Molecular epidemiology and environmental persistence of methicillin-resistant coagulase-positive Staphylococci in a Veterinary Teaching Hospital in Thailand: Evidence for nosocomial transmission and One Health implications
Punpichaya Fungwithaya, Jayaseelan Murugaiyan, David J.Hampson, Nuvee Prapasarakul

TL;DR
This study shows that methicillin-resistant staphylococci, especially MRSP, are widespread in a Thai veterinary hospital, suggesting nosocomial transmission and the need for improved infection control.
Contribution
The study provides evidence of clonal overlap between canine and environmental MRCoPS isolates, highlighting One Health implications and the need for integrated infection control.
Findings
MRSP was the most prevalent methicillin-resistant staphylococcus in the hospital environment.
Clonal similarity between canine and environmental isolates suggests potential nosocomial transmission.
Floors were identified as the main reservoir for MRCoPS contamination.
Abstract
Methicillin-resistant coagulase-positive Staphylococci (MRCoPS), including methicillin-resistant Staphylococcus pseudintermedius (MRSP), methicillin-resistant Staphylococcus aureus (MRSA), and methicillin-resistant Staphylococcus coagulans (MRSC), are emerging zoonotic pathogens in veterinary hospitals, posing significant infection control challenges. This study aimed to investigate the molecular epidemiology, antimicrobial resistance profiles, and clonal dissemination of MRCoPS across environmental surfaces, veterinary personnel, and canine patients at the Veterinary Teaching Hospital, Chulalongkorn University (VTH-CU), Thailand. A cross-sectional study was conducted involving 216 environmental samples, 23 veterinary staff, and 14 canine patients. Isolates were identified using biochemical tests, polymerase chain reaction (PCR), and matrix-assisted laser…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1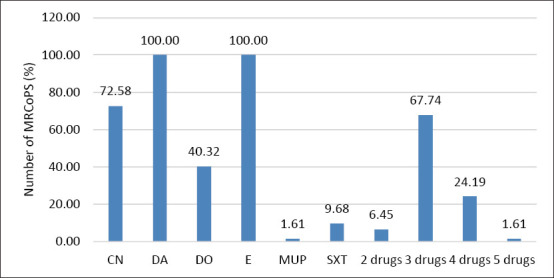 Figure 2
Figure 2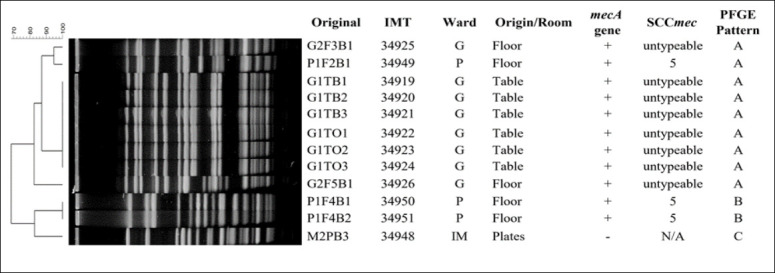 Figure 3
Figure 3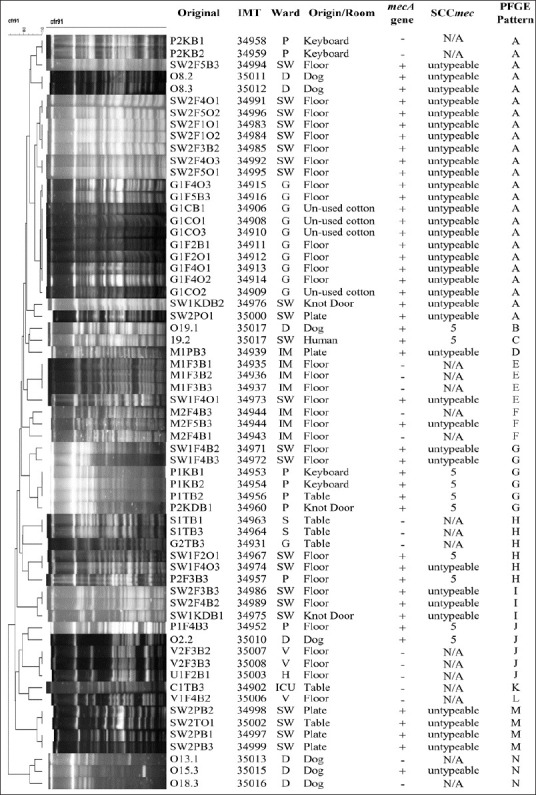 Figure 4
Figure 4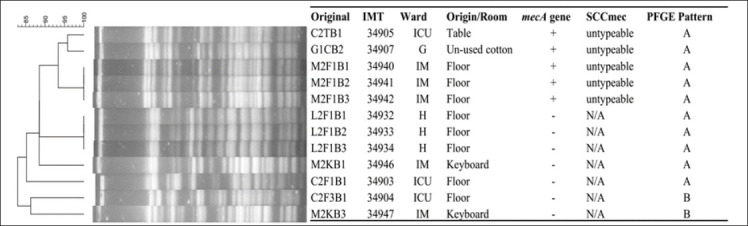 Figure 5
Figure 5| Environmental samples | Type | Sample/area/time | Swabbing criteria (area per swab) |
|---|---|---|---|
| Floor | Floor | 5/1/1 | 3 × 3 cm2 from five parts: right up, right down, middle, left up, and left down in the main examination room |
| Medical equipment and fittings | Wound cotton | 1/1/1 | Bandaging wound cotton (1 g) in the main examination room |
| Stethoscope | 1/1/1 | 0.1 × 0.1 cm2 of the animal contact surface of the stethoscopes in the main examination room | |
| Syringe tray | 1/1/1 | 0.1 × 0.1 cm2 of syringe tray in the main examination room | |
| Disinfectant water1 | 1/1/1 | 1 mL disinfectant water in a forceps jar in the main examination room | |
| Examination table | 1/1/1 | 10 × 10 cm2 on the examination table surfaces in the main examination room | |
| Waiting bench | 1/1/1 | 10 × 10 cm2 waiting bench in front of the main examination rooms | |
| Drug cabinet | 1/1/1 | 10 × 10 cm2 of drug cabinet in the division or unit in the main examination room | |
| Keyboard | 1/1/1 | 10 × 10 cm2 of keyboard in the main examination room | |
