The course of respiratory tract infections in pediatric hemato-oncology patients during and after the COVID-19 pandemic: single center retrospective cohort study
Yeter Düzenli Kar, İmran Sağlık, Gökalp Rüstem Aksoy, Harun Ağca, Aytül Temuroğlu, Cem Uğur Mete, Melike Sezgin Evim, Büşra Safiye Beygo, Ahmet İbrahim Aydoğan, Çağlar Ödek, Solmaz Çelebi, Mustafa Hacımustafaoğlu, Güven Özkaya, Adalet Meral Güneş

TL;DR
This study examines respiratory tract infections in children with blood or cancer disorders before and after the COVID-19 pandemic, finding increased infection rates after pandemic restrictions eased.
Contribution
The study identifies rhinovirus/enterovirus as the most common cause of RTI in this vulnerable group and highlights a post-pandemic surge in infections.
Findings
Rhinovirus/enterovirus and influenza A/B were the most common RTI pathogens.
Post-pandemic RTI outbreaks increased significantly after non-pharmacological measures were reduced.
LRTI was associated with more severe clinical outcomes compared to URTI.
Abstract
Respiratory tract infections (RTI) are a leading cause of hospitalization in children and remain a significant contributor to morbidity. Our study aimed to examine the epidemiology of RTI in children with hemato-oncologic disease during and after the coronavirus 2019 (COVID-19) pandemic. This retrospective study evaluated nasopharyngeal swab samples that were tested using multiplex PCR from 185 children hospitalized with respiratory symptoms between January 2020 and March 2025. A total of 313 RTI agents were identified in 185 children with hemato-oncologic disorders across 271 infectious episodes. The median age was 6 years. The infection rates for upper respiratory tract infections (URTI) and lower respiratory tract infections (LRTI) were 45% and 55%, respectively. A statistically significant difference was found between patients with URTI and LRTI in terms of CRP, tachypnea,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
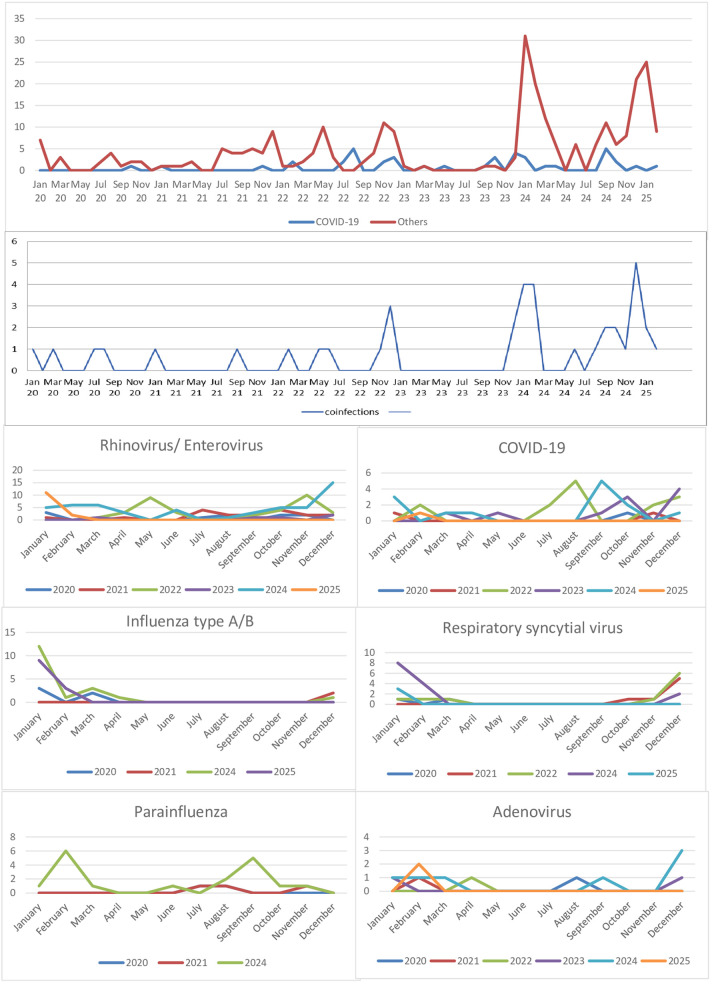 Figure 1
Figure 1| Variables (All episodes) | URTI ( | LRTI ( |
| |
|---|---|---|---|---|
| Age, year | 5 (0.3-21) | 7 (0.3-23) | 0.062 | |
| Gender | Female | 61 (50%) | 64 (43%) | 0.247 |
| Male | 61 (50%) | 85 (57%) | ||
| Diagnosis at episodes | Leukemia/MDS/JMML | 52 (42.6%) | 73 (49%) | 0.051 |
| Solid tumor | 43 (35.2%) | 44 (29.5%) | ||
| HSCT | 3 (2.5%) | 13 (8.7%) | ||
| Benign hematologic disorders | 24 (19.7%) | 19 (12.8%) | ||
| Laboratory | ||||
| White blood cell count (/mm3) | 3,800 ± 4,107 | 5,121 ± 13,619 | 0.303 | |
| White blood cell count category | Leukopenia (<4,000) | 90 (32.2%) | 104 (38.4%) | 0.719 |
