Transcranial magnetic stimulation in cocaine use disorder and the risk of seizure: a review of the evidence
Caesar G. Imperio, Eric Parmon, Vaughn R. Steele, Derek Blevins, Rebecca Chalme, Jonathan M. Wai, Kathleen Brady, Markus Heilig, Colleen A. Hanlon, Frances R. Levin, Diana Martinez

TL;DR
This paper reviews the risk of seizures when using transcranial magnetic stimulation (TMS) for treating cocaine use disorder and suggests ways to reduce that risk.
Contribution
The paper provides a risk assessment framework and mitigation strategies for seizure risks in TMS treatment for cocaine use disorder.
Findings
Seizures are more likely linked to recent cocaine use than TMS treatment itself.
High-dose cocaine use requiring urgent care is most associated with seizure risk.
Adjusting TMS parameters and monitoring motor thresholds can help mitigate seizure risks.
Abstract
Transcranial magnetic stimulation (TMS) has emerged as a promising intervention for cocaine use disorder (CUD). However, a key concern when employing TMS in CUD is the potential risk of seizures. Our goal was to assess seizure risk in individuals with CUD undergoing TMS and to propose parameters that could mitigate it. Our review of the literature indicated that seizures are primarily associated with high-dose cocaine use necessitating urgent medical care – and that the risk is likely low outside of this setting. Thus, to mitigate potential seizure risks during TMS sessions, we suggest an assessment of recent cocaine use and an evaluation for cocaine toxicity. Additionally, rechecking motor threshold levels during treatment with TMS is recommended, especially if patterns of cocaine use change. Previous studies of TMS in CUD reported on two seizures that were linked to recent cocaine use…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
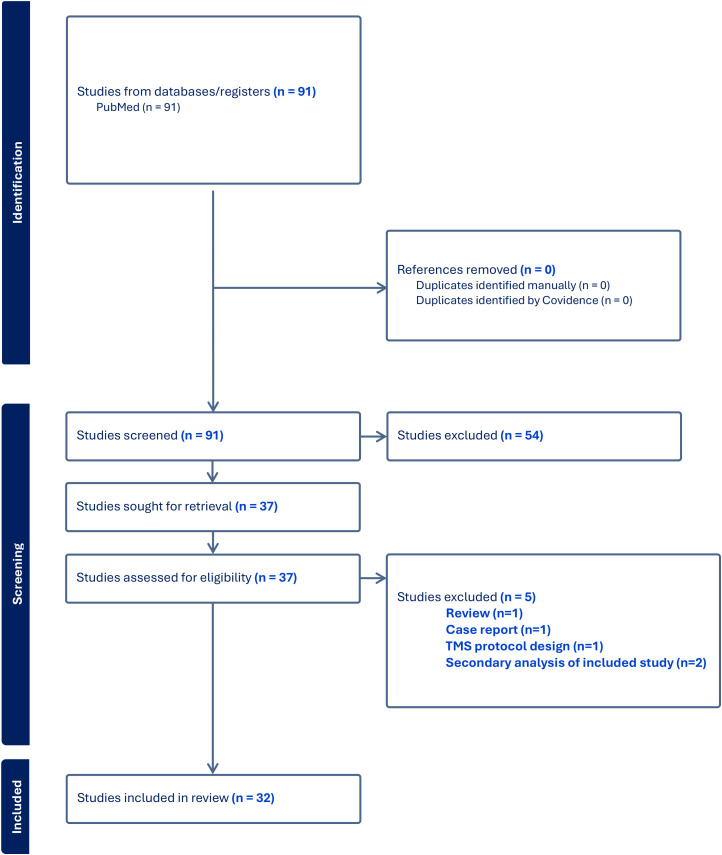 Figure 1
Figure 1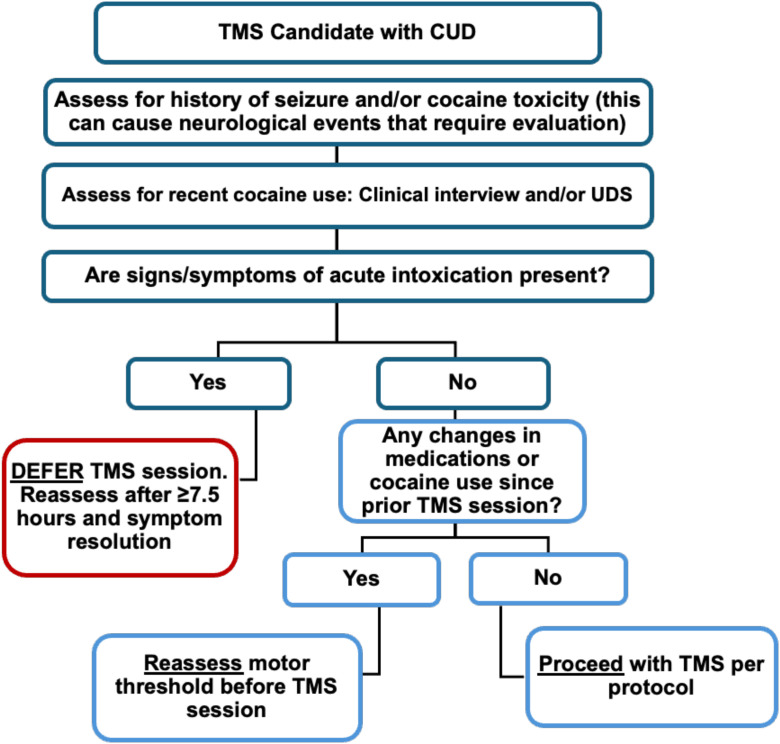 Figure 2
Figure 2| Study | Participant population and reported seizure |
|---|---|
| Case-control study | |
| Ng et al., 1990 ( | Cases: hospitalized patients with first episode non-febrile seizure (n=308); Controls: hospitalized patients without seizure (n=294). Subjects interviewed about drug use (cocaine, amphetamines, cannabis, LSD, PCP, heroin, methadone, methaqualone). AOR = 1.05 for any cocaine use; AOR = 1.69 for cocaine use within 1 day of admission |
| Retrospective record reviews of hospital charts | |
| Lowenstein et al., 1987 ( | ED visits + hospital admissions of patients with cocaine use as the primary problem (n=1275). Seizure reported in 2.3% of patients. |
| Choy-Kong et al., 1989 ( | Hospital admissions of patients where diagnosis cocaine ‘use or abuse’ in record (n=283). Seizure reported in 2.8%; clear temporal association seen in 1.4%. |
| Derlet et al., 1989 ( | ED visits of patients presenting with drug use or overdose (n=137 attributed to cocaine). Seizure reported in 8.8% of cocaine exposed. |
| Pascual-Leone et al., 1990 ( | ED visits of patients with medical complications caused by cocaine intoxication (n=474). Seizure reported in 16.9% among patients with a history of seizure; among patients with no seizure history, rate was 7.9% |
| Brody et al., 1990 ( | ED visits of patients using cocaine, including use with other drugs (n=216). Seizure reported in 4.3%. |
