Fluoroscopy-free mini-PCNL using CT–ultrasound fusion guidance in a pediatric patient with recurrent cystine stones: A case report
Surawach Piyawannarat, Kun Sirisopana, Yada Phengsalae, Premsant Sangkum, Wisoot Kongchareonsombat, Chinnakhet Ketsuwan

TL;DR
A new radiation-free method for kidney stone removal in a child with cystine stones is described, using CT and ultrasound fusion guidance.
Contribution
This case report demonstrates the feasibility of fluoroscopy-free mini-PCNL in pediatric patients using CT-ultrasound fusion guidance.
Findings
Renal access and complete stone clearance were achieved in a 12-year-old boy using the fusion-guided approach.
The procedure was completed safely with minimal blood loss and a 90-minute operative time.
CT-ultrasound fusion guidance overcomes limitations of ultrasound-only methods in complex pediatric cases.
Abstract
Pediatric patients are particularly susceptible to ionizing radiation risks. A fluoroscopy-free mini-percutaneous nephrolithotomy (mini-PCNL) was performed using computed tomography (CT)–ultrasound fusion guidance for recurrent cystine nephrolithiasis in a 12-year-old boy. Renal access and complete stone clearance were achieved. Integrating preoperative CT with real-time ultrasonography enabled precise targeting, overcoming limitations of ultrasound-only guidance. The procedure was completed safely, with minimal blood loss and 90-min operative time. CT–ultrasound fusion-guided mini-PCNL is a feasible radiation-sparing approach for pediatric patients with complex renal stones.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
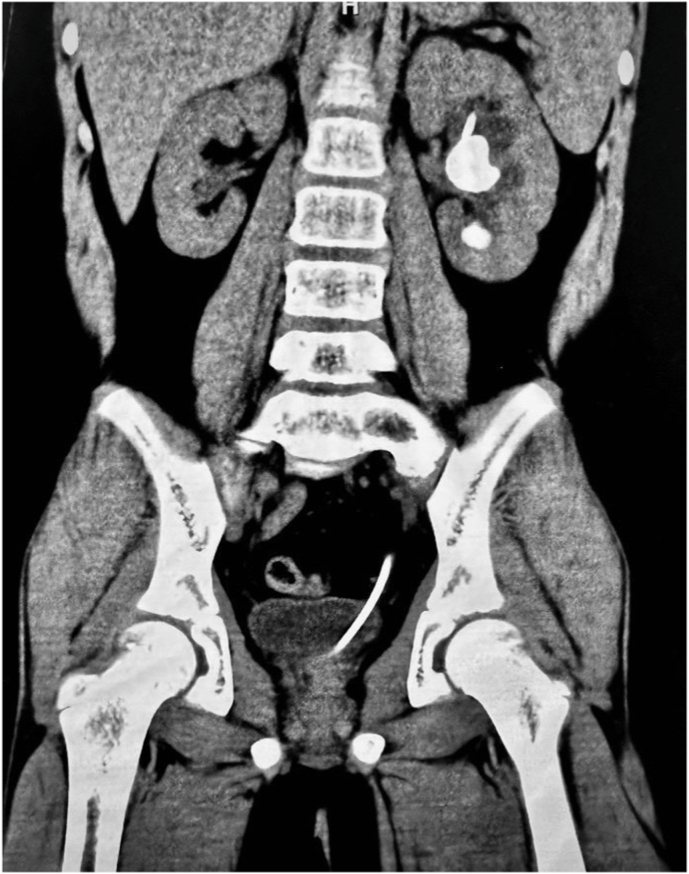 Figure 1
Figure 1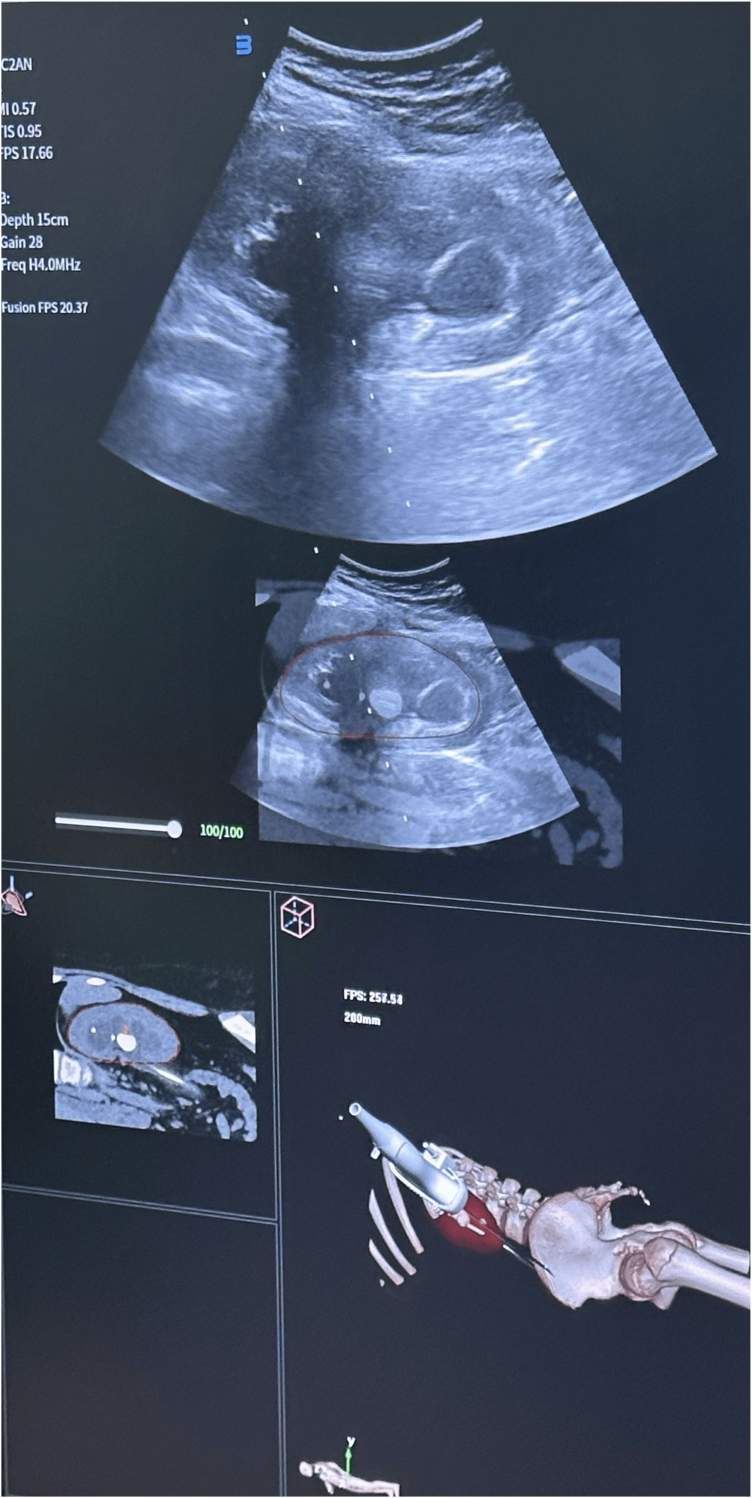 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsKidney Stones and Urolithiasis Treatments · Biomedical Research and Pathophysiology · Ureteral procedures and complications
