The effect of two remote exercise programs on cardiorespiratory fitness, cardiac function, and vascular health in patients with breast cancer
Nathan R. Weeldreyer, Charles C. Ellison, Mckenzie B. Mabalot, Cheyanne E. Helms, Zachariah B. Nealy, Zachary S. Leicht, Antonio Abbate, Christiana M. Brenin, Patrick M. Dillon, Trish Millard, Rebecca A. Krukowski, Jamie M. Zoellner, Siddhartha S. Angadi

TL;DR
This study compared two remote exercise programs for breast cancer patients and found that high-intensity interval training better preserved cardiorespiratory fitness during chemotherapy.
Contribution
The novel contribution is demonstrating that remote high-intensity interval training preserves VO2peak in breast cancer patients undergoing chemotherapy.
Findings
VO2peak declined in moderate-intensity group but remained stable in high-intensity group
NTproBNP levels increased significantly in moderate-intensity group but not in high-intensity group
Abstract
Breast cancer is a common, survivable malignancy affecting women. With improved survival, the off‐target effects of chemotherapy, such as a decline in cardiorespiratory fitness and worse cardiovascular outcomes, have been recognized. Exercise training may help mitigate these effects. In this study, patients with breast cancer (N = 24) scheduled to undergo chemotherapy were randomized to either remotely administered high‐intensity interval training (HIIT) or moderate‐intensity exercise (MOD) based on ACSM guidelines for cancer survivors. HIIT involved three weekly sessions using the 4 × 4 protocol at 85%–90% peak heart rate (PHR), while MOD consisted of 150 min per week at 70%–75% PHR. Exercise training began 1–2 weeks before chemotherapy and continued throughout treatment. Baseline testing was conducted prior to chemotherapy and follow‐up testing 7–10 days after completion. Assessments…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
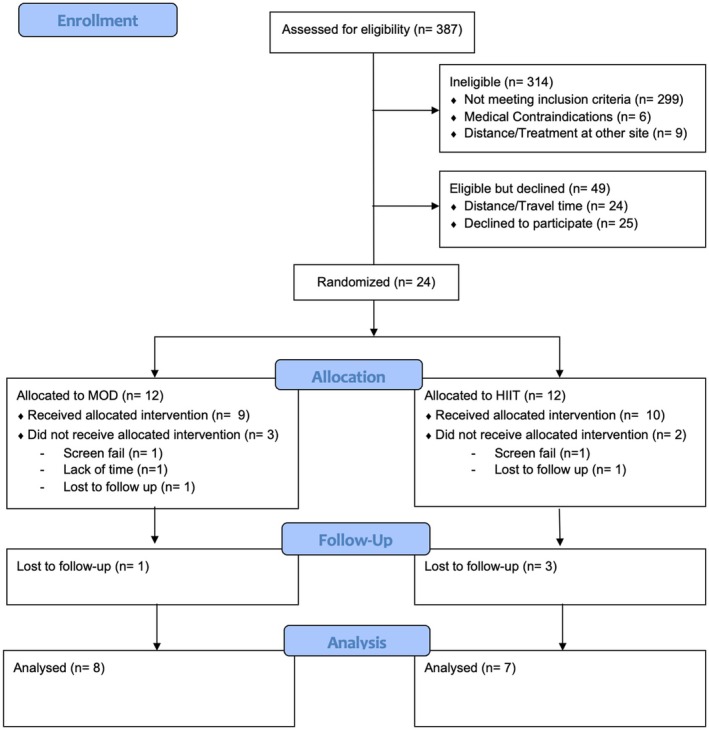 FIGURE 1
FIGURE 1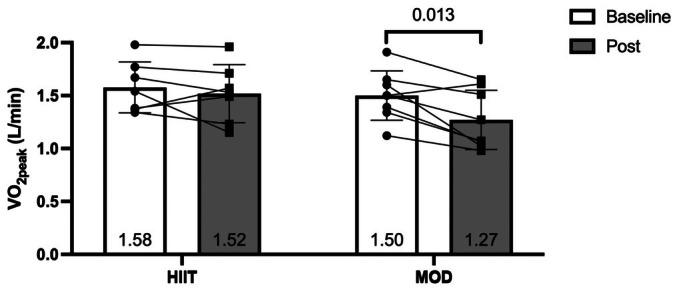 FIGURE 2
FIGURE 2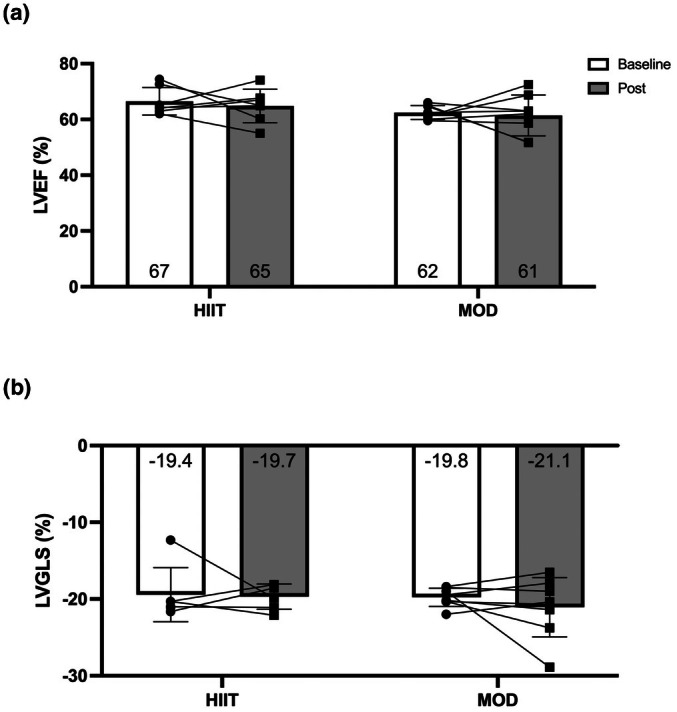 FIGURE 3
FIGURE 3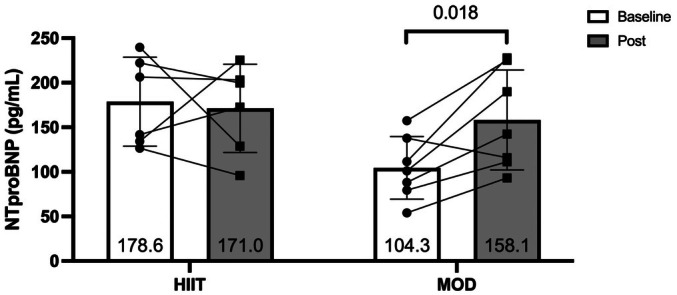 FIGURE 4
FIGURE 4| MOD ( | HIIT ( |
| |
|---|---|---|---|
| Age | 52.6 ± 11.2 | 55.3 ± 11.9 | 0.663 |
| Weight (kg) | 67.2 ± 9.1 | 78.7 ± 15.0 | 0.093 |
| BMI | 26.0 ± 4.9 | 28.9 ± 5.5 | 0.307 |
| VO2peak (L/min) | 1.50 ± 0.23 | 1.58 ± 0.24 | 0.539 |
| Ejection fraction (%) | 62.5 ± 2.5 | 67.5 ± 5.6 | 0.047 |
| Race | |||
| White | 8 | 4 | |
| Black/African American | 0 | 3 | |
| Breast cancer staging | |||
| Stage I | 3 | 3 | |
| Stage II | 5 | 3 | |
| Stage III | 0 | 1 | |
| Receptor status | |||
| ER and/or PR positive | 3 | 4 | |
| HER2 positive, ER, and PR negative | 1 | 0 | |
| HER2 and ER and/or PR positive | 0 | 2 | |
| Triple negative | 3 | 1 | |
| Chemotherapy regimen | |||
| Doxorubicin + Cyclophosphamide | 4 | 4 | |
| Docetaxel + Cyclophosphamide | 2 | 1 | |
| Paclitaxel + Trastuzumab | 1 | 2 | |
| Keynote522 | 1 | 0 | |
| MOD | HIIT | Between‐group | |||||
|---|---|---|---|---|---|---|---|
| Pre | Post |
| Pre | Post |
|
| |
| VO2peak (L/min) | 1.50 ± 0.23 | 1.27 ± 0.28 | 0.013 | 1.58 ± 0.24 | 1.52 ± 0.28 | 0.445 | 0.109 |
| VO2peak (mL/kg/min) | 22.6 ± 2.5 | 19.0 ± 4.3 | 0.021 | 20.7 ± 5.2 | 19.4 ± 4.3 | 0.167 | 0.151 |
| Peak power output (watts) | 110 ± 21 | 97 ± 28 | 0.089 | 125 ± 15 | 122 ± 27 | 0.625 | 0.319 |
| %VO2 at VT | 70.5 ± 8.5 | 82.6 ± 13.4 | 0.133 | 69.8 ± 4.9 | 73.2 ± 8.0 | 0.277 | 0.298 |
| VE/VO2 slope | 45.5 ± 7.9 | 55.4 ± 17.0 | 0.119 | 48.7 ± 9.1 | 51.0 ± 13.2 | 0.553 | 0.254 |
| VE/VCO2 slope | 31.6 ± 5.1 | 34.6 ± 8.3 | 0.19 | 33.2 ± 2.7 | 35.6 ± 4.8 | 0.12 | 0.86 |
| OUES | 1.63 ± 0.27 | 1.29 ± 0.26 | 0.002 | 1.57 ± 0.20 | 1.42 ± 0.23 | 0.15 | 0.14 |
| MOD | HIIT | Between‐group | |||||
|---|---|---|---|---|---|---|---|
