Predicting patient dropout: a nomogram for loss to follow-up after Helicobacter pylori eradication therapy
Xiao Zhao, Xiao She, Haiyan Yang, Jing Zhao, Shi Cheng, Haitao Guan, Ping Zhao

TL;DR
This study creates a tool to predict which patients are likely to miss follow-up after Helicobacter pylori treatment, helping improve treatment success.
Contribution
A novel nomogram was developed to predict patient dropout after Helicobacter pylori eradication therapy using clinical and demographic factors.
Findings
Six independent risk factors for loss to follow-up were identified, including BMI > 30 and distance to hospital > 10 km.
The nomogram achieved an AUC of 0.885 in training and 0.862 in testing, showing strong predictive accuracy.
Decision curve analysis confirmed the model's clinical utility for predicting patient follow-up risk.
Abstract
Helicobacter pylori (H. pylori) infection remains a global public health burden, particularly in developing countries. While its eradication is a cornerstone for gastric cancer prevention, management is challenged by high infection rates, rising antibiotic resistance, and suboptimal treatment efficacy. Compounding these issues, patient loss to follow-up (LTFU) has emerged as a critical factor directly undermining the success of eradication therapy. This study aimed to investigate the risk factors associated with LTFU after H. pylori eradication, and to develop a predictive model for assessing the risk of LTFU. We conducted a prospective cohort study (April 2023-September 2024) enrolling treatment-naïve patients from a tertiary gastroenterology clinic. Following data collection via questionnaires and follow-ups, a nomogram for predicting loss to follow-up (LTFU) was developed by…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
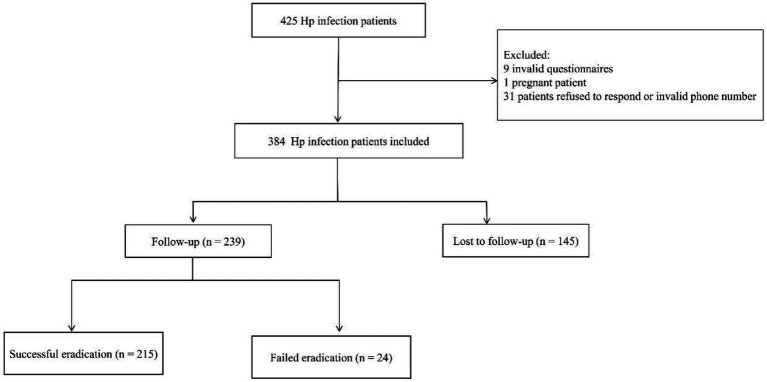 Figure 1
Figure 1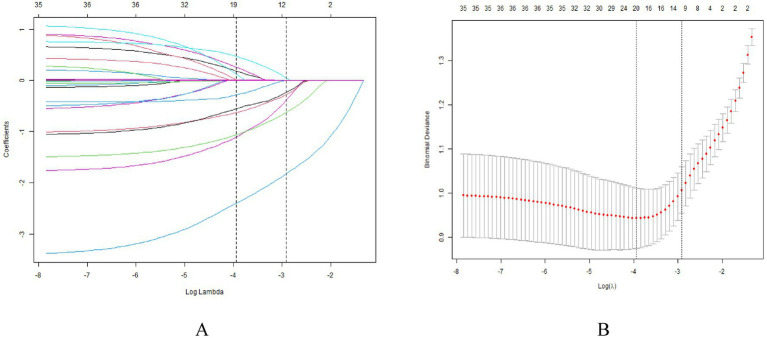 Figure 2
Figure 2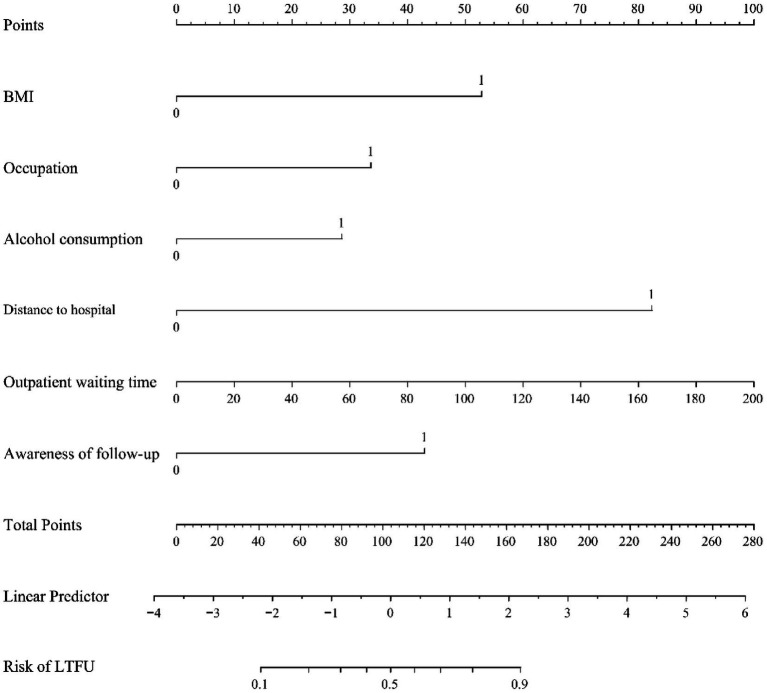 Figure 3
Figure 3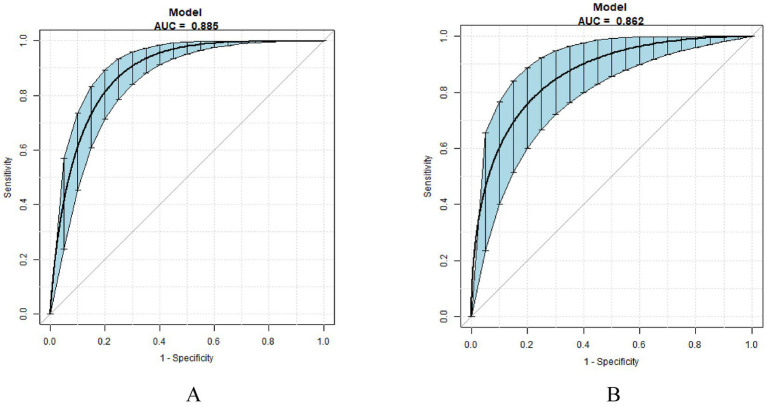 Figure 4
Figure 4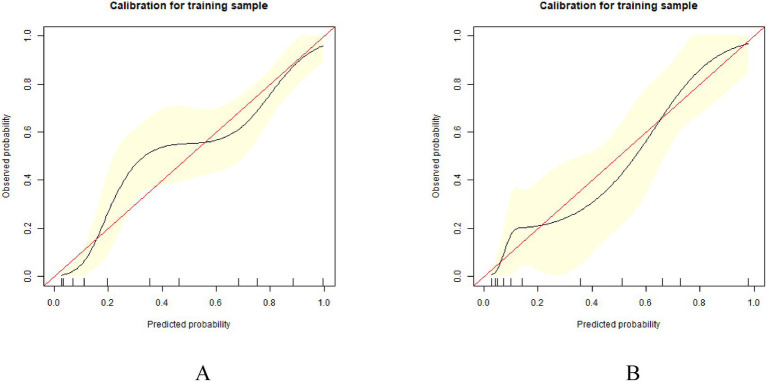 Figure 5
Figure 5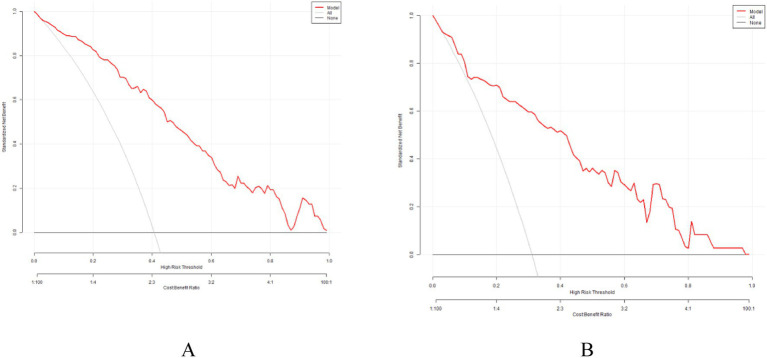 Figure 6
Figure 6| Variables | Training group ( | Test group ( |
|
|---|---|---|---|
