Effects of narrative‐based interventions on self‐efficacy and self‐management in chronic disease: A systematic review and meta‐analysis
Zhuangyan Yao, Edmond Pui Hang Choi, Do Do Wai Nei Chow, Hong Chen, Lizhen Wang, Mu‐Hsing Ho

TL;DR
Narrative-based interventions can improve self-efficacy and self-management in patients with chronic diseases, according to a review of 34 studies.
Contribution
This study provides the first comprehensive meta-analysis on the effectiveness of narrative interventions for chronic disease self-management.
Findings
Narrative interventions significantly increased self-efficacy (SMD = 0.66) and self-management (SMD = 1.73) in chronic disease patients.
Improvements in self-efficacy were greater in upper- to middle-income countries and among patients with heart disease, cancer, and stroke.
Self-management effects were most pronounced for patients with neurological diseases and cancer.
Abstract
This systematic review and meta‐analysis aimed to evaluate the impact of narrative interventions on self‐efficacy and self‐management behaviors in patients with chronic diseases. We systematically searched EMBASE, the Cochrane Library, CINAHL, PsycINFO, China National Knowledge Infrastructure (CNKI), and PubMed from conception to 2025, supplemented by manual searches of reference lists. Randomized controlled trials (RCTs) assessing the effects of narrative interventions on self‐efficacy or self‐management in adults with chronic diseases were included. Data were pooled using random‐effects meta‐analysis. A total of 34 RCTs involving 4584 participants were included. The meta‐analysis showed that narrative‐based interventions significantly enhanced patients' self‐efficacy (22 studies; SMD = 0.66, 95% CI: 0.35–0.96, p < .001; I 2 = 59.6%) and self‐management behaviors (12 studies; SMD =…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
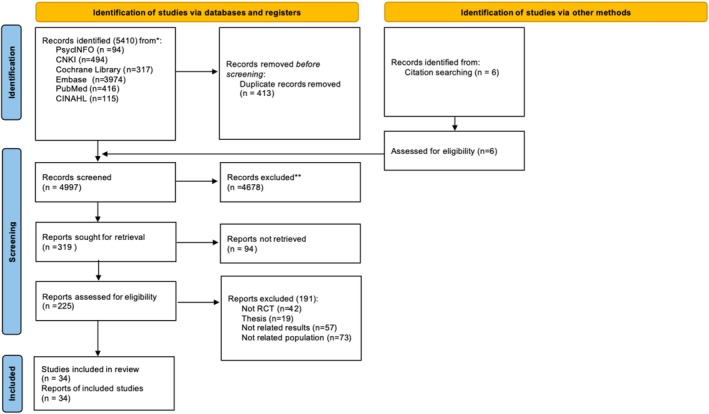 FIGURE 1
FIGURE 1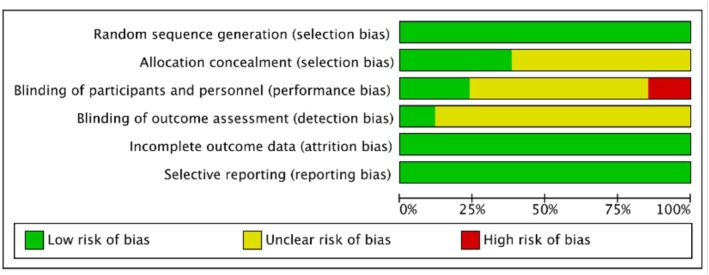 FIGURE 2
FIGURE 2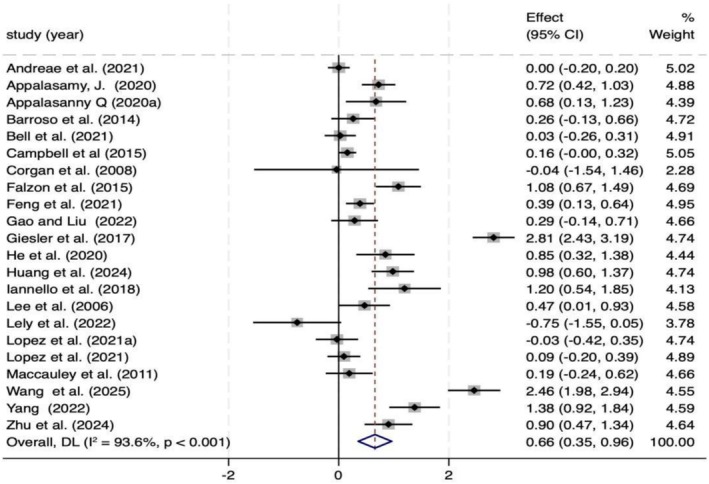 FIGURE 3
FIGURE 3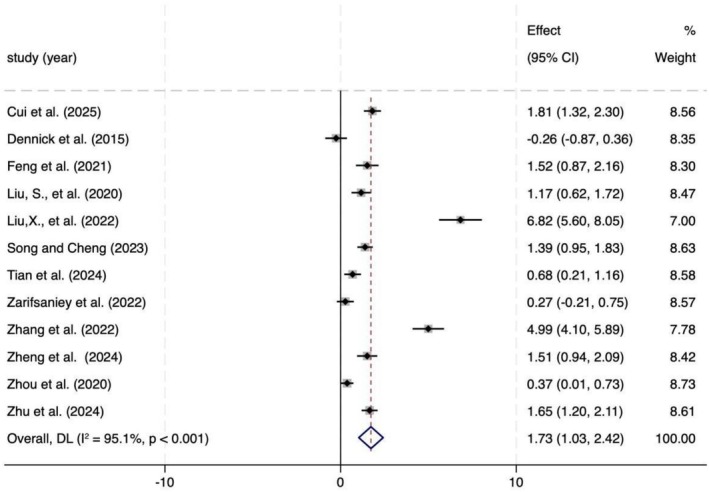 FIGURE 4
FIGURE 4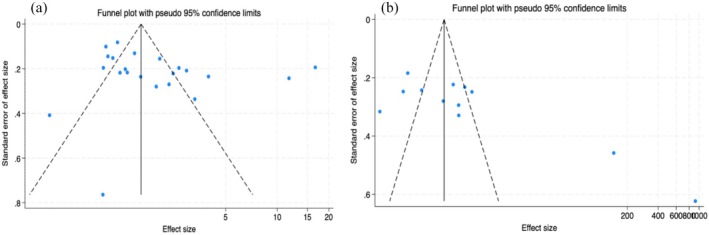 FIGURE 5
FIGURE 5| Variable | Subgroup | No. of studies | Sample size |
Overall effects ( ( |
|
‐value ( | Subgroup differences(‐value) |
|---|---|---|---|---|---|---|---|
| Country income‐level | High income | 13 | 2472 |
0.39 (0.01–0.77)
| 94.3 |
|
|
| Upper to middle income | 9 | 363 |
1.04 (0.65–0.31)
| 85.4 |
| ||
| Age | < 44 | 3 | 403 |
1.40 (−0.34–3.15)
| 98.5 |
|
|
| 45–59 | 12 | 2099 |
0.65 (0.33–0.97)
| 91.6 |
| ||
| > 60 | 7 | 333 |
0.31 (−0.06–0.68)
| 70.2 |
| ||
| Intervention type | Interpersonal narrative | 9 | 909 |
0.69 (0.08–1.30)
| 93.3 |
|
|
| Digital storytelling | 11 | 1,496 |
0.65 (0.22–1.07)
| 94.7 |
| ||
| Narrative message | 2 | 297 |
0.55 (−0.49–1.58)
| 94.2 |
| ||
| Duration | Single or brief sessions(s) | 5 | 629 |
0.35 (−0.05–0.75)
| 83.2 |
|
|
| Short‐term (1 day to 1 month) | 11 | 1,673 |
0.80 (0.33–1.27)
| 94.6 |
| ||
| Long‐term (> 1 month to 6 months) | 6 | 850 |
0.62 (−0.15–1.40)
| 95.3 |
| ||
| Publication year (period) | 2006–2019 | 8 | 1,221 |
0.80 (0.10–1.50)
| 96 |
|
|
| 2020–2025 | 14 | 1931 |
0.58 (0.25–0.90)
| 91.4 |
| ||
| Type of disease | Diabetes | 4 | 1,311 |
0.62 (−0.05–1.29)
| 96.7 |
|
|
| Stroke | 2 | 312 |
0.71 (0.45–0.98)
| 0.0 |
| ||
| Cancer | 6 | 575 |
0.98 (0.10–1.85)
| 95.0 |
| ||
| Arthritis and pain | 3 | 517 |
0.18 (−0.07–0.43)
| 48.9 |
| ||
| Others | 5 | 231 |
0.38 (−0.13–0.88)
| 77.4 |
| ||
| Heart disease | 2 | 206 |
1.16 (0.77–1.55)
| 40.3 |
| ||
| Type of self‐efficacy | Medication‐specific self‐efficacy | 4 | 874 |