| Pre | Post |
| Pre | Post |
|
| |
| Ejection Fraction (%) | 62.5 ± 2.5 | 61.4 ± 7.3 | 0.749 | 67.5 ± 5.6 | 62.6 ± 5.0 | 0.198 | 0.427 |
| LV GLS (%) | −19.8 ± 1.2 | 21.1 ± 3.9 | 0.674 | −19.11 ± 3.8 | −20.0 ± 1.7 | 0.893 | 0.622 |
| E/A | 1.18 ± 0.28 | 1.22 ± 0.50 | 0.699 | 1.4 ± 0.4 | 0.99 ± 0.3 | 0.081 | 0.059 |
| Deceleration time (ms) | 184 ± 41 | 176 ± 47 | 0.741 | 156 ± 60 | 175 ± 28 | 0.450 | 0.422 |
| e′ (cm/s) | 11.08 ± 2.51 | 10.66 ± 3.21 | 0.549 | 9.99 ± 2.87 | 8.33 ± 1.92 | 0.043 | 0.206 |
| E/e′ | 7.40 ± 1.70 | 7.95 ± 1.96 | 0.503 | 8.04 ± 2.21 | 9.17 ± 4.30 | 0.317 | 0.664 |
| LAVI (mL/m2) | 18.8 ± 8.2 | 23.1 ± 8.6 | 0.549 | 18.9 ± 9.4 | 28.6 ± 8.6 | 0.247 | 0.594 |
| SV (mL) | 64 ± 13 | 59 ± 19 | 0.487 | 65 ± 13 | 71 ± 15 | 0.270 | 0.224 |
| Heart rate (BPM) | 75 ± 6 | 80 ± 13 | 0.343 | 66 ± 9 | 77 ± 14 | 0.087 | 0.440 |
| CO (L/min) | 4.8 ± 1.0 | 4.7 ± 1.7 | 0.889 | 4.3 ± 1.1 | 5.3 ± 1.0 | 0.004 | 0.097 |
| MOD | HIIT | Between‐group | |||||
|---|---|---|---|---|---|---|---|
| Pre | Post |
| Pre | Post |
|
| |
| SBP (mmHg) | 120 ± 6 | 116 ± 6 | 0.067 | 131 ± 14 | 132 ± 11 | 0.806 | 0.206 |
| DBP (mmHg) | 78 ± 2 | 74 ± 6 | 0.135 | 79 ± 8 | 81 ± 9 | 0.405 | 0.099 |
| cSBP (mmHg) | 111 ± 4.9 | 104 ± 4 | 0.008 | 121 ± 14 | 122 ± 12 | 0.859 | 0.099 |
| cDBP (mmHg) | 78 ± 2 | 74 ± 6 | 0.093 | 80 ± 7 | 82 ± 9 | 0.356 | 0.073 |
| Aix (%) | 29.0 ± 13.2 | 20.8 ± 13.2 | 0.062 | 31.6 ± 6.9 | 31.5 ± 11.0 | 0.979 | 0.106 |
| Aix75 (%) | 26.4 ± 9.9 | 22.6 ± 9.4 | 0.027 | 26.2 ± 8.0 | 28.2 ± 10.7 | 0.402 | 0.040 |
| PWV (m/s) | 6.5 ± 0.8 | 6.1 ± 1.2 | 0.187 | 6.98 ± 0.61 | 6.64 ± 1.3 | 0.403 | 0.968 |
| FMD (%) | 12.2 ± 5.7 | 9.4 ± 2.9 | 0.378 | 9.9 ± 4.9 | 7.0 ± 3.9 | 0.063 | 0.979 |
- —UVA Cancer Center (Cancer Center)10.13039/100017397
- —UVA Imaging, and Informatics in Precision Immunomedicine (iPRIME) Initiative
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChemotherapy-induced cardiotoxicity and mitigation · Cancer survivorship and care · Cardiovascular and exercise physiology
INTRODUCTION
1
Breast cancer is one of the most common types of cancer amongst women, with a lifetime risk of 1 in 8 women, and it is the second leading cause of cancer death (National Cancer Institute, 2025). With advancements in treatments, the survival rate for breast cancer continues to improve, with 5‐year survival rates exceeding 90% (American Cancer Society, 2025). Treatment for Stages I–IV breast cancer commonly involves systemic chemotherapy with a range of agents. As a result of increased survival, the off‐target effects of chemotherapy are becoming increasingly appreciated in breast cancer survivors (Kirkham et al., 2019). Off‐target effects include reduced quality of life (QoL), increased fatigue, reduced functional capacity (VO_2peak_), as well as cardiac, vascular, and skeletal muscle toxicity (Dickinson et al., 2017; Given et al., 2001; Lenneman & Sawyer, 2016; Mclaughlin et al., 2021; Sweeney et al., 2006). In fact, older breast cancer survivors are more likely to die from cardiovascular disease than from breast cancer (Patnaik et al., 2011).
These adverse effects are well known, and a significant amount of research has examined various ways exercise can be used to improve health in survivors (Speck et al., 2010). However, fewer studies have investigated how exercise during chemotherapy treatment can be used to preserve health. The recent BREXIT trial (Foulkes et al., 2023) demonstrated that cardiorespiratory fitness and cardiac reserve improved with a supervised exercise training program that transitioned to unsupervised exercise compared to usual care (recommendations to perform 150 min of moderate‐intensity exercise per week) during anthracycline‐based treatment in women with breast cancer. However, the study may be difficult to generalize and scale due to the supervision of exercise training during chemotherapy, which can be challenging for populations with low access to healthcare resources as well as a higher burden on health system resources. Rehabilitation referral rates and adherence are low for survivors of cancer (Hardcastle et al., 2018) in part due to poor access opportunities and lack of insurance coverage making them unaffordable. In‐person exercise rehabilitation is especially challenging for patients living in low‐resource rural environments.
