Ondasetron as Premedication for Unsedated Upper Digestive Endoscopy: A Cross‐Sectional Study Assessing Tolerance and Acceptability
Espoir Batumike Murhi, Raissa Boroto Iranga, Corneille Lembembu, Tony Akilimali Shindano

TL;DR
This study shows that using ondansetron as premedication allows most patients to tolerate unsedated upper digestive endoscopy well, especially when the procedure starts smoothly.
Contribution
Demonstrates the feasibility of unsedated endoscopy in low-income settings using ondansetron premedication and highlights factors influencing patient tolerance.
Findings
91.72% of patients tolerated unsedated endoscopy well with ondansetron premedication.
Ease of endoscope insertion was the primary determinant of good tolerance (adjusted OR 44.34).
Abstract
In many low‐income countries, gastroduodenal endoscopy under conscious sedation remains uncommon due to added costs and concerns about managing complications and side effects. This study aimed to assess the feasibility of performing the procedure without sedation, using a potent antinauseant as premedication. We conducted a prospective, single‐center study between 2020 and 2022 in Bukavu, eastern Democratic Republic of the Congo. Endoscopies were performed without sedation, supplemented by a protocol involving sublingual ondansetron spray. Clinical outcomes, procedural data, and patient feedback before and after the procedure were analyzed. A total of 145 patients were enrolled, including 76 men (52.4%). Only 12 patients (8.28%) reported poor tolerance. The majority (91.72%) tolerated the procedure well, especially those who followed instructions and for whom endoscope insertion was…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1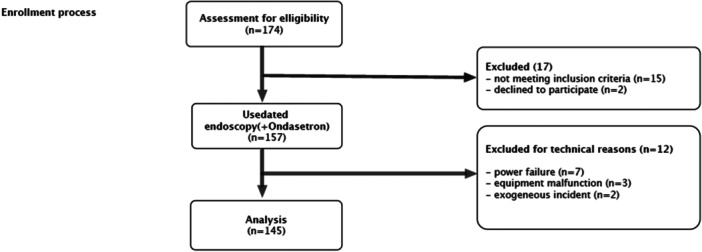 Figure 2
Figure 2| Variables | Intolerance |
| |
|---|---|---|---|
| No | Yes | ||
| Median age | 47 (18 80) | 60 (18 80) | 0.258 |
| Sex | |||
| Female ( | 62 (46.62) | 7 (58.33) | 0.436 |
| Male ( | 71 (53.38) | 5 (41.67) | |
| Level of education | |||
| None | 5 (3.76) | 4 (33.33) | < 0.001 |
| Primary | 37 (27.82) | 2 (16.67) | |
| Secondary | 66 (49.62) | 2 (16.67) | |
| University | 25 (18.80) | 4 (33.33) | |
| Height (cm) | 161.57 ± 8.83 | 161.08 ± 8.33 | 0.854 |
| Weight (Kgs) | 63.60 ± 13.71 | 55.23 ± 8.64 | 0.040 |
| BMI | 24.41 ± 5.3 | 21.16 ± 1.9 | 0.039 |
| Alcohol consumption | 65 (48.87) | 5 (41.67) | 0.632 |
| Smoking | 20 (15.04) | 2 (16.67) | 0.573 |
| Variables | Intolerance | ||
|---|---|---|---|
| No | Yes |
| |
| Endoscopy indications | |||
| Epigastralgia | 92 (69.17) | 9 (75) | 0.786 |
| Digestive bleeding/Anemia | 27 (20.30) | 3 (25) | |
| Others | 14 (10.53) | 0 (0) | |
| Medical history and pre‐endoscopic information | |||
| Previous endoscopy | 18 (13.53) | 0 (0) | 0.190 |
| Have received explanations about the procedure | 43 (32.33) | 4 (33.33) | 0.586 |
| Ever heard of endoscopy | 72 (54.14) | 4 (33.33) | 0.140 |
| Time interval since last meal (minutes) | 808.50 (450–1200) | 781.50 (30–1230) | 0.563 |
| Pre‐examination apprehensions | |||
| Subjective anxiety | 59 (44.36) | 8 (66.67) | 0.138 |
| Degree of anxiety (using the tolerance assessment tool) | 1.69 ± 2.05 | 2.91 ± 2.74 | 0.070 |
| Fear of pain | 40 (31.50) | 5 (45.45) | 0.264 |
| Fear of nausea | 4 (3.01) | 1 (8.33) | 0.355 |
| Fear of vomiting | 4 (3.01) | 0 (0) | 0.705 |
| Fear of suffocation | 4 (3 01) | 0 (0) | 0.705 |
