Extracellular Vesicles for Treatment of Bone Resorption-Related Diseases in Animal Models: Systematic Review
Francisco Mônico Moreira, Virgínia Amorin Fróes de Moraes, Carolina dos Santos Santinoni, Graziela Garrido Mori

TL;DR
This review shows that extracellular vesicles (EVs) can help reduce bone loss in animal models by improving bone density and reducing harmful inflammation.
Contribution
The study systematically evaluates the in vivo efficacy of EVs for bone resorption-related diseases using PRISMA guidelines.
Findings
EV therapy reduced bone resorption by increasing osteoprotegerin and decreasing RANKL, TRAP, and osteoclasts.
EVs enhanced bone formation markers like ALP, Runx2, and osteocalcin, leading to increased bone density.
The review highlights the potential of EVs as a treatment but notes the need for more research on safety and dosing.
Abstract
This systematic review aimed to analyze the usefulness of EV therapy in controlling bone resorption-related diseases in animal models. The study was conducted following the PRISMA guidelines. The search was conducted until November 2025 using PubMed/MEDLINE, Scopus, Cochrane Library, and OpenGrey databases to respond to the PICO question: Would therapy with EVs be efficient for the treatment of bone resorption-related diseases in vivo? The primary and secondary outcomes were the control of bone resorption and the molecular mechanisms involved, respectively. The risk of bias was examined according to the criteria of SYRCLE's RoB tool. A total of 1031 studies were reviewed, and after applying the eligibility criteria and excluding duplicates, 38 articles were included in the results. The usefulness of EVs in controlling bone resorption was established in the majority of studies. Increased…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
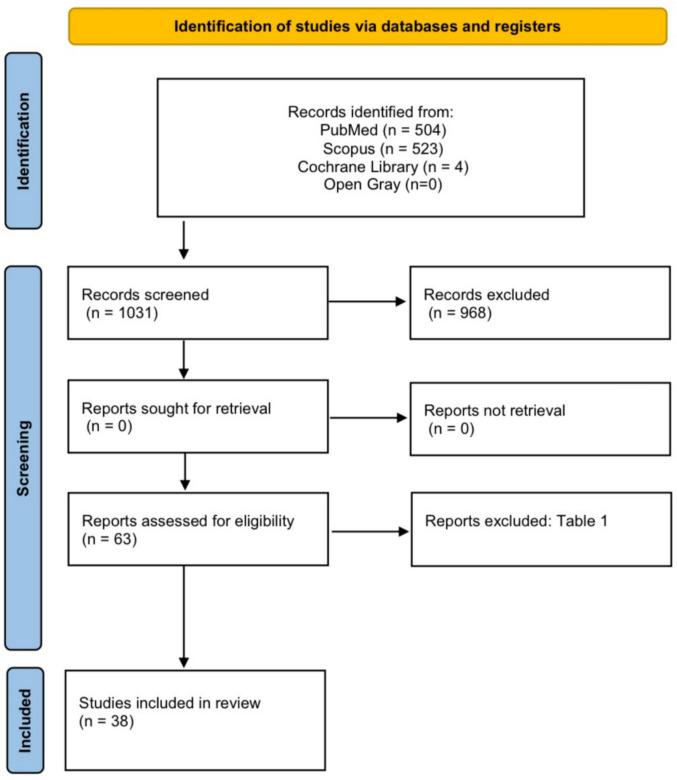 Figure 1
Figure 1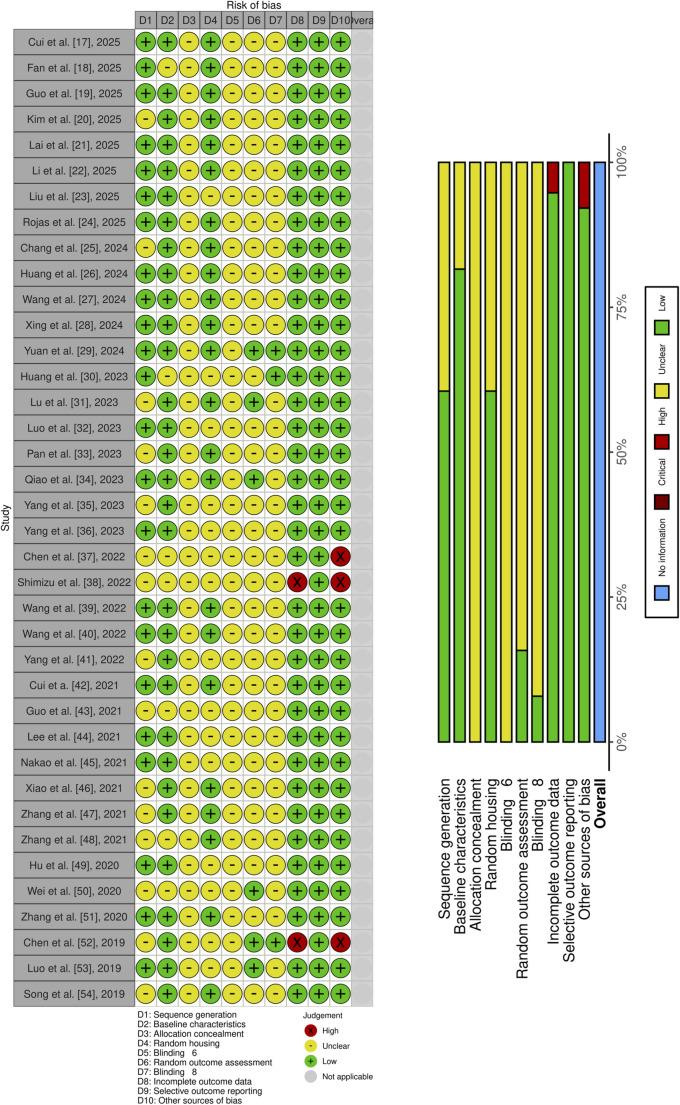 Figure 2
Figure 2- —Universidade Do Oeste Paulista
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsExtracellular vesicles in disease · Mesenchymal stem cell research · Alkaline Phosphatase Research Studies
Introduction
Bone remodeling, or bone turnover, is characterized by the balance between bone resorption and regeneration. This physiological process is vital for physiological activities that include adequate growth, skeletal maintenance, and proper serum calcium levels [1–3].
Osteoclastogenic cytokines, such as the ligand for receptor activating factor kB nucleus (RANKL) and macrophage colony-stimulating factor (M-CSF), participate in bone turnover [2–4]. RANKL is a cytokine that binds to the receptor activator of nuclear factor kB (RANK) present on the surface of hemopoietic cells and macrophage precursors of clastic cells [2–4]. In these same cells, there is the c-fms receptor where M-CSF binds. These cytokines, linked to their receptors, promote osteoclast differentiation [2–4].
Osteoclasts, with the aid of integrins and actin fibers, attach to the bone surface and secrete cathepsins, metalloproteinases, ions, and other products, leading to the degradation of the bone matrix and hydrolysis of the collagen-rich matrix [1–6]. Subsequently, osteoprotegerin (OPG) is secreted and binds to RANKL, modifying its form and blocking the interaction with RANK. Thus, the formation of new clastic cells is blocked, and the resorption process is interrupted [5, 6]. Bone sialoprotein (BSP) contributes to bone formation, restoring the bone tissue [5, 6], and consequently maintaining balance in the bone remodeling process. Macrophages also participate in bone remodeling by secreting pro- or anti-resorptive cytokines. Type 1 (M1) macrophages secrete interleukin 1 (IL-1) and tumor necrosis factor alpha (TNF-α), which are pro-resorptive cytokines that stimulate the production of RANKL and M-CSF. Type 2 macrophages (M2), under the action of IL-4, IL-10, or IL-13, enable osteoblasts to secrete OPG [3, 5–7].
Disorders in the bone turnover process can culminate in the onset of pathologies characterized by an increase in bone mass, such as in cases of osteopetrosis, or in situations in which the rates of bone resorption are greater than those of new formation, such as in cases of osteoporosis [8–11]. Chronic inflammatory diseases also influence disorders of the bone remodeling process, as they promote the significant production of pro-resorptive cytokines such as TNF-α, IL-1, and IL-6 [9], culminating in the interruption of the balance between the actions of osteoblasts and osteoclasts.
Current treatments for pathologies characterized by high rates of bone resorption and loss of bone mass involve the use of drugs that either inhibit osteoclastic action or increase bone deposition [10–12]. Clastic cell inhibitors, such as bisphosphonates, calcitonin, monoclonal antibodies, and estrogen, have been used in medical practice for many years [10–12]; however, these drugs negatively influence osteoblastic function and bone tissue deposition, in addition to causing gastrointestinal irritation [10, 12]. Medications that increase bone deposition, such as some hormones and strontium ranelate, can cause significant complications with long-term use; these include nausea, cramps, vascular changes, and osteosarcoma [11].
In an attempt to eliminate the side effects associated with the cited medications, different methods have been proposed and developed [9–11]. Among these, “cell-free” therapies, which use extracellular vesicles extracted from different cell types, especially stem cells, can be an alternative [13, 14].