The primary aim of this trial was to examine the feasibility and retention rate of conducting a fully remote exercise program for two exercise interventions: high intensity interval training (HIIT) vs. moderate intensity training (MOD) in women with breast cancer undergoing chemotherapy treatment (Helms et al., 2026). However, our secondary aim was to examine the effect of these remote interventions on important physiological outcomes such as cardiorespiratory fitness and cardiac function.
Exercise intensity plays an important role in the adaptations to VO_2peak_ and cardiac function seen following training in healthy volunteers without cancer (MacInnis & Gibala, 2017; Wisloff et al., 2009). However, data on the role of exercise intensity in patients with breast cancer undergoing active chemotherapy for preservation of VO_2peak_ is not well developed. Thus, the purpose of the current report was to compare these two remote interventions in attenuating reductions in cardiorespiratory fitness, cardiac function, and vascular function when initiated prior to and continued throughout chemotherapy treatment. We hypothesized that those randomized to the HIIT intervention would see a greater preservation of measures compared to those in the MOD intervention.
MATERIALS AND METHODS
2
Participants and study design
2.1
Patients enrolled for this study were recruited from the Breast Care Center at the University of Virginia Comprehensive Cancer Center. Eligible patients were those greater than 18 years old, had a breast cancer diagnosis (stages I–III or IV with minimal metastatic disease burden), spoke English, were given physician clearance for exercise training, and were prescribed one of the following chemotherapy regimens: Docetaxel/Cyclophosphamide (TC), Doxorubicin/Cyclophosphamide (AC), Docetaxel/Carboplatin/Trastuzumab/Pertuzumab (TCHP), Docetaxel/Carboplatin/Trastuzumab (TCH), or Pembrolizumab/Paclitaxel/Carboplatin followed by Pembrolizumab/Doxorubicin/Cyclophosphamide (KEYNOTE522 (Schmid et al., 2020)). Potential patients were excluded from the study if they had: (1) previous treatment with cardiotoxic chemotherapy; (2) clinically significant cardiac, renal, hepatic, hematologic, or pulmonary disease precluding exercise testing and training; (3) unstable angina or myocardial infarction within 4 weeks prior to treatment; (4) complex ventricular arrhythmias or New York Heart Association class IV symptoms; (5) symptomatic severe aortic stenosis; (6) recent pulmonary embolus; (7) acute myocarditis; (8) untreated high‐risk proliferative retinopathy; (9) recent retinal hemorrhage; (10) uncontrolled hypertension (systolic blood pressure >180 mm Hg or diastolic blood pressure >120 mm Hg); (11) severe baseline electrolyte abnormalities; (12) medication non‐compliance; (13) uncontrolled metabolic disease (diabetes with fasting blood sugar >300 mg/dL, thyrotoxicosis, myxedema); (14) or symptomatic peripheral vascular disease. This study was approved by the institutional review board at the University of Virginia and conducted in accordance with the Declaration of Helsinki. All patients provided written informed consent before partaking in any study procedures. This study was prospectively registered on clinicaltrials.gov (NCT05786014).