| Age, y | 39.64 ± 11.64 | 38.78 ± 11.25 | 0.505 |
| Sex | 0.690 | ||
| Male | 133 (49.63%) | 55 (47.41%) | |
| Female | 135 (50.37%) | 61 (52.59%) | |
| BMI, Kg/m2 | 0.983 | ||
| ≤30 | 254 (94.78%) | 110 (94.83%) | |
| >30 | 14 (5.22%) | 6 (5.17%) | |
| Type of work | 0.132 | ||
| Mental labor | 198 (73.88%) | 94 (81.03%) | |
| Physical labor | 70 (26.12%) | 22 (18.97%) | |
| Residence | 0.077 | ||
| Urban | 239 (89.18%) | 110 (94.83%) | |
| Rural | 29 (10.82%) | 6 (5.17%) | |
| Payment method | 0.142 | ||
| Medical insurance | 147 (54.85%) | 73 (62.93%) | |
| Out-of-pocket | 121 (45.15%) | 43 (37.07%) | |
| Occupation | 0.688 | ||
| Non-government employee | 191 (71.27%) | 85 (73.28%) | |
| Government employee | 77 (28.73%) | 31 (26.72%) | |
| Education | 0.697 | ||
| High school/technical secondary school or below | 65 (24.25%) | 26 (22.41%) | |
| College or higher education | 203 (75.75%) | 90 (77.59%) | |
| Marital status | 0.782 | ||
| Married | 188 (70.15%) | 83 (71.55%) | |
| Unmarried/Divorced or separated/Widowed | 80 (29.85%) | 33 (28.45%) | |
| Monthly household income per capita (CNY) | 0.545 | ||
| <2000 | 29 (10.82%) | 9 (7.76%) | |
| 2000–5,000 | 85 (31.72%) | 38 (32.76%) | |
| 5,000–1,000 | 107 (39.93%) | 53 (45.69%) | |
| >10,000 | 47 (17.54%) | 16 (13.79%) | |
| Smoking status | 0.178 | ||
| No | 221 (82.46%) | 102 (87.93%) | |
| Yes | 47 (17.54%) | 14 (12.07%) | |
| Alcohol consumption | 0.870 | ||
| No | 171 (63.81%) | 73 (62.93%) | |
| Yes | 97 (36.19%) | 43 (37.07%) | |
| Distance to hospital (km) | 0.440 | ||
| ≤10 | 148 (55.22%) | 69 (59.48%) | |
| >10 | 120 (44.78%) | 47 (40.52%) | |
| Outpatient waiting time (min) | 25.36 ± 28.29 | 27.13 ± 24.01 | 0.092 |
| Time to hospital (minutes) | 60.92 ± 67.39 | 55.35 ± 63.47 | 0.887 |
| Prior | 0.738 | ||
| No | 178 (66.42%) | 75 (64.66%) | |
| Yes | 90 (33.58%) | 41 (35.34%) | |
| Family history of | 0.305 | ||
| No | 197 (73.51%) | 91 (78.4:5:%) | |
| Yes | 71 (26.49%) | 25 (21.55%) | |
| Family history of gastric disease | 0.576 | ||
| No | 208 (77.61%) | 93 (80.17%) | |
| Yes | 60 (22.39%) | 23 (19.83%) | |
| Awareness of follow-up | 0.784 | ||
| Important | 184 (68.66%) | 78 (67.24%) | |