Extracellular vesicles (EVs) have similar functions to those of the cells from which they are extracted. Song et al. [10], in 2019, detected that EVs were able to inhibit osteoclastogenesis in vitro and reduce bone resorption in vivo. Hu et al. [9], in 2021, described that exosomes, a type of extracellular vesicle, were capable of affecting the polarization of macrophages and regulating the inflammatory response via RANKL. Lee et al. [13], in 2021, verified that EVs extracted from adipose stem cells participate in the suppression of osteoclast differentiation and support the secretion of cytokines that favor bone remodeling. Cui et al. [11], in 2022, concluded that EVs can collaborate with the decrease in RANKL expression and thus control the resorptive process.
Therefore, the use of EVs is considered a promising and biocompatible therapy focused on the treatment of diseases involving bone resorption. Thinking in the aspects discussed above, one emerging question is whether therapy with EVs is superior for addressing bone resorption. Additionally, important questions arise regarding the appropriate dosage, form of administration, methods for extraction and characterization, and the specific cell types from which the EVs originate. The investigation of molecular mechanisms and cell types involved in the control of bone resorption resulting from the use of EVs is also questioned. These data will be crucial for guiding future clinical practices in humans.
Thus, the objectives of the present study were, by a systematic review, to analyze the usefulness of EV therapy in controlling bone resorption-related diseases, and to recognize the molecular mechanisms participating in this process. The description of origin cells, dosage, form of administration for the use of EVs, as well as the method of extraction and characterization of them, were included in the objectives.
Material and Methods
The systematic review was conducted following the recommendations of “The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) [15]. This study was registered in Prospective Register of Systematic Reviews (PROSPERO CRD42024493291).
Eligibility Criteria and PICO Question
The inclusion criteria were: (1) in vivo animal models with stimulated bone resorption, (2) studies analyzing the EVs and bone resorption, (3) comparing studies to use of EVs or not, (4) studies explaining the molecular mechanisms involved in the control of bone resorption, (5) studies detailing the dosage, form of use, and origin-cell of EVs, as well as method of extraction and characterization of EVs.
The exclusion criteria were: (1) in vivo animal models without stimulated bone resorption, (2) studies that have not analyzed bone resorption, (3) studies with the absence of a comparator control group, (4) studies that have not analyzed the molecular mechanisms involved in the resorptive process, (5) studies have not analyzed the origin cell, and method of extraction and characterization of EVs, (6) studies have not analyzed the dosage and form administration of EVs, (7) studies with EVs from tumoral cells or plants, or mimetics extracellular vesicles, (8) review articles, non-comparative studies, commentaries, editorials, case reports, case series, conference abstracts, clinical cases, and sillico studies. For studies with missing data, including origin cell, method of extraction and characterization of EVs, dosage, or form of administration, authors were contacted via e-mail for three times; the lack of requested information resulted in the exclusion of the article.
The specific clinical question (PICO: Population, Intervention, Comparison, Outcome) was: Would therapy with EVs be useful for the treatment of bone resorption-related diseases in vivo? In this approach, (P) represented animals with stimulated bone resorption, (I) referred to therapy with EVs, in comparison to (C) not using them, and (O) related to the control of bone resorption. The control of bone resorption and its molecular mechanism were considered the primary and secondary outcomes, respectively. The dosage, form of administration, origin cell, and method for extraction and characterization of EVs were also described.
For each study, the comparison group was considered a criterion for inclusion, and the absence of a comparative control group was considered an exclusion criterion. Control groups consisted of animals not receiving EVs treatment, such as sham-operated groups, vehicle-treated animals (PBS or other non-EV treatments that did not affect outcomes), or untreated disease models. Our analysis focuses on comparing the use and non-use of EVs; therefore, studies lacking a comparison group were excluded.
Search Strategy and Selection Process
An electronic search was performed in the PubMed/MEDLINE, Scopus, Cochrane Library, and Open Gray Databases for the period up to November 2025. Two independent researchers (FMM and VAFM) led the search in the databases cited data, considering the following keywords: (a) exosome, (b) extracellular vesicles, and (c) bone resorption. The search strategy was based on the following crossings: #1 (exosome and bone resorption), #2 (extracellular vesicles and bone resorption), and #3 (exosome and extracellular vesicles and bone resorption). The crossing #exosome and extracellular vesicles was not executed because it included non-specific results directly related to the objectives of this study. No filters were used during searches in PubMed/MEDLINE, Cochrane Library, and Open Gray databases. For the Scopus database, the filter titles, summary, and keywords. The studies were selected by analyzing their title and abstracts regarding the inclusion and exclusion criteria. Disagreements were resolved through online or in-person dialogue, re-reading the article title and abstract, discussing inclusion or exclusion points, and reaching consensus with a third researcher (GGM). At the end of the selection of scientific articles, the level of agreement between the researchers was calculated using the Kappa statistical test [16].
Data Collection Process and Data List
The selected studies were completely considered, and a specific analysis was executed to extract significant data related to the PICO question and the objectives of the present study. A researcher (FMM) collected the pertinent information, adding it to a table that included animal species, diseases or conditions associated with bone resorption, particulars concerning EVs (type or size, method of extraction and characterization, origin cell, dosage, and form of administration of EVs), experimental groups, period, and types of analysis, and outcomes. A standardized form containing the previous items was used for notes and data collection. Afterward, a second researcher (GGM) reviewed the information collected by reading the articles and confirming each piece of information extracted by the first author, comparing the data presented in the table with the written article. Any disagreements were resolved through dialogue, either online or in person, by re-reading the article, selecting specific data, and comparing it with previously extracted data, with a consensus reached with another researcher (VAFM).
Data Synthesis Process
