Microbiome-mediated colonization resistance to and countermeasures of Klebsiella pneumoniae
Yongqiang Yang, Willem van Schaik, Alan McNally, Zhiyong Zong

TL;DR
This paper explores how the gut microbiome influences Klebsiella pneumoniae colonization and disease, and how the bacteria adapt to resist microbial defenses.
Contribution
The paper highlights novel mechanisms by which K. pneumoniae adapts to gut commensals and suggests microbiome-based therapeutic strategies.
Findings
Gut commensals provide colonization resistance against Klebsiella pneumoniae.
K. pneumoniae adapts via multiple mechanisms to overcome this resistance.
Microbiome-based therapies show potential for managing K. pneumoniae-related diseases.
Abstract
Klebsiella pneumoniae intestinal colonization contributes to infectious and non-infectious diseases. Recent studies have uncovered the complex interplay between the gut microbiota and K. pneumoniae colonization, highlighting its role in disease development and progression and illustrating the potential of microbiome-based therapies. Yang et al. summarize that Klebsiella pneumoniae affects infectious and non-infectious disease via gut colonization; commensals provide colonization resistance, but K. pneumoniae adapts via multiple mechanisms.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
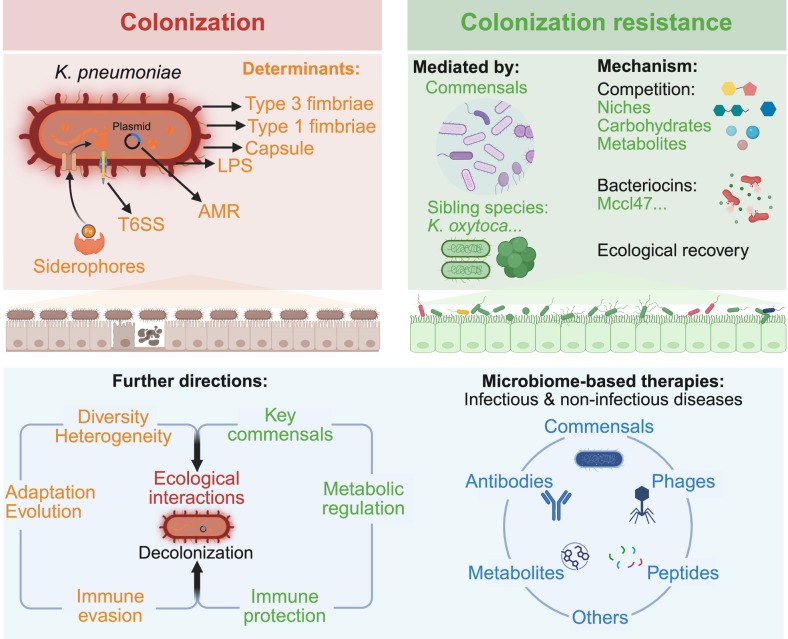 Figure 1
Figure 1- —https://doi.org/10.13039/501100002855Ministry of Science and Technology of the People's Republic of China (Chinese Ministry of Science and Technology)
- —https://doi.org/10.13039/501100009187RCUK | MRC | Medical Research Foundation
- —https://doi.org/10.13039/501100000265RCUK | Medical Research Council (MRC)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGut microbiota and health · Antibiotic Resistance in Bacteria · Clostridium difficile and Clostridium perfringens research
Klebsiella pneumoniae gut colonization contributing to diseases
Klebsiella pneumoniae is one of the ESKAPE pathogens, posing a dual threat due to its extensive antimicrobial resistance and virulence, which together impose substantial clinical and economic burdens^1^. K. pneumoniae is one of the leading causes of respiratory tract infections (pneumonia), urinary tract infections (cystitis, pyelonephritis), bloodstream infections, central nervous system infections (meningitis), wound and surgical site infections, liver abscesses, intra-abdominal infections, and ocular infections^1^. Capsule, lipopolysaccharide, and fimbriae are key virulence and colonization determinants that confer K. pneumoniae with advantages against bacterial competition, complement-mediated clearance, and host immune evasion^2^. Notably, beyond its established role in severe infections, K. pneumoniae is increasingly recognized as a contributor to non-infectious diseases, and its presence has been correlated with inflammatory bowel diseases^3^, non-alcoholic fatty liver disease^4^, hepatocellular carcinoma^5^, and auto-brewery syndrome^6^. The gastrointestinal tract constitutes the primary reservoir of K. pneumoniae, and intestinal colonization represents a pivotal risk factor to both local and systemic diseases. Intestinal colonization or outgrowth has been reported to directly contribute to the development of subsequent infections^7^ and various non-infectious diseases^3,5^.