| Unimportant | 84 (31.34%) | 38 (32.76%) | |
| LTFU | 0.:074 | ||
| No | 159 (59.33%) | 80 (68.97%) | |
| Yes | 109 (40.67%) | 36 (31.03%) |
| Variables | OR (95% CI) |
|
|---|---|---|
| BMI, Kg/m2 | ||
| ≤30 | 1.0 | |
| >30 | 3.81 (1.16, 12.50) | 0.0276 |
| Residence | ||
| Urban | 1.0 | |
| Rural | 0.55 (0.23, 1.30) | 0.1747 |
| Occupation | ||
| Non-government employee | 1.0 | |
| Government employee | 2.10 (1.21, 3.63) | 0.0083 |
| Alcohol consumption | ||
| No | 1.0 | |
| Yes | 2.27 (1.36, 3.79) | 0.0017 |
| Distance to hospital (km) | ||
| ≤10 | 1.0 | |
| >10 | 11.27 (6.29, 20.18) | <0.0001 |
| Outpatient waiting time (min) | 1.01 (1.00, 1.02) | 0.0035 |
| Awareness of follow-up | ||
| Important | 1.0 | |
| Unimportant | 3.32 (1.93, 5.69) | <0.0001 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHelicobacter pylori-related gastroenterology studies · Gastric Cancer Management and Outcomes · Statistical Methods in Clinical Trials
Introduction
1
Helicobacter pylori (H. pylori) infection is closely associated with the pathogenesis of various gastrointestinal conditions, including chronic gastritis, peptic ulcers, gastric cancer, and a range of extra-gastric diseases (1, 2). Due to its established carcinogenic potential, the World Health Organization (WHO) has classified H. pylori as a Group I carcinogen (3). Globally, the prevalence of H. pylori infection has declined, decreasing from 58.20% during 1980–1990 to 43.10% in the period 2011–2022 (4). Despite this overall decrease, significant regional disparities persist. Infection rates remain substantially higher in developing countries compared to developed nations. In China, the epidemiological pattern of H. pylori infection exhibits a distinct north–south gradient, with generally higher prevalence observed in northern regions. Recent studies report infection rates ranging from 30.53 to 60.8% across different parts of the country (5–8). This substantial and uneven disease burden underscores the urgent need for scientifically informed public health strategies to mitigate the impact of H. pylori infection.