Introduction
1
Cystinuria is a rare inherited disorder characterized by impaired renal tubular reabsorption of cystine, resulting in recurrent stone formation from childhood.1 Pediatric patients with cystinuria often require repeated surgical interventions, which leads to cumulative exposure to ionizing radiation. Given the increased radiosensitivity and longer life expectancy of pediatric patients and that pediatric patients with cystinuria have a high risk of lifelong stone recurrence and repeated exposure to diagnostic and therapeutic radiation,2^,^3 it is essential to apply the “as low as reasonably achievable” (ALARA) principle when planning treatment for patients in this group to minimize radiation exposure.4^,^5
Mini-percutaneous nephrolithotomy (mini-PCNL) is a popular surgical option for treating stones due to its lower incidence of serious complications and reduced need for blood transfusion compared to standard PCNL 6, 7, 8, 9. It is an established treatment for pediatric renal stones; however, the conventional fluoroscopic guidance method utilized during this procedure is a major source of intraoperative radiation.10 Ultrasound-guided PCNL is a widely accepted radiation-free alternative, although achieving accurate calyceal puncture can be challenging using this methodology, particularly in cases with complex renal anatomy and stone disease.11^,^12
Computed tomography (CT)–ultrasound fusion imaging, which integrates preoperative CT images showing anatomical features with real-time ultrasound guidance, may enhance puncture accuracy while avoiding intraoperative fluoroscopy. We report the use of fluoroscopy-free mini-PCNL with CT–ultrasound fusion imaging guidance to manage recurrent cystine nephrolithiasis in a pediatric patient.