| Doorknob | 1/1/1 | 0.1 × 0.1 cm2 of doorknob on the front door in the main examination |
| Unit | Main antibiotic used | Routine cleaning management (antiseptic, equipment, and time) | Average number of colonies on the floor | Average number of colonies on medical instruments | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
| ||||||||||||
| CoPS positive surfaces (%) | MRCoPS-positive surfaces (%) | MRCoPS-positive surfaces | CoPS positive surfaces (%) | MRCoPS-positive surfaces (%) | MRCoPS-positive surfaces | |||||||
|
|
| |||||||||||
| Odds ratio | 95% CI | p-value | Odds ratio | 95%CI | p-value | |||||||
| Gynecology | Enrofloxacin | 2.5% quaternary ammonium compound/Mob/1 | 5/10 (50) | 5/10 (50) | 4 | 0.50–31.84 | 0.294 | 3/18 (16.67) | 2/18 (11.11) | 2.13 | 0.17–26.15 | 1 |
| Medicine | Amoxicillin/clavulanic acid | 2.5% quaternary ammonium compound/Mob/1 | 4/10 (40) | 2/10 (20) | Reference | Reference | Reference | 3/18 (16.67) | 1/18 (5.56) | Reference | Reference | Reference |
| Post-operative care | Enrofloxacin | 2.5% quaternary ammonium compound/Mob/2 | 3/10 (30) | 3/10 (30) | 1.71 | 0.22–13.51 | 0.76 | 4/18 (22.22) | 3/18 (16.67) | 3.4 | 0.31–37.75 | 0.551 |
| Surgery | Enrofloxacin | 2.5% quaternary ammonium compound/Mob/1 | 1/18 (5.56) | |||||||||
| Dermatological | Amoxicillin/clavulanic acid, cephalexin, and metronidazole | No antiseptic/ Broom/1 | 6/10 (60) | 6/10 (60) | 6 | 0.79–45.72 | 0.155 | 3/18 (16.67) | 3/18 (16.67) | 3.4 | 0.31–37.75 | 0.551 |
| ICU | Amoxicillin/clavulanic acid, cephalexin, and metronidazole | 2.5% quaternary ammonium compound/Mob/2 | 2/10 (20) | 2/18 (11.11) | 1/18 (5.56) | Reference | Reference | Reference | ||||
| Vaccine | 2.5% quaternary ammonium compound/Mob/1 | 2/10 (20) | ||||||||||
| Lower floor | Unknown/Mob/1 | 1/10 (10) | ||||||||||
| Upper floor | Unknown/Mob/1 | 1/10 (10) | ||||||||||
| Unit | Floor | Examination table | Syringe tray | Keyboard | Wound cotton | Doorknob |
|---|---|---|---|---|---|---|
| Gynecology | △ | △▲ | △◯ | |||
| Medicine | △▲◯ | △▲ | ⚫ | |||
| Post-operative Care | △ | △ | △▲ | △ | ||
| Surgery | ▲ | |||||
| Dermatological | △ | △ | △ | △ | ||
| Vaccine | ▲ | |||||
| ICU | ⚫ | ◯▲ | ||||
| Hallways | ▲⚫ |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntimicrobial Resistance in Staphylococcus · Milk Quality and Mastitis in Dairy Cows · Clostridium difficile and Clostridium perfringens research
INTRODUCTION
Coagulase-positive Staphylococci (CoPS) are Gram-positive cocci responsible for a variety of infections, including dermatitis, wound infections, and septicemia in animals and humans [1–3]. Among these, Staphylococcus aureus, Staphylococcus pseudintermedius, and Staphylococcus coagulans are the most clinically relevant species that colonize and cause disease in animals [4–7]. Importantly, canine CoPS can exchange the mobile genetic element known as the staphylococcal cassette chromosome mec (SCCmec) both within and between species [8–10]. This element carries multiple antibiotic resistance determinants, particularly the mecA gene, which encodes resistance to β-lactam antibiotics such as oxacillin.