Helicobacter pylori infection initiates a pathological cascade in the gastric mucosa, progressing from chronic active gastritis to atrophic gastritis, intestinal metaplasia, and dysplasia, which may ultimately lead to gastric carcinogenesis (9). Eradication therapy is crucial in mitigating this progression by reducing gastric mucosal inflammation, accelerating ulcer healing, and reducing the recurrence of peptic ulcers and associated complications such as bleeding or perforation. Furthermore, such treatment can inhibit, or even partially reverse, the development of mucosal atrophy and intestinal metaplasia, thereby contributing to a reduction in the incidence of gastric cancer and related mortality. Despite these established benefits, H. pylori eradication efforts in China encounter significant challenges. The persistent challenges of high infection rates, heightened pathogenicity of prevalent strains, and suboptimal treatment efficacy collectively continue to pose a formidable public health threat. A major contributing factor is the increasing prevalence of antibiotic resistance, particularly to clarithromycin, levofloxacin, and metronidazole, which severely compromises the efficacy of standard therapeutic regimens.
There is some evidence reported that (10, 11) indicates a concerning rate of LTFU after initial H. pylori eradication, ranging from 14.30 to 32.10%. This high attrition rate poses a significant obstacle to effective long-term infection control. Failure to ensure follow-up delays necessary medical intervention for infected individuals, facilitates ongoing community transmission, and elevates the risk of antibiotic resistance development. Subsequent retreatment in patients initially lost to follow-up is often less effective, likely due to selection for resistant strains during periods of unmonitored infection or after incomplete treatment cycles. Current understanding of post-treatment attrition is primarily derived from studies on chronic infectious diseases such as tuberculosis and HIV. Established risk factors in these contexts encompass a range of demographic, behavioral, and socioeconomic variables, including male sex, extreme age groups, tobacco use, alcohol consumption, lower socioeconomic status, malnutrition, adverse drug effects, and geographical barriers to healthcare access (12–17).