| Dhuna et al., 1991 ( | Hospital admissions for non-traumatic complications of cocaine use (obstetric complications excluded) (n=945). Seizure reported in 10.4% (18.4% women, 6.2% men). |
| Rich et al., 1991 ( | ED visits where “cocaine” was reported by patients within 72 hours or detected on toxicologic screen (n=144). Seizure reported in 4.2%. |
| Anta et al., 1998 ( | ED visits directly related to patients’ cocaine use (injuries or obstetric/gynecologic, pediatrics excluded) (n=233). Seizure reported in 5.3%. |
| Blaho et al., 2000 ( | ED visits with suspected or confirmed cocaine use, independent of chief complaint (n=111). Seizure reported in 3%. |
| Sanjurjo et al., 2006 ( | ED visits where cocaine use occurred within “the previous hours” by patients (n=745). Seizure reported in 1.9%. Data from Spain. |
| Sopena et al., 2008 ( | Patients hospitalized due to complications of cocaine use (n=177). Seizure reported in 6.2%. Data from Spain. |
| Bodmer et al., 2014 ( | ED visits due to acute cocaine-related medical problems (n=165). Seizure reported in 4% of cocaine-only exposed; 1% with use of additional substances (mostly alcohol, tobacco, cannabis). Data from Switzerland. |
| Miro et al., 2019 ( | ED visits involving cocaine use (n= 3002 total cases; n=2600 for powder + n=376 for smoked cocaine). Seizure reported in 4.5% in the powder cocaine and 5% in the smoked cocaine. Data from 14 European countries. |
| Glidden et al., 2022 ( | Hospitalized patients receiving medical toxicology consultation (n=380 cocaine only; n=343 cocaine + opioid). Seizure reported in 8.1% of cocaine-only; 0% of cocaine and opioids. |
| Darke et al., 2023 ( | Cocaine-related deaths from 2000-2021 (n=26 for cocaine only related deaths with witness observation). Seizure reported in 26.9% fatal cocaine only toxicity. Data from Australia. |
| Miro et al., 2025 ( | ED visits for acute cocaine toxicity where cocaine was the only drug used except for alcohol (n=9365). Seizure reported in 4.8%. Data from 33 countries. |
| Study | Study design, TMS parameters, assessment of cocaine use |
|---|---|
| Politi et al., 2008 ( | Open label (n=36); L DLPFC (10 daily sessions: 15 Hz at 100% MT, presumed fig 8). Detoxification treatment prior to TMS, craving measured but not cocaine use. No serious adverse events. |
| Bolloni et al., 2016 ( | Double blind randomized (n=10 active; n=8 sham); bilateral PFC (3 sessions/week: 10 Hz at 100% resting MT over 4 weeks; H1 coil). Cocaine hair analysis at baseline and 1,3,6 months. Four subjects were excluded due to high cocaine use at screening. No serious adverse events (but headache reported). |
| Rapinesi et al., 2016 ( | Open label (n=7); L (preferential) DLPFC (12 sessions: 15 Hz at 100% MT over 1 month; H1 coil). Craving but not cocaine use obtained. No serious adverse events. |
| Terraneo et al., 2016 ( | Open label randomized (n=16 active; n=16 pharmacological control); L DLPFC (1 session/day:15 Hz at 90% resting MT for 5 days then 1 session/week x 3 weeks, fig 8). UDS obtained at each TMS visit, no report of sessions being held for a positive result. No serious adverse events. |
| Kearney-Ramos et al., 2018 ( | Open label (n=49); frontal pole (TMS during brain scan, single pulses at 100% resting MT every 10–12 seconds on 1 day; fig 8). Cocaine use self-report obtained; whether TMS session held (or not) for recent use not specified. No serious adverse events. |