A meta-analysis was not conducted due to insufficient data. The required data were presented in graphical or image-based formats in the majority of studies, which prevented accurate extraction of means and standard deviations for the control and treatment groups. It should be noted the numerical data were available in two studies related to periodontitis. Moreover, the authors of the relevant studies were contacted via e-mail on three separate occasions; however, only three provided the requested information, two specific to osteoporosis and one to periodontitis. In addition, the parameters used in these studies did not allow for comparison among obtained data (Table).Table 1. Articles excluded after full-text analysisAuthor/YearJustificativePI et al. [58]This study did not provide data regarding the dose, despite the author being requested to provide it via emailLi et al. [59]This study did not provide data regarding the dose, despite the author being requested to provide it via emailZhou et al. [60]Study in vitro, onlyCai et al. [61]The use of Evs was evaluated only in vitroChoi et al. [62]Study in vitro, onlyDuan et al. [63]The study evaluated the composition of vesicles extracted from sham and OVX rats and their action on cells in different conditionsLi et al. [64]This study did not provide data regarding the dose, despite the author being requested to provide it via emailLi et al. [65]Although authors studied osteolysis, its occurrence was due to the placement of prostheses and not a disease that induces bone resorption through its intrinsic physiopathologyPan et al. [66]Although authors studied osteolysis, its occurrence was due to the placement of prostheses and not a disease that induces bone resorption through its intrinsic physiopathologySedik et al. [67]This study did not evaluate bone resorptionXie et al. [68]Although authors studied osteolysis, its occurrence was due to the placement of prostheses and not a disease that induces bone resorption through its intrinsic physiopathologyYin et al. [69]This study did not evaluate the use of extracellular vesiclesZhang et al. [70]The focus was not the control of bone resorptionRen et al. [71]This study did not evaluate the treatment of bone resorptionYe et al. [72]Study in vitro, onlyGao et al. [73]Although authors studied osteolysis, its occurrence was due to the placement of prostheses and not a disease that induces bone resorption through its intrinsic physiopathologyLi et al. [74]Although authors studied osteolysis, its occurrence was due to the placement of prostheses and not a disease that induces bone resorption through its intrinsic physiopathologyWang et al. [75]Study in vitro, onlyYang et al. [76]The objective of this study was to compare the action of exosomes extracted from normal patients and patients with congenital pseudarthrosis of the tibiaHayashi et al. [77]The study used polyethyleneimine nanoparticles (PEI-NPs) and not extracellular vesicles (EVs)Qayoom et al. [78]The work did not focus on the study of EVs since no group was treated only with vesiclesYun et al. [79]The EVs were not extracted from cells, but from bovine colostrumCui et al. [80]This study did not analyze the use of EVs in an animal model with bone resorptionHu et al. [81]The EVs were not extracted from cells, but from blood plasmaXu et al. [55]This study did not analyze the use of EVs in an animal model with bone resorption
As a result, studies were grouped by disease model. Table 2 described the osteoporosis and related conditions, Table 3 addressed periodontitis, and Table 4 included other diseases for which there were insufficient studies for grouping. Each disease type was analyzed separately, providing a comprehensive overview. Outcomes were similar across groups, and final results were based on all collected data. The same analytical method was used for molecular and structural endpoints. For further details, the respective disease tables can be consulted.Table 2. Summary of characteristics and results from individual osteoporosis studies StudyAnimal specie and numberDisease associated with bone resorptionExtracellular vesiclesGroupsAnalysisPrimary outcomeSecundary outcomesizeextraction and characteriza-tionorigin-celldosageadministrationperiodstypesKim et al. [20]10-week-old female Sprague–Dawley rats (n = 48)OVX-osteoporosis < 100 nm (peak 77 nm)Ctfr, Filtration, and TEM, NTA, proteome analysis, WB, ELISAHuman Amniotic Membrane Stem CellsEVs (1 × 108, 3 × 108 or 1 × 109 particles/rat), ZA (100 ug/kg) or vehicle (PBS – 100 uL/rat)Systemic injection (intravenously once a week for 8 weeks)Sham, OVX, ZA, EVs (1 × 108), EVs (3 × 108) and EVs (1 × 109)8 weeksELISA, biochemistruy analysis, dual energy X-ray, micro-CT, Biomechanical MeasurementEVs treatment (1 × 10^9) attenuated cancellous bone loss and restored bone mineral density and bone strengthIncrease of 17β-estradiol, ALP, calcium, GFs, and osteogenesis after treatment (near-full recovery in the high-dose 1 × 10^9)Chang et al. [25]8-week-old female C57BL/6 mice (n = 40)OVX-osteoporosis150 nmUCtfr, flow cytometry, WB, RT-PCR, and TEMMesenchymal stem cellsAntimouse RANKL antibody (5 mg/kg), EV (5 μg/μL) and EV@R (5 μg/μL). Sham and OVX injected with PBSSystemic injection (intravenously injection through tail vein every 3 days for 8 weeks)Sham, OVX, EV, EV@R and anti-RANKL8 weeksMicro-CT, EDTA, TRAP, IHC, IF, WB, RT-qPCR, flow cytometryEV@R (EVs from MSCs overexpressing RANK) reversed osteoporosis conditions through inhibiting bone loss and promoting bone regenerationReduction of TRAP and RANKL, and increase of OCN, Osterix, Runx2, and COL-1 in EV@R groupWang et al. [27]3-month-old or 15-month-old male C57BL/6 mice (n = 30)Senile osteoporosis117.5 ± 32.5 nm (YO-EVs) and 107.5 ± 40.5 nm (SO-EVs)UCtrf and TEMyoung (YO) and senescent (SO) osteocytes100 ug per ml of PBSSystemic injection (in tail vein twice per week during 1 month)Control, YO-EVs, and SO-EVs4 weeksHE, IHC, micro-CT, qRT-PCR, flow cytometry, proteomic analysisControl of bone resorption and occurrence ofbone regeneration more significant in group with YO-Evs therapyDecrease of RANKL, TRAP and osteoclasts, and increase of ALP, OCN, and osteoblasts in YO-Evs therapy groupXing et al. [28]12-week-old male Sprague–Dawley rats (n = 24)DO30–130 nmCtfr and TEM, WB, NTASkeletal muscle tissues0.8 mg/kg body weightSystemic injection (in tail vein every other day for 8 times in total)Sham, DN + PBS and DN + ES_-_Exo8 weeksHE, IHC, micro-CT, WB, qRT-PCR, ELISAEVs promoted osteogenesis as well as suppress bone resorptionDN + ES-Exos enhanced OCN and Runx2, reduced positive staining of bone resorption marker CKHuang et al. [30]6-week-old male C57BL/6 J mice (n = 40)DO50–200 nm (114.3 nm ± 5.0 nm)Ctrf and CSLMSkeletal muscle tissue200 ug of EVs in 200uL of salineSystemic injection (intravenously injection twice per week for 3 weeks)Sham, Control1, Control2, DS + EVs1, and DS + EVs24 weeksMasson, IHC, IF, micro-CT, qRT-PCR, WBControl of bone resorption and occurrence of bone regenerationmore significant in therapy with EV independently of DO etiologyDecrease of TRAP and osteoclastogenesis, and increase of Runx2, ALP, Osterix, COL-1 and osteoblasts when the EVs therapy was usedYang et al. [35]Female C57BL/6 mice (n = 24)OVX-osteoporosis30-150 nmUCtrf and TEMMacrophage (Mφ) cultived with or without SrBGNs100 μg of EVs in 100 μl PBSLocal injection (intraperitoneally twice per week during 4 weeks)Sham, PBS, Mφ-EVs e SrBGN + Mφ-Evs4 weeksHE, Masson, IHC, micro-CT, qRT-PCR, WB e ELISAControl of bone resorption and occurrence of bone regeneration more significant in SrBGN + Mφ-Evs, groupDecrease of TRAP, RANKL, Th17, and osteoclasts, and increase of Treg, Runx2, OPN and osteoblastsYang et al. [36]8-week-old female C57BL/6 mice (n = 30) and 12-week-old female Wistar rats (n = 12)OVX-osteoporosis100 nmCtrf and TEMmc3t3-e1 cells30 μg of EVs in mice, and 100 µg of EVs in ratsLocal injection (in periosteal into the marrow cavity of the tibiae once a week during 8 weeks in mice; Injection in socket once a week during 8 weeks in rats)MIce: Sham, DS + EVs, DS + EVs + EphA2, DS + EVs + METTL14, DS + EVs + EphA2 + METTL14 Rats: DS + ZOL, DS + EVs + METTL14, and DS + EVs + EphA2 + METTL148 weeksHE, IHC, IF, micro-CT, WB, qRT-PCRBone regeneration, and absence of osteonecrosis in groups with EVs + METLL14Inhibition of osteoclast differentiation via inhibition of NFATc1 in groups with EVs + METLL14Wang et al. [40]12-week-old female C57BL/6 mice (n = 40)OVX-osteoporosis40–100 nmCtrf and TEMMesenchymal Stem Cells (MSCs)20 µL de MSC-EvsLocal injection (in femural periosteum twice at one week)Sham, DS, DS + miR-27, DS + miR-27 mimic, DS + DMSO, DS + MSC-EVs, DS + MSC-Evs + miR-27 inibidor, DS + MSC-Evs + miR-27 inibidor + RNA-DKK21 weekHE, IHC, micro-CT, ELISA, WB, qRT-PCRControl of bone resorption and occurrence of bone regeneration more significant in group with MSC-EVs therapyDescrease of osteoclasts differentiation, and increase of ALP, OCN and Runx2 with MSC-EVs therapymiR-27a participation in DKK2 inibitionYang et al. [41]8-week-old female C57BL/6 mice (n = 40)OVX-osteoporosis40-130 nmCtrf and SEM (scanning electron microscope)BMSCs modified or not with micro-nano bioactive glass (BGN)100 µg de EVs in 100 µL of PBSLocal injection (intraperitoneally injected thrice a week for 4 weeks)Sham, DS, DS + EVs e DS + BGN + EVs4 weeksHE, Masson, IHC, micro-CT, qRT-PCR, WB e ELISAControl of bone resorption and occurrence of bone regeneration more significant in group with BGN + EVs therapyInhibition of osteoclasts, and normal indices of