However, there is currently a lack of published data on the incidence and predictors of LTFU after H. pylori eradication therapy. Thus, we conducted a study to investigate the rate and risk factors associated with post-treatment attrition among individuals with H. pylori infection in Xi’an, China. Furthermore, we developed a nomogram to predict the probability of LTFU, aiming to facilitate early identification of high-risk patients and guide targeted interventions to improve follow-up rates.
Methods
2
Study design and populations
2.1
A prospective single-center cohort study was conducted at the Gastroenterology outpatient clinic of the Second Affiliated Hospital of Xi’an Jiaotong University. Between April 2023 and September 2024, 425 patients with H. pylori infection, who were initiating their first course of eradication therapy, were consecutively enrolled.
Inclusion criteria
2.1.1
(1) Undergoing their first course of H. pylori eradication therapy; (2) Prescribed an empirical bismuth-containing quadruple regimen (amoxicillin + clarithromycin + ilaprazole + colloidal bismuth pectin); (3) Capable of understanding the questionnaire content and providing accurate responses; (4) Provided written informed consent for the eradication therapy and agreed to participate in both outpatient and telephone follow-up surveys.
Exclusion criteria
2.1.2
(1) Missing or erroneous baseline information, unreachable by phone, or refusal to participate in the follow-up survey after contact; (2) Withdrawal during the study due to severe organ dysfunction, allergic drug reactions, disease progression, or other serious adverse events necessitating discontinuation of the protocol therapy; (3) Presence of cognitive impairment, severe hepatic or renal disease, or other significant chronic comorbidities; (4) Planning for pregnancy, current pregnancy, or lactation; and (5) History of gastrectomy.
Definitions
2.2
In this study, LTFU was defined as failure to complete the recommended confirmatory test within 8 weeks after completing the initial eradication therapy, or adherence to less than 80% of the prescribed medication. This definition is adapted from established criteria in the field to ensure accurate assessment of initial treatment failure versus later reinfection (11, 18–21).
Occupation was classified into a binary variable: government employee VS. Non-government employee (which encompassed all other occupations, including self-employed, corporate workers, farmers, etc.). This was done to test the potential influence of socioeconomic and occupational factors on follow-up adherence.
Payment method was categorized as “Out-of-pocket” or “Medical insurance” to evaluate the potential influence of financial burden on follow-up adherence.
Time to hospital was defined as the patient’s self-reported one-way travel time from their residence to the hospital under normal traffic conditions, measured in minutes. This measure reflects the actual door-to-door duration, which may include in-transit time and potential waiting periods, rather than mere geographical distance.
Ethical considerations
2.3
This prospective cohort study was conducted in accordance with the principles of the Declaration of Helsinki and received approval from the Medical Ethics Committee of the Second Affiliated Hospital of Xi’an Jiaotong University (Approval No. 2023231). The study protocol was prospectively registered with the Chinese Clinical Trial Registry (Registration number: ChiCTR2500096567). We received informed consent from all participants.
Data collection procedure
2.4
All participants completed a structured questionnaire under the guidance of uniformly trained research staff. The questionnaire was developed based on the survey instrument used in the National Epidemiological Investigation of H. pylori Infection in China. Data were collected through one-on-one interviews, and questionnaires were reviewed on-site upon completion to ensure completeness. In cases of missing or unclear information, follow-up contacts were made to supplement the data; otherwise, incomplete questionnaires were excluded from the analysis.
Data management and statistical analysis
2.5
The data were entered and verified using EpiData 3.2 software. All statistical analyses were performed via the R statistical package and EmpowerStats 4.2 software. Continuous variables were expressed as mean ± SDs and compared using the Student’s t-test or Mann–Whitney U test, as appropriate. Categorical variables were presented as frequencies and percentages and compared using the chi-square test or Fisher’s exact test.
The Least Absolute Shrinkage and Selection Operator (LASSO) regression method was applied to screen potential predictors. Variables with non-zero coefficients in the LASSO regression were subsequently entered into a multivariate logistic regression model to construct the final prediction model (22). The model’s discriminative ability was evaluated using the area under the receiver operating characteristic curve (AUC), with internal validation performed via the bootstrap method (500 resamples). Calibration curves and a decision curve analysis (DCA) were used to measure the predictive performance of the nomogram. Clinical utility was assessed using decision curve analysis (DCA). p < 0.05 was considered statistically significant.