| Normal (4,000–10,000) | 24 (8.9%) | 32 (11.8%) | ||
| Leukocytosis (>10,000) | 8 (3%) | 13 (4.8%) | ||
| Absolute neutrophil count (/mm3) | 1,834 ± 2,580 | 2,530 ± 6,123 | 0.242 | |
| Neutropenia status | Neutropenic | 76 (28%) | 95 (35.1%) | 0.804 |
| Non-neutropenic | 46 (17%) | 54 (19.9%) | ||
| Absolute lymphocyte count (/mm3) | 1,329 ± 1,575 | 1,850 ± 7,528 | 0.453 | |
| Lymphopenia status | Lymphopenic | 90 (33.2%) | 118 (43.5%) | 0.293 |
| Non-lymphopenic | 32 (11.8%) | 31 (11.4%) | ||
| Monocyte count (/mm3) | 470 ± 719 | 539 ± 789 | 0.460 | |
| HGB (g/dL) | 9.5 ± 1,9 | 9.1 ± 2.05 | 0.114 | |
| Thrombocyte count (/mm3) | 173.525 ± 145.647 | 164.315 ± 164.053 | 0.630 | |
| Eosinophil count (/mm3) | 71 ± 142 | 52 ± 126 | 0.262 | |
| CRP(mg/L) | 32 ± 38 | 56 ± 78 | 0.001 | |
| Fungal co-infection | 1 (0.8%) | 4 (2.7%) | 0.383 | |
| Bacteriemia | 0 | 9 (6%) | 0.005 | |
| Clinical findings | ||||
| Cough | 48 (39.7%) | 75 (50.3%) | 0.080 | |
| Fever | 99 (81%) | 129 (86.6%) | 0.224 | |
| Tachypnea, dyspnea | 2 (1.6%) | 30 (20.1%) | <0.001 | |
| Fever duration | 2 (1–11) | 2 (1–21) | 0.015 | |
| Infection-related length of stay | 7 (1–28) | 8 (1–45) | 0.001 | |
| Intensive care requirement | – | 13 (8.7%) | – | |
| Oxygen requirements | Nasal Mask | – | 11 (7.4%) | – |
| High-flow nasal oxygenation | – | 2 (1.3%) | ||
| Invasive mechanical ventilation | – | 11 (7.4%) | ||
| All infectious episodes | Lockdown period | 10 (43.4%) | 13 (56.6%) | 0.984 |
| Relaxation period | 41 (45.5%) | 49 (54.5) | ||
| After the end of COVID19 outbreak | 71 (45%) | 87 (55%) | ||
| Infectious episodes |
| 57 (46.7%) | 54 (36.2%) | 0.018 |
|
| 17 (13.9%) | 12 (8.1%) | ||
|
| 8 (6.6%) | 19 (12.8%) | ||
|
| 10 (8.2%) | 16 (10.7%) | ||
|
| 11 (9.0%) | 5 (3.4%) | ||
|
| 5 (4.1%) | 4 (2.7%) | ||
|
| 3 (2.5%) | 6 (4.0%) | ||
|
| 1 (0.8%) | 1 (0.7%) | ||
|
| 0 (0%) | 1 (0.7%) | ||
|
| 1 (0.8%) | 1 (0.7%) | ||
|
| 0 (0%) | 1 (0.7%) | ||
| Co-infection | 9 (7.4%) | 29 (19.5%) | ||
| Co-infection episodes | Lockdown period | 2 (1.6%) | 3 (2.0%) | 1.000 |
| Relaxation period | 0 (0%) | 8 (5.4%) | 0.009 | |
| After the end of COVID19 outbreak | 7 (5.7%) | 18 (12.1%) | 0.073 | |
| All infectious agents | Lockdown period | Relaxation period | After the end of the COVİD19 outbreak | Total |
|
|---|---|---|---|---|---|
|
| 12 (43.0) | 52 (53.6) | 70 (37.2) | 134 (42.8) | <0.001 |
|
| 2 (7.1) | 17 (17.5) | 22 (11.7) | 41 (13.1) | |
|
| 5 (17.9) | 2 (2.1) | 30 (16.0) | 37 (11.8) | |
|
| 2 (7.1) | 17 (17.5) | 17 (9.0) | 36 (11.5) | |
|
| 2 (7.1) | 3 (3.1) | 18 (9.6) | 23 (7.3) | |
|
| 2 (7.1) | 2 (2.1) | 10 (5.3) | 14 (4.5) | |
|
| 2 (7.1) | 3 (3.1) | 8 (4.3) | 13 (4.2) | |
|
| 0 (0.0) | 0 (0.0) | 6 (3.2) | 6 (1.9) | |