0.45 (0.16–0.73)
| 73.1 |
|
|
| General self‐efficacy | 9 | 634 |
0.82 (0.27–1.37)
| 89.7 |
| ||
| Disease‐specific self‐efficacy | 10 | 2048 |
0.54 (0.09–1.00)
| 95.7 |
|
| Variable | Subgroup | No. of studies | Sample size |
Overall effects ( ( |
|
( | Subgroup differences ( |
|---|---|---|---|---|---|---|---|
| Age | < 45 | 5 | 390 |
2.16 (0.93–3.39)
| 96 |
|
|
| 45–59 | 4 | 328 |
1.24 (0.54–1.95)
| 87.9 |
| ||
| > 60 | 3 | 193 |
1.78 (−0.75–4.31)
| 97.9 |
| ||
| Intervention type | Interpersonal narrative | 10 | 804 |
2.08 (1.32–2.84)
| 95.1 |
|
|
| Digital storytelling | 1 | 66 |
−0.27 (−0.21–0.75)
| 0.0 | |||
| Writing narrative | 1 | 41 |
−0.26 (−0.87–0.36)
| 0.0 | |||
| Duration | Short‐term (≤ 1 month) | 4 | 280 |
2.33 (1.02–3.64)
| 94.4 |
|
|
| Medium‐term (2–3 months) | 11 | 359 |
0.52 (0.03–1.00)
| 79.5 |
| ||
| Long‐term (≥ 6 months) | 6 | 272 |
3.16 (1.18–5.15)
| 97.1 |
| ||
| Publication year (period) | 2024–2025 | 4 | 324 |
1.41 (0.90–1.92)
| 76.5 |
|
|
| 2015–2020 | 3 | 221 |
0.44 (−0.27–1.14)
| 83 |
| ||
| 2021–2023 | 5 | 366 |
2.93 (1.15–4.71)
| 97.4 |
| ||
| Type of disease | Cancer | 3 | 232 |
2.73 (1.01–4.45)
| 95.6 |
|
|
| Diabetes | 5 | 287 |
0.67 (0.11–1.23)
| 80.9 |
| ||
| Neurological disorders | 3 | 272 |
3.16 (1.18–5.15)
| 97.1 |
| ||
| Other chronic conditions | 1 | 120 |
0.37 (0.01–0.73)
| 0.0 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEmpathy and Medical Education · Mental Health and Patient Involvement · Diabetes Management and Education
INTRODUCTION
Chronic diseases are characterized by a prolonged course and slow progression, and their onset is closely linked to the complex interplay of factors such as genetics, physiology, behavior, and environment (World Health Organization, 2024). Unlike acute conditions, managing chronic diseases not only relies on medical interventions and symptom control but also requires the maintenance of long‐term healthy behaviors and adaptive adjustments in psychological and social functioning (Duda‐Sikuła & Kurpas, 2024). With the aging global population and significant lifestyle changes, the prevalence of chronic diseases continues to rise, posing a major challenge to global public health (Anderson & Durstine, 2019; Rudnicka et al., 2020). According to the latest report from the World Health Organization (2024), non‐communicable diseases account for approximately 41 million deaths annually, representing 74% of total global mortality, with leading causes including cardiovascular diseases, cancer, chronic respiratory diseases, and diabetes. These conditions persist in imposing physical strain and restricting functional capabilities on patients, while also profoundly impacting their psychological well‐being and social interactions. As a result, they create significant challenges for individuals, families, and society at large (Christiansen et al., 2021). Furthermore, the rising incidence of chronic illnesses is placing extraordinary strain on global health‐care infrastructures and economic systems (World Health Organization, 2024). In response to this global challenge, the WHO launched the Global Action Plan for the Prevention and Control of Non‐communicable Diseases (2013–2020) in 2013, which emphasizes the reduction of morbidity and mortality from chronic diseases through multisectoral collaboration, health promotion, and disease management (World Health Organization, 2013). However, despite various measures taken at the policy level, the prevention and control of chronic diseases remains unsatisfactory, especially in low‐ and middle‐income countries (Mwangi et al., 2021).