OPG in BGN + EVs groupCui et al. [42]12-week-old female C57BL/6 mice (n = 48)OVX-osteoporosis99.8 ± 34 nm and 118 + -42 nmCtrf and TEMderivated of induzed pluripotent stem cells (iMSCs)1.0 × 10^11^ particles in 100 μL PBSSystemic injection (intravenouslyinjected once a week for 6 weeks through the tail vein)Sham, DS + PBS, DS + EVs (BT-Exo, Exo-siShn3, BT-Exo-siShn3, or BT-Exo-siCon)2 monthsHE, IF, RT-PCR, WB, ELISAControl of bone resorption and occurrence of bone regeneration more significant in group with BT-Exo-siShn3 therapyIncrease of OPG, ALP, OCN and osteoblastic differentiation in BT-Exo-siShn3 groupLee et al. [44]8-week-old female mice (n = 24)OVX-osteoporosis88 nmFiltration and TEMAdipose tissue derived Stem Cells (ASCs)ASC-EVs (1 × 10^8^ ou 5 × 10^8^ particles in 100 μl of PBS) or ASCs (5 × 10^5^ cells in 100 μl of PBS)Systemic injection (intravenously injected; ASC-EVs, thrice a week for 2 weeks; ASCs once a weekfor 2 weeks)Sham, DS + PBS, DS + ASCs, and DS + ASC-EVs5 weeksIHC, micro-CT, qRT-PCR, WB, ELISA,flow cytometrySimilar control of bone resorption in EVs and Cells groupsDecrease of RANKL, TRAP and osteoclast, and balance of OPG levelsmiR-21-5p participation in Acvr2a down-regulationXiao et al. [46]6-month-old male C57BL/6 J mice (n = 30)DOP105 nmCtrf and TEMBMSCs5 mg/kgSystemic injection (tailvein injections twice a week for 4 weeks of 0.1 mL per injection)DS + PBS, DS + EVs, DS + CMS-EVs (cyclic mechanical stretch-exposed EVs)4 weeksHE, IHC, micro-CTControl of bone resorption more significant in CMS-EVs groupDecrease of RANKL and actin of osteoclasts in CMS-EVs groupZhang et al. [47]8 and 10-week-old SD rat (n = 63)Diabetic osteoporosis40–100 nmFiltration, Centrifugation and TEMASCs1.6 mg/kg de EVsSystemic injection (in tail vein every two days)Sham, DS + PBS, DS + EVs42 daysdual-energy X-ray, WB, qRT-PCR, ELISAControl of bone resorption with EVs therapyDecrease of pro-inflammatory cytokines and osteoclasts, and inhibition of inflammassome in EVs groupsZhang et al. [48]8 and 10-week-old SD rat (n = 75)Diabetic osteoporosis50-100 nmUCtrf and TEMEpididimal adipose tissue derived MSCs1.6 mg/kg EVs (Exo, vector-Exo, or miR-146a-Exo)Systemic injection (into the tail vein)Sham, DS + PBS, DS + EVs (Exo, vector-Exo, or miR-146a-Exo)12 semanasdual-energy X-ray, WB, qRT-PCR, ELISAControl of bone resorption with EVs therapy, especially in miR-146a-Exo groupDecrease of pro-inflammatory cytokines and osteoclasts, and inhibition of inflammassome in EVs groupsmiR-146a enhanced the inhibitory effect on bone resorption of osteoclastsHu et al. [49]8-week-old female C57BL/6 mice (n = 30), 16-week-old male (n = 16) and 3-month-old mice (n = 30)OVX-Osteoporosis, senile osteoporosis and DO60-150 nmCtrf and TEMHuman umbilical cord MSCs100 μg of EVs in 100 μl of PBSSystemic injection (intravenously into the tail vein once a week during 2 or 3 months or OVX-and senile osteoporosis, respectively. For DO, the injection twice a week during 21 days)Sham, DS + PBS, and DS + EVs2 months (OVX) and 3 months (senile and DO)HE, IHC, micro-CT, ELISA, qRT-PCR e WBControl of bone resorption and occurrence of bone regeneration more significant in group with EVs therapyDecrease of TRAP and osteoclasts, and increase of Runx2, COL-1 and osteoblastsChen et al. [52]8 and 10 weeks-old female C57BL/6 mice (n = 30), 16-month-old mice (n = 16), 3-month-old mice (n = 31)OVX-osteoporosis, senile osteoporosis, DO50 nmCtrf and TEMurine-derived stem cells (postmenopausal women)100 µg de EVsSystemic injection (into tail vein once a week during 2 and 3 months for OVX-and senile osteoporosis, respectively. For DO, the injection twice a week for 3 months)Sham + PBS, DS + PBS, DS + EVs2 months (OVX) and 3 months (senile and DO)HE, IHC, micro-CT, WB, qRT-PCR, WB, ELISAControl of bone resorption and occurrence of bone regeneration more significant in group with EVs therapyDecrease of TRAP and osteoclasts, and Increase of OCN, ALP, Runx2, OPG and osteoblastsLuo et al. [53]3-month-old female C57BL/6 mice (n = 24) and 3-month-old male C57BL/6 mice (n = 12)OVX-osteoporosis and bone fracture35 a 105 nmCtrf and TEMBMSCs100µL of EVsSystemic injection (into the tail vein once a week during 2 or 6 weeks for OVX or frature, respectively)Sham + PBS, DS + PBS, DS + EVs, DS + EVs + Aptamer2 monthsIHC, micro-CT, qRT-PCR, flow cytometryBone regeneration more significant in group with EVs therapy; absence of influence in bone resorptionIncrease of ALP, Runx2, and osteoblasts in EVs groups; levels of TRAP and osteoclasts did not modify with use of EVsSong et al. [54]8-week-old female C57BL/6 mice (n = 27)OVX-osteoporosis106–150 nmUCtrf and TEM or NTAVascular Endothelial Cells100 μg of EVs in 100 μL of PBSSystemic injection (intravenous injection twice a week per 6 weeks)Sham, Disease, and Disease + EVs6 weeksHE, IHC, micro-CTControl of bone resorption and occurrence of bone regeneration more significat in EVs groupDecrease of pro-inflammatory cytocynes, TRAP, and osteoclasts in EVs groupmiR-155 participated reducing bone resorptionNTA: nanoparticle tracking analysis, Ctrf: centrifugation, TEM: Transmission electron microscopy, LPS: Lipopolysaccharides, EVs: Extracellular vesicles, PBS: Phosphate-Buffered Saline, DS: disease, HE: Hematoxylin and eosin, IHC: Immunohistochemistry, IF: Immunofluorescence, micro-CT: Micro computed tomography, WB: Western blot, qRT-PCR/RT-PCR: Real-time polymerase chain reaction, RANKL: Receptor activator of nuclear factor kappa-Β ligand, TRAP: Tartrate-resistant acid phosphatase, UCtrf: Ultracentrifugation, ALP: Alkaline phosphatase, OCN: Osteocalcin, IL-10: Interleukin-10, Runx2: Runt-related transcription factor 2, OPN: Osteopontin, VEGF: Vascular endothelial growth factor, DO: disuse osteoporosis, CLSM: confocal laser scanning microscope, COL-1: type 1 collagen, OVX: ovariectomy, SrBGNs: strontium doped bioactive glass nano-particles, Sham: un-manipulated animal, Th17: T helper 17 cell, Treg: regulatory T cell, EphA2: Ephrin type-A receptor 2—METTL14—methyltransferase 14, N6-adenosine-methyltransferase subunit, ZOL: Zoledronic acid, TGF-beta 1: transforming growth factor-beta 1, DMSO: dimethylsulfoxide, TNF-α: Tumor Necrosis Factor AlphaTable 3Summary of characteristics and results from individual periodontitis studiesStudyAnimal specie and numberDisease associated with bone resorptionExtracellular vesiclesGroupsAnalysisPrimary outcomeSecundary outcomesizeextraction and characteriza-tionorigin-celldosageadministrationperiodstypesCui et al.[17]8-week-old male C57BL/6 J mice (n = 24)PeriodontitisAE2Ns (157.9 nm), and Kae@AE2Ns (152.1 nm)UCtfr, TEM, NTAMacrophages M2 and macrophage-derived apoptotic vesiclesAE2Ns and Kae@AE2Ns (5 mg/kg)Local injection (periodontal tissue every two days)Control, ligature, AE2Ns and Kae@AE2Ns10 daysMicro-CT, HE, Masson, IHC, IF, WB, qRT-PCRThe EVs were capableof mitigate periodontal inflammation, reduced the periodontal deterioration, and promote periodontal bone repair. The Kae@AE2Ns group exhibiting the most pronounced improvementIncrease of of ONC and COL1, and reducion ofinflammatory cellsFan et al.[18]8-week-old male Sprague Dawley (n = 25)Diabetic periodontitisNSUCtfr and TEM, SEMSchwann cellsPGSP, SC Exo, and GSP@SC Exo (1 μg/μL, 100 μL) and Sham and control (equivalent PBS)Local injection (periodontal pocket twice weekly for 2 and 4 weeks)Sham, control, PGSP, SC Exo and GSP@SC-Exo2 and 4 weeksELISA, qRT-PCR, micro-CT, HE, IHCGSP@SC-Exo has effect on bone regeneration, promotes neovascularization. And immunoinflammatorymodulationIncrease of OPN and OCN, M2macrophage polarization, and alleviation of local inflammation and antioxidant and antibacterial capacityGuo et al.[19]4-week-old male Sprague Dawley rats (n = 26)Diabetic periodontitisAverage size 120 nmUCtfr and TEMTissue of antler blastema obtained from a healthy 2-year-old male sika deerAnSC exos (50 μg/ml) and hBMSC-exos (50 μg/ml) and PBS (10uL)Local injection (periodontal pocket on alternate days)Normal, Ligation, Control, hBMSC-exo and AnSC-exo3 weeksMicro-CT, HE, IHC, IF, ARS, ALP, qRT-PCR, WB,AnSC-Exo reduced effectively alveolar bone destruction and resorption under diabetes condition, and demonstrated significantly less inflammatory cells compared to other groupsReduction of IL-1β, and inflammatory process in AnSC-exo group, as well as increase of IL-10Lai et al.