Methicillin-resistant CoPS (MRCoPS) harboring the mecA gene represent a major concern in both human and veterinary healthcare environments due to their multidrug-resistant (MDR) nature and zoonotic potential. These pathogens can be transmitted among humans, animals, and contaminated surfaces, including medical instruments [11–13]. Although methicillin-resistant S. aureus (MRSA) is typically isolated in low numbers from veterinary hospitals and small-animal skin, it can occasionally cause severe outbreaks, as documented in equine facilities [14]. In humans, MRSA is associated with localized and systemic infections, including septicemia [15, 16]. In contrast, methicillin-resistant S. pseudintermedius (MRSP) commonly exhibits MDR to β-lactams, macrolides, lincosamides, fluoroquinolones, and aminoglycosides [13, 17, 18]. The growing prevalence of MRSP in veterinary hospitals has heightened the risk of surgical site infections and septicemia in companion animals, posing significant challenges to infection control and hospital management [19, 20]. Consequently, MRSP has emerged as a leading cause of nosocomial infections in veterinary settings [21].
Environmental surfaces, veterinary staff, and animal patients serve as critical reservoirs and vectors for MRSA, MRSP, and methicillin-resistant S. coagulans (MRSC) within clinical environments [22]. Continuous monitoring of MRCoPS is therefore essential to predict and mitigate their spread [22, 23]. These organisms have been recovered from diverse surfaces and instruments, such as floors, examination tables, stethoscopes, and weighing scales, indicating widespread environmental persistence [13, 22, 24]. The persistence of MRCoPS even after standard disinfection underscores the risk of ongoing cross-contamination [18, 23]. Transmission can also occur between pets, veterinarians, and owners, facilitated by inadequate hygiene and contaminated medical devices. Notably, the prevalence and distribution of MRCoPS vary across hospitals, depending on disinfection practices, hand hygiene, and infection control standards [25, 26]. Thus, rigorous hygiene policies and accreditation protocols, including adherence to proper hand hygiene, use of protective clothing, and application of effective disinfectants, are imperative for controlling MRCoPS dissemination [25].
In Thailand, research on MRCoPS in veterinary hospitals has primarily focused on MRSA, with limited attention to other coagulase-positive species. Early investigations characterized MRSA in humans, pets, and the hospital environment but did not extend to MRSP or MRSC [27]. Our previous study was among the few to explore transmission dynamics involving staff, animal patients, and the surgical unit environment, providing critical insight into potential pathways of hospital contamination [19].
Despite growing awareness of methicillin-resistant Staphylococcus species in veterinary hospitals, existing literature has several critical limitations. Most prior investigations in Thailand have centered on S. aureus (MRSA), often overlooking the broader spectrum of CoPS (MRCoPS), particularly S. pseudintermedius (MRSP) and S. coagulans (MRSC), which are increasingly recognized as major nosocomial and zoonotic pathogens. Moreover, previous environmental surveillance studies have largely been descriptive, focusing on detection frequency rather than exploring the molecular epidemiology and clonal relationships among isolates from animals, humans, and hospital surfaces. Consequently, there remains a limited understanding of how MRCoPS persist in different clinical units, their antimicrobial resistance mechanisms, and their genetic relatedness, all of which are essential for determining infection sources and transmission routes. In addition, the efficacy of disinfection and hospital-specific risk factors influencing the persistence of these organisms have rarely been statistically evaluated. The lack of integrative, cross-sectional molecular studies hampers the development of evidence-based infection control strategies in veterinary settings, particularly in tropical hospital environments where cleaning conditions, antibiotic usage, and patient load may differ significantly from those in temperate regions.
This study aimed to investigate the molecular epidemiology, antimicrobial resistance patterns, and environmental distribution of MRCoPS in a major veterinary teaching hospital (VTH) in Thailand. Specifically, the study sought to (i) determine the prevalence and diversity of MRCoPS species recovered from environmental surfaces, veterinary personnel, and canine patients; (ii) identify mecA-positive isolates and characterize their SCCmec types; (iii) evaluate antimicrobial susceptibility profiles to commonly used veterinary antibiotics; (iv) determine the clonal relationships among isolates using pulsed-field gel electrophoresis (PFGE); and (v) analyze environmental and operational risk factors contributing to MRCoPS persistence using multivariate logistic regression. By integrating microbiological, molecular, and epidemiological data, this research provides the first comprehensive evidence of MRCoPS transmission dynamics within a Thai veterinary hospital context, supporting the design of targeted infection control and antimicrobial stewardship strategies aligned with the One Health framework.
MATERIALS AND METHODS
Ethical approval
Ethical clearance for the study was obtained from both the Institutional Animal Care and Use Committee (approval no. 113/56) and the Ethical Review Committee for Research Involving Human Research Subjects, Health Science Group, Chulalongkorn University (approval no. 137/57), Research and Innovation for Society, Chulalongkorn University. The overall workflow of the study is summarized in Figure 1.
Outline of the study workflow.
Study period and location
A cross-sectional study was conducted during May 2014 at the VTH, Chulalongkorn University (VTH-CU), within the Small Animal Teaching Hospital of the Faculty of Veterinary Science, Bangkok, Thailand.