Microbiome-mediated colonization resistance against K. pneumoniae
The gut microbiota in healthy individuals harbors an ecosystem with a high microbial diversity, including numerous commensal bacteria that collectively confer colonization resistance against pathogenic invasion^8^. Identifying key commensals capable of inhibiting K. pneumoniae gut colonization has important implications for both therapeutic and preventive strategies.
Two main approaches are applied to identify such commensals, including direct screening from the microbiota of healthy donors and reverse identification of species with reduced abundance in hosts with gut dysbiosis. Colonization resistance can be evaluated either by in vitro inhibition of K. pneumoniae growth or by in vivo murine decolonization models. A coculture competition assay involving 100 human gut bacterial isolates against K. pneumoniae has revealed that single species provided no robust colonization resistance, while resistance required a diverse community, dependent on specific compositions and interactions^9^. A defined consortium of 10 species was able to suppress K. pneumoniae growth by >1000-fold in vitro^9^. In another study, human fecal microbiota transplantation (FMT) samples that could effectively decolonize K. pneumoniae in a mouse model with a humanized microbiota were used to isolate commensal bacteria, with further optimization yielding an 18-member consortium (F18-mix). In germ-free mice monocolonized with carbapenemase-producing K. pneumoniae, oral inoculation of F18-mix reduced its levels in feces by three orders of magnitude by day 7 and maintained the effect through day 28^10^.
In contrast, in dysbiotic hosts such as patients in intensive care units whose gut microbiota are severely disrupted due to intensive medical interventions, colonization resistance is compromised, allowing the outgrowth of carbapenem-resistant K. pneumoniae (CRKP). Both in vitro and in vivo studies have demonstrated that probiotic supplementation of Lactiplantibacillus plantarum 21790 and Bifidobacterium longum 6188 contributed significantly to CRKP decolonization^11^. Notably, decolonized subjects exhibited ecological recovery marked by increased microbial diversity and enrichment of key commensals, including Bacteroides dorei, Bifidobacterium bifidum, Bifidobacterium pseudocatenulatum, and Faecalibacterium prausnitzii, all of which are also known to enhance colonization resistance and thus support CRKP clearance^12^. However, determining the precise combinations of commensals against different K. pneumoniae lineages remains a critical step toward developing probiotic-based therapeutic strategies.
Microbial interactions conferring colonization resistance
Key commensals employ diverse competitive strategies to suppress K. pneumoniae colonization, including nutrient competition, production of inhibitory metabolites, and stimulation of host immune defenses (Fig. 1). In murine models, Klebsiella oxytoca suppresses K. pneumoniae colonization by facilitating the functional recovery of beneficial commensal bacteria, thereby restoring colonization resistance in a diet-dependent manner^13^. Mechanistically, K. oxytoca exhibits a broader carbon utilization spectrum that overlaps with K. pneumoniae, thereby limiting its invasion^14^. Specifically, protective K. oxytoca strains were more adapt at utilizing β-glucosides and thus outcompeted K. pneumoniae in vitro and in mice^14^. Three additional bacterial strains, Blautia coccoides YL58*, Enterococcus faecalis* KB1*, and Enterocloster clostridioformis* YL32, were identified to cooperate with K. oxytoca for long-term clearance of K. pneumoniae strain MDR1 by further restricting access to carbon sources^14^. The importance of carbon sources in the intestinal environment for colonization by K. pneumoniae is further supported by the observation that lactulose can enhanced gut colonization, as it is not absorbed by the host and can be metabolized by K. pneumoniae^15^. K. oxytoca has also been evaluated as a live biotherapeutic, demonstrating the ability to decolonize K. pneumoniae, restore gut barrier integrity, and prevent its translocation from the intestine to the liver^5^. Because certain K. oxytoca strains can be pathogenic^16^, careful safety evaluation and selection of commensal strains are necessary. Lactobacillus-driven expansion of Clostridiales also reduces multidrug-resistant K. pneumoniae colonization by secreting butyrate and depleting key nutrients such as serine, threonine, and glucose^17^. At the community level, commensal consortia conferring colonization resistance have been found to suppress K. pneumoniae by competitively depleting gluconate, a preferential carbon source for Enterobacteriaceae, including K. pneumoniae, while leaving non-competing commensals unaffected^10^.Fig. 1. Microbiome-mediated colonization resistance and Klebsiella pneumoniae countermeasures.Recent studies have highlighted the important role of K. pneumoniae in both infectious and non-infectious diseases, as well as the complex interplay between the gut microbiota and K. pneumoniae colonization. In healthy individuals, the gut microbiota establishes colonization resistance against K. pneumoniae through balanced ecological niches shaped by key commensals, thereby limiting its colonization. The underlying mechanisms include competitive exclusion for nutrients and ecological niches, secretion of antagonistic molecules, and metabolic interference. However, K. pneumoniae can overcome these defenses through intrinsic traits and adaptations, developing multiple strategies to facilitate colonization, such as acquisition of AMR and virulence alterations, unique structural features (e.g., capsule, LPS, and fimbriae), elimination of competitors via T6SS, and metabolic adaptations conferring survival advantages. Future studies should consider the diversity and heterogeneity of K. pneumoniae populations, as well as their adaptability and evolutionary dynamics. Research on colonization resistance may focus on the identification of key commensals and their mechanisms of action, including regulation at the metabolic level. In addition, further investigation is needed into the complex interactions between K. pneumoniae and other gut microbes, as well as host immune evasion strategies. Microbiome-based therapeutic approaches against K. pneumoniae, including commensals, phages, peptides, metabolites, and antibodies, represent promising candidates. AMR antimicrobial resistance, LPS lipopolysaccharide, T6SS the type VI secretion system. Created in BioRender. Yang, Y. (2026) https://BioRender.com/ytu7xgk.