|
| 0 (0.0) | 0 (0.0) | 4 (2.1) | 4 (1.3) | |
|
| 0 (0.0) | 0 (0.0) | 3 (1.6) | 3 (1.0) | |
|
| 1 (3.6) | 1 (1.0) | – | 2 (0.6) | |
| Total | 28 (8.9) | 97 (31) | 188 (60.1) | 313 (100) | <0.001 |
| No | Age (year) | Infection date | Gender | Agents | Bacterial or fungal or viral coinfections | Diagnosis | Neutrophil count (/mm3) | Lymphocyte count (/mm3) | Monocyte count (/mm3) | C-Reactive Protein (mg/L) | Last stiuation | Causes of death |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 8 | 10.02.2020 | Male |
| ALL + HSCT + GvHD | 1.443 | 565 | 446 | 2 | Ex | LRTI + Lung GvHD | |
| 2 | 2 | 07.08.2020 | Female | CMV viremia | Combined Immunodeficiency | 1.930 | 144 | 229 | 144 | Ex | LRTI + CMV viremia | |
| 3 | 6 | 18.08.2020 | Male |
| – | Hodgkin lymphoma | 1.620 | 1.210 | 1.706 | 54 | Ex | LRTI |
| 4 | 13 | 08.11.2021 | Male |
| – | AML | 0 | 190 | 16 | 255 | Ex | LRTI |
| 5 | 3 | 11.04.2022 | Female |
| – | MDS | 370 | 2.380 | 2.480 | 21 | Ex | LRTI + intracranial hemorrhage |
| 6 | 4 | 16.12.2022 | Male | – | ALL + HSCT + GvHD | 11.830 | 880 | 474 | 57 | Alive | – | |
| 7 | 13 | 16.03.2023 | Male |
| – | AML following MDS | 9.100 | 1.650 | 2.780 | 18 | Alive | – |
| 7 | 13,5 | 20.09.2023 | Male |
| – | AML following MDS | 540 | 1.100 | 178 | 51 | Ex | LRTI |
| 8 | 12 | 29.01.2024 | Female |
| – | Ewing Sarcoma | 6.200 | 280 | 669 | 157 | Ex | LRTI + progressive disease |
| 9 | 16 | 12.11.2024 | Female |
| – | ALL | 3.520 | 300 | 362 | 278 | Alive | – |
| 10 | 4 | 28.11.2024 | Male |
| – | Combined Immunodeficiency + HSCT + GvHD | 14.900 | 330 | 826 | 53 | Alive | – |
| 11 | 13 | 06.12.2024 | Female | Stenotrophomonas maltophilia + Mucorales spp. in the nasal septum | Anaplastic ependimoma | 720 | 180 | 91 | 463 | Ex | LRTI + progressive disease | |
| 12 | 14 | 13.01.2025 | Female |
| Pineoblastoma | 8.340 | 710 | 249 | 381 | Ex | LRTI + progressive disease |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRespiratory viral infections research · Pediatric health and respiratory diseases · Pneumonia and Respiratory Infections
Introduction
In healthy children, respiratory viruses usually have a self-limiting, mild clinical course in the form of upper respiratory tract infection (URTI). However, in immunocompromised children receiving myelosuppressive therapy and/or hematopoietic stem cell transplantation (HSCT), they can progress to lower respiratory tract infection (LRTI) and cause widespread and severe disease (1). Therefore, despite advances made in childhood cancer treatment outcomes in the last decade, respiratory tract infections (RTI) and their complications can negatively affect treatment outcomes (2).