Hospital setting
The VTH-CU is one of the largest veterinary referral hospitals in Thailand, handling approximately 140,000 patient visits annually. The hospital comprises five main divisions: Intensive Care Unit (ICU), General Medicine, Surgical, Gynecological, and Special Units, including Cardiology, Nephrology, Diabetes, Dermatology, Oncology, Feline Medicine, and Neurology. During the study period, an average of 389 animal patients visited the hospital daily, distributed across General Medicine (96 patients), Gynecology (30), Dermatology (27), and Surgery (8).
The hospital’s sanitation management routine was standardized but varied slightly by location. Hallways were mopped daily using a 2.5% (w/v) quaternary ammonium compound disinfectant (Umonium38®; Laboratoire Huckert’s International, Thailand) between 3:30 PM and 4:00 PM. Examination tables, stethoscopes, syringe trays, waiting benches, drug cabinets, keyboards, and doorknobs were sanitized with 0.5% (w/v) Umonium38® spray during off-patient hours. Sampling locations were selected based on previously identified high hand-touch areas [28]. Wound-dressing cotton was stored in the same examination room until use. Forceps jars containing 1% (w/v) povidone–iodine solution (Betadine®; Pathum Thani, Thailand) were replenished daily.
Sampling strategy
Environmental sampling
A total of 216 environmental samples were collected from nine functional units of the VTH-CU: ICU (C), Dermatological Unit (SW), Gynecology (G), General Medicine (M), Post-surgery Care (P), Surgery (S), Vaccination (V), and both lower and upper hallways (L, U). At the time of collection, the Medicine, Dermatological, and Vaccination units were located in a newly constructed building, while Gynecology, Post-surgery, Surgery, and hallway areas were part of the older hospital wing.
The room inclusion criteria required a minimum of 8 animal patients per day. Environmental samples were collected twice on the same weekday, before clinic opening (7:30–8:00 AM) and after daily cleaning (3:30–4:00 PM). For each room, swabs were taken from five specific floor areas and frequently touched instruments, as summarized in Table 1.
Sampling was performed using sterile cotton swabs pre-moistened with 2 mL of peptone-saline diluent (100 mg/mL peptone and 850 mg/mL sodium chloride). The swab was rolled over the defined surface area, after which the cotton tip was aseptically detached, placed into the same tube, stored on ice, and processed within 2 h.
Veterinary staff sampling
One veterinary nurse from each clinical unit and 16 veterinarians, each with more than 2 years of service and over 40 working h/week, were enrolled. All participants routinely used protective masks while on duty. Sterile swabs were used to collect nasal cavity samples according to the standard protocol described by Chanchaithong et al. [29].
Canine patient sampling
Fourteen samples were obtained from superficial wound abscesses of dogs admitted to the Dermatological, Post-surgery Care, and Surgery rooms on the same days as environmental and personnel sampling. Outpatient dogs with wound infections or dermatitis were included following approval from the attending veterinarian. Each sterile swab was moistened in 2 mL of peptone saline diluent and applied to the wound site following the treatment protocol described by Chanchaithong et al. [29].
Culture and identification of isolates
All samples were cultured within 2 h of collection. A 0.1 mL aliquot of each bacterial suspension was inoculated onto Baird–Parker agar (Difco, France) plates with and without 0.5 µg/mL oxacillin for Staphylococcus screening, performed in duplicate. Black, Staphylococcus-like colonies were sub-cultured on tryptic soy agar (Difco) and examined for coagulase activity. Up to three coagulase-positive colonies per sample were retained for analysis.
Species identification was performed using standard biochemical tests [30], multiplex polymerase chain reaction (M-PCR), and matrix-assisted laser desorption/ionization–time of flight mass spectrometry (MALDI-TOF MS) [31, 32]. Control strains included S. aureus American Type Culture Collection (ATCC) 25923, S. pseudintermedius CVMC 0108, S. coagulans CVMC 0208, Staphylococcus intermedius CVMP 0309, Staphylococcus delphini CVMP 0109, and sterile water as the negative control.
Oxacillin (1 µg) and cefoxitin (30 µg) disk diffusion tests were performed according to Clinical and Laboratory Standards Institute (CLSI) guidelines [33]. Methicillin resistance was confirmed by mecA gene detection via PCR [34]. S. aureus ATCC 25923 and MRSA N315 served as positive controls.
Antimicrobial susceptibility testing
All confirmed MRCoPS isolates were tested for antimicrobial susceptibility using the disk diffusion method [33]. Antibiotics included clindamycin (DA) (2 µg), doxycycline (DO) (30 µg), erythromycin (E) (15 µg), gentamicin (CN) (10 µg), mupirocin (200 µg), and sulfamethoxazole/trimethoprim (25 µg) (Oxoid/Thermo Fisher Scientific, UK). S. aureus ATCC 25923 served as the control strain. Oxacillin (1 µg) was used for MRCoPS testing, and cefoxitin (30 µg) for S. aureus. Results were interpreted according to CLSI (2013) breakpoints; DO breakpoints were determined according to Maaland et al. [35].