Exercise interventions
2.2
Patients were randomized into one of two exercise interventions: (1) high‐intensity interval training (HIIT) using a stationary, recumbent bicycle; (2) moderate‐intensity exercise (MOD) based on ACSM guidelines for cancer survivors which are similar to those used in the BREXIT trial (Foulkes et al., 2023) with remote monitoring. Exercise interventions were performed in an unsupervised, remote manner following two initial in‐person training sessions. Patients were given a smartwatch (Unite, Polar Electro, Finland) as well as a heart rate strap (H10, Polar Electro, Finland) in order to track their workouts and monitor heart rates throughout their exercise sessions. In addition, these data were uploaded and tracked via cloud‐based software (Polar Flow) for each patient. This allowed for real‐time data tracking and the delivery of personalized text messages throughout the intervention based on participants' current adherence. Patients randomized to the HIIT group were instructed to perform exercise sessions 3 days per week. Each session consisted of four 4‐min intervals at 85%–90% PHR separated by 3 min of active recovery at ~50% PHR. Sessions started with a 10‐min warmup and ended with a 5‐min cool down at ~50% PHR. In addition, patients were allowed to perform eight 2‐min intervals with 2‐min recovery, or five 3‐min intervals with 3‐min recovery as alternative options if they felt unable to complete the 4 × 4 protocol. Patients in the MOD group were asked to accumulate 150 min a week of moderate to vigorous physical activity via walking at 70%–75% of PHR in accordance with current American College of Sports Medicine Guidelines for patients with cancer (American College of Sports Medicine et al., 2021). Participants were allowed to exercise in bouts that added up to 150‐min/week in any way they liked.
To minimize barriers to exercise, participants in the HIIT group had recumbent bikes delivered and assembled in their homes, and those in the walking group were given gift cards to purchase running shoes. Interventions were guided by Social Cognitive Theory and evidence‐based behavioral change techniques (goal setting, action planning, problem solving, feedback, and self‐monitoring) (Helms et al., 2026). Patients in both groups attended two in‐person familiarization sessions to learn how to use the equipment, demonstrate proficiency in using them, and familiarize themselves with their exercise intensities. To support the participants' goals and adherence, the intervention also included one telephone‐based core session, personalized short message services (SMS), and telephone‐based stepped care sessions for problem solving. To monitor reasons for nonadherence, one SMS was sent out each week if exercise goals were not met, in which participants could choose from the following reasons: (1) chemotherapy side effects, (2) lack of time, (3) depression, (4) other, and (5) weather (MOD only).
Maximal exercise testing
2.3
All baseline testing occurred between 1 and 2 weeks prior to the initiation of chemotherapy. Post testing occurred 7–10 days following the last chemotherapy infusion. Cardiorespiratory fitness was assessed via maximal cardiopulmonary exercise tests. VO_2peak_ was determined by a ramp protocol conducted on a recumbent cycle ergometer (Ergoselect 600, Ergoline, Germany). Cycle ergometry was chosen over a treadmill in order to reduce potential discomfort associated with palmo‐plantar dysesthesia, a common side effect associated with chemotherapies (Kwakman et al., 2020). In addition, a recumbent ergometer was selected to reduce the strain on surgical sites that may come from the use of an upright ergometer. Following 2 min of resting data collection, a 5‐min warmup at 25 watts was performed. A ramp protocol was performed such that following the warmup the resistance continuously increased by 15 watts/min. Cadence was kept steady between 60 and 65 RPMs. Gas exchange data was collected as breath‐by‐breath data on the Vyntus CPX metabolic cart (Vyaire, Mettawa, IL). Continuous 12‐lead EKG was monitored throughout the test to measure heart rate and rhythm (CardioSoft, Vyaire, Mettawa, IL). VO_2peak_ was calculated as the average of the two highest VO_2_ values during the test. Peak heart rates obtained from this test were used to inform exercise prescriptions used in the intervention. In addition, ventilatory efficiency slopes (VE/VCO_2_ and VE/VO_2_) were calculated from the lines of best fit from the ramp portion of the exercise test. Oxygen uptake efficiency slope (OUES) was derived from plotting VO_2_ and log_10_VE (Baba et al., 1996).
Echocardiograms
2.4
Transthoracic echocardiograms (TTEs) were performed by trained sonographers following American Society of Echocardiography guidelines (ASE) (Mitchell et al., 2019) and read by cardiologists who were blinded to study allocation. Standard parasternal long and short axis views, apical 4 and 2 chambers views, apical long axis, and subcostal views were obtained. Main outcome measures included measures of left ventricular (LV) function and diastology. Specifically, systolic function was assessed using Simpson's biplane to determine LV ejection fraction (LVEF), 2‐dimensional speckle tracking was used to calculate LV global longitudinal strain (LVGLS) from apical 2, 4 and long axis views. In addition, cardiac output (CO) was estimated by multiplying heart rate by the product of the left ventricular outflow tract (LVOT) area and LVOT velocity (Zhang et al., 2019). LV diastology was assessed using mitral inflow velocities (E and A waves), mitral valve annular velocities (e′), tricuspid valve regurgitation velocity (TR VMAX), and left atrial volume index (LAVI). Values from these were used to calculate diastolic dysfunction (DD) grade based on ASE guidelines (Nagueh et al., 2016). Any missing values from the echocardiogram reports were calculated utilizing commercially available software (AGFA Enterprise Imaging) by a blinded member of the study team.