During the coronavirus disease 2019 (COVID-19) outbreak, some universal practices were implemented to protect public health around the world in order to prevent COVID-19 transmission. These included public education about universal mask use in public areas, the obligation to pay attention to hand hygiene, and infection control measures such as quarantine, social distancing (closure-partial closure), and occupational health policies for sick healthcare workers (being considered on leave during the illness) (3, 4). Therefore, there was a significant decrease in the incidence of respiratory viruses other than COVID-19 worldwide with the pandemic (5). Since May 5, 2023, the date when the World Health Organization (WHO) officially announced the end of the COVID-19 pandemic, an increase in non-COVID-19 viral respiratory infections has been reported (6). In our country, the most frequently detected respiratory viral agents in pediatric cancer patients in the pre-pandemic period were reported to be rhinovirus/enterovirus, parainfluenza (PIV), respiratory syncytial virus (RSV), and influenza (7, 8). There are limited data evaluating the distribution of viral agents in children during three different time periods; the pandemic, relaxation of pandemic measures and after the COVID-19 outbreak in various disease settings.
The aim of the study is to evaluate the changes in viral RTI agents after COVID-19 compared to the lockdown period and to investigate the associated clinical findings, complications and mortality data for our pediatric hematology and oncology patients.
Material and method
Study design and data collection
In this study, nasopharyngeal swab samples were taken from children with signs and symptoms of acute RTI hospitalized at Bursa Uludag University Sabahattin Gazioğlu Pediatric Hematology and Oncology Hospital between 01.01.2020 and 01.03.2025. The study included patients aged <23 years old, who either had cancer treatment within the last six months, or received HSCT with ongoing immunosuppressive therapy. Children with benign immunosuppressive hematological disorders were also included in the study. Patients considered immunosuppressive with benign hematological diseases were those using long-term high-dose corticosteroids and/or immunosuppressive drugs such as cyclosporine due to immune cytopenia (anemia, thrombocytopenia), patients with congenital hemolytic anemia (thalassemia, hereditary spherocytosis) who had splenectomy and/or receive regular blood transfusions, and patients with common variable immune deficiency, combined immune deficiency and congenital neutropenia.
RTI was defined as episodes with fever ≥38°C at least once in the previous 72 h, and also one of the symptoms of cough, sore throat, nasal congestion, runny nose, or respiratory distress. Age, gender, diagnosis of hemato-oncological disease, date of onset of symptoms and hospitalization, duration of hospital stay, duration of fever, presence of tachypnea/dyspnea, need for intensive care, duration of hospitalization due to infection, concomitant blood-urine-catheter-stool culture positivity, other concomitant infection focus, white blood cell count (WBC), neutrophil, lymphocyte, monocyte and platelet counts, C-reactive protein (CRP), and final status (alive/died) of the patients were evaluated based on their electronic hospital records.
Respiratory tract infectious episodes were divided into two groups; URTI and LRTI. URTI was defined as the presence of at least one of the following symptoms: cough, fever, sore throat, runny nose, or nasal congestion, without abnormal chest examination findings. LRTI was described as the presence of findings indicating lower respiratory tract involvement on chest examination (tachypnea, oxygen requirements, rales, rhonchi, bronchial breathing sounds, etc.), and/or signs of new pulmonary infiltrates observed on chest radiography and/or computed tomography (CT).
We divided the COVID-19 pandemic and afterwards into three time periods;
- Lockdown period: Between January 2020 and May 2021 including the beginning of the pandemic and lockdowns and distance learning at schools in Türkiye.
- Relaxation Period: Between May 2021 and May 2023 when rules were loosened after the lockdowns.
- After the end of COVID-19: Between 5 May 2023 and March 2025.
Supportive care
All patients were placed in protective isolation in single rooms. All immunosuppressed patients received cotrimoxazole administered for consecutive 2 days a week as prophylaxis for Pneumocystis carinii pneumonia from the start of immunosuppressive treatment until three months after the discontinuation of immunosuppression. HSCT recipients received acyclovir prophylaxis against CMV infection until the discontinuation of immunosuppression. Patients with neutrophil counts <100/mm^3^ for more than seven days were given antifungal prophylaxis until the neutrophil count was >500/mm^3^ (9). Intravenous immunoglobulin was administered if the patient immunoglobulin G levels were <500 mg/dL and immunoglobulin G levels were monitored every 3 weeks (10). The febrile neutropenic phase was treated with broad-spectrum antibiotics and this treatment was modified subsequently according to the results of blood or tissue cultures (9, 10).