Molecular typing of MRCoPS
The mec and ccr gene complexes were characterized in all MRCoPS isolates by M-PCR to determine SCCmec types [36]. Clonal relatedness was evaluated using PFGE following the method of Chanchaithong et al. [29]. Genomic DNA embedded in Seakem® agarose (Bio-Rad, USA) was digested with Cfr9I or ApaI restriction enzymes [37]. DNA fragments were separated using a CHEF-DR III apparatus (Bio-Rad) at 6 V/cm and 14°C with a pulse-switching interval of 5–15 s for 18 h, followed by 15–60 s for 5 h. Gels were stained with Red Safe™ Nucleic Acid Stain (iNtRON Bio, NSW, Australia) and visualized under ultraviolet illumination. A Lambda Ladder PFGE marker (New England BioLabs, USA) served as a size standard. Dendrograms were generated using BioNumerics software version 4.0 (Applied Maths, Kortrijk, Belgium) with the Dice coefficient (1.5%) and Unweighted Pair Group Method with Arithmetic mean (UPGMA) clustering, applying an 80% similarity threshold to define distinct pulsotypes [38].
Statistical analysis
All statistical analyses were performed using the Statistical Package for the Social Sciences Statistics 22 (IBM Corp., Chicago, IL, USA). The prevalence of Staphylococcus species was expressed as percentages for CoPS, methicillin-resistant (MRCoPS), and methicillin-susceptible CoPS (MSCoPS) isolates.
Associations between environmental factors and MRCoPS occurrence were analyzed using Chi-square or Fisher’s Exact Tests, with 95% confidence intervals (CI). Odds ratios (ORs) and adjusted odds ratios (AORs) were calculated to identify independent risk factors using multivariate logistic regression. Independent variables included room type (Gynecology, Post-surgery, Dermatological; Medicine as the reference), surface type (medical instruments vs. floor), cleaning frequency (once vs. twice daily), and antiseptic use (present vs. absent). Statistical significance was set at p < 0.05.
RESULTS
Prevalence and distribution of CoPS
A total of 253 samples were collected from environmental surfaces (n = 216), veterinary personnel (n = 23), and canine patients (n = 14) across nine functional units of the VTH-CU. Among these, 88 CoPS isolates were obtained from 48 positive samples, representing an overall isolation rate of 18.97%. Specifically, 40 isolates originated from environmental surfaces (15.81%), seven from canine wound swabs (2.76%), and one from the nasal cavity of a veterinarian (0.40%) (Table 2).
Among the 88 CoPS isolates, Staphylococcus pseudintermedius was the predominant species (n = 75; 85.23%), followed by S. coagulans (n = 12; 13.64%) and a single isolate of S. aureus (1.14%) obtained from a veterinary staff member. Methicillin resistance was detected in 62 isolates (70.5% of all CoPS), comprising 57 MRSP (91.9%) and 5 MRSC (8.1%).
Environmental and operational risk factors for MRCoPS contamination
Multivariate logistic regression analysis was performed to determine environmental predictors associated with MRCoPS contamination. The analysis identified surface type and room type as the major independent factors influencing contamination levels. After adjusting for confounding variables, medical instruments were significantly less likely to harbor MRCoPS compared with floor surfaces (AOR = 0.32; 95% CI: 0.12–0.86; p = 0.024). Floors were therefore identified as the principal environmental reservoirs for MRCoPS in the hospital.
The dermatological unit demonstrated the highest contamination risk, with odds of MRCoPS detection approximately 6 times greater than those in the medicine unit (AOR = 5.86; 95% CI: 1.22–28.14; p = 0.027). In contrast, neither increased cleaning frequency nor the use of antiseptics showed a statistically significant effect on MRCoPS occurrence (Table 2).
Of the 62 MRCoPS isolates, 26 were recovered from environmental surfaces, 5 from canine patients, and 1 from a veterinary staff member. Floor samples accounted for the majority of environmental contamination (16/26; 61.54%), followed by examination tables and other high-contact surfaces. The Dermatology and Post-surgery Care Units exhibited the highest proportion of MRCoPS-positive surfaces (up to 60%), whereas no MRCoPS was detected in the Vaccination Unit (Table 3).
Seven distinct antibiogram patterns were identified. The predominant resistance phenotype among MRSP isolates was CN–DA–E (CN, DA, and E). All MRSC isolates demonstrated the same triple-resistance pattern (CN–DA–E), confirming a consistent MDR phenotype across species (Figure 2).
Percentile of antibiotic drugs resistant to clindamycin, doxycycline, erythromycin, gentamicin, mupirocin, and sulfamethoxazole/trimethoprim; 2 drugs = resistant to 2 antibiotic drugs in the same samples; 3 drugs = resistant to 3 antibiotic drugs in the same samples; 4 drugs = resistant to 4 antibiotic drugs in the same samples; 5 drugs = resistant to 5 antibiotic drugs in the same samples.
Antimicrobial resistance profiles
All 62 MRCoPS isolates were tested for antimicrobial susceptibility to six commonly used veterinary antibiotics. Universal resistance to DA and E was observed. A high proportion of isolates (58/62; 93.5%) exhibited MDR, defined as resistance to three or more antimicrobial classes.
