI 0.57-0.60). Full details are presented in Table 2.Table 2. Multivariable Survival Analysis for Heart Transplants With Donors Aged ≥45 YearsTable 2Risk factorsHazard ratio [95% CI]p-valueDonorsIschemic time ≥4 hours1.12 [1.03-1.23]0.011CMV Donor (−)/recipient (−)Ref Donor (−)/recipient (+)1.07 [0.94-1.22]0.313 Donor (+)/recipient (+)1.18 [1.05-1.33]0.007 Donor (+)/recipient (−)1.14 [1.00-1.29]0.044Gender mismatch0.99 [0.91-1.08]0.835Donor/recipient weight ratio <0.81.02 [0.91-1.16]0.700Donor hypertension1.03 [0.95-1.12]0.476Left ventricular ejection fraction >50%1.06 [0.69-1.63]0.795Diabetes1.01 [0.87-1.17]0.861Cigarette use1.10 [1.01-1.19]0.028Cocaine use0.92 [0.83-1.03]0.146Cause of death AnoxiaRef Stroke1.01 [0.91-1.13]0.801 Head trauma1.00 [0.89-1.12]0.978 Others1.04 [0.80-1.36]0.761 RecipientsAge ≤45Ref 46-551.07 [0.94-1.23]0.275 56-651.35 [1.19-1.53]<0.001 >651.61 [1.41-1.85]<0.001Female0.94 [0.86-1.03]0.169Black1.21 [1.10-1.34]<0.001Obesity1.21 [1.11-1.32]<0.001Diabetes1.26 [1.17-1.38]<0.001Pretransplant dialysis1.46 [1.25-1.71]<0.001Pretransplant cardiac surgery1.26 [1.17-1.37]<0.001Pretransplant mechanical ventilator1.45 [1.09-1.93]0.011Pretransplant ECMO1.26 [0.89-1.79]0.186IV inotropes at transplant0.95 [0.87-1.03]0.212VAD0.99 [0.89-1.10]0.887End status 10.94 [0.79-1.12]0.517 20.98 [0.82-1.18]0.833 3-6RefTransplant era 2000-2005Ref 2006-20100.99 [0.86-1.15]0.917 2011-20150.96 [0.82-1.13]0.627 2016-20200.91 [0.77-1.10]0.313 2021-20240.82 [0.64-1.04]0.104Abbreviations: CMV, cytomegalovirus; ECMO, extracorporeal membrane oxygenation; IV, intravenous; VAD, ventricular assist device.
Mortality risk score for adult heart transplant with donors aged ≥45 years
Pretransplant ECMO was not a statistically significant risk factor (p = 0.183), probably due to the fact that only 117 patients (1.8%) were on ECMO. However, given its clinical relevance and relatively large effective size (HR = 1.25; 95% CI, 0.90-1.73), we still included it together with 10 other statistically significant variables in the multivariable model to develop the risk score. Three donor-related factors (ischemic time ≥4 hours, CMV-positive serostatus, and cigarette use) were each assigned a score of 1 point. Recipient-related factors contributed more substantially to overall risk. Recipient diabetes, pretransplant ECMO, and history of cardiac surgery were each assigned 3 points, while Black race and obesity contributed 2 points each. The highest individual scores were attributed to age >55, pretransplant dialysis, and mechanical ventilator support, each contributing 4 points. Based on cumulative scores, patients were stratified into 3 risk categories: low risk (total score <5), moderate risk (score 5-7), and high risk (score >7). Details are presented in Table 3. Kaplan-Meier analysis and log-rank test revealed significantly reduced survival in the high-risk group (p < 0.001), validating the utility of the score for clinical risk stratification (Figure 1). One-, 5, and 10-year survival rates by risk categories were presented in Table 4.Table 3. Multivariable Model for the 11 Most Significant Factors and Their Corresponding Risk ScoresTable 3Risk factorsHazard ratio [95% CI]p-valueCoefficientsScoreDonorsIschemic time ≥4 hours1.11 [1.02-1.21]0.0180.1031Donor CMV positive1.11 [1.03-1.19]0.0090.1001Cigarette use1.09 [1.01-1.18]0.0260.0881 RecipientsAge >551.37 [1.27-1.49]<0.0010.3174Black1.19 [1.08-1.30]<0.0010.1732Obesity1.20 [1.11-1.30]<0.0010.1812Diabetes1.27 [1.17-1.37]<0.0010.2383Pretransplant dialysis1.44 [1.24-1.69]<0.0010.3684Pretransplant cardiac surgery1.29 [1.19-1.38]<0.0010.2523Pretransplant mechanical ventilator1.37 [1.10-1.74]0.0110.3134Pretransplant ECMO1.26 [0.92-1.73]0.1480.2343Low risk: total score <5; Moderate risk: total score 5-7; High risk: total score >7Abbreviations: CMV, cytomegalovirus; ECMO, extracorporeal membrane oxygenation.Figure 1. Heart transplant survival with donors aged ≥45 years by risk categories. Patients were grouped into low risk (<5), moderate risk (5-7), and high