Sample collection and screening
This study included patients who were hospitalized at Bursa Uludağ University Children's Hematology and Oncology Hospital, which is the largest referral center in the south Marmara region with a population of nearly six million. Nasopharyngeal swab specimens were transported to the department of microbiology laboratory in a transport medium (UTM-RT, Copan, Italy) and were tested using the fully automated multiplex polymerase chain reaction (PCR)-based BioFire FLOQ Swabs (Copan, Italy). The respiratory pathogens were identified using the QIAStat Dx Respiratory SARS-CoV-2 (COVID-19) Panel (Qiagen, Germany) on the QIAStat Dx system (Qiagen, Germany) from 2020 to 2021, followed by the BioFire FilmArray Respiratory Panel (bioMérieux, Marcy-l'Étoile, France) on the FilmArray 2.0 System (bioMérieux) from 2021 to February 2025. These panels are multiplex PCR-based syndromic testing platforms capable of detecting respiratory pathogens simultaneously. Both panels included influenza A, influenza B, and influenza A H1N1 2009, rhinovirus/enterovirus, PIV 1,2,3,4, coronaviruses (CoVs) NL 63, 229E, 0C43, HKU1 and COVID-19, human metapneumovirus (MPV) A/B, RSV A/B, adenovirus, Mycoplasma pneumoniae and Bordetella pertussis. However, only bocavirus and Legionella pneumophila can be detected by the QIAStat Dx respiratory panel, and only Bordetella parapertussis and Chlamydophila pneumoniae can be detected by the BioFire FilmArray panel. Detection of more than one agent at the same time in the PCR panel in the same person was considered co-infection. If the same patient was re-infected with the same virus one month after complete clinical recovery, this event was accepted as a second episode. If the patient continued to have RTI symptoms without any clinical improvement, a repeat PCR panel was obtained in the third week of the infection to assess whether the viral agent persisted or whether a new agent had been added to the picture. If the same agent was still detected after one month, persistent infection was considered in the patient.
Ethics committee
This retrospective study was conducted using anonymized patient data from electronic medical records. Institutional Review Board of Bursa Uludag University Health Research Ethic Committee on 19.03.2025 with decision number 2025/558-6/22. Written informed consent was obtained from the parents of patients who participated in this study.
Statistics
Mean, standard deviation, median, minimum-maximum values, frequency, and percentage were used for descriptive statistics. The distribution of variables was checked with the Kolmogorov–Smirnov test. The independent samples t-test and Mann–Whitney U test were used to compare quantitative data. The chi-square test was used for the comparison of qualitative data. A forward stepwise multivariate binary logistic regression model was constructed at the patients' episodes level (n = 271 episodes), incorporating age, gender, diagnosis, HSCT status, neutropenia, pathogen type, and pandemic period to estimate adjusted associations with outcomes. Moreover, the multivariable binary logistic regression analysis was constructed at the patient level (n = 185 patients), incorporating age, gender, diagnosis, HSCT status, with only the first recorded infectious episode per patient included to avoid within-subject correlation. A backward stepwise elimination procedure was applied to identify independent predictors of the outcome. Gender and diagnosis categories were initially entered into the model, and variables were sequentially removed based on likelihood-ratio criteria to identify independent predictors of the outcome. All tests adopted a value of p ≤ 0.05 for statistical significance. Analyses were conducted using SPSS (version 22.0).
Results
In this study, 271 RTI episodes in 185 children with hemato-oncologic disorders were analyzed. The median age of the patients was 6 years (range: 4 months–23 years), with a female-to-male ratio of 85:100. Episodes were divided into four groups according to patient diagnosis (Table 1).
Group 1 (n = 77 patients): RTI episodes in children with hematologic malignancies n = 125 episodes (46%); acute lymphoblastic leukemia (ALL) 36.9% (n = 100), acute myeloblastic leukemia (AML) 4.4% (n = 12), relapsed ALL 3.3% (n = 9), myelodysplastic syndrome (MDS) (n = 2), relapsed AML (n = 1), juvenile myelomonocytic leukemia (JMML) (n = 1).
Group 2 (n = 67 patients): RTI episodes in children with solid tumors n = 87 (32.1%) (n = 67 patients).
Group 3 (n = 12 patients): RTI episodes in those receiving immunosuppressive therapy following HSCT, n = 16 (5.9%).
Group 4 (n = 29 patients): Other RTI episodes; n = 43 (15.9%) in those with benign hematologic diseases (thalassemia, hereditary spherocytosis, congenital neutropenia, immunodeficiency, immune cytopenia).