Commensals also secrete bactericidal or bacteriostatic compounds against K. pneumoniae. For example, class IIb microcin I47 (MccI47), a siderophore-linked antimicrobial peptide produced by E. coli, significantly inhibited CRKP in murine models when delivered either as a purified peptide or via an engineered E. coli strain Nissle 1917 producing MccI47, without disrupting the resident microbiota^18^. This highlights the potential of narrow-spectrum targeted intervention strategies for selective K. pneumoniae suppression. In addition, tilimycin, a DNA-alkylating enterotoxin produced by K. oxytoca, functions as a mutagen that increases mutation rates and induces DNA damage of K. pneumoniae, thereby facilitating decolonization^19^. Collectively, these findings suggest that targeting K. pneumoniae-specific metabolic pathways and leveraging commensal-derived metabolites or nutrient competition may provide novel microbiome-based interventions to prevent or eliminate K. pneumoniae colonization.
K. pneumoniae countering colonization resistance
Despite the protective role of the gut microbiota, K. pneumoniae has evolved multiple mechanisms to overcome colonization resistance, enabling its expansion in dysbiotic hosts^5^ (Fig. 1). The bacterial type VI secretion system (T6SS) is a phage tail-like contractile nanomachine that mediates contact-dependent killing of bacterial competitors as well as adhesion and invasion of host cells. The T6SS of K. pneumoniae is required for robust colonization of the murine gastrointestinal tract under conditions of an intact microbiota. Notably, gut-mimetic conditions, characterized by high arginine availability, low iron, and hypoxia, strongly induce T6SS expression. These signals upregulate transcription and enhance T6SS activity, resulting in the targeted killing of competing Betaproteobacteria and thus facilitating K. pneumoniae persistence^20^.
K. pneumoniae further facilitates gut colonization by compromising host mucosal defenses. A recent study has shown that K. pneumoniae was highly enriched in stool samples from patients with hepatocellular carcinoma, and a similar enrichment was observed in the feces of mice receiving FMT from these patients. Further gavage of isolated K. pneumoniae strains to germ-free mice revealed that these strains disrupted colonic intercellular junctions, thinned the protective mucus layer, downregulated tight junction proteins, and enhanced bacterial penetration into the lamina propria and muscularis mucosa^5^. This study provides a new perspective on how K. pneumoniae gains a colonization advantage in the gut, translocates via the gut-liver axis, and ultimately contributes to the progression of non-infectious liver diseases. K. pneumoniae has some structural features that contribute to its colonization capacity. Type 1 and type 3 fimbriae are commonly associated with adherence to mucosal surfaces^21^; however, the regulatory mechanisms governing bacterial colonization are largely unknown. Notably, regulatory genes can be conserved across K. pneumoniae strains, which means modulation of gene expression through a signaling pathway involving environmental stimuli, rather than gene presence or absence, may be a key determinant of colonization fitness. In one study, clinical K. pneumoniae strains with high colonization abilities were identified from a murine colonization model and subsequently subjected to in vitro experimental evolution. This approach led to the identification of functional mutations in cpxA, encoding the sensor kinase of the CpxR-CpxA two-component system. Mechanistically, CpxA negatively regulates type 3 fimbriae expression, thereby influencing colonization efficiency^22^.
Together, these strategies, including competitive killing via T6SS, specialized surface structures, and direct host barrier disruption, highlight the evolutionary plasticity of K. pneumoniae in overcoming colonization resistance and establishing persistent niches in the gut, which can impact the health of the host. These findings also highlight K. pneumoniae as a highly heterogeneous population in which distinct strains exhibit divergent regulatory strategies and colonization phenotypes. Such diversity may confer population-level adaptability, enabling different lineages to colonize and persist across host-associated environments.