Flow mediated dilation
2.5
Endothelial function was measured via flow mediated dilation (FMD) of the brachial artery using 2‐dimensional and doppler ultrasound (EPIQ 7, Philips, Andover, MA or a usmart3300 ultrasound, Terason Ultrasound, Burlington, MA). FMDs were performed in accordance with current expert consensus recommendations (Thijssen et al., 2019) and as previously described (Tucker et al., 2021). Videos were analyzed within Vascular Tools 5 (Medical Imaging Applications, Coralville, Iowa).
Central hemodynamics
2.6
Both pulse wave analysis (PWA) and pulse wave velocity (PWV) were measured using the SphygmoCor Xcel system (AtCor Medical, Sydney, New South Wales, Australia). Data were collected as previously described (Tucker et al., 2021). Three trials were performed, and the two closest data points were averaged to obtain brachial and central blood pressure, augmentation pressure (AP), augmentation index (Aix), and augmentation index corrected for a heart rate of 75 bpm (Aix75).
Serum biomarkers
2.7
At baseline and post testing, blood samples were collected from the antecubital fossa or from an in‐dwelling port following an overnight fast. Samples were drawn into Ethylenediaminetetraacetic (EDTA) and serum separator tubes, centrifuged, and immediately stored in a −80°C freezer until analysis. In addition, standard of care blood draws were collected at the initial and final chemotherapy infusion visits via indwelling catheter, and an accredited laboratory was used to analyze changes in patient blood counts.
Stored samples were used to analyze markers of inflammation and cardiac damage via multiplex ELISA (MAGPIX, Luminex, Austin, TX). Specifically, we measured interleukin (IL)‐1β, IL‐6, and tumor necrosis factor (TNF) (HADK2MAG‐61K‐04 Millipore Sigma); N‐terminal prohormone of brain natriuretic peptide (NTproBNP) (HCVD1MAG‐67K‐01 Millipore Sigma); and C‐Reactive Protein (CRP) (HCVD3MAG‐67K‐01 Millipore Sigma) in accordance with manufacturer's instructions. Serum samples were run in duplicate, and trials with a greater than 20% coefficient of variance were excluded and rerun if necessary. In addition, samples with less than 70% recovery or greater than 130% recovery were also excluded per manufacturer recommendations. The average of all runs meeting the above criteria was used in the final analysis.
Statistical analysis
2.8
Statistical analyses were performed using SPSS Statistics v29.0.2.0 (IBM Armonk, NY). Independent samples t‐tests were used to assess for differences between groups at baseline. Changes (Delta) following intervention were calculated as post minus pretesting values. Normality of the deltas from pre‐ and post‐testing was assessed via Shapiro‐Wilks tests. To examine for between‐group differences, independent samples t‐tests were used to compare deltas between both groups for all outcome measures. In addition, paired samples t‐tests were run to assess for changes within‐group from pre‐ to post‐intervention. For measures that were not normally distributed, Wilcoxon‐signed rank tests and Mann–Whitney U‐tests were used. As this was a pilot study aimed to generate effect sizes to inform a large‐scale future trial, Cohen's d effect sizes were also calculated to examine the magnitude of effect from each study intervention. Data are presented as mean ± SD unless otherwise noted. Alpha was a priori set to 0.05.
RESULTS
3
Subject characteristics
3.1
As shown in Figure 1, 24 patients consented and enrolled in the trial, and 15 patients completed all aspects of the study protocol (HIIT: n = 7, MOD: n = 8). Baseline characteristics and breast cancer treatments are presented in Table 1. At baseline, there was a significant between‐group difference in ejection fraction (HIIT: 67.5 ± 5.6% vs. MOD: 62.5 ± 2.5%, p = 0.047). No other differences were observed at baseline. While similar, due to different chemotherapy regimens the intervention duration for HIIT was 10.6 ± 3.8 weeks and 13.0 ± 6.2 weeks for MOD (p = 0.374). This difference was largely driven by one patient on the KEYNOTE522 therapy (which lasts 24 weeks).
Prisma flow diagram of study recruitment and retention.
Exercise adherence
3.2
Patient adherence to the exercise programs was similar between the two arms: 61 ± 32% for HIIT and 64 ± 37% for MOD, respectively (p = 0.868). Principle cause of exercise noncompliance was chemotherapy related side‐effects. Full adherence data can be found elsewhere (Helms et al., 2026). No significant correlations were observed for exercise adherence and the delta of any primary outcome measure when assessed across groups (all p > 0.05).
Cardiorespiratory fitness
3.3
Those in the MOD group experienced a significant reduction in VO_2peak_ of 0.23 L/min from pre‐ to postintervention (1.50 ± 0.23 to 1.27 ± 0.28 L/min; p = 0.013, d = 1.2). In contrast, those in the HIIT group saw a nonsignificant reduction of 0.06 L/min (1.58 ± 0.24 to 1.52 ± 0.28 L/min; p = 0.445, d = 0.3) (Figure 2). While not statistically significant, the between‐group differences showed a large effect size (p = 0.109, d = 0.9). This resulted in a trend for reduction in peak power output in the MOD group (Table 2). Additionally, there were no significant within‐ or between‐group differences in VE/VCO_2_ slope (MOD: 31.6 ± 5.1 to 34.6 ± 8.3; p = 0.19, d = 0.5, HIIT: 33.2 ± 2.7 to 35.6 ± 4.8; p = 0.12, d = 0.7; between‐group: p = 0.86, d = 0.1). Of note, at the end of the trial, both groups had mean VE/VCO_2_ slopes >34, which is often used as a threshold beyond which patients with heart failure have worse outcomes (Myers et al., 2008). There was a significant reduction in OUES for MOD from pre‐ to post‐testing that did not occur in the HIIT group. While not significant, a large effect size for between‐group differences was observed (MOD: 1.63 ± 0.27 to 1.29 ± 0.26 L/min; p = 0.002, d = 2.5, HIIT: 1.57 ± 0.20 to 1.42 ± 0.23 L/min; p = 0.15, d = 0.6; between‐group: p = 0.14, d = 0.9).