Of the 271 episodes, URTI and LRTI were detected in 45% (n = 122/271) and 55% (n = 149/271), respectively. There was no statistically significant difference between the URTI and LRTI groups in terms of WBC, neutrophil, lymphocyte, monocyte, hemoglobin, and platelet counts (p > 0.05). The only difference was found for CRP, which was significantly higher in the LRTI group (p = 0.02) (Table 1). The clinical findings, in terms of tachypnea, dyspnea, duration of fever, duration of hospital stay due to infection, need for intensive care unit, and oxygen requirements, were also significantly different between the two groups (p < 0.05) (Table 1). Fungal co-infection was present in five of the episodes and bacteremia co-infection was present in nine. Of the 271 episodes, 40% (n = 111/271) were rhinovirus/enterovirus infection which was followed by influenza 10.7% (n = 29/271), COVID-19 10% (n = 27/271), and co-infections 14% (n = 38/271). The frequency of co-infections was significantly higher in those with LRTI compared to URTI (p = 0.018) (Table 1). The frequency of co-infections increased gradually and reached its highest value in the post-pandemic period (lockdown 5/38, relaxation 8/38, after the outbreak 25/38) (Table 1).
When co-infection episodes are evaluated, co-infections were rare during the lockdown period. In the relaxation period, LRTI cases had a significant increase (8/149, 5.4%; p = 0.009). After the end of the COVID-19 outbreak, co-infection rates rose in both groups (URTI 7/122, 5.7%; LRTI 18/149, 12.1%), with a trend toward higher rates in LRTI that did not reach statistical significance (p = 0.073) (Table 1).
PIV was more frequent in the URTI group (p < 0.05). No statistically significant difference was found for other agents in terms of causing upper or lower RTI (Table 1).
In the adjusted multivariate logistic regression model that accounted for age, gender, diagnostic category, HSCT status, neutropenia, pathogen type, co-infection status, and pandemic period, HSCT status emerged as the only independent predictor of developing LRTI (n = 185 patients = 271 episodes). HSCT recipients episodes (n = 16/271 episodes) and HSCT recipients (n = 12/185 patients) demonstrated significantly higher odds of developing LRTI compared with leukemia/MDS/JMML patients (episodes: OR = 4.05, 95% CI 1.06–15.44, p = 0.040; patients: OR = 11.29, 95% CI = 1.32–96.70, p = 0.027). Although co-infections showed a trend toward increased risk for developing LRTI in episodes (n = 38/271) (OR = 4.60, 95% CI 0.97–21.92, p = 0.055), this did not reach statistical significance, and no other diagnostic or pathogen categories were independently associated with LRTI after adjustment.
A total of 313 infectious agents were identified in 185 children across 271 infectious episodes. The detected pathogens are given in Table 2. We found that the infectious episodes in total increased significantly after the end of pandemic (p < 0.001) (Table 2). The only significant increase among the all pathogens was observed for influenza A/B (lockdown period; n = 5, 17.9%, after the outbreak; n = 30, 16%) and rhinoviruses (lockdown period; n = 12, 43%, relaxation period; n = 52, 53.6%, after the outbreak; n = 70, 37.2%, p < 0.001). Although no statistically significant difference was detected for COVID-19, most cases were seen in the post-outbreak period (Table 2).
Using two different PCR kits can introduce inconsistencies in pathogen detection. Bocavirus was detected in one patient during the lockdown period and in one patient during the relaxation period. We were aware that the PCR kit did not contain Bocavirus at the time it was changed. However, we did not conduct any additional studies because supportive care is recommended since there is no specific treatment.
Twelve patients (6.5%) out of 185 children with LRTI required intensive care unit (ICU) admission, of whom only one child was admitted to the ICU twice. Therefore, 13 episodes (5%; n = 13/271) were monitored in the ICU. In this cohort, 9 out of 185 children (5%) died of LRTI. They all required intensive care prior to death. Only 3 of these patients died secondary to RTI. None of these patients had progressive disease or other lethal conditions. Two patients died due to rhino/enterovirus pneumonia and one patient died due to COVID-19 pneumonia. Three of the other six patients had progressive disease accompanying the viral infection, one had cytomegalovirus (CMV) infection, one had lung graft-vs.-host disease (GvHD), and one had intracranial hemorrhage (Table 3). Although episodes in HSCT patients comprised 5.9% (n = 16/271) of all episodes, the majority had LRTI (n = 13/16), and approximately 19% (n = 3) required intensive care. Two of these patients died (Tables 1, 3).
Discussion
Uludağ University Hospital, located in Bursa, Türkiye's fourth-most populous city, is the only reference center in the southern Marmara region that offers solid organ and bone marrow transplants and treatment for hemato-oncological disorders. With a population of approximately six million and proximity to Istanbul, the southern Marmara region was significantly impacted by the pandemic (11).
Most of the RTI data for the COVID-19 pandemic comes from the period of the outbreak. There is scarce data available afterwards (12–17). Epidemiological data about RTI in children with cancer from Türkiye were examined during the pandemic (13). This study is particularly important because it examines the distribution and pathogenic properties of RTI in detail and compares data during and after the pandemic covering the entire southern Marmara region.