Conclusions and future perspectives
The role of K. pneumoniae in both infectious and non-infectious diseases receives increasing attention. In infectious contexts, research has focused primarily on antimicrobial resistance and virulence, while in non-infectious diseases focused on metabolic interactions and host immune modulation. Recent findings underscore the complex interplay between colonization-resistant commensals and K. pneumoniae. Key commensal species or microbial consortia can suppress K. pneumoniae through nutrient and metabolic competition, secretion of effector molecules, and reinforcement of host epithelial and immune barriers. Conversely, K. pneumoniae has evolved counterstrategies, including unique cell wall and capsule structures, specialized metabolic pathways, and deployment of the T6SS to evade colonization resistance.
Microbiome-based decolonization is a promising therapeutic approach, but current studies remain limited, and several research gaps need to be considered. First, the genetic and phenotypic diversity of K. pneumoniae is rarely addressed, particularly in non-infectious diseases, as only a few studies have examined which specific K. pneumoniae lineages are effectively suppressed by colonization-resistant microbiota^3^. Notably, some K. pneumoniae types, like hypervirulent sequence type 23 strains with thick capsules, can colonize in the presence of an intact microbiota^23^ and have been detected in the gastrointestinal tracts of healthy individuals^24^. Importantly, the diversity of K. pneumoniae must be considered across geographic contexts and host populations, with distinctions between colonizing and infecting strains, as well as between healthy carriers of strains or hospitalized individuals. While healthcare-associated infections are often dominated by a limited number of high-risk clones, the dominant epidemic lineages vary substantially between regions. Moreover, the dynamic replacement and expansion of specific clones represent an underestimated but clinically significant phenomenon. Examples include the decline of ST258 and ST307 in the United States^25^, capsular-type replacement within ST11 strains in China^26^, and the dynamic predominance of multiple sequence types in South Africa^27^. The replacement of dominant clones and emergence of novel clones underscore the need for sustained genomic surveillance.
Second, gastrointestinal carriage of K. pneumoniae is a major risk factor for subsequent infection. Systematic monitoring of intestinal colonization in both healthy individuals and patients remains limited. Colonization rates of K. pneumoniae in healthy populations were reported as 5–35% in Western countries and 18.8–87.7% in Asian countries^24^. Among hospitalized patients, carriage rates range from 23 to 70%^21^. The lineages of colonizing strains often overlap with those causing clinical infections, indicating that gut-adapted K. pneumoniae can retain pathogenic potential. However, clinical K. pneumoniae strains undergoing within-host evolution more commonly acquire mutations in virulence genes, including the capsule, lipopolysaccharide, and iron utilization pathways, leading to attenuated virulence while enhancing fitness in extraintestinal niches through evolutionary trade-offs^28^. Furthermore, colonizing bacterial populations can be more genetically diverse than predominantly invasive strains. This raises the question of why some colonizing types do not cause invasive disease. One possible explanation is the selective pressure of antimicrobial agents, which preferentially drives the expansion and dissemination of some high-risk clones. This discrepancy may also reflect complex ecological interactions involving K. pneumoniae, including intra-species interactions, interactions with co-colonizing microbes (bacteria, virus, and fungi), and interactions with the host. Specifically, the gut virome, which is dominated by bacteriophages, is established early in life and exhibits greater diversity than the bacteriome. It plays a critical role in shaping the composition of the gut microbiota, affecting pathogen colonization, and also serve as a biomarker distinguishing different human populations^29^. Bacteriophages have been used for intestinal decolonization of K. pneumoniae^30^, and phage cocktails or phage-antibiotic synergy may work synergistically to delay phage resistance and provide broader-spectrum efficacy. Taken together, elucidating these mechanisms will be essential for the rational design of microbiome-based decolonization strategies.
Third, the K. pneumoniae lineages and the pathogenic mechanisms for infections and non-infectious conditions may be different. Future studies should consider these differences, distinguishing between infection-associated K. pneumoniae, which typically involves rapid expansion of defined clones that breach host defenses, and non-infectious contexts, where more diverse lineages coexist with the host and contribute to disease progression via metabolic pathways. Infection-focused studies will require high-resolution, fine-scale analyses beyond sequence type classification, whereas investigations into non-infectious diseases need to study specific metabolic pathways and their host interactions. Third, the identification of key commensals that confer colonization resistance against K. pneumoniae requires careful consideration of geographic, population-specific, and disease-specific heterogeneity. Furthermore, these commensals, which could serve as potential biotherapeutics, need to be validated in vivo to guide the development of precise microbiome-targeted therapeutic strategies.