| Cardullo et al., 2019 ( | Case series of CUD with gambling (n=7); L DLPFC (twice daily sessions for 5 days: 15 Hz at 100% MT followed by twice daily sessions once/week for 8 weeks, fig 8). UDS and self-report obtained as clinical outcome; whether TMS session held (or not) for recent use not specified. No serious adverse events. |
| Pettorruso et al., 2019 ( | Open label (n=20); L DLPFC (5 sessions/week: 15 Hz at 100% resting MT for 2 weeks, then TMS twice/day for 2 weeks, fig 8). UDS and self-report obtained; whether TMS session held (or not) for recent use not specified. No serious adverse events. |
| Sanna et al., 2019 ( | Open label randomized (n=25 iTBS; n=22–15 Hz TMS); bilateral PFC (iTBS: 5 Hz at 80% MT; 20 sessions in 4 weeks; 15 Hz TMS: 15 Hz at resting 100% MT; 20 sessions in 4 weeks; H4). UDS obtained at baseline and twice weekly during TMS sessions; whether TMS session held (or not) for recent use not specified. No serious adverse events. |
| Steele et al., 2019 ( | Open label (n=19); L DLPFC (3 iTBS sessions per day: 50 Hz at 100% resting MT for 10 days over 2 weeks). UDS obtained, 73% of TMS sessions performed with positive UDS, fig 8). Neurological event of uncertain etiology (right-hand supination/pronation at the wrist) 10–15 min following iTBS. |
| Gomez Perez et al., 2020 ( | Retrospective observational study (n=87); L DLPFC (2 sessions/day at 15 Hz with 100% resting MT for 5 days; then 2 sessions/week for 12 weeks, butterfly). UDS, self-report, and reports from significant others were obtained at each TMS visit; whether TMS session held (or not) for recent use not specified. No serious adverse events. |
| Madeo et al., 2020 ( | Retrospective observational study (n=284); L DLPFC (2 x day sessions:15 Hz at 100% MT for 5 days, then 2 x day sessions once weekly x 12 weeks, fig 8). UDS, self-report, and reports from significant others at each TMS visit. No report of sessions held due to use. Seizure in 1 participant - not close to the recent session. Additional events: headache, dizziness, anxiety, hypomania, nausea, irritability, dental/scalp discomfort. |
| Cardullo et al., 2021 ( | Retrospective, open label ADHD/CUD (n=22) and CUD-only (n=208); L DLPFC (twice/day of 15 Hz at 100% MT for 5 days then twice daily sessions once a week for 12 weeks, fig 8). UDS, self-report, or reports from significant others obtained at each visit; whether TMS session held (or not) for recent use not specified. No serious adverse events. |
| Garza-Villarreal et al., 2021 ( | Double-blind, randomized (n=24 active; n=20 sham); L DLPFC (twice daily sessions of 5Hz at 100% MT for 10 days, then two sessions per week for up to 6 months, fig 8). UDS obtained at baseline, 2 weeks, 3 months, and 6 months; whether TMS session held (or not) for recent use not specified. No serious adverse events. |
| Lolli et al., 2021 ( | Double-blind, randomized (n=32 active; n=30 sham); L DLPFC (15 sessions: 15 Hz at 100% resting MT over 3 weeks, fig 8). UDS obtained at baseline and twice weekly; whether TMS session held (or not) for recent use not specified. One participant in sham group experienced mild and transient paresthesia. No serious adverse events. |