Changes in absolute VO2peak following exercise training while undergoing chemotherapy treatment.
Cardiac function
3.4
In assessing systolic function, no significant reductions were seen in ejection fraction (MOD: 62.5 ± 2.5% to 61.4 ± 7.3%; p = 0.749, d = 0.1, HIIT: 67.5 ± 5.6% to 62.6 ± 5.0%; p = 0.198, d = 0.7; between‐group: p = 0.427, d = 0.5) or in LVGLS (MOD: −19.8 ± 1.2% to −21.1 ± 3.9%; p = 0.380, d = 0.3, HIIT: −19.11 ± 3.8% to −20.0 ± 1.7%; p = 0.676, d = 0.2; between‐group: p = 0.851, d = 0.1) (Figure 3). A significant reduction was observed for e′ in the HIIT group, and there was no significant change observed for e’ in MOD or between groups (MOD: 11.08 ± 2.51 to 10.66 ± 3.21 cm/s; p = 0.549, d = 0.2, HIIT: 9.99 ± 2.87 to 8.33 ± 1.92 cm/s; p = 0.43, d = 1.1; between‐group: p = 0.206, d = 0.7). No other measures of diastolic function showed significant changes (Table 3). A trend for significant between‐group differences was observed for resting CO (p = 0.097) and a significant increase in the HIIT group (MOD: 4.8 ± 1.0 to 4.7 ± 1.7; p = 0.889, HIIT: 4.3 ± 1.1 to 5.3 ± 1.0 L/min; p = 0.004) owing to nonsignificant increases in heart rate and stroke volume (Table 3).
Measures of resting cardiac function in response to exercise training.
Vascular outcomes
3.5
No significant between‐group differences were observed for peripheral or estimated central blood pressures. There were trends for between‐group differences in peripheral diastolic blood pressure (DBP), central systolic blood pressure (SBP), and central DBP. Table 4 contains a full breakdown of vascular outcomes. A significant difference was observed in Aix75 between groups as well as within the MOD group (MOD: 26.4 ± 9.9% to 22.6 ± 9.4%; p = 0.027, d = 1.0, HIIT: 26.2 ± 7.9% to 28.2 ± 10.7%; p = 0.402, d = 0.3; between‐group: p = 0.04, d = 1.2). No significant differences were found within the HIIT group for any vascular outcome. In contrast, those in the MOD group had significant reductions in central SBP (111 ± 5 to 104 ± 4 mmHg; p = 0.008, d = 1.3). There were also trends for reductions in peripheral SBP (120 ± 6 to 116 ± 6 mmHg; p = 0.067, d = 0.8), DBP (78 ± 2 to 74 ± 6 mmHg; p = 0.093, d = 0.6), and Aix (29.0 ± 13.2 to 20.8 ± 13.2%; p = 0.062, d = 0.8) for those in MOD.
Biomarkers
3.6
Patients in both groups became anemic throughout the study. Hemoglobin was reduced significantly in both groups (MOD: 13.0 ± 0.6 to 10.7 g/dL ± 0.9; p = < 0.001, d = 2.2, HIIT: 12.4 ± 1.5 to 10.9 ± 0.9 g/dL; p = 0.015, d = 1.3; between‐group: p = 0.171, d = 0.8), and there was no significant difference between groups. No significant between‐ or within‐group differences were found in any marker of inflammation (all p > 0.05) (Table S1). A significant increase in NTproBNP was observed in the MOD group (104.3 ± 35.1 to 158.1 ± 56.0; p = 0.018), and no change was observed in the HIIT group (178.6 ± 49.9 to 171.1 ± 49.5; p = 0.793). This resulted in a trend for significant differences observed between groups (p = 0.075) (Figure 4).
Changes in NTproBNP following exercise training.
DISCUSSION
4
The primary finding from this pilot trial was that there were no significant between‐group differences when comparing HIIT and MOD for preserving cardiorespiratory fitness (VO_2peak_) in women with breast cancer undergoing treatment with chemotherapy. However, a large effect size was observed when comparing between‐group differences (d = 0.9). In addition, there were no significant within‐ or between‐group differences when examining LV ejection fraction or LVGLS. However, there was a significant increase in resting CO in the HIIT group secondary to an increase in stroke volume and heart rate, which was not observed in MOD. While overall exercise adherence was moderate to low, primarily due to reported symptom burden during chemotherapy weeks, there were no differences in exercise adherence between groups.
The lower‐than‐expected adherence rate observed in the current trial may be an inherent limitation to remote exercise interventions prescribed for patients undergoing chemotherapy. For example, two supervised exercise programs for women being treated for breast cancer reported ~83% adherence on average (Jones et al., 2013; Lee et al., 2019), a 20% difference from the current trial. Throughout the intervention, patients received weekly personalized text messages, which included motivational support and, when low adherence was observed, asked about the primary reason for it. The largest reason for low exercise adherence was symptom burden during chemotherapy. This issue was addressed in the recent BREXIT trial (Foulkes et al., 2023), in which low‐intensity physical activity was prescribed the week of chemotherapy infusions, with intensity increased in the subsequent weeks. Since the purpose of the current trial was to explicitly compare the effects of moderate‐ versus high‐intensity exercise, this is an inherent limitation to the study design.
