Public Electric Baths in Japan: A Risk of Inappropriate Implantable Cardioverter‐Defibrillator Shock
Takahisa Ido, Takashi Nakashima, Makoto Yamaura, Shigekiyo Takahashi, Takuma Aoyama

TL;DR
A man in Japan received an unnecessary electric shock from a public bath due to his implantable defibrillator.
Contribution
This is the first documented case of an inappropriate implantable cardioverter-defibrillator shock caused by a public electric bath in Japan.
Findings
A public electric bath triggered an inappropriate shock in a patient with an S-ICD.
This incident highlights potential risks of public electric baths for patients with implantable devices.
Abstract
This case represents the first reported instance of an inappropriate S‐ICD shock caused by a public electric bath in Japan.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
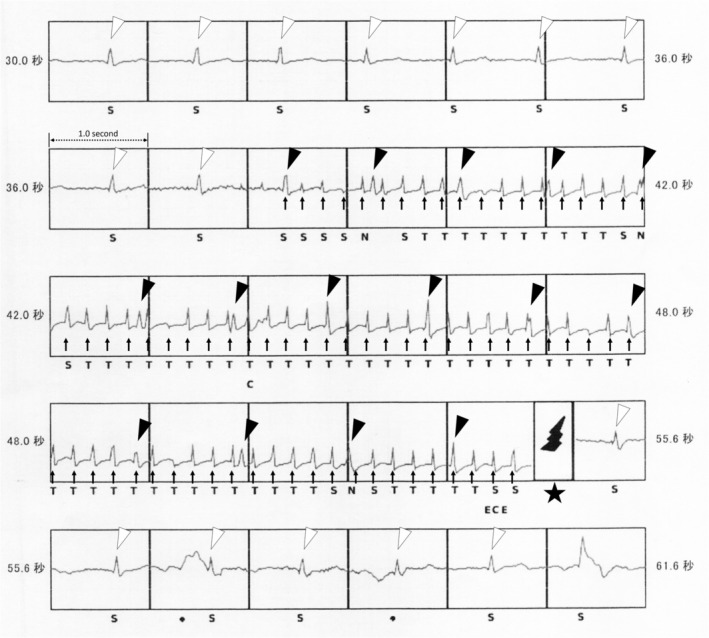 FIGURE 1
FIGURE 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPotassium and Related Disorders · Cardiac pacing and defibrillation studies · Medical Device Sterilization and Disinfection
Case Presentation
1
A 50‐year‐old man was diagnosed with idiopathic ventricular fibrillation (VF) after experiencing a cardiopulmonary arrest due to VF three years earlier. A subcutaneous implantable cardioverter‐defibrillator (S‐ICD; EMBLEM MRI S‐ICD, model A219, Boston Scientific, Natick, MA) was implanted for secondary prevention. The S‐ICD sensing filter (SMART Pass) was activated. The sensing vector was set to the secondary vector, which is recorded between the distal ring on the lead and the can. The shock zone was programmed at 240 beats per minute (cycle length: 250 milliseconds [ms]). The patient was instructed to avoid “denki‐buro” (electric baths), a common feature in Japanese public baths where a mild electric current is discharged into the water.
During a routine outpatient follow‐up, device interrogation revealed an ICD shock (Figure 1). The pacing threshold, sensing sensitivity, and lead impedance were all within normal limits. A medical interview revealed that the patient had fallen in a public bathhouse and had accidentally immersed his left upper limb—from the fingertips to the shoulder—in the “denki‐buro” at the time the S‐ICD shock was delivered. No other body parts were submerged. He had no predisposing symptoms. Simultaneously with the defibrillator discharge, he withdrew his left upper limb from the water.
The tracing shows an inappropriate S‐ICD shock induced by the “denki‐buro.” High‐frequency signals with a cycle length of approximately 200 ms are detected as ventricular fibrillation (arrows), resulting in shock delivery (star). Dissociated sinus QRS complexes are also present (black and white arrowheads).
The intracardiac electrogram revealed high‐frequency signals with a cycle length of approximately 200 ms. These signals were interpreted as VF and subsequently triggered shock delivery (arrows and star in Figure 1). During VF detection, regular signals with a cycle length of 1000–1100 ms were also present (black arrowheads). These signals were dissociated from the high‐frequency signals, showed relatively regular intervals, and were similar to those recorded before VF detection (white arrowheads). Therefore, the regular signals observed during VF detection were presumed to represent QRS complexes of the underlying sinus rhythm. The high‐frequency signals interpreted as VF were, in fact, external noise generated by the “denki‐buro.” Based on the medical interview and the intracardiac electrogram findings, we concluded that the ICD shock had been inappropriately delivered due to electric currents from the “denki‐buro.”
Inappropriate ICD shocks may be caused by external electromagnetic interference and have been associated with increased mortality [1]. A “denki buro,” is relatively common in Japan [2]. In Japan, the use of “denki‐buros” is prohibited for patients with cardiac implantable electronic devices. However, inappropriate ICD shocks induced by “denki‐buros” have rarely been reported. Inappropriate ICD shocks induced by a public “denki‐buro” have previously been reported in a patient with a transvenous ICD [2]. To the best of our knowledge, no such cases have been reported in patients with an S‐ICD.
This is the first reported case of an inappropriate ICD shock caused by a “denki‐buro” in a patient with an S‐ICD. Physicians should be aware that a “denki‐buro” may trigger inappropriate ICD shocks in patients with ICDs. Inappropriate shocks can occur despite prior patient awareness. Patients, as well as public bath operators, should be informed of this potential risk.
Funding
The authors have nothing to report.
Ethics Statement
This study was approved by the institutional review board of Central Japan International Medical Center.
Consent
Informed consent was obtained from the patient.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1J. B. van Rees , C. J. Borleffs , M. K. de Bie , et al., “Inappropriate Implantable Cardioverter‐Defibrillator Shocks: Incidence, Predictors, and Impact on Mortality,” Journal of the American College of Cardiology 57 (2011): 556–562.21272746 10.1016/j.jacc.2010.06.059 · doi ↗ · pubmed ↗
- 2M. Hashimoto , K. Yamagata , J. Yokota , I. Tanikawa , and K. Fujiu , “Denki Buro: A Japanese Electric Bath in Public Space Causing Inappropriate ICD Shock,” Journal of Interventional Cardiac Electrophysiology 67 (2024): 1501–1503.38848008 10.1007/s 10840-024-01832-9PMC 11522063 · doi ↗ · pubmed ↗