| Fear of injury | 1 (0.7) | 2 (16.67) | 0.018 |
| Endoscopy process | |||
| Easy introduction | 119 (89.47) | 4 (33.33) | <0.001 |
| Good cooperation (following instructions correctly) | 119 (89.47) | 5 (41.67) | <0.001 |
| Variables | OR adj (95% CI) |
|
|---|---|---|
| Weight | 0.90 (0.78–1.04) | 0.148 |
| Level of education | ||
| None | 3.67 (0.03–463.52) | 0.598 |
| Primary | 0.34 (0.01–8.29) | 0.509 |
| Secondary | 0.01 (0.00–0.98) | 0.049 |
| University | 1 | |
| Fear of injury | ||
| Yes | 1 | |
| No | 5.97 (0.01–207413.80) | 0.738 |
| Easy introduction | ||
| Yes | 44.34 (2.78–708.22) | 0.007 |
| No | ||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAnesthesia and Sedative Agents · Colorectal Cancer Screening and Detection · Gastrointestinal motility and disorders
Introduction
1
Gastroduodenal endoscopy (GDE) is among the most widely performed diagnostic procedures worldwide. It can be carried out by direct inspection or, more commonly today, with flexible video‐endoscopes. The technique enables both diagnosis and therapeutic intervention for major upper gastrointestinal diseases. Conscious sedation is increasingly used to enhance patient tolerance. Reports indicate that up to 5% of patients refuse the procedure without sedation, while 10% require significant persuasion to accept it under such conditions [1, 2, 3, 4].
Nevertheless, sedation carries risks and limitations. These include hypoxia, extended post‐procedure monitoring, increased staffing needs, higher costs, absence from work, and the requirement for an escort home. Adverse events occur in approximately 1 in 200 procedures, with 60% related to road accidents [2]. Some practitioners also argue that sedation may compromise diagnostic accuracy, particularly due to sedation‐induced gastro‐esophageal reflux [5, 6]. For these reasons, unsedated GDE remains the preferred approach in certain regions [7].
In Sub‐Saharan Africa, where universal healthcare coverage is lacking, endoscopy is frequently performed without sedation. Cost considerations are central, given the population's average income and the predominance of fee‐for‐service care [3].
Although tolerance and acceptance of unsedated GDE have been studied worldwide, data from the Democratic Republic of the Congo (DRC) are scarce. Endoscopy is relatively new in the country and limited to major cities due to shortages of equipment, trained personnel, and accessibility. A 2013 survey identified only 14 gastroenterologists nationwide (1 per 4 million inhabitants), compared with 1 per 14,000 in France; of these, only 4 were actively performing endoscopy [8].
In South Kivu province, endoscopy has been available at the Hôpital Provincial Général de Bukavu (HPGRB) since 2002. Since its introduction, the procedure has been surrounded by misinformation, rumors, and apprehension among the population. Some medical staff also hesitate to recommend it due to limited awareness. To date, no study has examined its sociological impact locally.
The present study aimed to assess the extent of reluctance, the underlying reasons for fear, and the degree of tolerance. We also sought to evaluate patient perceptions after the procedure and identify predictors of poor tolerance to improve practice. As a secondary objective, we investigated the potential benefit of ondansetron, a potent antinauseant, as premedication to enhance clinical tolerance.