SCCmec typing
SCCmec typing revealed that all MRSC isolates possessed type V cassettes. In contrast, MRSP isolates exhibited both SCCmec type V and several untypeable variants, suggesting the circulation of atypical or possibly novel mec element configurations. The heterogeneity of SCCmec types among MRSP correlated with their diverse antimicrobial resistance profiles (Figures 3–5).
Staphylococcus pseudintermedius digested with Apal: The figure shows the staphylococcal cassette mec type and pulsed-field gel electrophoresis pattern of S. pseudintermedius isolates from various sources in the Small Animal Teaching Hospital; G = Gynecology room, IM = Internal Medicine room, P = Post-surgery, and N/A = not detected.
Staphylococcus pseudintermedius digested with Cfr9I: The figure shows the staphylococcal cassette mec type and pulsed-field gel electrophoresis pattern of S. pseudintermedius isolates from various sources in the Small Animal Teaching Hospital; G = Gynecology room, IM = Internal Medicine room, ICU = Intensive care unit, SW = Dermatological room, P = Post-surgery room, S = Surgery room, V = Vaccination room, H = Hall way, D = Dog, and N/A = not detected.
Staphylococcus coagulans digested with cfr9I: The figure shows the staphylococcal cassette mec type and pulsed-field gel electrophoresis patterns of S. coagulans isolates from various sources in the Small Animal Teaching Hospital; G = Gynecology room, IM = Internal Medicine room, ICU = intensive care unit, and H = Hallway.
Clonal relatedness of isolates
PFGE analysis demonstrated considerable genetic diversity among MRCoPS isolates. S. pseudintermedius isolates were grouped into 14 distinct PFGE patterns (A–N), while S. coagulans isolates were categorized into two major patterns (A and B). Notably, PFGE pattern A was shared among MRSP isolates from dogs and environmental samples obtained from the Dermatology, Gynecology, and Post-surgery Care units. This finding strongly indicates clonal dissemination of MRSP strains within the hospital environment.
Twelve S. pseudintermedius isolates were non-typeable using Cfr9I digestion but were successfully resolved with ApaI, yielding three additional unique banding profiles. This result suggests the presence of methylated or atypical restriction sites in certain isolates, reflecting genetic variability and potential genomic adaptation within circulating MRSP strains.
DISCUSSION
The management and veterinary staff at the VTH-CU, as in other major veterinary hospitals worldwide, recognize the critical threat posed by nosocomial infections, particularly those involving MDR pathogens such as MRCoPS. This study was therefore designed to systematically investigate the presence and distribution of CoPS and MRCoPS within the hospital environment, encompassing medical instruments, equipment, floors, staff nasal cavities, and lesions from canine patients. Identifying contamination “hotspots” for these pathogens is essential for guiding the implementation of improved infection prevention and control strategies in the VTH-CU.
Environmental persistence and reservoirs
MRCoPS, particularly MRSP, were frequently isolated from hospital floors and medical instruments across multiple rooms, indicating substantial environmental persistence despite routine sanitation. The consistently high contamination rate on floor surfaces, especially in the Dermatological Unit, reveals gaps in existing cleaning and disinfection protocols. Floors often act as reservoirs for pathogen accumulation and serve as hubs for indirect transmission through human footwear, equipment, or animal contact.
Although the VTH-CU followed standard cleaning procedures, the persistence of MRCoPS suggests potential inefficiencies related to disinfectant type, concentration, or application technique. More effective agents, such as sodium hypochlorite, 2% phenolic solutions, or 0.5% chlorhexidine, should be considered for integration into hospital sanitation regimens [25, 39]. In cases of persistent contamination, advanced surface-decontamination methods such as levulinic acid–sodium dodecyl sulfate combinations or the “MoWa” (spray-wash) technique have shown promising results [40]. Ensuring sufficient disinfectant contact time (≥20 min) and replacing mop-bucket solutions at least twice daily are critical operational measures. The persistence of MRCoPS even after cleaning underscores the need to revise these protocols as part of a targeted hospital-wide infection control plan.
Disinfection practices and protocol optimization
Examination tables, although disinfected between patient uses, were also found to harbor residual MRSP, particularly in the Dermatology, Gynecology, ICU, and Post-surgery Care Units. This persistence suggests suboptimal disinfection, likely due to inadequate contact duration or the use of less potent agents. Evidence-based cleaning guidelines, such as those recommended by Portner and Johnson [25], should be strictly followed.
In addition, reinforcing World Health Organization (WHO) hand-hygiene standards (e.g., alcohol-based rubs or 0.5% chlorhexidine) and adopting rapid-action disinfectants such as hydrogen peroxide, peracetic acid, or peroxymonosulfate, which provide significant microbial reduction within 5 min, could substantially reduce surface contamination and cross-transmission risks [41].