risk (>7) based on cumulative risk scores. The high-risk group demonstrated significantly reduced survival compared to low- and moderate-risk groups (p < 0.001), supporting the prognostic utility of the risk score.Figure 1. Table 4Survival Rates of Heart Transplants With Donors Aged ≥45 Years by Risk CategoriesTable 4Patient survival estimates with 95% confidence intervalsTime frame (years)Low risk (risk score <5)Moderate risk (risk score 5-7)High risk (risk score >7)191.5 (90.2-92.7)88.0 (86.9-89.1)82.9 (81.1-84.6)580.0 (78.0-81.9)79.0 (72.6-75.7)67.4 (64.9-69.7)1064.7 (62.0-67.3)54.4 (52.2-56.5)42.6 (39.4-45.7)
Discussion
In response to the persistent shortage of donor hearts, there has been growing interest in expanding the donor pool by utilizing older donor hearts. The most recent ISHLT guidelines do not impose an upper age limit for donor heart selection and recommend considering donors aged ≥45 years, provided they are appropriately screened for coronary artery disease and short ischemic times (<4 hours) are anticipated.13 In our cohort, the oldest donor was 73 years old, and a total of 9,843 heart transplants (16.7% of all adult transplants between January 2000 and June 2024) involved donors aged ≥45 years. These organs represent a valuable resource that might otherwise have been discarded due to age alone.
Historically, advanced donor age has been associated with increased morbidity and mortality following heart transplantation.4, 5, 6, 7, 9, 10 However, recent studies using propensity score matching have demonstrated that, with careful donor-recipient matching, recipients of older donor hearts can achieve survival outcomes comparable to those receiving younger hearts.11, 12 These findings support the notion that older donor hearts, when appropriately selected, can be safely used in suitable candidates.
We found 10 significant risk factors associated with increased mortality in heart transplants with donors aged ≥45 years: ischemic time ≥4 hours, CMV-positive donor, donor cigarette use and the following recipient factors: age>55, Black race, obesity, diabetes, pretransplant dialysis, mechanical ventilation support, and prior cardiac surgery. Though not statistically significant, pretransplant ECMO was included in our risk score model given its large effect size and clinical relevance. In total, there are 11 factors we recommend to screen when considering heart donors aged ≥45 years. To the best of our knowledge, our model has fewer variables than previously published risk scores while still maintains a similar C-statistics of 0.58 (95% CI 0.57-0.60).15, 16, 17, 18, 19, 20, 21, 22 This suggests our work may offer a more streamlined and clinically friendly tool.
While most of the risk factors in our model are consistent with those reported in existing literature, CMV-positive donor status stands out.15, 16, 17, 18, 19, 20, 21, 22 CMV-positive donor is a well-established risk factor for CMV disease, which might lead to graft rejection and cardiac allograft vasculopathy. However, recent studies showed no statistically significant effect of CMV-positive donor on heart transplant survival.23, 24, 25 It might be due to the protective effect of antiviral prophylaxis and treatment. Our findings on the significant role of CMV status on heart transplant mortality might be specific for older donors only. Prior research has shown that donor age is an independent predictor of reduced CAV-free survival, implying that older hearts may be more susceptible to CMV-related endothelial injury, a key mechanism in the development of CAV.26 Further studies are warranted to explore the interaction between donor age and CMV infection in heart transplant outcomes.
Study limitations
This study is based on a retrospective analysis of the United Network for Organ Sharing registry data, which is subject to several inherent constraints. Missing data and inaccuracies in reporting may affect the reliability of certain variables, and incomplete follow-up can limit the assessment of long-term outcomes.