Enhancing patients' self‐management abilities is widely recognized as a core strategy for addressing the challenges associated with chronic disease management (Lorig & Holman, 2003; Richardson et al., 2014; Timmermans et al., 2023). Effective self‐management involves a range of behaviors, including adhering to medical advice, maintaining a balanced diet, engaging in regular physical activity, and continuously monitoring one's health status (Iovino et al., 2024; Kim et al., 2021). However, despite its indispensable role in improving clinical outcomes, patients often encounter considerable barriers when attempting to sustain these behaviors over the long term. These obstacles stem from multiple sources, such as perceived difficulties, fluctuating emotions and psychological states, and the practical challenges of integrating complex medical advice into daily life (Yıldırım, 2020). Research has shown that an individual's belief in their ability to carry out and adhere to self‐management behaviors—known as self‐efficacy—plays a critical role in overcoming these challenges (Chan, 2021). According to Bandura's (1977) Social Cognitive Theory, self‐efficacy influences not only motivation and behavioral choices but also the degree of persistence and emotional responses when facing obstacles. Importantly, self‐efficacy and self‐management behavior have a mutually reinforcing relationship. A substantial body of empirical evidence indicates that self‐efficacy is a key psychological antecedent that drives and sustains effective self‐management behaviors, such as medication adherence, symptom monitoring, and lifestyle modification (Chen et al., 2023; González‐Conde et al., 2019; Montalbano et al., 2023). Meanwhile, successful self‐management experiences further strengthen patients' self‐efficacy, creating a positive feedback loop (Huang, Li, et al., 2024).
However, this virtuous cycle is often difficult to initiate and sustain among adolescents. Gauci et al. (2021) reported in a systematic review of face‐to‐face, skills‐based self‐management programs (including educational sessions, behavioral skills training, and problem‐solving approaches) for adolescents with chronic diseases that, although such interventions may yield short‐term improvements in treatment adherence, they generally fail to produce clinically meaningful or durable long‐term effects. The review found that while some included studies demonstrated immediate or short‐term positive changes following the intervention, none provided evidence of sustained benefits. Over time, patients' adherence tended to decline or revert to baseline levels, and improvements in self‐efficacy were similarly difficult to maintain. This widespread limitation has prompted researchers to engage in deeper reflection. Traditional intervention strategies that focus primarily on knowledge dissemination and behavioral guidance may have inherent shortcomings in effectively and sustainably enhancing self‐efficacy (Farley, 2020). These approaches tend to rely on one‐way information delivery and often overlook patients' individual experiences and emotional needs, thereby failing to provide the contextual resonance and deeper psychological support required to genuinely motivate behavioral change (Devan et al., 2018).
Further evidence suggests that many existing self‐management programs do not systematically incorporate emotion regulation or physiological arousal management strategies—both of which play key roles in shaping self‐efficacy—ultimately limiting their clinical applicability and long‐term impact (Benzo, 2024; Boger et al., 2015; Jiang et al., 2019). As a result, identifying new intervention strategies that can more deeply and sustainably enhance self‐efficacy has become a critical and urgent priority in improving chronic disease self‐management. Against this backdrop, narrative‐based intervention—a patient‐centered psychological and behavioral approach—has attracted growing attention in recent years (Yang et al., 2020). The core of narrative‐based intervention lies in guiding patients to express, listen to, and reconstruct their illness‐related experiences in a structured manner, transforming internal, often fragmented or distressing experiences into coherent, shareable, and meaningful life stories (Yang et al., 2020).
The application forms of narrative‐based intervention are diverse. Common forms include digital storytelling, which presents first‐person accounts of patients or fictional characters through videos, multimedia, or animations to enhance emotional engagement and vicarious experience (Moreau et al., 2018); information‐based narrative messages, which embed health knowledge, behavioral recommendations, or treatment information within a storyline to improve comprehension and acceptance (Cates et al., 2015); and interpersonal or oral narratives, which facilitate meaning‐making, social support, and psychological adjustment through the telling and listening of illness experiences in individual interviews or group discussions (Roikjær et al., 2022). Additional forms include expressive or narrative writing and testimonial narratives, in which patients share their personal experiences (Roikjær et al., 2022).
