Case Report: Successful treatment of pityriasis rubra pilaris with deucravacitinib
Yixuan Li, Meiliang Guo, Ziyao Sheng, Zhehong Zhou, Na Liu, Qinqin Meng, Hui Deng

TL;DR
A 39-year-old man with a rare skin disease called pityriasis rubra pilaris showed significant improvement after being treated with a new drug called deucravacitinib.
Contribution
This is the first reported case of using a TYK2 inhibitor (deucravacitinib) to successfully treat pityriasis rubra pilaris.
Findings
The patient showed significant improvement in erythema, desquamation, and pruritus after one month of treatment with deucravacitinib.
At the six-month follow-up, skin lesions almost resolved, with only mild erythema and desquamation remaining.
The treatment improved both disease severity and the patient's quality of life without major side effects.
Abstract
Pityriasis rubra pilaris (PRP) is a rare inflammatory skin disease characterized by hyperkeratotic follicular papules, palmoplantar hyperkeratosis, and associated normal “islands of unaffected skin”. Its pathogenesis has not been fully elucidated, and treatment poses significant challenges. Conventional therapies include oral retinoids and topical emollients. In recent years, although biological agents have been used in treatment, they are associated with side effects such as an increased risk of infection, and some patients show no response to treatment, thus necessitating the exploration of new therapeutic approaches.This case represents the first reported use of a TYK2 inhibitor (deucravacitinib) for the treatment of PRP. The patient was a 39-year-old male who developed extensive erythema in December 2024. The erythema gradually increased and progressed to red punctate eruptions…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1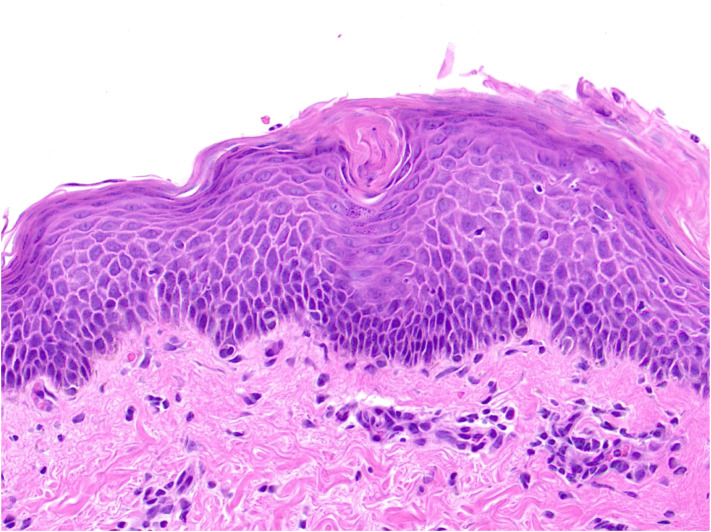 Figure 2
Figure 2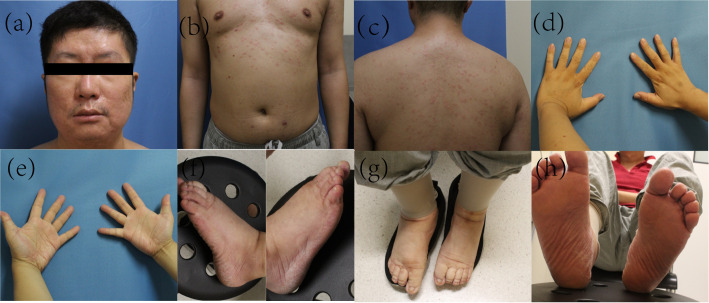 Figure 3
Figure 3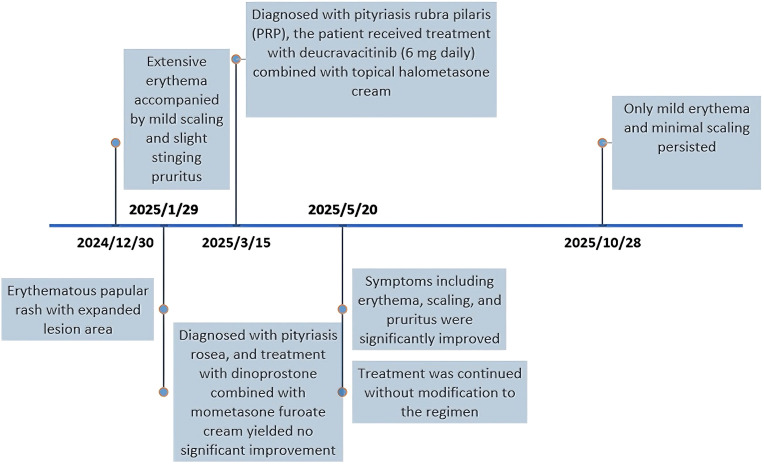 Figure 4
Figure 4- —National Natural Science Foundation of China10.13039/501100001809
- —Fundamental Research Funds for the Central Universities10.13039/501100012226
- —China Postdoctoral Science Foundation10.13039/501100002858
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSkin Diseases and Diabetes · Psoriasis: Treatment and Pathogenesis · Cutaneous lymphoproliferative disorders research
Introduction
Pityriasis rubra pilaris (PRP) is a rare inflammatory skin disorder characterized by hyperkeratotic follicular papules, palmoplantar hyperkeratosis, and well-demarcated orange-red scaly plaques with intervening normal “islands of sparing” (1). Due to its incompletely understood pathogenesis, treatment remains a significant challenge. Traditional therapies include oral retinoids (1) and topical emollients to alleviate symptomatic discomfort. Recent studies have implicated dysregulation of the IL-23/Th17 axis in PRP pathogenesis (2), providing a theoretical basis for the use of biologics such as ustekinumab and secukinumab in PRP treatment. Additionally, Janus kinase (JAK) inhibitors and phosphodiesterase-4 (PDE4) inhibitors have shown promising efficacy in PRP management (3–5). However, the potential side effects of biologics and small-molecule inhibitors, including increased infection risk, cannot be overlooked. Moreover, some patients remain refractory to these treatments, necessitating the exploration of novel therapeutic options. We report the first case of significant improvement in PRP skin lesions using deucravacitinib, a TYK2 inhibitor.