We believe fewer variables will make our risk score more clinically friendly and widely utilized. However, we might not have controlled other unmeasured confounders that might contribute to heart transplant survival. Our 10 recommended risk factors are by no means exhaustive. Each heart transplant team should consider other factors such as the availability of organ to a highly sensitized recipient and the survival chance of a patient while on the waiting list before deciding to accept or reject a heart donor ≥45 years. Despite a clinically important criterion to screen for in ISHLT guideline, due to the limited availability of angiographic data present in only 662 donors (6.7%), coronary artery stenosis was not included in the multivariable analysis and in the risk score.
Conclusions
Building on the ISHLT recommendations of avoiding significant coronary artery disease (coronary artery stenosis >50%) and ischemic time ≥4 hours, we have developed a novel risk score for use when considering heart transplant with a donor heart >45 years old. This risk score added CMV-positive donor status, donor cigarette smoking, and the following recipient factors: age >55, Black race, obesity, diabetes, pretransplant dialysis, pretransplant mechanical ventilator support, pretransplant ECMO, and prior cardiac surgery. While further prospective validation is warranted, this clinically useful and simple risk score may be utilized when considering the use of older donors for heart transplant.
CRediT authorship contribution statement
Anh Nguyen: Conceptualization, Methodology, Formal analysis, Data curation, Writing – original draft. Abbas Rana: Methodology, Resources, Writing – review & editing. Alexis Shafii: Methodology, Resources, Writing – review & editing. Gabriel Loor: Methodology, Resources, Writing – review & editing. Andrew Civitello: Methodology, Resources, Writing – review & editing. Todd Rosengart: Resources, Writing – review & editing, Supervision. Kenneth Liao: Conceptualization, Methodology, Resources, Writing – review & editing, Supervision.
Financial disclosure statement
This project does not have funding support from any sources.
Declaration of Competing Interests
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bozkurt B.Ahmad T.Alexander K.HF STATS 2024: heart failure epidemiology and outcomes statistics an updated 2024 report from the Heart Failure Society of America J Card Fail 3120246611610.1016/J.CARDFAIL.2024.07.00139322534 · doi ↗ · pubmed ↗
- 2Colvin M.Smith J.M.Ahn Y.OPTN/SRTR 2020 annual data report: heart Am J Transplant 22202235043710.1111/AJT.16977/ASSET/9A 37BF 42-B 025-4EE 1-AAE 6-8C 58B 30694 F 0/MAIN.ASSETS/GR 49.JPG 35266620 · doi ↗ · pubmed ↗
- 3Bakhtiyar S.S.Godfrey E.L.Ahmed S.Survival on the heart transplant waiting list JAMA Cardiol 520201227123510.1001/JAMACARDIO.2020.279532785619 PMC 7675100 · doi ↗ · pubmed ↗
- 4Nagji A.S.Hranjec T.Swenson B.R.Donor age is associated with chronic allograft vasculopathy after adult heart transplantation: implications for donor allocation Ann Thorac Surg 90201016817510.1016/j.athoracsur.2010.03.04320609769 PMC 3033784 · doi ↗ · pubmed ↗
- 5Roig E.Almenar L.Crespo-Leiro M.Heart transplantation using allografts from older donors: multicenter study results J Heart Lung Transplant 34201579079610.1016/j.healun.2014.10.00625499140 · doi ↗ · pubmed ↗
- 6Weber D.J.Wang I.W.Gracon A.S.A.The impact of donor age on survival after heart transplantation: an analysis of the United Network for Organ Sharing (UNOS) registry J Card Surg 29201472372810.1111/JOCS.1240625041692 · doi ↗ · pubmed ↗
- 7Weiss E.S.Allen J.G.Kilic A.Development of a quantitative donor risk index to predict short-term mortality in orthotopic heart transplantation J Heart Lung Transplant 31201226627310.1016/J.HEALUN.2011.10.00422093382 · doi ↗ · pubmed ↗
- 8Bergenfeldt H.Lund L.H.Stehlik J.Andersson B.Höglund P.Nilsson J.Time-dependent prognostic effects of recipient and donor age in adult heart transplantation J Heart Lung Transplant 38201917418310.1016/j.healun.2018.10.00330502009 · doi ↗ · pubmed ↗