Implications of antimicrobial resistance
The widespread resistance of MRCoPS to critical antibiotics, notably DA and E, reflects an alarming MDR phenotype. This trend aligns with global evidence linking extensive antibiotic use, especially β-lactams, to the emergence of resistance in pathogens such as Enterococcus faecium, Acinetobacter baumannii, and Pseudomonas aeruginosa [42]. At the VTH-CU, β-lactam antibiotics were the most commonly prescribed in three clinical areas, yet MRCoPS were detected in five units, including one where enrofloxacin was predominantly used. Given that most MRCoPS isolates displayed resistance to multiple antibiotic classes, the routine empirical use of β-lactams may be ineffective against circulating strains. This highlights the urgent need to implement a robust Antimicrobial Stewardship Program (ASP) and continuous resistance surveillance to guide rational antibiotic use and minimize the spread of resistant pathogens [43, 44]. Although MRSA has been the traditional focus of most veterinary hospital studies, the present findings emphasize the growing clinical relevance of MRSP. Interestingly, reports from Brazil have documented a higher prevalence of MRSA than MRSP [43], whereas the current data from Thailand indicate the opposite. These differences may reflect geographical variation, antibiotic usage patterns, and local infection-control practices [13, 22].
MRSP prevalence in Thai veterinary facilities
The higher prevalence of MRSP observed in this study compared with previous reports from veterinary hospitals in southern Thailand [19, 22] can be attributed to the scale and activity level of the VTH-CU. As a central referral hospital managing a significantly larger patient load, the VTH-CU presents increased opportunities for bacterial shedding and environmental contamination. High patient turnover and the diverse range of clinical services contribute to the persistence and dissemination of MRSP across multiple hospital units.
Occupational exposure and human health risks
An MDR MRSP isolate was recovered from the nasal cavity of one veterinarian, consistent with previous findings of occupational exposure in veterinary personnel. Although MRSP carriage in humans remains relatively uncommon, it is strongly associated with close animal contact in veterinary settings [15, 29, 45, 46]. The reported human MRSP carriage rate typically ranges from 1% to 5%, with Thailand showing the highest prevalence (8%) [29].
In this study, the PFGE profile of the human isolate differed from those of canine or environmental sources, suggesting independent acquisition rather than direct transmission. Nonetheless, this underscores the occupational hazard faced by veterinary professionals. Stringent hand hygiene, proper use of personal protective equipment (PPE), and adherence to WHO protocols are essential preventive strategies, particularly in high-risk areas [26, 47–49].
Clonal dissemination and genetic diversity
The frequent use of antimicrobials in veterinary hospitals promotes the emergence of resistant commensal bacteria on animal skin and mucosal surfaces [50]. All canine patients in this study harbored CoPS, though only a subset carried methicillin resistance. PFGE analysis revealed a shared clonal pattern (pattern A) among MRSP isolates from dogs and environmental surfaces in the Dermatology, Gynecology, and Post-surgery Care Units, indicating clonal dissemination within the hospital. This pattern aligns with earlier findings of MRSP contamination on surgical instruments and in infected dogs [19].
Some MRSP isolates were untypeable by standard SCCmec typing, possibly due to atypical or hybrid genetic elements such as ΨSCCmec57395 or SCCmecAI16-SCCczrAI16-CI, previously detected in Thailand [50, 51]. The diversity of SCCmec structures and their association with MDR highlight the dynamic genetic evolution of MRSP under selective antimicrobial pressure. Given that SCCmec is a mobile element capable of transferring resistance genes across Staphylococcus species, stringent infection-control policies are critical to curbing its intra-hospital dissemination.
Interestingly, 12 S. pseudintermedius isolates were non-typeable using Cfr9I but could be digested with ApaI, a restriction enzyme used for MRSA sequence type 398 [52]. This difference implies the presence of methylated or atypical restriction sites and further underscores the genetic heterogeneity of circulating MRSP strains. Whole-genome sequencing is warranted to characterize these untypeable isolates and elucidate potential novel genomic adaptations.
Future directions and one health implications
The findings reaffirm the interconnectedness of animal, human, and environmental health within the One Health framework. MRCoPS, including MRSA, MRSP, and MRSC, are zoonotic agents capable of cross-transmission between species and persistence on environmental surfaces and medical devices [13, 18, 53, 54]. The detection of identical or closely related clones among hospital staff, patients, and surfaces underscores the need for integrated surveillance and infection-control systems.
Based on these insights, a comprehensive infection-control strategy for the VTH-CU is recommended, structured around three domains:
- Human domain: Enforce strict hand hygiene (WHO’s five moments of hand hygiene [55]), PPE usage (gloves, masks, and gowns), and occupational screening programs to minimize zoonotic exposure [26, 47, 48]
- Animal domain: Implement prudent antimicrobial use, targeted screening for high-risk or recurrently treated animals, and isolation protocols for colonized or infected patients
- Environmental domain: Strengthen cleaning frequency (especially in high-risk units), ensure appropriate disinfectant selection and contact time, and establish standardized sanitation and accreditation frameworks [22, 43].
Annual environmental and clinical MRCoPS surveillance should be institutionalized to support early detection and continuous quality improvement. Collectively, these interventions will mitigate the spread of MDR Staphylococcus species, safeguard both animal and human health, and reinforce biosecurity within veterinary facilities.