| Martinotti et al., 2022 ( | Double-blind, randomized (n=42 active; n=38 sham) L DLPFC (20 sessions over 4 weeks:15 Hz at 100% resting MT for 5 days then 2 sessions/week for 12 weeks, butterfly). UDS and self-report obtained at each TMS visit. No reports of TMS being held for recent use. No serious adverse events in treatment phase, 1 participant in maintenance phase had seizure-like activity after cocaine use. |
| Sanna et al., 2022 ( | Retrospective analysis (n=89); bilateral PFC and insula (20 sessions over 4 weeks at 50 Hz with 100% resting MT, H4). UDS obtained twice weekly, self-report weekly; whether TMS session held (or not) for recent use not specified. No serious adverse events (headache, dizziness, sleepiness, and insomnia reported). |
| Angeles-Valdez et al., 2024 ( | Double-blind randomized clinical trial (n=30 active; n=24 sham); L DLPFC (Acute phase: 2 sessions/day at 5 Hz 100% MT for 10 days; open label maintenance phase: 2 sessions per week 5 Hz,100% MT, fig 8). UDS was performed prior to fMRI scans; whether TMS session held (or not) for recent use not specified. No serious adverse events. |
| Cardullo et al., 2024 ( | Open label (n=40); L DLPFC (2 sessions/day at 15 Hz with 100% resting MT for 5 days, fig 8) UDS, self-report, and reports from significant others were obtained; whether TMS session held (or not) for recent use not specified. No serious adverse events |
| De Rossi et al., 2026 ( | Open label (n=33); L DLPFC. (2 sessions/day at 15 Hz with 100% resting MT for 5 days; then 2 sessions/week for 3 months; then as needed sessions depending on clinical need, butterfly). UDS, self-report, and reports from significant others were obtained; whether TMS session held (or not) for recent use not specified. No serious adverse events. |
| Casula et al., 2025 ( | Randomized clinical trial (n=19 active; n=23 sham); L DLPFC (1session/day for 2 weeks at 10 Hz with 90% MT, fig 8). UDS not obtained; whether TMS session held (or not) for recent use not specified. No serious adverse events. |
| Gomez Perez et al., 2025 ( | Retrospective observational study (n=1011); L DLPFC (2 sessions/day at 15 Hz with 100% resting MT for 5 days; then 2 sessions/week for 12 weeks; then discretion of the treatment team could add iTBS to L DLPFC targeting anti-cocaine craving or low-frequent TMS over the presupplementary motor area for perseverative cocaine use; butterfly). UDS and self-report were obtained; whether TMS session held (or not) for recent use not specified. Reports of headache, scalp discomfort, along with 2 cases of hypomania, 2 cases of psychosis, 1 migraine, and 1 left upper limb paresthesia that resolved after stoppage of TMS. |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTranscranial Magnetic Stimulation Studies · Neuroethics, Human Enhancement, Biomedical Innovations · Electroconvulsive Therapy Studies
Introduction
Cocaine use disorder (CUD) can lead to impaired social and vocational functioning, lost opportunities, and the increased risk of morbidity and mortality (1, 2). However, effective pharmacologic treatment remains elusive (3, 4). Clinical trials have searched for medications that could help patients reach remission, but no clear options have emerged. While studies suggest that some pharmacotherapy (such as long-acting stimulants or combined medications) may help some patients, there remains a need for therapeutic options (1, 2, 5).