The patient was a 39-year-old male with a history of hypertension. In December 2024, he developed a large erythematous patch that gradually increased in number, accompanied by mild scaling and slight prickling pruritus, which later progressed to red punctate rashes with expanding lesion areas. Physical examination revealed generalized erythema and scaly plaques with follicular hyperkeratosis affecting the trunk, abdomen, limbs, face, and scalp, with visible “islands of sparing” (Figure 1). Initially, he was diagnosed with pityriasis rosea, but treatment with dinoprostone combined with mometasone furoate cream for one month yielded no significant improvement. To further confirm the diagnosis, a pathological section was performed for him.Histopathological examination showed squamous epithelial hyperplasia with parakeratosis, elongated rete ridges, edema in the papillary dermis, and perivascular infiltration of numerous chronic inflammatory cells and the presence of cutaneous horny plugs (Figure 2). Initial treatment with topical dinoprostone and mometasone furoate cream yielded no significant improvement. Based on histological findings and clinical presentation, a diagnosis of pityriasis rubra pilaris was favored, with the specific subtype being typical adult-type pityriasis rubra pilaris. After taking the medical history, it was found that the patient was infected with COVID-19 in December 2022. In addition, a previous literature has reported a case of pityriasis rubra pilaris following COVID-19 infection, which may suggest a potential association with the onset of the disease (6). The patient had no other specific infection history or relevant family history prior to the onset of skin lesions. Previous studies have indicated that the efficacy of acitretin varies from person to person. A systematic review conducted by Kromer et al. showed that only 43 out of 174 pityriasis rubra pilaris (PRP) patients achieved favorable efficacy after receiving acitretin treatment (7).Considering that deucravacitinib is non-immunogenic, which reduces the production of anti-drug antibodies and thus ensures more stable long-term therapeutic efficacy. Meanwhile, deucravacitinib selectively inhibits tyrosine kinase 2 (TYK2) without exerting inhibitory effects on other Janus kinases, thereby decreasing the incidence of adverse reactions. In addition, deucravacitinib has shown favorable efficacy in improving psoriasis in special sites such as palms, soles, scalp and nails. Therefore, we recommend deucravacitinib for the treatment of the patient. On March 4, 2025, the patient began treatment with deucravacitinib (6 mg daily), combined with topical halometasone cream. At the first follow-up (1 month), significant improvements in erythema, scaling, and pruritus were observed. The patient continued deucravacitinib therapy. By the final visit to our hospital (6 months), his lesions had nearly resolved, with only mild erythema and minimal scaling remaining (Figure 3). The Psoriasis Area and Severity Index (PASI) score decreased from 33.5 to 2.6, and Dermatology Life Quality Index (DLQI) score improved from 23 to 4, indicating substantial improvements in both disease severity and quality of life. These results demonstrate the significant potential of our treatment regimen in managing PRP.
Systemic PRP leisions before the initiation of treatment. The images show the face, chest and back of the patient with histologically confirmed pityriasis rubra pilaris at initial presentation with follicular papules, scaly red-orange patches (a–c). Additionally, hyperkeratotic plaques are observed on the bilateral palms, the dorsum of the hands (d, e), as well as the dorsal and plantar feet (f–h).
Histopathological examination showed squamous epithelial hyperplasia with parakeratosis, elongated rete ridges, edema in the papillary dermis, and perivascular infiltration of numerous chronic inflammatory cells and the presence of cutaneous horny plugs.
Systemic PRP leisions after 6 months of treatment. At months 7 of deucravacitinib therapy, the erythema on the face, anterior and posterior chest was significantly relieved (a–c), and the hyperkeratosis on both hands and feet was markedly improved (d–h).