[21]8-week-old male C57BL/6 mice (n = 24)Periodontitis50-150 nmUCtfr and TEM, NTA, WB, RT-PCRMacrophages DP7-C stimulated10 µL of exosome suspension (1.2 µg/µL, containing 12 µg of exosomal protein) or 10 µL of PBSLocal injection (into the gingiva tissue at six distinct buccal and palatal sites every 3 days)Control, Exo^Blank^, Exo^DP7−C^ and Exo^miR−21b^14 daysMicro-CT, HE, IHC, dual-luciferase, qRT‒PCR, WBExo^miR−21b^ group demonstrated reduced alveolar bone loss, higher bone volume and bone mineral density, greater trabecular thickness and number, and New bone formation were detected at the alveolar crest areaReduction of inflammatory infiltrates and osteoclast. Increase of Osterix in Exo^miR−21b^ group. Exosomal miR-21b targets SOCS1 to activate the JAK2/STAT3 signaling pathwayLi et al.[22]7-weeks-old female C57BL/6 mice (n = 20)Periodontitis50-150 nmLyophilized-Evs, TEM, SEM, and DLSHuman Umbilical Cord Mesenchymal Stem Cells50μL (hydrogel) and 50μL (exo@H = 1.2 × 1010 particles /mL)Local injection (around mouse’s teeth twice a day during 8 days)Sham, Model, Hydrogel and Exo@H8 daysWB, HE, GO and KEGG, RT-qPCR, Luciferase Reporter AssayExo@H group revealed significant reduction in alveolar bone resorption and inflammatory response of periodontal tissues. There was no significant difference between model and hydrogel groupDecrease of TRAP and osteoclasts numbers, downregulation of miRNAs which modulates inflammatory responses pathways in periodontal tissue in Exo@H groupLiu et al.[23]6-week-old male C57BL/6 mice (n = 20)PeriodontitisNC-EVs (130 ± 50.0 nm) and EPO-EVs (131 ± 50.9 nm)Ctfr UCtfr, and TEM, NTAErythropoietin stimulated macrophage100uL hydrogel, NC-EVs/hydrogel, EPO-EVs/hydrogel (100uL) or PBS (100uL)Local injection (once a week for 3 weeks)Control, Hydrogel, NC-EVs/hydrogel and EPO-EVs/hydrogel3 weeksqPCR, WB, micro-CT, IF, HE, dual-luciferase assayEPO-EVs/hydrogel effectively alleviated the destruction of alveolar bone in the experimental periodontitis mouse modelIncrease of OCN in EPO-EVs/hydrogel treatment. miR-5107-5p promotes alveolar bone regeneration via the EGFR/RhoA axis in EPO-EVs groupRojas et al.[24]C57BL/6 wild-type mice (N = NS)Periodontitis100–200 nm (mean size 141 nm ± 71 nm). Other three small fractions were observed, ranging from around 288–506 nmUCtfr and TEM or NTARegulatory T cell (Treg)1 × 10^8^ or 2.5 × 10^8^ RATEVs in 5µL of PBS. Sham injections with PBS as RATEVs-free control were usedLocal injection (palatal periodontal mucosa to the second molars at day 3 and 6 after ligature)Healthy, Perio, Perio + RATEVs-lo and Perio + RATEVs-hi10 daysWB, flow cytometry, TRAP, EDTARATEVs inhibit osteoclastogenesis and ameliorate alveolar bone loss during experimental periodontitisReduced TRAP, RANKL, CD4 + Foxp3 + Tregs, IL-17A, and osteoclast number in the groups RATEVs. Increase of CD73 expression in RATEVs groupHuang et al. [26]8-week-old male C57BL/6 mice (n = 18)Periodontitis130 nm (NTA) or 30–200 nm (TEM)Ctrf and TEMLPS-dental follicle cells100 ug of Evs per ml of PBSLocal injection (in periodontal tissue on 3 times at 2-day intervals over one week)Control, DS, and DS-EVs2 weeksHE, IHC, IF micro-CT, WB, qRT-PCR, flow cytometryControl of bone resorption more significant in group with EVs therapyDecrease of RANKL, TRAP and osteoclasts, and increase of M2-type macrophage in EVs groupLu et al. [31]6 and 8-week-old male mice (n = 24)Periodontitis50–150 nmCtrf and TEMPeriodontal ligament stem cells300 ug of EvsLocal injection (in periodontal tissue once a week during 4 weeks)Control, DS, DS-EVs1 (normal glucose), and DS-EVs2 (high glucose)4 weeksHE, micro-CT, RT-PCR, WBControl of bone resorption and occurrence of bone regeneration more significant in therapy with EV cultured in normal glucose conditionsDownregulation of genes involved in osteoclastogenesis was more significant when EVs were extracted from stem cells and cultured in normal glucose conditionsMiR-31-5p participation on eNOS inhibitionLuo et al. [32]8-week-old male SD ratsPeriodontitis40–120 nmUCtrf and TEMCXCR4-overexpressing 293 T/17 cells300 ugLocal injection (into the periodontiumof the second maxillary molar)Control, DS-EVs, DS-CXCR4-miR126-EVs, miR126-EVs2 weeksHE, IHC, micro-CT, WB, qRT-PCR, ELISAControl of bone resorpotion more significant in CXCR4-miR126-Evs groupDescrease of pro-inflammatory cytocines, TRAP, M1-type macrophage and osteoclasts, and increase of IL-10, and M2 type macrophage in CXCR4-miR126-Evs groupmiR-126 participation in p48 MAPK signaling pathwayPan et al. [33]6 and 8-week-old male C57BL/6 mice(n = 24)Periodontitis30–200 nmUCtrf and TEMOsteoclasts4ug of EvsLocal injection (10μL of PBS or OC-EVs in second molar at 0, 4, 8, and 12 days)Control, DS-PBS, and DS + EVs14 daysHE, IHC, micro-CT, qRT-PCR, WBAbsence control of bone resorption and bone regeneration when EVs from osteoclasts were usedDecrease of Runx2, ALP and osteoblasts, and increase of pro-inflammatory cytokines, TRAP and osteoclastsmiR-5134-5p participation in JAK2/STAT3 axisQiao et al. [34]8-week-old male SD rats (n = 24)Periodontitis30–150 nm (average size de 84.06 nm)UCtrf and TEMDental Pulp Stem Cells50 ug of EVs per mL of PBSLocal injection (10µL in molars daily per 30 days)Control, DS, DS + PBS, and DS + EVs30 daysHE, IHC, micro-CT, qRT-PCR, WB, flow cytometryControl of bone resorption and occurrence of bone regeneration more significant in EVs groupDecrease of pro-inflammatory cytokines, M1 types macrophages, and osteclasts, and increase of OCN, OPN, COL-1, and M2 type macrophageChen et al. [37]6 and 8-week-old C57BL/6 micePeriodontitis30–150 nmUCtrf and TEMM2 type macrophage50 or 100 µg of EVs in mL of PBSLocal injection (Periodontal)DS + PBS, DS + EVs1, DS + EVs22 weeksHE, IHC, micro-CT, ELISA, flow cytometryControl of bone resorption and occurrence of bone regeneration more significant in EVs groups, especily in high concentrationDescrease of TRAP and osteoclasts, and increase of Runx2, ALP, OCN, and IL-10 in EVs groupsShimizu et al. [38]9 and 10-week-old male C57BL/6 J rats (n = 30)Periodontitis66–110 nmUCtrf and NTAhuman leukocyte antigen (HLA) haplotype homodental pulp cells (HHH-DPCs)5µL of EVs (7.5 × 10^8^ particles)Local injection (at 0, 2 and 4 days after periodontal ligature)DS, DS + saline, and DS + EVs7 days (3 days after the end of applications)HE, IHC, WB, qRT-PCR, micro-CTControl of bone resorpotion more significant in EVs groupDecrease of RANKL, and osteoclasts in EVs groupNakao et al. [45]8-week-old female C57BL/6NCrSLc mice (n = 20)Periodontitis109 ± 3.1 nm and 104 ± 1.8 nmCtrf and TEMGingival tissue derived MSCs20 μg of EVs in 20 μL de PBSLocal injection (into the palatal gingiva)Control-PBS, DS + PBS, DS + EVs, DS + EVs-TNF-α7 daysIHC, RT-PCR, WBControl of bone resorption more significant in group with EVs therapy, especially in EVs-TNF-α groupDecrease of M1-type macrophages, TRAP, RANKL, and osteoclasts, and increase of OPG and M2-type macrophage in EVs groups, especially in group with TNF-αmiR-1260b targeting Wnt5a expression and JNK signaling pathwayWei et al. [50]9 and 10-month-old C male D-1 micePeriodontitis100 nmUCtrf and TEMStem cells from human exfoliated deciduous teeth20 μg of EVsLocal injection (periodontal injection once a week during 2 weeks)Control, DS, DS + PBS, DS + Cell, and DS + EVs4 weeksHE, Masson, IHC, qRT-PCR, WB and flow cytometryControl of bone resorption and occurrence of bone regeneration more significant in group with EVs therapyDecrease of pro-inflammatory cytokines, and increase of ALP, Runx2, and osteogenic differenciationNTA: nanoparticle tracking analysis, Ctrf: centrifugation, TEM: transmission electron microscopy, LPS: lipopolysaccharides, EVs: extracellular vesicles, PBS: phosphate-buffered saline, DS: disease, HE: hematoxylin and eosin, IHC: immunohistochemistry, IF: immunofluorescence, micro-CT: micro computed tomography, WB: western blot, qRT-PCR/RT-PCR: real-time polymerase chain reaction, RANKL: receptor activator of nuclear factor kappa-Β ligand, TRAP: tartrate-resistant acid phosphatase, UCtrf: ultracentrifugation, ALP: alkaline phosphatase, OCN: osteocalcin, IL-10: interleukin-10, Runx2: runt-related transcription factor 2, OPN: osteopontin, VEGF: vascular endothelial growth factor, DO: disuse osteoporosis, CLSM: confocal laser scanning microscope, COL-1: type 1 collagen, OVX: ovariectomy, SrBGNs: strontium doped bioactive glass nano-particles, Sham: un-manipulated animal, Th17: T helper 17 cell, Treg: regulatory T cell, EphA2: ephrin type-A receptor 2—METTL14—methyltransferase 14, N6-adenosine-methyltransferase subunit, ZOL: Zoledronic acid, TGF-beta 1: transforming growth factor-beta 1, DMSO: dimethylsulfoxide, TNF-α: tumor necrosis factor alpha, NS: not specified, DLS: dynamic light scattering, KEGG: kyoto encyclopedia of genes and genomes, GO: gene ontologyTable 4Summary of characteristics and results from individual studies of other diseasesStudyAnimal specie and numberDisease associated with bone resorptionExtracellular vesiclesGroupsAnalysisPrimary outcomeSecundary outcomesizeextraction and characteriza-tionorigin-celldosageadministrationperiodstypesYuan et al. [29]8 and 10-week-old male SD rats (n = 60)Steroid-induced osteonecrosis40–150 nmUCtrf and TEMM2-type macrophage100 ug per ml of PBSSystemic injection (intravenously once a week during 4 weeks)control, PBS, and EVs therapy4 weeksHE, IHC, micro-CT, WB, qRT-PCRControl of bone resorption and occurrence of bone regeneration more significant in group with EVs therapyDescrease of pro-inflammatory cytokines, TRAP and M1-type macrophage, and increase of M2-type macrophage, IL-10, ALP, Runx2, OPN, OCN, VEGFWang et al. [39]8-week-old male C57BL/6 mice (n = 48)Osteoartritis30–150 nmExossome extraction kit and NTABone Marrow Stem Cells (BMSCs)10 µL of Evs per mL of salineLocal injection (in joint cavity everyday per 8 weeks)Sham, Saline, EVs, and EVs + TGF-beta14 and 8 weeksHE, IHC, IF, RT-PCR, WB, micro-CTControl of bone resorption and occurrence of bone regeneration more significant in group with EVs-TGFbeta therapyDescrease of TRAP, RANKL and osteoclastogenesis when the EVs-TGFbeta therapy was usedmiR-135b participation in MAPK6 pathwayGuo et al. [43]Male rats (n = 20)Mandibular hypoplasia (GATA-4 knockout)100 nmCtrf and TEMOrofacial stem cells2 mg of EVs per ml of PBSLocal injection (two injection in periosteum of mandibular molar region every 3 days until 21 days)control (PBS), and EVS21 daysHE,micro-CT, qRT-PCR e WBControl of bone resorption and occurrence of bone regeneration more significant in group with EVs therapyIncrease of OPG, OCN, OPN, Runx2 and decrease of RANKL and activation of osteoclast when EVs were usedmiR-206-3p participation on NFATc1 regulationZhang et al. [51]Female SD rats with 200-300 g (n = 60)Glucocorticoid-induced osteonecrosis20-100 nmUCtrf and TEMHuman MSCs100 uL of EVs in 200 uL of PBSSystemic injection (in tail vein daily for three weeks)Sham, Disease, Disease + EVs, and Disease + EVs + miR-135b3 semanasIHC, micro-CT, WB, qRT-PCR, flow cytometryControl of bone resorption and occurrence of bone regeneration more significant in group with EVs therapy, especially in EVs + miR-135b groupDecrease of apoptosis to osteocytes, and increase of OCN and osteoblasts in EVs therapy groupsmiR-135b regulated PDCD4, caspase-3 and OCNNTA: nanoparticle tracking analysis, Ctrf: centrifugation, TEM: transmission electron microscopy, LPS: lipopolysaccharides, EVs: extracellular vesicles, PBS: phosphate-buffered saline, DS: disease, HE: hematoxylin and eosin, IHC: immunohistochemistry, IF: immunofluorescence, micro-CT: micro computed tomography, WB: western blot, qRT-PCR/RT-PCR: real-time polymerase chain reaction, RANKL: receptor activator of nuclear factor kappa-Β ligand, TRAP: tartrate-resistant acid phosphatase, UCtrf: ultracentrifugation, ALP: alkaline phosphatase, OCN: osteocalcin, IL-10: interleukin-10, Runx2: runt-related transcription factor 2, OPN: osteopontin, VEGF: vascular endothelial growth factor, DO: disuse osteoporosis, CLSM: confocal laser scanning microscope, COL-1: type 1 collagen, OVX: ovariectomy, SrBGNs: strontium doped bioactive glass nano-particles, Sham: un-manipulated animal, Th17: T helper 17 cell, Treg: regulatory T cell, EphA2: ephrin type-A receptor 2—METTL14—methyltransferase 14, N6-adenosine-methyltransferase subunit, ZOL: zoledronic acid, TGF-beta 1: transforming growth factor-beta 1, DMSO: dimethylsulfoxide, TNF-α: tumor necrosis factor alpha
Study Risk of Bias Assessment and Reporting Bias Assessment
The risk of bias and the quality of scientific evidence were assessed using SYRCLE's RoB tool, specifically designed for animal studies. This tool consists of 10 items, subdivided into six categories: selection bias, performance bias, detection bias, attrition bias, reporting bias, and other sources of bias. For each of the ten items in this tool, two independent researchers (FMM and VAFM) read the full text article and assigned one of three concepts: affirmative (yes), negative (no), or uncertain (?). These concepts designate low risk of bias, high risk of bias, and unclear data, respectively. Any disagreements were resolved through discussion and agreement with another researcher (GGM), who reread the article and searched for the inconclusive item. The risk of bias for each study was qualitatively assessed by individually observing each item, without applying different weights to them.
Results
Study Selection
A total of 1031 titles and abstracts of articles were analyzed in cited databases, and after applying the eligibility criteria and excluding articles in duplicate, 63 studies were selected (Fig. 1). The Kappa test conducted between the two researchers in the systematic search for databases showed almost perfect since the agreement level was 0.866. After completing the reading and analysis of selected studies, 25 articles were excluded, totaling 38 studies included in our systematic review. Explanations for such exclusions can be seen in Table 1.Fig. 1PRISMA 2020 flow diagram for new systematic reviews which included searches of databases and registers only. From: Page MJ, Mackenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an update guideline for resporting systematic reviews. BMJ 2021;372: n. 71. https://doi.org/10.1136/bmj.n71
Characterization of Studies
All included studies analyzed the control of bone resorption in animal models [17–54]. Bone resorption was induced by different diseases, including osteoporosis [20, 25, 27, 28, 30, 35, 36, 40–42, 44, 46–49, 52–54], periodontitis [17–19, 21–24, 26, 31–34, 37, 38, 45, 50], steroid-induced osteonecrosis [29, 51] osteoarthritis [39], and mandibular hypoplasia [43].
A total of 736 mice and 415 rats were used to evaluate the inhibition of the resorptive process in osteoporosis [20, 25, 27, 28, 30, 35, 36, 40–42, 44, 46–49, 52–54], being 397 mice [25, 35, 36, 40–42, 44, 49, 52–54] and 60 rats [20, 36] with ovariectomy/postmenopausal osteoporosis, 62 mice with senile osteoporosis [27, 29, 49, 52], 155 mice with osteoporosis by disuse [28, 30, 46, 49, 52] and 138 rats with diabetic osteoporosis [47, 48]. Regarding the evaluation of periodontitis, 204 mice [17, 21–23, 26, 31, 33, 38, 45] and 75 [18, 19, 34] rats were used [20, 22, 23, 27, 34, 55]; Luo et al., 2023 [32] did not mention the exact number of rats used, while Rojas et al. [24] and Chen et al. [37] did not accurately determine the number of mice. From another perspective, Wei et al. [50], 2020 cited only the range of animals used in their study, with the sample size being between 4 and 6 rats per group, without precision in the values. For other defects where EVs where tested, 12 mice were used in the bone fracture model associated with osteoporosis [53], 120 rats for defects arising from steroid-induced osteonecrosis [29, 51], 48 mice to evaluate osteoarthritis [39], and 20 rats for investigation of mandibular hypoplasia [43].
In general, EVs were extracted from origin cells using centrifugation [23, 26, 28, 30, 31, 36, 40–43, 45–47, 49, 52, 53], ultracentrifugation [17–19, 21, 23–25, 27, 29, 32–35, 37, 38, 48, 50, 51, 54] or filtration [20, 44, 47]. However, exceptions can be observed in the studies by Li et al. [22] which used the lyophilized EVs; Wang et al. [39], which used an exosome extraction kit, and Lee et al. [44], 2021, which used a multi-filtration system based on tangential flow filtration for the extraction of EVs. Most studies used transmission electron microscopy (TEM) to characterize extracellular vesicles [17–29, 33–37, 40, 42–54]. In addition, some studies used Nanoparticle tracking analysis (NTA) [17, 20, 21, 23, 24, 38, 39, 54], Scanning Electron Microscopy (SEM) [18, 22, 41], Confocal Laser Scanning Microscope (CLSM) [30], and Dynamic Light Scattering (DLS) [22]. All studies used the small extracellular vesicles [17–54].