Methodology
2
Study Design and Setting
2.1
We conducted a cross‐sectional study over 3 years (2020–2022) at HPGRB, a university hospital serving as the referral center for South Kivu province, which has a population of approximately 6 million. The province has two endoscopy units; the HPGRB unit is managed by a gastroenterologist assisted by a trainee intern.
Study Population
2.2
Eligible participants were patients undergoing diagnostic GDE without sedation. Exclusion criteria included pregnancy, age under 18 years, procedures performed under sedation or general anesthesia, therapeutic endoscopy, technical incidents (e.g., power failure, equipment malfunction), refusal to participate, or insufficient comprehension of the survey. Participants were continuously enrolled during the study period. The study was approved by the Ethical Committee of our hospital, and all patients enrolled gave their written informed consent to participate in the study.
Endoscopic Procedure and Data Collection
2.3
All procedures were performed by the same gastroenterologist using video endoscopy with an OLYMPUS multidirectional axial‐view fiberscope.
Prior to the procedure, the nurse provided psychological preparation and explained potential discomforts. Premedication consisted of sublingual ondansetron (8 mg spray, administered 15–30 min before) and oropharyngeal anesthesia with 2% Lidocaine spray. The choice of this formulation and route of administration (ondansetron oral spray) is related to the proven superiority of selective 5‐HT3 serotonin‐receptor antagonists over other conventional anti‐nausea drugs and the fact of their rapid absorption and quick reach of peak plasma concentration (10–15 min) at the standard dose of 8 mg in adults. Additionally, ondansetron has a significantly lower risk of severe cardiovascular and central nervous system side effects [9, 10].
Patients were positioned in the left lateral decubitus. The endoscope was introduced orally under direct vision, and the esophagus, stomach, and first two duodenal segments were examined. Five gastric biopsies were systematically obtained (two from the antrum, one from the angle, and two from the body).
Each patient completed a questionnaire before and after the procedure, covering:
- Pre‐procedure data: clinical history, last meal, prior information received, and apprehensions.
- Technical data: ease of endoscope insertion, cooperation, incidents, duration, and findings.
- Post‐procedure data: subjective tolerance and willingness to repeat the procedure under similar conditions.
Tolerance was assessed using a visual analog scale (endoscopy tolerance assessment tool, see Figure 1), with scores categorized as:
- Excellent tolerance: 0–2
- Acceptable tolerance: 3–4
- Low tolerance: 5–8
- Intolerance: > 8
Endoscopy tolerance assessment tool.
Statistical Analysis
2.4
We used STATA 17 software (StatCorp) for data analyses. Quantitative variables were described by means and their standard deviations or medians and their interquartile ranges. The Kruskal–Wallis, Mann–Witney, and Student's t‐tests were used to assess the association between quantitative and categorical variables, as appropriate. Categorical variables were compared using the Chi‐square test and Fisher's exact test.
Simple logistic regression was performed by calculating the Odds ratio (OR) at its 95% confidence interval (CI). Differences observed were considered significant at a p < 0.05.
Results
3
Of the 174 participants initially enrolled, only 145 took part in the study (Figure 2). Their general data according to tolerance are shown in Table 1. Epigastralgia was the main reason for consultation in about two‐thirds (69%). The most common diagnoses were gastritis (45.4%) and peptic ulcer disease (21.3%). Twelve percent had already had an endoscopy, while nearly half (47%) had never heard of it (Table 2). Only 12 patients (8.3%) said they didn't tolerate the procedure well, while most (91.7%) reported good or excellent tolerance. Age and gender did not seem to matter. A small amount of intolerance was seen among illiterate and university‐level patients. Those who tolerated the procedure best were the ones who followed instructions carefully and when the scope was easy to insert (p < 0.001). These patients were also much more willing to repeat the procedure compared with those who struggled (84.9% vs. 16.7%) [data not shown]. In multivariate analysis (Table 3), ease of insertion stood out as the main factor for good tolerance (adjusted OR 44.34 [2.78–708.22], p = 0.007).
flowchart for patients' inclusion.