The effectiveness of narrative‐based intervention has been preliminarily demonstrated across a variety of chronic disease contexts. For example, this approach has been successfully applied in diabetes management, stroke rehabilitation, and cancer care, where it has been shown to reduce anxiety and depression and enhance patients' adherence to treatment plans (Andreae et al., 2021; Appalasamy, Quek, et al., 2020; Crogan et al., 2008). In chronic pain management, narrative intervention has been found to strengthen patients' confidence in managing their symptoms, facilitate identification with peers' experiences, and thereby improve coping strategies and overall quality of life (Lopez‐Olivo, Des Bordes, et al., 2021; Perrier & Martin Ginis, 2017). In adolescent cancer patients, digital narrative creation enables the sharing of personal experiences, promotes trauma healing, and helps integrate past adversity with current life. For patients with dementia, narrative intervention can meet both physical and psychological needs, improve daily functioning, and delay cognitive decline (Laing et al., 2017).
From a theoretical perspective, social cognitive theory (Bandura, 1989) provides the core foundation for narrative‐based interventions, emphasizing that through vicarious experiences and observational learning, individuals can enhance self‐efficacy and thereby strengthen their capacity to manage chronic diseases (Shaffer et al., 2018). The elaboration likelihood model (Petty & Cacioppo, 1986) suggests that narratives influence individuals through two pathways: the central route, which stimulates deep cognitive processing, and the peripheral route, which triggers emotional resonance, thereby jointly promoting attitude change. The empathy elicited by narratives also enhances audience identification and emotional engagement with the story (Gesser‐Edelsburg, 2021; Hinyard & Kreuter, 2006). Compared with traditional didactic approaches, narrative‐based interventions have shown significant advantages in improving health‐related knowledge, attitudes, and behavioral intentions (Bell et al., 2021; Murphy et al., 2013). This advantage arises from narratives' ability to reduce psychological resistance to health information and enhance comprehension and memory retention (Bell et al., 2021; Falzon et al., 2015). Belief system theory (Rokeach, 1968) further explains the capacity of narrative‐based interventions to reshape individuals' core values and beliefs; when narrative content aligns with or constructively challenges a person's worldview, it can facilitate lasting behavioral change (Appalasamy, Quek, et al., 2020). The narrative immersion model provides additional support, suggesting that deep immersion and identification with a story can promote belief adjustment and emotional responses, thereby effectively predicting changes in health behaviors (Lee et al., 2015; Shaffer et al., 2018). Together, these theories form an integrated framework that systematically clarifies how narrative‐based interventions promote health behavior change through the synergistic effects of cognition, emotion, and belief.
Nevertheless, studies in this area exhibit significant variation in both theoretical foundations and methodological approaches. Numerous investigations are hindered by the absence of a standardized framework for categorizing narrative forms and explaining their underlying mechanisms, which limits their practical application in clinical settings and complicates the integration of research findings (Gucciardi et al., 2016; Winterbottom et al., 2008). Therefore, this study aims to conduct a systematic review and meta‐analysis to comprehensively evaluate the impact of narrative intervention on the self‐efficacy and self‐management behaviors of patients with chronic diseases. It also aims to explore potential moderating factors, including intervention type, disease type, intervention duration, publication time, and self‐efficacy type to identify the sources of heterogeneity. The research results are expected to provide high‐quality evidence for the effectiveness of this intervention measure, fill the existing research gaps, and provide guidance for developing more patient‐centered and evidence‐based chronic disease management methods.
METHODOLOGY
This systematic review protocol has been registered in the International Prospective Systematic Review Register (PROSPERO). Systematic reviews and meta‐analyses complied with the PRISMA guidelines and the Cochrane Handbook of Systematic Reviews (Higgins et al., 2022).
Inclusion and exclusion criteria
Based on the population, intervention, comparison, and outcome criteria, studies that met the following criteria were included: (1) Participants were diagnosed with chronic diseases as defined by the world health organization (WHO), including cardiovascular disease, diabetes, or cancer; (2) randomized control trails (RCTs) with narrative therapy, storytelling, narrative information, narrative diary, and other interventions related to the narrative; (3) the control group received usual care or placebo intervention; (4) self‐efficacy (the individual's confidence in their ability to take specific actions in managing chronic diseases [measured through validated self‐reporting scales] or self‐management behavior; (5) unlimited publication time, and only articles published in peer‐reviewed journals were considered.
Exclusion criteria: (1) Studies with no control group, or non‐RCTs (e.g., observational studies, conference papers, thesis, etc.); (2) studies that did not report self‐efficacy or self‐management data; and (3) studies that have not been published in either Chinese or English were excluded
Search strategy
A comprehensive search of six databases, including EMBASE, Cochrane Controlled Trials Centre, CINAHL, PsycINFO, CNKI, and PubMed, was conducted. A librarian was consulted to develop the search strategy. Search strategies were shown in Supplementary Table S1. Medical subject headings and free text keywords related to narrative‐based interventions were used from inception through August 2025. The reviewers also manually searched the reference lists of previously reviewed papers and included studies. The studies included in this review were RCTs of any design, published in either English or Chinese.
Study selection
The screening process in this study was divided into several steps. First, the reviewer conducted an initial screening of titles and abstracts based on the research question and the inclusion and exclusion criteria of this review. Subsequently, two reviewers further screened the abstracts after the initial screening to identify the literature that required full reading. If there was any disagreement between the two reviewers on the included literature, it was resolved through discussion with the third reviewer.
Data extraction
A table covering the study data was designed with reference to the Cochrane Handbook of Systematic Reviews (Higgins et al., 2022). Two researchers independently collected data from each study. The data collected included the name of the study lead author, year of publication, country, age, number of subjects, type and duration of intervention, assessment tool, and the data (mean ± SD) required for the meta‐analysis. If studies reported multiple self‐efficacy measures (e.g., both medication adherence efficacy and diabetes management efficacy), the most representative measure was selected from each study based on its primary focus and the content of the intervention to ensure data independence. Subgroup analyses were subsequently conducted according to the type of self‐efficacy.