Research shows that transcranial magnetic stimulation (TMS) may serve as a treatment for CUD by reducing craving and cocaine use (6, 7). Although a pivotal trial has yet to be published, early studies using heterogeneous approaches – including imaging, open-label trials, retrospective record reviews, and randomized controlled trials – have shown promise for this refractory disorder.
Seizure is a rare but concerning potential adverse event associated with TMS (8, 9). While the incidence is low, there is a concern of increased seizure risk among individuals with CUD based on data showing that cocaine exposure itself can cause a seizure (10–26).
Given the promise of TMS for CUD, our goal was to characterize the risk of seizure and to identify methods to reduce it. We began with a review of seizures and cocaine use, followed by an analysis of studies where cocaine was safely administered in laboratories. We then reviewed clinical trials of TMS in CUD, with a focus on reports of seizures in this population. From this analysis, we provide suggestions that can be used to mitigate the seizure risk on TMS in CUD.
Cocaine use and the risk of seizure
In the 1980s, cocaine production and consumption increased across the globe. Clinical researchers soon identified the association between cocaine exposure and seizure, which is now a recognized potential adverse event. We reviewed the literature on this topic, starting with a systematic review by Sordo et al. (27), which identified 11 cross-sectional studies (10–20) and one case-control study (21) reporting on seizure prevalence among individuals using cocaine. We then replicated the search of Sordo et al., to identify additional studies published since their 2013 review by searching Medline, EMBASE, and PsycINFO using the terms “cocaine, cocaine-related disorders, cocaethylene, and seizures” and excluded unverified reports of seizure.
This returned a total of 17 studies (Table 1), which show that seizure was seen in 1% to 27% of individuals who had used cocaine recently (intravenous, smoked, insufflated, or oral) (10–26). As shown in Table 1, all studies included patients receiving acute medical care in emergency departments or hospitals due to cocaine use alone or due to illness where cocaine use was a contributing factor. The highest prevalence (27%) was reported in a retrospective analysis of cocaine-related deaths, suggesting that the greatest risk of seizure may be during a fatal overdose (23).
We then reviewed studies that included self-reports of seizure by cocaine users, which was not observed by medical personnel (28–32). The prevalence rates varied from 0.9% to 18.1%. This large range can be partly attributed to seizures being described as “fits, convulsions, fainting, and loss of consciousness” – such that these reports included non-seizure events. Nonetheless, these studies also indicated that seizures occurred in the setting of recent, high dose cocaine use that caused symptoms of physical and/or mental distress. Thius, this finding is similar to the studies with confirmed seizures witnessed by medical personnel.
Taken together, this research indicates that individuals who use cocaine and consequently require acute medical attention are at risk of seizure. We found no reports of increased seizure in persons with CUD outside of this setting. While the lack of data cannot provide definitive evidence, it is remarkable that there are no reports of increased rates of seizure associated with CUD itself.
With respect to TMS, this data suggests that seizure risk would be elevated following recent cocaine use, especially at toxic doses that induce illness – and could be low outside of this setting. In the next sections, we review methods that can be used to assess recent use and toxic doses.
Evaluating recent cocaine use
A urine drug screen (UDS) is a reliable method for determining recent cocaine use. However, it detects benzoylecgonine (an inactive metabolite), which can persist in the urine for 2–4 days, well after cocaine has cleared the plasma (33). Additionally, although uncommon, a UDS can return a false negative result where cocaine is in the blood but benzoylecgonine has yet to appear in urine (34, 35). This can occur when cocaine use is very recent (within about 2 hours) before the metabolite is detectable (35, 36).
We sought to identify clinical parameters that could assess recent use – instead of a UDS or in addition to this test. For this goal, we reviewed studies where cocaine was taken by participants in a laboratory setting under close monitoring. This provided information on the signs and symptoms of recent cocaine use, which correlate with its pharmacokinetic profile.