CONCLUSION
This study provides comprehensive insight into the prevalence, molecular epidemiology, and antimicrobial resistance of MRCoPS in a major VTH in Thailand. Among 253 samples collected from the environment, veterinary personnel, and canine patients, S. pseudintermedius predominated (85.23%), followed by S. coagulans (13.64%), with 70.5% of all isolates confirmed as methicillin-resistant. Floors and high-contact surfaces, particularly in the Dermatological and Post-surgery Care Units, represented major environmental reservoirs, while one veterinary staff member harbored an MDR MRSP strain. Most MRCoPS isolates were resistant to DA and E, and 93.5% exhibited MDR, highlighting the threat of therapeutic failure and nosocomial transmission. PFGE analysis confirmed clonal relatedness between canine and environmental isolates, indicating intra-hospital dissemination.
These findings emphasize the urgent need for strengthened hospital sanitation protocols, evidence-based disinfectant use, and routine environmental surveillance. Implementation of ASPs, combined with hand hygiene compliance and PPE use, can substantially reduce the risk of MRCoPS transmission among animals and staff. The study’s main strength lies in its integrated approach, linking molecular typing, antimicrobial profiling, and statistical risk assessment. However, it was limited to a single institution and a cross-sectional sampling design, which restricts temporal interpretation and generalization to other hospital settings.
Longitudinal monitoring, genomic characterization of untypeable SCCmec variants, and evaluation of disinfection efficacy are warranted to better understand persistence mechanisms and emerging clones. The detection of widespread MRSP contamination and evidence of clonal spread underscore the necessity of adopting One Health-based infection-control strategies to safeguard both animal and human health within veterinary facilities.
AUTHORS’ CONTRIBUTIONS
PF: Designed the study, sampling, isolation, characterization of the various bacterial isolates, pulsed-field gel electrophoresis, data analysis, and drafted the manuscript. JM: Conducted MALDI-TOF MS, analyzed the results, and edited the manuscript. DJH and NP: Conceptualized the study, analyzed the data, and edited the manuscript. All authors have read and approved the published version of the manuscript.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Yang C Chen X Li M Yuan W Li S Han D Feng J Luo H Zheng M Liang J Chen C Qu P Li S Author correction:Genomic epidemiology and phenotypic characterization of Staphylococcus aureus isolated from atopic dermatitis patients in South China Sci. Rep 202515191914009760110.1038/s 41598-025-93289-7PMC 11914183 · doi ↗ · pubmed ↗
- 2Pleskova S.N Bobyk S.Z Kriukov R.N Gorshkova E.N Bezrukov N.A Staphylococcus aureus causes the arrest of neutrophils in the bloodstream in a septicemia model Microorganisms 202210(9)16963614429810.3390/microorganisms 10091696 PMC 9502802 · doi ↗ · pubmed ↗
- 3Ariens R.A.S Cassat J.E Surviving a sticky situation:Therapeutic administration of fibrinogen variant γ'improves outcomes of Staphylococcus aureus septicemia J. Thromb. Haemost 2023218204820503746817410.1016/j.jtha.2023.04.013PMC 10947783 · doi ↗ · pubmed ↗
- 4Marek L Irimaso E Turikumwenayo J.B Mukamulisa B Ndishimye P Muragijemariya F Cabal-Rosel A Desvars-Larrive A Fischer O.W Szostak M.P Muller E Braun S.D Ehling-Schulz M Spergser J Grunert T Ruppitsch W Fessler A.T Schwarz S Monecke S Ehricht R Kunzel F Loncaric I Staphylococcus aureus in Rwandan dogs predominantly representing human-associated lineages Lett. Appl. Microbiol 202578(5)ovaf 0654028739510.1093/lambio/ovaf 065 · doi ↗ · pubmed ↗
- 5Katakweba A.A.S Iversen C.M Tsaxra J.B Muhairwa A.P Moodley A Olsen J.E Brief communication:Carrier rate, antimicrobial resistance and molecular typing of Staphylococcus aureus and Staphylococcus pseudintermedius in healthy dogs from Morogoro, Tanzania Vet. Dermatol 20243555575623888795610.1111/vde.13272 · doi ↗ · pubmed ↗
- 6Del Pilar Zarazaga M Tinti M.G Litterio N.J Himelfarb M.A Andres-Larrea M.I.S Rubio-Langre S Serrano-Rodriguez J.M Lorenzutti A.M Dose regimen optimization of cephalothin for surgical prophylaxis against Staphylococcus aureus and coagulase-negative staphylococci in dogs by pharmacokinetic/pharmacodynamic modeling Res. Vet. Sci 20241711052023849227910.1016/j.rvsc.2024.105202 · doi ↗ · pubmed ↗
- 7Cengiz S Okur S Oz C Turgut F Gumurcinler B Sevuk N.S Kekec A.I Cepoglu H Sevimli U Adiguzel M.C Prevalence and clonal diversity of methicillin-resistant Staphylococcus aureus and methicillin-resistant Staphylococcus pseudintermedius isolated from dogs and cats with eye discharge Acta Microbiol. Immunol. Hung 20237021341413672393310.1556/030.2023.01899 · doi ↗ · pubmed ↗
- 8Hammer N.D Cassat J.E Noto M.J Lojek L.J Chadha A.D Schmitz J.E Creech C.B Skaar E.P Inter-and intraspecies metabolite exchange promotes virulence of antibiotic-resistant Staphylococcus aureus Cell Host Microbe 20141645315372529933610.1016/j.chom.2014.09.002PMC 4197139 · doi ↗ · pubmed ↗