Assessment
The risk of bias was assessed using the Risk of Bias 2.0 tool from the Cochrane Handbook of Systematic Reviews, covering the following aspects: selection bias, performance bias, detection bias, attrition bias, reporting bias, and other biases (Higgins et al., 2022). Review Manager 5.4 was used to evaluate the risk of bias. The quality of the evidence was assessed using the GRADE profiler, which includes five levels: study limitations (risk of bias), inconsistencies, indirectness, imprecision, and publication bias (Guyatt et al., 2011). The third reviewer was consulted to resolve any discrepancies.
Data analysis
This meta‐analysis was performed using RevMan 5.4 and Stata 18.0 software. Results were reported as mean difference (MD) if the outcome was measured on the same scale and as standard mean difference (SMD) otherwise. The size of the combined intervention effect was expressed as Cohen's d. A significance level of p < 0.05 was used. Heterogeneity between studies was assessed by calculating I ^2^. When I ^2^ > 50%, significant heterogeneity was indicated, and a random‐effects model was used. If I ^2^ ≤ 50%, a fixed‐effects model was used. Funnel plot and Egger's tests (using Stata 18.0) were used to explore publication bias (Egger et al., 1997). To further investigate potential sources of heterogeneity, this study conducted subgroup analyses and meta‐regression on the effect sizes of self‐efficacy, examining how factors such as intervention type, disease type, participant age, publication period, country, and income level influenced the estimated effects.
RESULTS
After searching with the strategies, 5410 records were retrieved from the following databases: PsycINFO (94), CNKI (494), Cochrane Library (317), EMBASE (3974), PubMed (416), and CINAHL (115). Four hundred thirteen duplicate records were removed using EndNote software. An additional six articles were identified by reference search. Two reviewers screened the titles and abstracts according to the inclusion criteria, ultimately excluding 4678 articles. A total of 319 records were retained for full‐text search, of which 94 were unavailable. Finally, the remaining 225 articles were evaluated in detail, and 187 were excluded for reasons including non‐randomized controlled trials (42), theses (19), outcome irrelevance (57), and population irrelevance (73). Ultimately, 34 studies were included in the review and meta‐analysis (Andreae et al., 2021; Appalasamy, Joseph, et al., 2020; Appalasamy, Quek, et al., 2020; Barroso et al., 2014; Bell et al., 2021, p. 202; Campbell et al., 2015; Crogan et al., 2008; Cui et al., 2025; Dennick et al., 2015; Falzon et al., 2015; Feng, Malloch, et al., 2021; Feng, Shen, & Jin, 2021; Gao & Liu, 2022; Giesler et al., 2017; He et al., 2020; Huang, Xuan, et al., 2024; Iannello et al., 2018; Lee et al., 2006; Lely et al., 2022; Liu et al., 2020; Liu et al., 2022; Lopez‐Olivo, Des Bordes, et al., 2021; Lopez‐Olivo, Lin, et al., 2021; McCaughan et al., 2013; Song & Cheng, 2023; Tian et al., 2024; Wang et al., 2025; Yang, 2022; Zarifsaniey et al., 2022; Zhang et al., 2022; Zheng et al., 2024; Zhou et al., 2020; Zhu, Jia, et al., 2024; Zhu, Chen, et al., 2024). The PRISMA flowchart (Figure 1) illustrates the search process.
PRISMA flow chart.
Characteristics of included studies
The relevant features of the included studies were shown in Table S2. This systematic and meta‐analysis included 34 RCTs involving patients with a variety of chronic conditions, most commonly cancer (nine trials), diabetes (nine trials), and stroke (three trials), alongside other conditions such as HIV, arthritis, chronic pain, and post‐traumatic stress disorder (PTSD). Sample sizes ranged from 10 to 670 participants, with a total of 4584 individuals. The age range was broad, spanning from adolescence (mean 12.54 ± 3.46 years) to older adulthood (mean 79.67 ± 9.03 years).
The studies were geographically diverse, with China contributing the largest number (n = 16), followed by the United States (n = 8) and Malaysia (n = 2). Additional studies were conducted in Australia, Canada, France, Germany, Iran, Italy, the Netherlands, and the United Kingdom (n = 1 each). Publication years ranged from 2006 to 2025, with 25 studies published after 2020, reflecting sustained and growing scholarly interest in this field.
Narrative‐based interventions encompass a wide range of approaches. On the one hand, technology‐enabled methods include digital storytelling, narrative websites, and message‐based narratives. On the other hand, structured therapeutic practices led by health‐care professionals employ techniques such as problem externalization, deconstruction, identity reconstruction, and the collaborative creation of alternative stories. Narrative Exposure Therapy has been primarily applied in trauma populations, whereas narrative care delivered by health‐care professionals integrates emotional support with individualized narrative reconstruction, representing a particularly prominent model in clinical practice.
Across the included studies, both self‐efficacy and self‐management were assessed using self‐report measures. In terms of self‐efficacy, the assessment tools can be categorized into three major types. The most widely used are disease‐specific self‐efficacy scales, such as the Diabetes Management Self‐Efficacy Scale (DMSES), the Strategies Used by People to Promote Health (SUPPH), the Arthritis Self‐Efficacy Scale (ASES), the Exercise Self‐Efficacy Scale, the Epilepsy Self‐Management Scale (ESMS), and the Chronic Disease Self‐Efficacy Scale (CSES). In addition, the General Self‐Efficacy Scale (GSES) is applied to assess overall confidence, while medication‐specific self‐efficacy scales, including the Self‐Efficacy for Appropriate Medication Use Scale (SEAMS) and the Medication Understanding and Use Self‐Efficacy Scale (MUSE), are used to evaluate medication‐related confidence and adherence.
For self‐management, commonly adopted tools include the Summary of Diabetes Self‐Care Activities Scale (SDSCA), the Exercise of Self‐Care Agency Scale (ESCA), and disease‐specific instruments such as the Liver Cirrhosis Self‐Management Scale. Moreover, some studies employed comprehensive self‐management scales encompassing multiple domains to evaluate patients' actual behaviors in daily life, symptom control, treatment adherence, and social adaptation.