Results
3
Demographic and clinical characteristics
3.1
The flow chart of patients throughout this analysis is reported in Figure 1. The demographic and clinical characteristics of the participants are presented in Table 1. Among the 425 patients initially enrolled, 41 were excluded for the following reasons: 9 patients provided invalid questionnaires, 1 patient was excluded due to pregnancy, and 31 patients could not be contacted (refused to respond or provided invalid phone numbers). The final analytical cohort therefore consisted of 384 participants, who were randomly allocated into a training group (n = 268) and a test group (n = 116). In the training and test groups, 40.67% (109/268) and 31.03% (36/116) of participants were LTFU, respectively. Common reasons for attrition included being too busy at work, failure to initiate medication, and resolution or absence of symptoms. After comparing the baseline data of both groups, it was found that there were no significant differences in sex, age, BMI, type of work, residence, payment method, occupation, education, marital status, monthly household income per capita, smoking status, alcohol consumption, distance to the hospital, outpatient waiting time, time to hospital, and various medical histories (prior H. pylori infection, family history of H. pylori, family history of gastric disease), indicating a generally comparable outcome distribution between the two sets for model building.
A flow chart shows the inclusion and exclusion criteria.
Predictor selection and model construction
3.2
To minimize the risk of overfitting, a LASSO regression analysis was employed. This approach identified seven robust predictors of LUFU from the 19 baseline variables (Table 1; Figure 2): BMI, occupation, distance to the hospital, outpatient waiting time, alcohol consumption, type of residence, and awareness of the need for follow-up.
The LASSO regression analysis identified variables predicting LTFU. (A) Number of non-zero coefficients in the model. (B) Number of variables corresponding to different λ values. Seven variables were selected by LASSO regression and constituted the basic factors of the prediction model.
After multivariate analysis, the independently statistically significant predictors of LTFU were BMI, occupation, distance to hospital, outpatient waiting time, alcohol consumption, and awareness of follow-up (Table 2). The final model is expressed as: logit (LTFU) = −7.29047 + 1.84325BMI + 1.17386occupation +0.99756alcohol consumption +2.87117distance to hospital +0.01744outpatient waiting time +1.49824awareness of follow-up (Figure 3).
Nomogram for predicting LTFU in patients with H. pylori eradication. Instructions: Factors include BMI, occupation, distance to hospital, outpatient waiting time, alcohol consumption, and awareness of follow-up—points assigned by that variable value. Then, the points from each variable value were summed. The sum on the total points scale was located and vertically projected onto the bottom axis, and then a personalized risk for LTFU was obtained.
The performance of the LTFU nomogram
3.3
The prediction model is verified internally. Internal verification is done through bootstrapping, times = 500. In the training set, the model demonstrated an AUC of 0.885 (95% CI: 0.843–0.918), with a sensitivity of 93.58% and a specificity of 67.92%. Comparatively, in the test set, the model achieved an AUC of 0.862 (95% CI: 0.794–0.925), with a sensitivity of 83.33% and a specificity of 77.50% (Figure 4). The calibration curves showed that the predicted probabilities were closely aligned with the observed outcomes across a range of predicted probabilities, confirming the model’s accuracy in estimating LTFU risk (Figure 5). Effectively forecasting the risk of patient LTFU in H. pylori eradication.
The ROC curve after internal validation using bootstrap resampling (times = 500). (A) ROC curves of the nomogram in the training group. (B) ROC curve of the nomogram in the test group.
Calibration curves of the nomogram. (A) Calibration curve of the predictive model in the training group. (B) Calibration curve of the predictive model in the test group.
To evaluate clinical utility, DCA was performed on both the training and validation cohorts. As shown in Figure 6, the DCA results demonstrated that the proposed model yielded favorable clinical utility in both the training and validation cohorts, providing meaningful support for individualized risk assessment and clinical decision-making across reasonable threshold ranges.
Decision curve of the nomogram. (A) Decision curves of the nomogram in the training group. (B) Decision curves of the nomogram in the test group.