Similar to other rare diseases, the low incidence of PRP makes large-scale controlled trials challenging, complicating the development of widely accepted, effective treatment guidelines. Currently, systemic retinoids are the most commonly used treatment. In recent years, case reports have documented the use of biologics and small-molecule inhibitors; however, their potential side effects, such as increased infection risk, remain a concern.
Pityriasis rubra pilaris is classified into six subtypes: Classical adult (I), Atypical adult (II), Classical juvenile (III), Circumscribed juvenile (IV), Atypical juvenile (V), HIV-related (VI), In this case, the patient is classified as Type I, it’s the commonest type (55% of cases), cephalocaudal progression, ‘suberythrodermia’ with nappes claires, palmoplantar keratoderma (1). This case represents the first report of a TYK2 inhibitor used to treat PRP. The timeline of onset, diagnosis and treatment for this patient is shown in Figure 4. We observed that PRP shares significant genetic and immunological overlap with psoriasis (8), as well as similarities in clinical and histopathological features. Studies have shown that TYK2 inhibitors bind to the regulatory domain of TYK2 (a Janus kinase), disrupting IL-23, IL-12, and type I interferon signaling pathways, which are considered critical in psoriasis pathogenesis (9). TYK2 inhibitors, including deucravacitinib, have demonstrated a favorable safety profile. Deucravacitinib has shown remarkable efficacy in psoriasis treatment, effectively alleviating symptoms, reducing clinical manifestations, and significantly improving patients’ quality of life (10). The drug has also recently received FDA approval for moderate-to-severe psoriasis. Our study highlights the efficacy and safety of deucravacitinib in PRP treatment. Nowadays, the patient is still receiving continuous medication. During the follow-up period, the patient’s condition has remained stable without signs of recurrence, but data regarding the disease progression and potential recurrence risk after drug withdrawal are still lacking. In subsequent research, continuous follow-up of this case will be conducted to further improve the relevant data. Moreover, future clinical trials are needed to further investigate its therapeutic potential and safety profile in PRP management.
Case timeline.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Roenneberg S Biedermann T . Pityriasis rubra pilaris: algorithms for diagnosis and treatment. J Eur Acad Dermatol Venereol. (2018) 32:889–98. doi: 10.1111/jdv.14761, PMID: 29247481 · doi ↗ · pubmed ↗
- 2Potestio L D’Agostino M Portarapillo A Esposito V Tommasino N Salsano A . Emerging role of biologic drugs targeting IL-17 and IL-23: pityriasis rubra pilaris. Life (Basel). (2024) 14:923. doi: 10.3390/life 14080923, PMID: 39202665 PMC 11355122 · doi ↗ · pubmed ↗
- 3Inoue E Arase N Hanaoka Y Tanemura A Fujimoto M . The beneficial effect of a PDE 4 inhibitor in a patient with juvenile-onset intractable pityriasis rubra pilaris without CARD 14 mutation. Dermatol Ther. (2021) 34:e 14714. doi: 10.1111/dth.14714, PMID: 33368948 · doi ↗ · pubmed ↗
- 4Saad M Spurr A Lipson J . Pityriasis rubra pilaris partially responsive to treatment with upadacitinib: A case report. SAGE Open Med Case Rep. (2023) 11:2050313 X 231160927. doi: 10.1177/2050313 X 231160927, PMID: 37009550 PMC 10064474 · doi ↗ · pubmed ↗
- 5Tan H Zhang B Kang X Wang L Qiu X Hu X . Tofacitinib for pityriasis rubra pilaris: A case report. Clin Cosmet Investig Dermatol. (2024) 17:1917–20. doi: 10.2147/CCID.S 470170, PMID: 39220289 PMC 11363948 · doi ↗ · pubmed ↗
- 6Aromolo IF Pisapia A Riva D Barberi F Marzano AV Moltrasio C . COVID-19 induced pityriasis rubra pilaris: A superantigenic disease? J Eur Acad Dermatol Venereol. (2023) 37:e 26–8. doi: 10.1111/jdv.18556, PMID: 35993491 PMC 9538733 · doi ↗ · pubmed ↗
- 7Kromer C Sabat R Celis D Mössner R . Systemic therapies of pityriasis rubra pilaris: a systematic review. J Dtsch Dermatol Ges. (2019) 17:243–59. doi: 10.1111/ddg.13718, PMID: 30520557 · doi ↗ · pubmed ↗
- 8Fuchs-Telem D Sarig O van Steensel MA Isakov O Israeli S Nousbecket J . Familial pityriasis rubra pilaris is caused by mutations in CARD 14. Am J Hum Genet. (2012) 91:163–70. doi: 10.1016/j.ajhg.2012.05.010, PMID: 22703878 PMC 3397268 · doi ↗ · pubmed ↗