Intervention durations ranged from a single session to 6 months. Most studies evaluated outcomes over the short term (immediately post‐intervention) or medium term (1–6 months), while only a limited number included long‐term follow‐up beyond 6 months. Seven studies specifically assessed the effects during the follow‐up period after the intervention.
Risk of bias in the included studies
A summary of the risk of bias in the included studies was shown in Figures 2 and S1. All 34 studies demonstrated a low risk of bias in random sequence generation (selection bias) and outcome reporting (reporting bias), suggesting that the quality control in these methodological domains was relatively robust. In contrast, there was a considerable risk of bias regarding allocation concealment and blinding of outcome assessment: five studies explicitly reported not using blinding, 30 studies did not specify whether outcome assessors were blinded, and 21 studies did not report on allocation concealment (selection bias). The absence or insufficiency of methodological reporting in these areas constituted the primary source of bias in this review.
Risk of bias summary for included studies.
Self‐efficacy
This meta‐analysis included 22 studies comprising a total of 3152 patients with chronic diseases (1526 in the intervention group and 1626 in the control group). As shown in Figure 3, narrative‐based interventions were found to significantly improve self‐efficacy (p < .001). However, according to the GRADE framework, the certainty of the evidence for this outcome was rated as low. Despite observed heterogeneity, most studies consistently reported improvements in self‐efficacy, and the overall effect remained positive. Nevertheless, because of small sample sizes and methodological limitations in some studies, the overall reliability of the evidence was limited. Moreover, subgroup analysis indicated that the intervention effect diminished over time, showing significant short‐term benefits but no significant long‐term effects (p > .05; see Figure S2).
Forest plot of self‐efficacy effects across 22 studies.
Self‐management
A meta‐analysis examining the effect of interventions on self‐management included 12 studies, with 458 participants in the intervention group and 453 in the control group. As shown in Figure 4, narrative‐based interventions significantly improved self‐management abilities in patients with chronic diseases (p < .001). However, substantial heterogeneity was observed across the studies. According to GRADE criteria, owing to this considerable heterogeneity and the potential risk of bias, the certainty of the evidence was rated as low.
Forest plot of self‐management effects across 12 studies.
Subgroup analysis of self‐efficacy effects
The subgroup analysis revealed that the impact of narrative‐based interventions on self‐efficacy was significantly moderated by national economic level, patient age, and disease type, whereas no significant differences were observed across groups in terms of intervention format or duration (Table 1). Moreover, the meta‐regression analysis shows that the effect of national income level on the effect size approaches statistical significance (p = .055), whereas other variables—such as type of self‐efficacy, age, and intervention format—are not significant independent predictors. Detailed meta‐regression results are provided in Table S3.
Subgroup analysis of self‐management effects
The subgroup analysis of the self‐management effect based on narrative‐based intervention revealed significant heterogeneity in intervention outcomes, requiring cautious interpretation (see Table 2). The findings indicated that intervention duration, intervention type, disease type, and publication year were associated with differences in intervention effects. However, no significant differences were observed across age groups. Although the subgroup analysis suggested that certain variables might be related to the intervention effect, the multivariate meta‐regression analysis—after further examining the independent predictive roles of these variables—found that age, disease type, intervention type, intervention duration, and publication year did not have significant predictive effects on the self‐management outcomes of narrative intervention (p > .05) (Table S4).
Publication bias and sensitivity analysis
Self‐efficacy
The funnel plot (Figure 5a) indicates that there may be some degree of publication bias because the distribution of points on both sides of the plot was not completely symmetric, and there were some outliers. According to Egger's test, no significant publication bias was found (t = 1.83, p = .082), which indicates that there was no obvious systematic bias. The leave‐one‐out sensitivity analysis revealed that excluding any single study resulted in combined effect sizes (SMD) ranging consistently from 0.55 to 0.71, closely aligning with the overall effect size (SMD = 0.66). Moreover, all corresponding confidence intervals excluded 0, indicating that the overall pooled effect size estimate was robust. Details were shown in Tables S5 and S7.
Funnel plot for studies on self‐efficacy and self‐management.
Self‐management
The funnel plot appeared asymmetrical (see Figure 5b), and Egger's test indicated potential publication bias (p = .007); however, meta‐analysis without imputing missing studies did not alter the combined effect size. Sensitivity analysis revealed that the overall conclusion was slightly influenced by individual studies, particularly Liu et al. (2020) and Zhang et al. (2022), with the combined effect size ranging from 1.33 to 1.91. Overall, despite minor indications of publication bias and slight dependence on specific studies, the evidence supports a positive effect of the intervention. Details were shown in Supplementary Table S6 and Table S8.
DISCUSSION
This systematic review and meta‐analysis examined the effects of narrative‐based interventions on self‐efficacy and self‐management in patients with chronic diseases. The findings showed that narrative‐based interventions significantly improved both outcomes; however, substantial heterogeneity was present across studies, and some results were sensitive to individual trials. Consequently, the certainty of the evidence is limited, and the conclusions should be interpreted with caution.
Effects of self‐efficacy
Narrative‐based interventions can significantly enhance the self‐efficacy of patients with chronic diseases. This supports the core mechanism whereby narratives promote cognitive reconstruction through role identification and emotional resonance (Georgiadis & Johnson, 2023; Gurney et al., 2023). However, the sustainability of these effects remains a key concern, which aligns with earlier findings indicating that narrative interventions primarily yield short‐ to mid‐term benefits (Georgiadis & Johnson, 2023). The emotional activation and immediate cognitive shifts elicited by narratives may naturally diminish without ongoing reinforcement. In addition, the disease experiences and psychological needs of patients with chronic illnesses are dynamic, and static narrative content may fail to align with their evolving life contexts, thereby compromising the stability of long‐term effects (Gucciardi et al., 2016). Despite this time‐dependent attenuation, the subgroup analysis (Table 1) found no significant differences across types of interventions, suggesting that narrative efficacy is driven more by shared cognitive–emotional mechanisms than by specific modes of delivery.