Cardiorespiratory fitness
4.1
The current study found no significant between‐group differences in VO_2peak_. However, while the MOD group saw a significant reduction in VO_2peak_, no such change was observed in the HIIT group. The current study is largely in agreement with previous trials in breast cancer patients receiving chemotherapy which show a preservation or improvement in VO_2peak_ with any prescribed exercise (Courneya et al., 2007; Foulkes et al., 2023; Hornsby et al., 2014; Mijwel et al., 2018). The majority of prior trials include a mix of exercise modes or intensities and cannot conclude superiority of any modality. A primary pathway by which chemotherapies elicit cytotoxicity is through increased reactive oxygen species (Yang et al., 2018). Exercise may counteract this in a tissue‐specific manner by increasing antioxidant capacity within metabolically active tissues (i.e., cardiac and skeletal muscle) (Assi et al., 2020), thereby contributing to the preservation of VO_2peak_. Indeed, previous animal models have shown exercise to be protective during doxorubicin treatment in cardiomyocytes and skeletal muscle (Dickinson et al., 2017; Kavazis et al., 2010). With this framework in mind, HIIT may lead to greater protection than MOD due to its greater ability to increase antioxidant capacity (Paramita et al., 2022). Our study is the first to directly compare the two exercise intensities and support this hypothesis. Larger, adequately powered studies should be performed to confirm this hypothesis and compare these changes to a true control group.
Cardiac function
4.2
There were no significant changes seen within or between HIIT or MOD for LVEF or LVGLS. This is a promising finding as it is well established that chemotherapy can lead to significant reductions in cardiac systolic function. However, previous clinical trials during anthracycline and trastuzumab therapies have been unsuccessful in showing differences in cardiac function with exercise compared to usual care (Hornsby et al., 2014; Jacquinot et al., 2022; Kirkham et al., 2017, 2018). This may be due to the fact that previous studies did not observe a decline in function within the usual care groups. Foulkes et al. reported a limited effect of exercise on resting measures of cardiac function when compared to usual care. However, they observed significant improvements in exercising cardiac function and cardiac reserve in the exercise group. To this end, they conclude that changes in peak exercise cardiac function, as opposed to resting function, drive changes in VO_2peak_ (Foulkes et al., 2023). Additionally, the lack of change in cardiac function may also be due to the time course of chemotherapy‐induced cardiotoxicity. It is appreciated that drugs such as doxorubicin can have a delayed cardiotoxic response, leading to clear dysfunction and symptomatic disease years after treatment (Zamorano et al., 2016). As such, a longer follow‐up period may yield different results.
Blood pressure
4.3
Patients in the MOD group saw significant reductions in central SBP and trended toward a decrease in brachial SBP. This finding was unexpected as HIIT typically leads to greater reductions in blood pressure than MOD in healthy individuals (Angadi et al., 2015; Boutcher & Boutcher, 2017). In this study, patients in both groups saw significant reductions in hemoglobin concentrations. It is known that reduced blood viscosity due to anemia can lead to hypoxic vasodilation and thus decreased systemic vascular resistance (Metivier et al., 2000; Tanimura et al., 2017). Using left ventricular outflow tract velocity time integral and diameter, we estimated cardiac output pre‐ and post‐testing. We observed a significant increase in cardiac output in the HIIT group (4.3 ± 1.1 to 5.3 ± 1.0 L/min; p = 0.004) owing to slight increases in both stroke volume and heart rate, and no such increase occurred in the MOD group. Thus, in the face of anemia, those in the HIIT group may have been able to augment cardiac output to maintain blood pressures while those in the MOD group could not.
Biomarkers
4.4
Chemotherapy leads to increases in proinflammatory cytokines, which may be related to an increased risk of cardiotoxicity (Ky et al., 2014). In addition, this cardiotoxicity may be reflected by increases in NTproBNP, an important marker for heart failure risk (Vergaro et al., 2021). In the present study, NTproBNP significantly increased within the MOD group, while no changes were observed in the HIIT group. Previous trials have shown similar, albeit mixed, results compared to those found in the present study. Currently, there is limited literature for the ability of NTproBNP/BNP to predict chemotherapy‐related changes in cardiac function (Michel et al., 2020). In a long term follow up of the OptiTrain trial, it was found that those in the exercise groups had lower levels of NTproBNP compared to usual care, and those with higher levels of NTproBNP showed a reduction in VO_2peak_ compared to those with lower levels (Ansund et al., 2021).
Study strengths and limitations
4.5
As reported previously (Helms et al., 2026), our study saw a greater than anticipated dropout rate and as a result was statistically underpowered making it hard to appreciate between‐group differences. One limitation to the current study is a lack of true control group which makes it difficult to draw definitive conclusions on the ability of exercise to preserve measures of CVD risk in this population. In addition, due to the use of different exercise modalities for our exercise groups (walking vs. cycling), and use of cycle ergometry for testing, it could be argued that any differences between groups may not be due solely to differences in training intensities, but rather specificity of training. However, the maintenance of heart rate and stroke volume in the face of profound anemia as well as maintenance of NTproBNP in the HIIT group suggest that the findings are unlikely to be due to the modality of testing but due to differences in training interventions.
In addition, while our study was randomized, due to chance all African American participants were in the HIIT group. It has been previously reported that African Americans may have different blood pressure responses following exercise compared to European Americans (Pescatello et al., 2003). While slight differences were noted between ethnicities for blood pressure outcomes in the HIIT group, due to the small sample included it is hard to draw definitive conclusions. Future studies should ensure even distribution of race and ethnicities between groups.
While echocardiography is the standard measure of cardiac function within clinical practice, it has poor test–retest reliability and has limitations in chamber volume estimation (Houard et al., 2021; Jenkins et al., 2004). Use of a more sensitive measure, such as cardiac magnetic resonance (CMR), may lead to different outcomes. In addition, resting measures of cardiac function may not adequately demonstrate changes in systolic function seen during exercise (Foulkes et al., 2023) and, as such, exercise measures of cardiac function should also be obtained.
Further, chemotherapy regimens not traditionally considered to be cardiotoxic were included in the present trial. Previous trials looking at the role of exercise to prevent worsening VO_2peak_ and cardiovascular function during chemotherapy have focused largely on anthracycline therapies (Foulkes et al., 2023; Hornsby et al., 2014; Jones et al., 2013; Kirkham et al., 2017, 2018; Lee et al., 2019; Mijwel et al., 2018). Our trial included both those on immunotherapies (i.e., immune checkpoint inhibitors), as well as other non‐cardiotoxic therapies (i.e., platinum‐based drugs and microtubule inhibitors). The inclusion of broader chemotherapeutic agents allows our results to be more generalizable to breast cancer populations as opposed to just those being treated with anthracyclines. However, this inclusion of less cardiotoxic chemotherapies may have muted our findings.