Discussion
4
This study, done in a large hospital in South Kivu, showed that endoscopy was generally well tolerated (91.7%) even without sedation. Most patients were open to repeating the test under the same conditions. The key factor was how easily the scope could be inserted. In fact, 90.2% of patients had easy insertion. Most (84.9%) reported no unexpected symptoms, which gave them confidence for future exams. On average, the procedure lasted about 6 min, similar to sedated procedures. Some studies have found similar results [11, 12, 13]. This suggests that skipping sedation doesn't necessarily make the procedure longer if the doctor is experienced.
More than half of patients (52.7%) already knew about endoscopy, either because they had heard of it or had done it before (12.3%). Still, about a third (33.1%) were nervous, mainly afraid of pain. This shows that awareness of endoscopy is still limited in Sub‐Saharan Africa. In Morocco, though, almost half of patients had already had at least one endoscopy, showing higher familiarity [12].
Out of the 145 patients in our study, 68 (46.5%) felt anxious before the exam, mostly because they were worried about pain. This was lower than in Salwa's study, where nearly 78% of patients reported anxiety [12]. Only 4.1% of our patients experienced nausea, compared with almost 80% in Sombié's study [11]. The low rate of nausea here is probably thanks to our department's protocol, which combines Ondansetron with Lidocaine. Indeed, the addition of sublingual Ondasetron as premedication, a powerful anti‐nauseant, seems to have helped reduce this side effect.
We initially offered endoscopy to 147 patients, but two refused because of fear, giving us an acceptability rate of 98.6%. Of the 145 who went through with it, most (91.7%) tolerated the procedure well or found it acceptable. These results are very encouraging, showing tolerance levels close to those seen with sedation. For comparison, a study in Kinshasa (DRC) reported only 60% tolerance [13], while in Senegal, intolerance was seen in 42.5% of unsedated cases [14]. In Burkina Faso, tolerance was 84.6% [15], and in Iraq and Iran, rates were around 80% [16, 17]. Some Western data have reported tolerance rates of around 80% to 85% with conventional endoscopy without sedation [13, 14]. Nevertheless, better tolerance rates for procedures without sedation have been achieved with the use of ultrathin endoscopes via the transoral route or, better still, the transnasal route [18, 19, 20, 21, 22, 23].
What stands out is the importance of good preparation. Clear explanations of the procedure and possible discomforts make a big difference, as other studies have shown [24, 25, 26, 27, 28]. Patients in our study almost unanimously said the exam matched the explanations they were given beforehand, which likely boosted their confidence and tolerance.
The high tolerance we found may reflect both good practice and the effectiveness of our protocol. While sedation is usually recommended, our results suggest that adding Ondansetron can be a good alternative. It seems to make the insertion of the scope easier, which was the main factor linked to patient comfort. However, it should not be forgotten that easy insertion of the endoscope also depends on several other factors, including the operator's experience, the patient's level of preparation, and the anatomical characteristics specific to each patient.
Sedation is not common in our setting, mostly for financial reasons. Even so, the tolerance levels we achieved were similar to those in Western countries where sedation is standard, which suggests our approach is worth further evaluation.
Tolerance of the first endoscopy is important because it influences whether patients are willing to repeat the procedure. Sombié's study found similar acceptability rates (83.7% vs. 84.9%) [11]. In Morocco, however, only 43% of patients said they would repeat the exam under the same unsedated conditions [12].
It's also worth noting that patient comfort depends heavily on the operator's experience, and cultural factors play a role in how invasive procedures are accepted.
Study Limitations
5
This was a single‐center study, so the findings cannot be generalized to the whole Congolese or South Kivu population. Indeed, selection bias could occur due to the socio‐demographic and economic characteristics of the participants. We also didn't compare different premedication protocols (Lidocaine alone, Lidocaine + Ondansetron, or conscious sedation), which would have strengthened the conclusions. Another limitation is that the data came from only one operator, which could lead to a certain degree of subjectivity bias. Still, this is the first study to look at endoscopy acceptability in this community and the first to assess Ondansetron premedication. Finally, the study was conducted during the COVID‐19 pandemic, which may have reduced the number of procedures and influenced patient reactions.