This systematic review and meta‐analysis also observed differences in the point estimates of effects across national income levels and disease types. National income level may reflect variations in health system structures, cultural contexts, medical accessibility, and patient needs, all of which could influence the adaptability and acceptability of narrative content in different settings (Abel et al., 2024; Metanmo et al., 2024; Naderbagi et al., 2024). For example, this numerical trend may be partially explained by the combination of limited systemic resources in upper‐ to middle‐income countries and high patient demand, where traditional health‐care systems often provide insufficient psychological and social support (Acharibasam & Wynn, 2018; Galagali & Brooks, 2020; Pham et al., 2020). In such settings narrative‐based interventions—being low‐cost and easy to implement—may be more appealing (Loy & Kowalsky, 2024; Ranjit et al., 2015), whereas in high‐income countries with diverse cultures and complex health‐care systems, insufficient cultural adaptation of narrative materials may attenuate their effectiveness (Larkey & Hecht, 2010; Murphy et al., 2013). Similarly, higher point estimates were observed among patients with severe chronic conditions, possibly because of their greater psychological needs, more complex self‐management demands, and heightened perceptions of health threats, which may enhance emotional resonance with narrative content (Lévai et al., 2024).
Effects of self‐management
Compared with self‐efficacy, the overall effect of narrative‐based interventions on self‐management behaviors was larger, yet the heterogeneity among studies was extremely high. This suggests that behavioral change is inherently more complex than psychological perception, with outcomes shaped by both contextual factors and individual‐level differences. Although the pooled effect was statistically significant, the substantial heterogeneity indicates that the findings should be interpreted with caution.
The subgroup analysis indicated that multiple study characteristics significantly moderated the effects of narrative‐based interventions on self‐management. First, intervention type emerged as the most critical influencing factor. Interpersonal narrative interventions showed the strongest effect, suggesting a stable and reliable impact. This advantage may stem from the immediate social feedback and stronger emotional resonance inherent in interactive contexts, which can enhance participants' engagement and meaning‐making processes (Kleinbub et al., 2020). In contrast, digital storytelling and writing narratives did not demonstrate significant effects, indicating that narrative formats lacking interactive components may have limited influence on self‐management, and their underlying mechanisms warrant further investigation (Perski et al., 2017).
Second, the duration of intervention differed significantly across subgroups, showing a clear “U‐shaped” pattern: both short‐term interventions (≤1 month) and long‐term interventions (≥6 months) yielded large effect sizes, whereas medium‐term interventions (2–3 months) showed markedly attenuated effects. This suggests that narrative interventions may exert strong early effects through emotional activation and motivational priming, while long‐term benefits may stem from sustained exposure and repeated meaning reconstruction. In contrast, a temporary “effect plateau” may emerge during the medium‐term period (Oschatz & Marker, 2020).
Moreover, this effect is observed across various disease types; its magnitude may differ, potentially reflecting variations in how different conditions influence patients' self‐identity and the depth of emotional resonance elicited by the narrative content (Lévai et al., 2024). Publication year also acted as a moderating factor. Subgroup analysis revealed temporal variations, with more recent studies (2021–2025) generally reporting stronger effect sizes compared with earlier studies (2015–2020). This trend may reflect improvements in intervention design and implementation quality over time. Additionally, age did not serve as a significant moderator, suggesting that the core mechanisms of narrative interventions—grounded in stories that evoke emotional and cognitive processing—may be universally effective across age groups.
Analysis of the potential sources of heterogeneity
The meta‐regression analysis indicated that all the preset variables did not emerge as significant independent predictors after controlling for other factors, contrasting with some significant inter‐group differences observed in the subgroup analysis. This inconsistency may reflect the synergistic, multi‐factorial nature of narrative intervention effects, where the independent contribution of a single variable is diluted by complex interactions. It also highlights the potential role of unmeasured key moderators, such as the quality of narrative content, cultural adaptability, patient engagement, and immersion. Furthermore, given the limited number of included studies, the statistical power of the meta‐regression may be insufficient, representing an area for improvement in future research.
Although the funnel plot and Egger test suggested the possibility of publication bias (especially in self‐management outcomes), the leave‐one‐out sensitivity analysis indicated that the combined results were highly robust. The consistency of self‐efficacy improvement was relatively high, while self‐management outcomes were more sensitive to individual studies, such as Liu et al. (2020) and Zhang et al. (2022), indicating that behavioral transformation may be more influenced by situational and individual factors compared to psychological perception.
Strengths and limitations
The strength of this study lies in its systematic inclusion of multiple RCTs and its simultaneous evaluation of two key outcomes—self‐efficacy and self‐management behavior. This approach provides a comprehensive overview of the evidence regarding narrative interventions in chronic disease management. The study adhered rigorously to methodological standards for systematic review and meta‐analysis, incorporating multiple layers of sensitivity and subgroup analyses to enhance the transparency and robustness of the findings.
However, this systematic review and meta‐analysis also has several limitations. The methodological quality of the included trials varies considerably, with many failing to report essential details such as randomization procedures, allocation concealment, and blinding. In addition, substantial heterogeneity exists across studies, likely stemming from variations in intervention content, implementation fidelity, and outcome measurement tools. Finally, most studies were conducted within similar cultural contexts, which limits the cross‐cultural generalizability of the findings.
Future research directions
Future research should focus on enhancing the scientific rigor and clinical translational value of narrative‐based interventions and directly address the main limitations identified in this review, including variable methodological quality, insufficient intervention standardization, lack of mechanism‐focused variables, and short follow‐up periods. A primary task is to improve methodological quality and reporting transparency. Future studies should rigorously adhere to guidelines such as CONSORT, comprehensively report key aspects including randomization, blinding, and implementation processes, and provide standardized descriptions of intervention content and procedures. Core elements—such as narrative material development, cultural adaptation, storytelling methods, and interaction structures—should be systematically reported, and scalable intervention frameworks should be explored.