Future directions
4.6
Future research should examine acute and long‐term changes in NTproBNP and other biomarkers and the relationship of these changes to potential declines in VO_2peak_ and cardiac function, following breast cancer treatment. In addition, future studies should compare the efficacy of remotely monitored exercise to supervised exercise training in this population. Given the low usage of supervised rehabilitation in cancer survivors (Hardcastle et al., 2018), it is imperative that effective alternate options are available. Studies should also examine the influence of exercise adherence on the efficacy of outcomes. Additionally, there remains a question about whether there is a minimum amount of exercise required to preserve function, above which there are no additional benefits seen during chemotherapy treatment. Interventions could be designed to examine different exercise amounts/intensities to determine if there is a minimum threshold required for cardio‐protection.
CONCLUSIONS
5
In conclusion, this trial found that there were no significant between‐group differences in VO_2peak_ or cardiac function for patients with breast cancer in remotely delivered HIIT and MOD interventions throughout chemotherapy. Adherence to the remote exercise intervention was lower than anticipated (~63% for each group) and may be a limitation to remote interventions. There were no exercise‐related serious adverse events reported in either group, indicating that remotely administered interventions are safe in this population after adequate screening by their physicians. Despite being underpowered, this study is the first to directly compare the effects of different exercise intensities on mitigating cardiotoxicity. Our trial builds on the existing literature indicating that exercise should be prescribed throughout chemotherapy to help offset some of the negative off‐target effects of chemotherapy.
AUTHOR CONTRIBUTIONS
R.A.K., J.M.Z, and S.S.A. conceived and designed the study. R.A.K., J.M.Z, S.S.A., and A.A. were awarded funding for the study. N.R.W., C.C.E., M.B.M., C.E.H., and Z.S.L. participated in data collection. N.R.W., C.C.E., and M.B.M. analyzed and interpreted the results of the data. N.R.W. drafted the manuscript. Z.B.N., A.A., C.M.B., P.M.D., and T.M. screened and identified patients. All authors edited, revised manuscript, and approved the final version of the manuscript.
FUNDING INFORMATION
This research was supported by funding within the UVA Comprehensive Cancer Center (P30CA044579) and seed funding from the UVA Imaging and Informatics in Precision Immunomedicine (iPRIME) initiative.
CONFLICT OF INTEREST STATEMENT
The authors declare no potential conflicts of interest.
ETHICS STATEMENT
This study was approved by the institutional review board at the University of Virginia and conducted in accordance with the Declaration of Helsinki. All participants provided informed consent prior to any study procedures.
Supporting information
Table S1.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1American College of Sports Medicine , Liguori, G. , Feito, Y. , Fountaine, C. , & Roy, B. (2021). ACSM's Guidelines for Exercise Testing and Prescription (Eleventh ed.). Wolters Kluwer.
- 2Angadi, S. S. , Bhammar, D. M. , & Gaesser, G. A. (2015). Postexercise hypotension after continuous, aerobic interval, and Sprint interval exercise. Journal of Strength and Conditioning Research, 29(10), 2888–2893. 10.1519/JSC.0000000000000939 25785706 · doi ↗ · pubmed ↗
- 3Ansund, J. , Mijwel, S. , Bolam, K. A. , Altena, R. , Wengström, Y. , Rullman, E. , & Rundqvist, H. (2021). High intensity exercise during breast cancer chemotherapy—Effects on long‐term myocardial damage and physical capacity—Data from the Opti Train RCT. Cardiooncology, 7(1), 7. 10.1186/s 40959-021-00091-1 33588948 PMC 7883413 · doi ↗ · pubmed ↗
- 4Assi, M. , Dufresne, S. , & Rebillard, A. (2020). Exercise shapes redox signaling in cancer. Redox Biology, 35, 101439. 10.1016/j.redox.2020.101439 31974046 PMC 7284915 · doi ↗ · pubmed ↗
- 5Baba, R. , Nagashima, M. , Goto, M. , Nagano, Y. , Yokota, M. , Tauchi, N. , & Nishibata, K. (1996). Oxygen uptake efficiency slope: A new index of cardiorespiratory functional reserve derived from the relation between oxygen uptake and minute ventilation during incremental exercise. Journal of the American College of Cardiology, 28(6), 1567–1572. 10.1016/s 0735-1097(96)00412-3 8917273 · doi ↗ · pubmed ↗
- 6Boutcher, Y. N. , & Boutcher, S. H. (2017). Exercise intensity and hypertension: what's new? Journal of Human Hypertension, 31(3), 157–164. 10.1038/jhh.2016.62 27604656 · doi ↗ · pubmed ↗
- 7Courneya, K. S. , Segal, R. J. , Mackey, J. R. , Gelmon, K. , Reid, R. D. , Friedenreich, C. M. , Ladha, A. B. , Proulx, C. , Vallance, J. K. , Lane, K. , Yasui, Y. , & Mc Kenzie, D. (2007). Effects of aerobic and resistance exercise in breast cancer patients receiving adjuvant chemotherapy: A multicenter randomized controlled trial. Journal of Clinical Oncology, 25(28), 4396–4404. 10.1200/JCO.2006.08.2024 17785708 · doi ↗ · pubmed ↗
- 8Dickinson, J. M. , D'Lugos, A. C. , Mahmood, T. N. , Ormsby, J. C. , Salvo, L. , Dedmon, W. L. , Patel, S. H. , Katsma, M. S. , Mookadam, F. , Gonzales, R. J. , Hale, T. M. , Carroll, C. C. , & Angadi, S. S. (2017). Exercise protects skeletal muscle during chronic doxorubicin administration. Medicine and Science in Sports and Exercise, 49(12), 2394–2403. 10.1249/MSS.0000000000001395 28767526 · doi ↗ · pubmed ↗