Case report
2
A 12-year-old male with a known history of cystinuria presented with left flank pain. The patient's condition was previously managed with lifestyle modifications, oral alkalinization, and a right-side PCNL two years prior. A non-contrast CT scan revealed a 3.0 cm renal pelvic stone and a 0.7 cm lower pole stone in the left kidney (mean density: 720 HU; Fig. 1). A recurrent 3.5 cm staghorn calculus was also noted in the right kidney. Initial management involved inserting a left ureteral stent for pain relief before referral to our institution. Given the patient's pediatric status and stone burden, a fluoroscopy-free mini-PCNL was planned to minimize radiation exposure.Fig. 1. Preoperative non-contrast computed tomography image showing a 3.0 cm renal pelvic stone and a 0.7 cm lower pole stone in the left kidney.Fig. 1
Under general anesthesia, intravenous fosfomycin was administered for perioperative prophylaxis. The ureteral stent was removed, and a 5-Fr retrograde ureteral catheter was inserted to allow saline instillation, if required.
The patient was placed in the prone position. CT–ultrasound fusion imaging was performed using the VENUS system (Carbon [Shenzhen] Medical Device Co., Ltd., China). Preoperative CT images were imported and co-registered with real-time ultrasound images using renal anatomical landmarks. The fusion imaging enabled the precise identification of the targeted upper-pole calyx (Fig. 2).Fig. 2Intraoperative view of the computed tomography–ultrasound fusion technique.Fig. 2
Fusion imaging was used to guide renal access, which was achieved using an 18-gauge needle. Successful puncture was confirmed by urine efflux. A Sensor™ guidewire (Boston Scientific, Natick, MA, USA) was advanced into the collecting system under ultrasound visualization. The tract was sequentially dilated, and a 14/16-Fr suction access sheath (Clear Petra, Well Lead Medical Co., China) was inserted. A 12-Fr miniature nephroscope (MIP M system; Karl Storz, Tuttlingen, Germany) was used.
Lithotripsy was performed using a 60-W thulium fiber laser (SOLTIVE™, Olympus, MA, USA) with energy settings of 0.2–1 J and frequencies of 10–30 Hz. Continuous suction facilitated fragment evacuation and maintained low intrarenal pressure. Complete stone clearance was confirmed endoscopically and by intraoperative ultrasound. A 6-Fr antegrade ureteral stent was inserted, and the procedure was completed without nephrostomy tube placement.
The operative time was 90 min, and the estimated volume of blood lost was 10 mL. The postoperative course was uneventful. A postoperative renal and bladder ultrasound confirmed complete stone clearance and that the stent was appropriately positioned. The patient was discharged on postoperative day three. The ureteral stent was removed four weeks later without complications. A three-month postoperative ultrasound showed no residual stones or hydronephrosis. At follow-up, the contralateral 3.5 cm staghorn calculus was scheduled for staged fluoroscopy-free mini-PCNL using a similar CT–ultrasound fusion-guided approach.
Discussion
3
In this case, we utilized CT–ultrasound fusion imaging during a mini-PCNL to overcome limitations associated with standard and ultrasound-guided PCNL techniques. This involved integrating detailed preoperative anatomical information derived from CT with real-time ultrasound images.13^,^14 The resultant overlay functioned as a “virtual roadmap” and enabled us to confidently and accurately puncture the calyx without fluoroscopy.15 This approach was particularly valuable for targeting the upper-pole calyx, which might have been challenging using ultrasound alone.
Recent studies conducted with adult populations have demonstrated that CT–ultrasound fusion-guided PCNL can reduce the operative time and complications while improving access accuracy.11^,^12 Our case extends these findings to the pediatric setting, illustrating its feasibility and safety in a child with complex, recurrent cystine stones.