In addition, research should move beyond demographic variables to investigate process‐related factors, including narrative quality, emotional immersion, and patient engagement. Both theoretical and empirical studies indicate that highly immersive narratives enhance cognitive and emotional involvement, thereby facilitating behavioral change (Oschatz & Marker, 2020; Shaffer et al., 2018). Mixed‐methods and multi‐level designs can help elucidate the mechanisms of intervention and identify the populations for whom they are most effective. Furthermore, cross‐cultural and cross‐disease multi‐center studies are needed, with particular attention to applicability in disadvantaged groups and resource‐limited settings. Intervention designs should incorporate longer follow‐up periods and dynamic assessment strategies to capture the nonlinear trajectory of narrative effects. Digital innovations can also be integrated to enhance interactivity, immersion, and personalized adaptation, exploring novel intervention formats, such as virtual reality and artificial intelligence‐based narrative assistants, thereby optimizing both effectiveness and accessibility.
CONCLUSION
This systematic review and meta‐analysis indicate that narrative‐based interventions can improve the self‐efficacy and self‐management behaviors of patients with chronic diseases. The evidence shows that their effect on self‐efficacy is significant but may be more limited to the short term, whereas their effect on self‐management is larger yet highly variable and influenced by intervention type and duration. However, these conclusions are constrained by several important factors. The overall quality of evidence is low, with major limitations including substantial heterogeneity across studies, methodological weaknesses in the original trials, and a potential risk of publication bias—particularly for self‐management outcomes. Therefore, the current findings should be interpreted with caution. Narrative‐based interventions, as an adjunct strategy for chronic disease management, demonstrate promising clinical potential, especially when delivered in an interactive format and supported by sustained engagement. To translate this potential into robust clinical practice, future research must prioritize methodological rigor, investigate underlying mechanisms of action, and develop dynamic, personalized, and culturally responsive intervention models.
CONFLICT OF INTEREST STATEMENT
No potential conflict of interest was reported by the authors.
FUNDING INFORMATION
The authors reported that there is no funding associated with the work featured in this article.
Systematic Review Register (PROSPERO).
CRD42023413162.
ETHICS STATEMENT
This study is a systematic review and meta‐analysis of previously published literature and does not involve direct contact with human or animal subjects. Therefore, ethical approval was not required.
Supporting information
Table S1. Search strategies. Table S2. Characteristics of Included Studies. Table S3. Summary of meta‐regression results. Table S4. Results of leave‐one‐out method in sensitivity analysis. Table S5. Results of leave‐one‐out method in sensitivity analysis. Figure S1. Risk of Bias Assessment of 34 Included Studies. Figure S2. Egger's Test for Publication Bias in a Meta‐Analysis for Self‐Efficacy. Figure S3. Egger's Test for Publication Bias in a Meta‐Analysis for Self‐Management.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Abel, Z. D. V. , Roope, L. S. J. , Duch, R. , & Clarke, P. M. (2024). Access to healthcare services during the COVID‐19 pandemic: A cross‐sectional analysis of income and user‐access across 16 economically diverse countries. BMC Public Health, 24(1), 2678. 10.1186/s 12889-024-20147-y 39350210 PMC 11443786 · doi ↗ · pubmed ↗
- 2Acharibasam, J. W. , & Wynn, R. (2018). Telemental health in low‐ and middle‐income countries: A systematic review. International Journal of Telemedicine and Applications, 2018, 1–10). Hindawi Publishing Corporation. 10.1155/2018/9602821 PMC 624137530519259 · doi ↗ · pubmed ↗
- 3Anderson, E. , & Durstine, J. L. (2019). Physical activity, exercise, and chronic diseases: A brief review. Sports Medicine and Health Science, 1(1), 3–10. 10.1016/j.smhs.2019.08.006 35782456 PMC 9219321 · doi ↗ · pubmed ↗
- 4Andreae, S. J. , Andreae, L. J. , Cherrington, A. L. , Richman, J. S. , Johnson, E. , Clark, D. , & Safford, M. M. (2021). Peer coach delivered storytelling program improved diabetes medication adherence: A cluster randomized trial. Contemporary Clinical Trials, 104, 106358. 10.1016/j.cct.2021.106358 33737200 · doi ↗ · pubmed ↗
- 5Appalasamy, J. R. , Joseph, J. P. , Seeta Ramaiah, S. , Md Zain, A. Z. , Quek, K. F. , & Tha, K. K. (2020). Video narratives intervention among stroke survivors: Feasibility and acceptability study of a randomized controlled trial. JMIR Aging, 3(2), e 17182. 10.2196/17182 32469839 PMC 7382013 · doi ↗ · pubmed ↗
- 6Appalasamy, J. R. , Quek, K. F. , Md Zain, A. Z. , Joseph, J. P. , Seeta Ramaiah, S. , & Tha, K. K. (2020). An evaluation of the video narrative technique on the self‐efficacy of medication understanding and use among post‐stroke patients: A randomized‐controlled trial. Patient Preference and Adherence, 14, 1979–1990. 10.2147/PPA.S 253918 33116441 PMC 7585263 · doi ↗ · pubmed ↗
- 7Bandura, A. (1977). Self‐efficacy: Toward a unifying theory of behavioral change. Psychological Review, 84(2), 191–215.847061 10.1037//0033-295x.84.2.191 · doi ↗ · pubmed ↗
- 8Bandura, A. (1989). Human agency in social cognitive theory. American Psychologist, 44(9), 1175–1184. 10.1037/0003-066x.44.9.1175 2782727 · doi ↗ · pubmed ↗