Discussion
4
This study firstly addresses the critical clinical challenge of follow-up adherence after H. pylori eradication by developing the nomogram to predict the risk of LTFU. Based on six readily available variables, the model demonstrated robust discriminative ability (AUC: 0.885 training, 0.862 validation), good calibration, and meaningful clinical utility via decision curve analysis. This tool provides a quantitative method for the early identification of high-risk individuals in resource-constrained settings. By enabling risk-stratified management, it facilitates targeted interventions—such as prioritized reminders or enhanced patient education—thereby optimizing the allocation of clinical resources, supporting sustained patient engagement, and ultimately aiming to improve follow-up rates and patient outcomes.
Interpretation of key predictors and clinical context
4.1
Consistent with prior evidence (23, 24), our study found a travel distance of >10 km to the healthcare facility as an independent risk factor for LTFU. Patients residing farther away face greater time commitments and financial costs for follow-up visits, which may further reduce adherence to post-eradication assessments. Furthermore, Denis Opio et al. (25) found that long outpatient waiting time was a risk factor for LTFU, which is consistent with our study.
Alcohol consumption is a known risk factor for H. pylori management (26, 27). In our study, alcohol use significantly increased the likelihood of LTFU, with drinkers exhibiting a 1.82-fold higher risk than non-drinkers. This is consistent with previous research (28, 29). One possible explanation is that alcohol use often co-occurs with poor mental health, including anxiety (30) and depression (31), which may diminish a patient’s motivation to attend follow-up appointments.
Obesity is reported to increase the incidence of LTFU, Torrens C. et al. (32) found severe obesity (BMI > 35 kg/m^2^) was associated with a 2.44-fold increase in LTFU risk. Vejrup K. et al. (33) also found that individuals with higher BMI were more likely to be LTFU. These findings are in line with our results. Obesity is closely linked to metabolic syndrome (34), and patients with obesity often carry a higher burden of comorbidities, which may further affect their ability or willingness to adhere to follow-up schedules. However, contrasting results have been reported by Soedarsono et al. (35) and Frijtersa et al. (36), who found that underweight BMI was associated with LTFU. Thus, the relationship between BMI and LTFU warrants further investigation.
Interestingly, we observed unexpectedly that civil servants were more likely to be lost to follow-up compared with other occupational groups. Similarly, consistent with Mulat A et al. (37), who also reported higher LTFU among government employees. This may reflect competing demands and institutional constraints rather than lack of access: despite having health coverage and formal leave, rigid work schedules and high occupational demands may impede attendance for non-acute appointments. Additionally, reliance on annual employer-organized health checks might lead to underestimation of the need for timely, condition-specific follow-up. In contrast, Soedarsono et al. (35) and Frijters et al. (36) found that unemployment or informal employment was associated with LTFU. Therefore, the influence of occupation on LTFU remains complex and merits further research.
Clinical utility, implementation, and strategies for high-risk patients
4.2
The primary value of this nomogram lies in enabling risk-stratified patient management. By providing a quantitative, individualized risk score at the point of prescription, it shifts the clinical approach from a uniform, reactive follow-up protocol to a proactive, resource-efficient strategy. For patients stratified as high-risk, targeted interventions can be immediately deployed: (1) Enhanced Pre-treatment Counseling: Structured education emphasizing the critical importance and specific timing of the confirmatory test; (2) Proactive Engagement: Implementing scheduled check-in calls or messages during the treatment course to address side effects and reinforce adherence. (3) Reducing Logistical Barriers: Exploring flexible scheduling, telehealth options for post-therapy consultation, or facilitating testing at more convenient locations. (4) Digital Reinforcement: Automated SMS or application-based reminders tailored to high-risk individuals.
This approach optimizes the allocation of limited clinical resources (e.g., nursing time, digital health infrastructure) to the patients who need them most, aiming to improve follow-up completion rates and, consequently, long-term clinical outcomes.