Cystine stones are typically hard and resistant to conventional lithotripsy.2^,^16 Hence, it is critical to select an effective and efficient stone fragmentation method when treating cystinuria. In this case, the use of thulium fiber laser lithotripsy combined with a suction access sheath facilitated effective stone fragmentation, continuous debris evacuation, and low intrarenal pressure. The latter is an important consideration for infection prevention in pediatric patients.17
Despite these advantages, CT–ultrasound fusion imaging has some limitations, including additional cost, the need for preoperative CT imaging, and a learning curve for image co-registration. Therefore, this technique should be reserved for selected cases in which ultrasound-only guidance is anticipated to be challenging rather than as a routine replacement.
Conclusion
4
Our findings indicate that fluoroscopy-free mini-PCNL with CT–ultrasound fusion imaging guidance is a safe and feasible technique for selected pediatric patients with complex renal stone disease. By enabling precise renal access without intraoperative radiation, this approach abides by the ALARA principle and is a valuable adjunct to ultrasound-guided PCNL in pediatric endourology.
CRediT authorship contribution statement
Surawach Piyawannarat: Writing – original draft, Project administration, Formal analysis, Data curation, Conceptualization. Kun Sirisopana: Methodology, Investigation. Yada Phengsalae: Methodology, Investigation. Premsant Sangkum: Validation, Supervision. Wisoot Kongchareonsombat: Validation, Supervision. Chinnakhet Ketsuwan: Writing – review & editing, Supervision.
Ethical approval
This case report was conducted in accordance with the ethical standards of the institution and the 1964 Helsinki Declaration and its later amendments or comparable ethical standards (ethical approval number: COA No. MURA2025/717). Informed consent was obtained from the patient.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Declaration of competing interest
The authors declare that they have no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Gökçe M.İ.Karaburun M.C.Cystinuria in children: diagnosis and treatment World J Urol 4312025 Apr 1522610.1007/s 00345-025-05604-6PMID: 40234286; PMCID: PMC 1200026140234286 PMC 12000261 · doi ↗ · pubmed ↗
- 2Clark C.S.Gnanappiragasam S.Thomas K.Cystinuria: an overview of challenges and surgical management Front Surg 92022 Jun 1681222610.3389/fsurg.2022.812226 PMID: 35784929; PMCID: PMC 9243440 PMC 924344035784929 · doi ↗ · pubmed ↗
- 3Kowalczyk N.S.Zisman A.L.Cystinuria: review of a life-long and frustrating disease Yale J Biol Med 9442021 Dec 29681686 PMID: 34970106; PMCID: PMC 868676834970106 PMC 8686768 · pubmed ↗
- 4Varda B.K.Johnson E.K.Johnson K.L.Imaging and surgical utilization for pediatric cystinuria patients: a single-institution cohort study J Pediatr Urol 1222016 Apr 106.e 1106.e 710.1016/j.jpurol.2015.08.019Epub 2015 Oct 22. PMID: 2659722926597229 · doi ↗ · pubmed ↗
- 5Saadeh S.A.Pediatric nephrolithiasis: risk factors, evaluation, and prevention Pediatr Ann 4962020 Jun 1e 262e 26710.3928/19382359-20200518-01PMID: 3252036732520367 · doi ↗ · pubmed ↗
- 6Ekkasak S.Cherntanomwong P.Phengsalae Y.Massive haemothorax from percutaneous nephrolithotomy requiring video-assisted thoracoscopic surgery: a case report Int J Surg Case Rep 1062023 May 10825110.1016/j.ijscr.2023.108251 Epub 2023 Apr 21. PMID: 37087937; PMCID: PMC 10149323 PMC 1014932337087937 · doi ↗ · pubmed ↗
- 7Ketsuwan C.Pimpanit N.Phengsalae Y.Peri-operative factors affecting blood transfusion requirements during PCNL: a retrospective non-randomized study Res Rep Urol 122020 Jul 2227928510.2147/RRU.S 261888 PMID: 32802804; PMCID: PMC 738310832802804 PMC 7383108 · doi ↗ · pubmed ↗
- 8Rujithamkul M.Sirisopana K.Piyawannarat S.Simultaneous Mini-ECIRS and low-energy TFL endopyelotomy for recurrent UPJO with pelvic renal calculus: a case report Urol Case Rep 632025 Aug 3110319010.1016/j.eucr.2025.103190 PMID: 40949714; PMCID: PMC 12423339 PMC 1242333940949714 · doi ↗ · pubmed ↗