Conclusion
6
Upper gastrointestinal endoscopy is still relatively new in many African countries, including the DRC. Its wider use is limited by patient fears and the challenges of sedation. Our study showed that endoscopy without sedation but with Ondansetron was well tolerated and comfortable for patients. Larger multicentric comparative studies (randomized controlled trial with stratification by drug dosages, patient groups, or endoscopy indications), including assessment of early or delayed adverse reactions, are needed to confirm these findings.
Author Contributions
Espoir Batumike Murhi produced endoscopic data, assisted in data collection, and drafted the manuscript. Raissa Boroto Iranga, Corneille Lembembu, and Corneille Lembembu are responsible for data analysis. Tony Akilimali Shindano conceived and designed the study, produced endoscopic data, assisted in data analysis, and reviewed the manuscript. All authors have read and approved the final version of the manuscript.
Funding
The authors received no specific funding for this work.
Conflicts of Interest
The authors declare no conflicts of interest.
Transparency Statement
The lead author, Tony Akilimali Shindano, affirms that this manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1H. Yahya , H. Umar , B. T. Shekari , K. Sani , and M. H. Yahya , “Tolerance and Acceptance for Unsedated Diagnostic Upper Gastrointestinal Endoscopy in Kaduna, North‐West Nigeria,” Nigerian Postgraduate Medical Journal 29, no. 2 (2022): 138–145, 10.4103/npmj.npmj_697_21.35488582 · doi ↗ · pubmed ↗
- 2R. Campo , E. Brullet , A. Montserrat , et al., “Identification of Factors That Influence Tolerance of Upper Gastrointestinal Endoscopy,” European Journal of Gastroenterology & Hepatology 11, no. 2 (1999): 201–204, 10.1097/00042737-199902000-00023.10102233 · doi ↗ · pubmed ↗
- 3N. J. Shaheen , M. B. Fennerty , and J. J. Bergman , “Less Is More: A Minimalist Approach to Endoscopy,” Gastroenterology 154, no. 7 (2018): 1993–2003, 10.1053/j.gastro.2017.12.044.29454789 · doi ↗ · pubmed ↗
- 4M. Lauriola , M. Tomai , R. Palma , et al., “Intolerance of Uncertainty and Anxiety‐Related Dispositions Predict Pain During Upper Endoscopy,” Frontiers in Psychology 10, no. May (2019): 1112, 10.3389/fpsyg.2019.01112.31156518 PMC 6529782 · doi ↗ · pubmed ↗
- 5H. J. Lee , B. Kim , D. W. Kim , et al., “Does Sedation Affect Examination of Esophagogastric Junction During Upper Endoscopy?,” Yonsei Medical Journal 56, no. 6 (2015): 1566–1571, 10.3349/ymj.2015.56.6.1566.26446638 PMC 4630044 · doi ↗ · pubmed ↗
- 6F. W. D. Tai , H. L. Ching , M. Sloan , R. Sidhu , and M. Mc Alindon , “Comparison of Patient Tolerance and Acceptability of Magnet‐Controlled Capsule Endoscopy and Flexible Endoscopy in the Investigation of Dyspepsia,” Endoscopy International Open 10, no. 06 (2022): E 735–E 744, 10.1055/a-1790-5996.35692932 PMC 9187367 · doi ↗ · pubmed ↗
- 7A. L. Faulx , A. Catanzaro , S. Zyzanski , et al., “Patient Tolerance and Acceptance of Unsedated Ultrathin Esophagoscopy,” Gastrointestinal Endoscopy 55, no. 6 (2002): 620–623, 10.1067/mge.2002.123274.11979240 · doi ↗ · pubmed ↗
- 8A. W. Tshimpi , “Il Faut Relancer L'endoscopie Digestive En République Démocratique Du Congo It Is Necessary to Restart the Digestive Endoscopy in Democratic Republic of Congo,” Janvier PTD, Hoépato‐ R. Nasogastroscopie: l’ âge de raison? 8 (2015): 1922–1923.