Methodological considerations: definition of LTFU
4.3
In defining LTFU as a missed confirmatory test within 8 weeks post-therapy, we aimed to balance clinical guidelines with diagnostic accuracy. This operational definition, adapted from established criteria (11), is designed to maximize the likelihood that a positive test result within this window reflects true eradication failure rather than early reinfection, a distinction that becomes less clear beyond this period (21). While this timeframe is clinically reasoned for our setting, its optimality may vary in different healthcare contexts and remains a parameter for consideration in future research or implementation.
Strengths and limitations
4.4
Key strengths of this study include its prospective design, the incorporation of diverse and clinically relevant predictors, rigorous internal validation using bootstrapping, and evaluation of clinical utility via decision curve analysis. The nomogram offers an intuitive, visual tool that could be integrated into routine practice. The study has several limitations. Its prospective cohort design is inherently resource-intensive. Moreover, the reliance on questionnaire-based data collection led to the exclusion of participants with incomplete responses, potentially introducing selection bias. Most importantly, the predictive nomogram was developed and internally validated within a single-center context. Consequently, its generalizability to other healthcare settings remains unestablished and warrants external validation through future multi-center studies.
Conclusion
5
In conclusion, BMI, occupation, distance to hospital, outpatient waiting time, alcohol consumption, and awareness of follow-up were identified as predictive factors of LTFU. Based on these factors, we constructed a robust and clinically applicable nomogram that accurately estimates the individual risk of LTFU, thus offering potential for targeted intervention in clinical practice.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Malfertheiner P Megraud F Rokkas T Gisbert JP Liou JM Schulz C . Management of Helicobacter pylori infection: the Maastricht VI/Florence consensus report. Gut. (2022) 71:327745. doi: 10.1136/gutjnl-2022-327745, 35944925 · doi ↗ · pubmed ↗
- 2Wang L Cao ZM Zhang LL Dai XC Liu ZJ Zeng YX . Helicobacter pylori and autoimmune diseases: involving multiple systems. Front Immunol. (2022) 13:833424. doi: 10.3389/fimmu.2022.833424, 35222423 PMC 8866759 · doi ↗ · pubmed ↗
- 3Bouvard V Baan R Straif K Grosse Y Secretan B El Ghissassi F . A review of human carcinogens--part B: biological agents. Lancet Oncol. (2009) 10:321–2. doi: 10.1016/s 1470-2045(09)70096-8, 19350698 · doi ↗ · pubmed ↗
- 4Li Y Choi H Leung K Jiang F Graham DY Leung WK. Global prevalence of Helicobacter pylori infection between 1980 and 2022: a systematic review and meta-analysis. Lancet Gastroenterol Hepatol. (2023) 8:553–64. doi: 10.1016/S 2468-1253(23)00070-5, 37086739 · doi ↗ · pubmed ↗
- 5Gong Y Luo Y Chen Z Sui Y Zheng Y. Longitudinal analysis of factors related to Helicobacter pylori infection in Chinese adults. Open Med. (2022) 17:1742–9. doi: 10.1515/med-2022-0564, 36407872 PMC 9635269 · doi ↗ · pubmed ↗
- 6Yao P Millwood I Kartsonaki C Mentzer AJ Allen N Jeske R . Sero-prevalence of 19 infectious pathogens and associated factors among middle-aged and elderly Chinese adults: a cross-sectional study. BMJ Open. (2022) 12:e 058353. doi: 10.1136/bmjopen-2021-058353, 35534062 PMC 9086621 · doi ↗ · pubmed ↗
- 7Xie L Liu GW Liu YN Li PY Hu XN He XY . Prevalence of Helicobacter pylori infection in China from 2014-2023: a systematic review and meta-analysis. World J Gastroenterol. (2024) 30:4636–56. doi: 10.3748/wjg.v 30.i 43.4636, 39575409 PMC 11572641 · doi ↗ · pubmed ↗
- 8Ye YF Chen YH Hong D Jiesisibieke ZL Tung TH Zhang MX. Association of Helicobacter pylori infection with osteoporosis risk in a physical examination population. Arch Osteoporos. (2022) 17:35. doi: 10.1007/s 11657-022-01074-035156153 · doi ↗ · pubmed ↗