We found that the frequency of all viral agents, including COVID-19, was low during the pandemic between March 2020 and May 1, 2021, when the pandemic rules were strictly implemented in Türkiye (Figure 1; Table 2). During this period, only two of our patients were hospitalized due to COVID-19. We believe that the reason fewer COVID-19 and other RTI agents were detected is the effective implementation of non-pharmacological measures. Current treatment options for RTI largely involve supportive care. Protection from respiratory viruses is crucial. Therefore, it is vital for patients and their caregivers/close contacts to adhere to preventive measures, such as wearing masks, maintaining social distancing, and practicing hand hygiene. Annual influenza vaccination is also recommended for all immunocompromised patients aged six months and older, as well as those in close contact with patients. Early diagnosis, careful monitoring, and appropriate treatment for RTI are crucial to prevent potential serious complications (10, 13). The influenza vaccination status of our patients and their close contacts was unknown.
Seasonal distribution of RTI.
In addition, patients without severe and persistent fever and/or LRTI findings and/or severe neutropenia were closely monitored by telemedicine without hospitalization. If possible, chemotherapy was usually administered in the outpatient unit with outpatient follow-up. All patients requiring hospitalization were subjected to a COVID-19 test along with their companions before hospitalization, and they were admitted if the test result was negative. Other studies also reported similar results in that both COVID-19 and other RTI decreased significantly in the first months of the COVID-19 outbreak due to strictly applied pandemic measures (15, 18–20). The decrease in all RTI agents during the pandemic led to a decrease in immunity in the entire society, creating an “immunity gap”. For this reason, the frequency of some viral agents has significantly increased and more severe clinical courses occurred with the relaxation of non-pharmacological measures (16–18, 21). Our findings showed a gradual increase in all infection agents (Table 2). Rhinovirus/enterovirus was the most frequent agent detected in all time periods. Specifically, significant increases in the frequency of rhinovirus/enterovirus and influenza A/B were observed following the relaxation of pandemic regulations (Table 2). In a study examining 319 nasopharyngeal swab samples from 0 to 92 year olds in our hospital during the period, rhino/enterovirus was the most commonly identified causative agent during the pandemic (11).
While viruses cause URTI in the general population, they also cause LRTI in hemato-oncology patients (22). In our cohort, the frequency of URTI and LRTI was similar in all periods (p = 0.984) (Table 1). However, co-infections were significantly more common in the LRTI group, and parainfluenza frequently caused URTI (Table 1). After the end of the COVID-19 outbreak, co-infection rates increased in both upper and lower groups, with a trend toward higher rates in LRTI that did not reach statistical significance (Table 1). The literature reports that the frequency of co-infections increased after the pandemic, and that there was no relationship between co-infections and LRTI (13, 23). CRP and clinical findings supporting the diagnosis of LRTI, such as tachypnea, dyspnea, duration of fever, and duration of hospital stay due to infection, were also found to be significantly higher (p < 0.05) (Table 1). The need for intensive care and oxygen requirements were not present in URTI cases (Table 1).
Since HSCT recipients among hemato-oncology patients were more immunosuppressive, in our study, in line with the literature, HSCT recipients were found to be more susceptible to LRTI compared to other patient groups (n = 12/185 patients, p = 0.027) (13, 24).
Thirteen episodes (5%; n = 13/271) were monitored in the ICU. In our study, 3% of all episodes (n = 9/271) resulted in death, which corresponds to 5% (n = 9/185) of all children (Table 3). It is difficult to attribute these deaths to RTI because of other comorbidities. Six of the 9 children who died had underlying conditions and they all had LRTI. Kaçar et al. (13) reported that 28.7% of all episodes were LRTI in Türkiye. However, the frequency of LRTI in our cohort was high (55%) and it is also noteworthy that all those who died had LRTI. The LRTI rate may have been higher because our study only evaluated inpatients. The death rate in the study by Kaçar et al. (13) was slightly higher than in our study, but it included only the COVID-19 pandemic period. In this cohort, two patients out of 41 (4.8%; n = 2/41) died from COVID-19 infection (Table 3). A study in Türkiye by Rejin Kebudi et al. (24) reported a death rate of 2% (n = 1/51) related to COVID-19 in 51 children with cancer and stem cell transplant recipients. COVID-19 infection generally progressed with mild clinical symptoms during the pandemic. It was not reported as the most lethal RTI agent during or after the pandemic (4, 18, 25–30). In a study conducted in China about 285 pediatric patients with hematological malignancies, 89.1% of the patients had mild infection course while 1.8% had severe course, and 0.7% had critical course and died (30). In meta-analysis and cohort studies conducted in children with hemato-oncological diseases, mortality rates associated with COVID-19 ranging from 3.8% to 4% were reported (31, 32).