Principally, the EVs were extracted from mesenchymal stem cells (MSCs) [19, 20, 22, 25, 34, 39–49, 51], especially those derived from bone marrow [19, 39, 41, 46, 53]. Mesenchymal cells from human amniotic membrane [20], gingival tissue [45], orofacial tissue [43], adipose tissue (ASCs) [44, 47], dental pulp [34], epididymis [48], and umbilical cord tissue (UC-MSCs) [22, 49] were also used for extraction. Chang et al. [25], Wang et al. [40], and Zhang et al. [51] removed the EVs from mesenchymal cells but did not specify the type, and Cui et al. [42] obtained the extracellular vesicle from induced mesenchymal stem cells. Other origin cells were used, such as macrophages [17, 21, 23, 29, 35, 37], regulatory T cells [24], dental pulp [38], exfoliated primary teeth [50], skeletal muscle [28, 30], Schuwann cells [18], and multipotent progenitor cells [19]. Furthermore, several other cell types were included as origin cells, and specific information about each can be seen in Tables 2, 3 and 4.
Regarding the posology of EVs in the intervention group, there was no constant value, with a wide variation in both dose and route of administration. Furthermore, EVs were injected locally [35, 36, 40, 41] or systemically [20, 25, 27, 28, 30, 42, 44, 46–49, 52–54], associated with vehicles (PBS or saline) for osteoporosis therapy. For periodontitis, the EVs were administrated via local injection into periodontal tissue in all studies [17–19, 21–24, 26, 31–34, 37, 38, 45, 50]. Systemic administration of EVs was performed for steroid-induced osteonecrosis [29, 51], and local administration was made for osteoarthritis [39], and mandibular hypoplasia [43]. Specific information concerning the posology for each study included in this review can also be seen in Tables 2, 3 and 4.
To assess bone resorption control, regeneration, and the involved molecular mechanisms, the studies utilized histological, image, and molecular analyses. In histological analysis, the tissue was stained or marked with hematoxyline-eosine [17–19, 21–23, 26–29, 31–43, 46, 49, 50, 52, 54], Masson’s trichrome [17, 30, 35, 41, 50], immunohistochemistry [17–19, 21, 25–30, 32–41, 44–46, 49–54] and immunofluorescence [17, 19, 23, 25, 26, 30, 36, 39, 42]. The studies evaluated the quality and quantity of bone with the aid of micro-CT [17–23, 25–41, 43, 48, 49, 51–54] or dual energy X-ray [20, 47, 48] for image analysis. Considering the molecular analysis, the studies used real-time polymerase chain reaction (qRT-PCR/RT-PCR) [17, 19, 21–23, 25–36, 38–44, 46–53], Western-Blot [17, 19–27, 29–52], flow cytometry [18, 20, 24–27, 34, 37, 44, 50, 51, 53], enzyme-linked immunosorbent assay (ELISA) [18, 20, 28, 32, 35, 37, 40–42, 44, 47–49, 52], proteomic analysis [20, 27], and luciferase assay [21–23].
In Tables 2, 3, and 4, findings can be observed about the studied diseases, EVs (type, origin cell, extraction and characterization), posology, experimental groups, periods and analysis, as well as data about the primary and secondary outcomes.
Risk of Bias
The risk of bias was assessed using SYRCLE's RoB tool, considering six categories: selection bias, performance bias, detection bias, attrition bias, reporting bias, and other sources of bias. Selection bias included domains 1 to 3, which encompassed sequence generation, baseline characteristics, and allocation concealment, respectively. Thus, high scientific quality was observed for domains 1 and 2 in 29 [17–19, 21–24, 26–30, 32, 34, 36, 39, 40, 42, 44–54] and 31 [17, 19–29, 31–36, 39–42, 44–47, 49, 51–54] studies; however, for domain 3, all studies showed an unclear risk of bias because it was not possible to determine how, or whether, allocation concealment was performed [17–54].
Regarding performance bias, domain 4, which refers to random housing, showed low and unclear risk of bias in 23 [17–22, 24–29, 31, 34, 39, 40, 42, 46–48, 51, 54] and 15 [23, 30, 32, 35–38, 41, 43–45, 49, 50, 52, 53] studies, respectively. For blinding in domain 5, it was not possible to determine whether blinding occurred during the investigation, as no study clearly reported this information [17–54].
Detection bias, involving randomization and blinding in outcome assessment, demonstrated unclear risk of bias for most studies, as only 6 [29, 31, 34, 50, 52, 53] and 3 [29, 30, 52] studies provided information on these aspects in domains 6 and 7, respectively. Domain 8, referring to attrition bias, showed a low risk of bias for nearly all studies [17–37, 39–51, 53, 54], with the exception of two studies that presented a high risk of bias [38, 52]. Domain 9, addressing reporting bias, showed a low risk of bias for all studies [17–54]. In domain 10, other sources of bias, only three studies showed a high risk of bias [37, 38, 52], while the majority presented a low risk [17–36, 39–51, 53, 54].
The risk of bias for each study was qualitatively assessed by individually observing each item, without applying different weights to them, and the data were entered into a pre-formulated table that summarized the results and generated Fig. 2.Fig. 2. Risk of bias based on SYRCLE´s ROB tool represented by Risk-of-bias VISualization (Robvis)
Results of Individual Studies
The majority of studies demonstrated that EVs are promising in controlling bone resorption-related diseases in vivo [17–32, 34–52, 54]. Also, some of these studies evaluated the influence of EVs in promoting bone regeneration [18–25, 27–31, 34–37, 39–41, 43, 49–54], collaborating with the resolution of bone loss. Some studies have shown that functionalized or modified EVs are more effective for both actions compared to un-modified EVs [17, 18, 21, 23, 25, 32, 35, 36, 39, 41, 42, 45, 46, 48, 51].
Lee et al. [44], in 2021, verified similar effects to control of bone resorption when adipose tissue-derived stem cells (ASCs) or ASCs-EVs were used for therapy to osteoporosis. Luo et al. [53], in 2019, demonstrated EVs extracted from bone marrow stem cells promoted bone regeneration, but they did not influence bone resorption. Pan et al. [33], in 2023, using EVs extracted from osteoclasts, verified the absence of control of bone resorption and regeneration. And, Wang et al. [27], in 2024, verified senescent osteocytes were not able to control bone resorption in senile osteoporosis, and Lu et al. [31], in 2023, demonstrated that EVs extracted in high glucose conditions were not efficient to control bone resorption and promote bone regeneration.
Considering the secondary outcome of studies demonstrated the efficacy of EVs to control bone resorption, it was observed the significant reduction of TRAP [22, 24–30, 35, 37, 39, 44, 45, 49, 52, 54], RANKL [25–27, 35, 38, 39, 43–46], pro-inflammatory cytokines [19, 22, 24, 29, 32, 34, 47, 48, 50, 54], as well as inhibition or controlling on osteoclasts [19, 21, 26, 27, 30–32, 34–41, 43, 44, 46–49, 52, 54], M1-type macrophages [29, 32, 34, 45], and Th17 [35].
The molecular mechanisms involved in bone regeneration that collaborate with the boost of bone mass and control of bone resorption highlight the increase of molecules and growth factors essential to osteoblast differentiation. Thus, the presence of factor of runt-related transcription 2 (Runx2) [25, 28–30, 35, 42, 49–51, 53], alkaline phosphatase (ALP) [25, 27, 29, 30, 37, 40, 42, 50, 52, 53], osteocalcin (OCN) [17, 18, 23, 25, 27–29, 34, 37, 40, 42, 43, 51, 52], osteopontin (OPN) [18, 29, 34, 35, 52], type 1 collagen (COL-1) [17, 25, 30, 34, 49], Osterix [21, 25, 30]. Besides these aspects, osteoblast differentiation also influenced positively bone health in some studies [20, 27, 30, 35, 42, 49–51, 53]. An increase of OPG [41–44], regulatory T cell [35], Interleukin-10 (IL-10) [19, 29, 32, 47], and M2-type macrophage [18, 26, 32, 34, 45] is important to the regulation of bone resorption. It is also important to highlight the presence of vascular endothelial growth factor (VEGF), essential for angiogenic differentiation and consequent bone regeneration was noted by Kim et al. [20], and Wang et al. [27].
It was possible to highlight that the BMSCs-EVs were able to reduce RANKL [39, 46], TRAP [39], and pro-inflammatory cytokine (IL-1) [19], thereby controlling bone resorption [19, 39, 41, 46]. These studies also demonstrated bone regeneration [39, 41, 53], restored the normality of OPG levels [41], and showed increased level of IL-10, an immunosuppressive cytokine [19]. The UC-MSCs-EVs and ASCs decreased the number of osteoclasts [22, 44, 47] and levels of TRAP [22, 44, 49], inflammatory cytokines [47], and RANKL [44], as well as increased the number of osteoblasts [49], and level of COL1 [49], Runx2 [49], and OPG [44].
Also, the EVs obtained from macrophages controlled the bone resorption and increased bone regeneration [21, 23, 29], due decrease in osteoclast activity [21, 29, 35, 37] and improvement of Runx2 [29, 35, 37], OCN [17, 23, 29, 35], OPN [29, 37], Osterix [21], COL-1 [17] e IL-10 [29, 37] levels. The EVs isolated from skeletal muscle enhanced OCN [28], Runx2 [28, 30], Osterix [30], COL-1 [30], and osteoblasts [30], and controlled the bone resorption [28, 30].
For the other origin cells used for extraction and included in this review [18, 20, 24–27, 31–34, 36, 38, 40, 42, 43, 45, 48, 50–52, 54], despite the beneficial effects obtained in most studies, the absence of multiple studies for specific type of cells using the same EV origin prevented a comparative analysis of findings. Details about the primary and secondary outcomes were summarized in Tables 2, 3 and 4.
Besides that, the studies demonstrated that vesicles extracted from identical origin cells, even if utilized in different dosages, were efficient and promoted similar effects and outcomes, suggesting the potential to use lower doses of EVs for the treatment of diseases related to bone resorption.
Likewise, some authors have also evaluated the biodistribution of vesicles in different organs [23–25, 27, 35, 41, 42, 44, 52–54]. The main organs evaluated were bones [24, 25, 27, 35, 41, 42, 44, 52–54], more specifically the femur [35, 41, 42, 52, 54] and the tibia [42, 52], as well as liver [23–25, 35, 41, 42, 44, 52, 54], kidneys [23–25, 35, 41, 42, 44, 52, 54], spleen [23, 25, 35, 41, 42, 44, 52, 54], lungs [23, 25, 35, 41, 42, 44, 52, 54], heart [23, 25, 35, 42, 44, 52, 54], and lynphonods [24]; Wang et al. [27], Lee et al. [44], and Luo et al. [53], 2019 did not specify the bone evaluated; Cui et al. [42], and Chen et al. [52] even evaluated the brain. Overall, the liver showed the highest concentration of vesicles [35, 41, 42, 44, 52, 54], but some studies also reported significant vesicle signals originating from the bone [27, 35, 44, 52, 53], particularly from the trabecular surface [52]. Cytotoxicity was also assessed, revealing the absence of toxicity when using EVs [29, 30, 34, 43, 45–47].
Discussion
The PICO question of the present systematic review "Would extracellular vesicle therapy be efficient for treating bone resorption?" was interpreted as having an affirmative answer, since the majority of studies have confirmed successful control bone resorption after using EVs, regardless of the disease responsible for this problem [17–32, 34–52, 54].
Despite five articles showing data indicating the absence of superiority of EVs therapy, the affirmative above remains possible. One study demonstrated similar and promising results when EVs or stem cells were used for treating bone resorption [44]. Due to difficulties in accessing stem cells and their possible immunological limitations, such as immune rejection in genetically different individuals [56], and the availability and low risk of immune rejection when using EVs [26–32, 34–43, 45–52, 54], making EV therapy a preferred choice.
EVs removed from senescent osteocytes [27] or extracted in high glucose conditions [31] were inefficient in controlling bone resorption. In contrast, EVs from young osteocytes or extracted in normal glucose conditions demonstrated effectiveness in this regard. Therefore, the condition of the EVs requires to be carefully assessed for clinical applications [27, 31]. Although Luo et al. [53] demonstrated EVs did not interfere in bone resorption, these vesicles stimulate bone regeneration, which benefits the imbalance of bone remodeling.
The unique study reporting an unsatisfactory outcome for controlling bone resorption was that of Pan et al. [33], in which EVs were derived from osteoclasts. Since EVs have the similar biological functions of their origin cells [9–11, 13], the ineffectiveness may be justified considering the intrinsic bone-resorptive function of osteoclasts [1–6]. Therefore, the appropriate choice of the cell of origin for EV extraction is essential for future clinical approaches.
The satisfactory effect of EVs can be explained when the molecular mechanisms are analyzed carefully. In the present review, it was observed EVs were able to decrease levels of TRAP [22, 24–30, 35, 37, 39, 44, 45, 49, 52, 54], RANKL [25–27, 35, 38, 39, 43–46], pro-inflammatory cytokines [19, 22, 24, 29, 32, 34, 47, 48, 50, 54], as well as the inhibition and control of osteoclasts [19, 21,2627, 30–32, 34–41, 43–44, 46–49, 52, 54], M1-type macrophages [29, 32, 34, 45], and Th17 [35]. These molecules and cells participate in bone resorption [1–6, 9] and their control or inhibition improves the therapy for bone resorption [1–6, 9]. In addition, the EVs increased levels of OPG [41–44], regulatory T cell [35], IL-10 [19, 29, 32, 47], and M2-type macrophage [18, 26, 32, 34, 45], collaborating with control bone resorption [3, 5–7].
In addition to these aspects, the EVs still promoted bone regeneration which enhances the quality and the quantity of bone [17, 18, 20, 21, 23–25, 27–31, 34–37, 39–41, 43, 49–54]. This characteristic collaborates with the balance of bone loss generated by different diseases linked to bone resorption.
Although the included studies are heterogeneous in terms of origin cells, doses, administration routes, and disease models, we addressed this variability by grouping the studies according to the disease investigated, as shown in Tables 2, 3, and 4. This approach allowed the identification of patterns that appear to be more consistent within each specific disease context. As a result, it can be observed that 14 [20, 25, 27, 28, 30, 35, 42, 44, 46–49, 52–54] of the 18 studies related to osteoporosis prioritized administration by intravenous route, with the effect being dose-dependent when different doses were compared within the same study [20, 44]. Regarding periodontitis, all studies applied EVs directly to the site of the bone defect resulting from the resorptive process [17–19, 21–24, 26, 31, 34, 37, 38, 45, 50]; due to the similarity of the outcomes, it is believed that in this case, lower doses may be more appropriate. It should be emphasized that these interpretations represent preliminary inferences, serving as initial indications rather than definitive conclusions. Future studies are needed to validate and strengthen these disease-specific observations.
Concerning the origin cell, new approaches are needed to determine the ideal one. Since the majority of studies demonstrated positive results for the control of bone resorption, considering accessibility, ease of obtaining, and ethical aspects is essential. Thus, bone marrow stem cells [19, 41, 46, 53] and macrophages [17, 21, 25, 37] can be prioritized in future studies.
A limitation of the present review is linked to the impossibility of the performance of meta-analysis. The meta-analysis was not conducted due to insufficient data. The necessary data for this analysis were published through graphs and images in the included studies in the present review. Thus, the precise collection of the means and standard deviations to control and treated groups to carry out the meta-analysis was impossible. The authors of published studies were contacted at three different times by email, however only three decided to furnish the requested information.
Another limitation was related to the risk of bias, as in several domains the risk was classified as unclear due to the lack of information regarding whether the assessed procedures were performed. This highlights the need for caution when extrapolating these findings to clinical trials and reinforces the necessity of additional studies before such translation can be considered. Additionally, the heterogeneity of origin cells, posology and experimental models represented another limitation, and as previously discussed, future studies focusing on addressing these aspects are required to enhance translational potential and support the development of future clinical applications.
Furthermore, considering the eligibility criteria, 24 articles were excluded after full-text reading, as shown in Table 1. The eligibility criteria addressed aspects included in the objectives of this systematic review. Therefore, in the absence of any essential data required to answer the proposed questions, the study was excluded and the reason for exclusion was justified.
Differences can be observed between animal and human studies, such as the use of certain vehicles like PBS [18–21, 23, 25–27, 34, 35, 37, 41–43, 45, 49, 54], the employment of simulated models to induce disease in animals [17–54], and some types of analysis [17–54]. Moreover, it is important to emphasize that early studies in animals are essential for testing initial hypotheses and assessing potential therapeutic effects prior to use in humans. Therefore, the EV-based therapy under investigation appears comparable across animal and human models, supporting a cautious but meaningful interpretation of the preclinical findings [57].
Despite these limitations, considering the descriptive data in this review, associated with the number of animals and statistical analysis of individual articles, as well as overall scientific quality of evidence, it is possible to infer the potential use of EVs for treating bone resorption-related diseases. Early-phase or Phase I/II translational studies that first assess safety, dosing, and feasibility in humans must be conducted to confirm the results obtained in this systematic review.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Wang ZX, Lin X, Cao J, Liu YW, Luo ZW, Rao SS, Wang Q, Wang YY, Chen CY, Zhu GQ, Li FX, Tan YJ, Hu Y, Yin H, Li YY, He ZH, Liu ZZ, Yuan LQ, Zhou Y, Wang ZG, Xie H (2024) Young osteocyte-derived extracellular vesicles facilitate osteogenesis by transferring tropomyosin-1. J Nanobiotechnology. 2 10.1186/s 12951-024-02367-x.10.1186/s 12951-024-02367-x PMC 1104687738664789 · doi ↗ · pubmed ↗
- 2Xing Z, Guo L, Li S, Huang W, Su J, Chen X, Li Y, Zhang J. Skeletal muscle-derived exosomes prevent osteoporosis by promoting osteogenesis. Life Sci. 2024 Nov 15;357:123079. 10.1016/j.lfs.2024.123079. Epub 2024 Sep 24. PMID: 39326580.10.1016/j.lfs.2024.12307939326580 · doi ↗ · pubmed ↗