The limitations of our study are that it included a single center, that two separate RTI panels were used during the study, patients were a heterogeneous group in terms of underlying disease, the lack of vaccination information for patients and being conducted as a retrospective data analysis.
Conclusions
A total of 313 RTI agents were identified in 185 children with hemato-oncologic disorders across 271 infectious episodes. In our study, the largest RTI outbreak occurred between November 2023 and May 2024, following the end of the COVID-19 pandemic (Figure 1; Table 2). RTI outbreaks were especially observed as a result of the reduction in non-pharmacological preventive measures. With the reopening of schools during the relaxation period, the announcement that the pandemic was over, and the lifting of the mask mandate, RTI incidence increased. This suggests that the most effective RTI control method for immunosuppressed patients remains adherence to non-pharmacological measures, such as social distancing, mask-wearing, and hand hygiene, among both patients and those in close contact with them. In our study, the most common pathogens causing RTI were rhinovirus/enterovirus and influenza A/B, and their frequencies increased significantly in the post-pandemic period. Another preventive measure against RTI is annual influenza vaccination for patients and their caregivers. In our study, the frequency of deaths related solely to RTI was low (n = 3). The majority of deaths occurred in patients with other comorbidities and progressive underlying disease. Clinicians should be aware that the number of viral RTI episodes increased following the pandemic related to immune debt that occurred during the lockdown period, and that agents that are not expected to be fatal may cause severe clinical conditions. It is essential to keep in mind that the most crucial step in treatment is implementing effective infection preventive measures.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hijano DR Maron G Hayden RT. Respiratory viral infections in patients with cancer or undergoing hematopoietic cell transplant. Front Microbiol. (2018) 9:3097. 10.3389/fmicb.2018.0309730619176 PMC 6299032 · doi ↗ · pubmed ↗
- 2Soudani N Caniza MA Assaf-Casals A Shaker R Lteif M Su Y Prevalence and characteristics of acute respiratory virus infections in pediatric cancer patients. J Med Virol. (2019) 91(7):1191–201. 10.1002/jmv.2543230763464 PMC 7166696 · doi ↗ · pubmed ↗
- 3Lefebvre M-A Rajda E Frenette C Paquet F Rubin E Sleno H Impact of the COVID-19 pandemic on healthcare-associated viral respiratory infections at a tertiary care pediatric hospital. Am J Infect Control. (2023) 51(8):961–3. 10.1016/j.ajic.2023.01.01736736901 PMC 9889274 · doi ↗ · pubmed ↗
- 4Ryoo J Kim SC Lee J. Changes in respiratory infection trends during the COVID-19 pandemic in patients with haematologic malignancy. BMC Pulm Med. (2024) 24(1):259. 10.1186/s 12890-024-03071-038797852 PMC 11129456 · doi ↗ · pubmed ↗
- 5Groves HE Piché-Renaud P-P Peci A Farrar DS Buckrell S Bancej C The impact of the COVID-19 pandemic on influenza, respiratory syncytial virus, and other seasonal respiratory virus circulation in Canada: a population-based study. Lancet Reg Health Am. (2021) 1:1–9. 10.1016/j.lana.2021.100015 PMC 828566834386788 · doi ↗ · pubmed ↗
- 6Sarker R Roknuzzaman A Nazmunnahar Shahriar M Hossain MJ Islam MR. The WHO has declared the end of pandemic phase of COVID-19: way to come back in the normal life. Health Sci Rep. (2023) 6(9):e 1544. 10.1002/hsr 2.154437674622 PMC 10478644 · doi ↗ · pubmed ↗
- 7Büyükkapu-Bay S Kebudi R GörgünÖ Meşe S Zülfikar B Badur S. Respiratory viral infections frequency and clinical outcome in symptomatic children with cancer: a single center experience from a middle-income country. Turk J Pediatr. (2018) 60(6):653–9. 10.24953/turkjped.2018.06.00531365201 · doi ↗ · pubmed ↗
- 8Köker SA DemirağB Tahta N Bayram N Oymak Y Karapinar TH A 3-year retrospective study of the epidemiology of acute respiratory viral infections in pediatric patients with cancer undergoing chemotherapy. J Pediatr Hematol Oncol. (2019) 41(4):e 242–6. 10.1097/MPH.000000000000141830688827 · doi ↗ · pubmed ↗