The half-life of cocaine in the plasma is 45 to 90 minutes following smoked, intranasal, or intravenous administration (37–40). Once five half-lives have passed (or about 7.5 hours), plasma levels become undetectable (37–40). The subjective effects of cocaine intoxication include feeling high, alert, self-confident, social, talkative, anxious, irritable, and ‘on edge’ (41–46). These symptoms peak within about 5 minutes and resolve within about 30–45 minutes following a single dose (40, 45, 47–50). Repeated dosing extends the subjective effects of cocaine longer, beyond 100 minutes or more (41, 51, 52).
Increases in vital signs are another sign of cocaine intoxication. Studies show that cocaine increases heart rate by about 20–40 beats per minute and increases blood pressure (systolic and diastolic) by about 10–30 mmHg over baseline (41–46). These remain elevated for 2 to 3 hours following smoked or intravenous cocaine use (41, 44, 53).
Thus, the signs and symptoms of cocaine intoxication can be used to evaluate individuals for recent use, including subjective effects and vital signs. However, an additional approach is to establish a collaborative, non-judgmental dialogue with individuals about their patterns of cocaine use This could include the estimated dosage, timing, and route of administration – as well as a discussion of the potential risk of TMS in the setting of recent cocaine exposure.
Assessing toxic cocaine use
The difference between a euphorigenic dose of cocaine (which produces a desired effect) and a toxic dose (which causes distress) can be miscalculated, even among individuals with regular cocaine use. A toxic dose, also called an overdose, leads to symptoms of physical and mental distress and requires a medical assessment. Thus, in addition to recent use, evaluating this parameter would improve safety.
The signs and symptoms of cocaine toxicity have been divided into three stages of increasing severity (54). Stage 1 includes central nervous system effects (headache, nausea, mydriasis, vertigo, twitching, pseudo-hallucinations, and pre-convulsive movements); changes in vital signs (hypertension, tachycardia, tachypnea, hyperthermia, ectopic beats); and psychiatric symptoms (paranoia, euphoria, confusion, aggression, agitation, emotional lability, restlessness). Stage 2 consists of additional symptoms of greater severity: encephalopathy, seizures, increased deep tendon reflexes, incontinence, arrhythmias, peripheral cyanosis, gasping, apnea, and irregular breathing (54). Stage 3 includes symptoms that can be life-threatening: areflexia, coma, fixed and dilated pupils, loss of vital function, hypotension, ventricular fibrillation, cardiac arrest, respiratory failure, cyanosis, and agonal breathing (54).
In reviewing the symptoms of cocaine toxicity, it is key to recognize that some individuals will experience stage 1 symptoms without progressing to stage 2 or 3 – and that not all symptoms listed above are required to meet criteria for cocaine overdose. Furthermore, some individuals might not have sought medical care despite having severe symptoms.
With respect to TMS, an evaluation of cocaine overdose should include both recent and past episodes. A recent episode could indicate that a clinical evaluation is needed to rule out ongoing illness, such as neurological or cardiac events. A past event may not be exclusionary for TMS, but should be assessed, since an overdose could have included neurological events, like ischemic stroke and intracerebral or subarachnoid hemorrhage (55, 56).
TMS studies on CUD
We reviewed studies of TMS in CUD, in order to evaluate two parameters: 1) whether an assessment of recent use was included prior to the delivery of TMS; and 2) whether seizure was reported. In May 2025, we searched PubMed using the term “cocaine and transcranial magnetic stimulation,” which returned 91 studies (Figure 1). Inclusion criteria consisted of investigational studies examining the use of TMS for CUD that were published in English. Publications were excluded if they were literature reviews, conference abstracts, commentaries, secondary analysis of already included data, or non-human investigations, leaving 32 studies for further review.
PRISMA flow diagram of study selection. PRISMA diagram detailing database search, number of abstracts screened, full texts retrieved, and number of studies included.
Of these, 11 studies required abstinence or a urine drug screen negative for cocaine prior to the delivery of TMS sessions (57–67). Notably, these studies used outcomes that were not affected by the requirement of abstinence, such as imaging, measures of craving, or cocaine self-administration. There were no reports of seizures.
We then reviewed publications that did not specifically require abstinence, in order to determine whether recent cocaine use was assessed prior to the delivery of TMS. This resulted in 21 studies (Table 2). As shown in Table 2, these publications assessed cocaine use with heterogeneous methods, including UDS, hair analysis, self-report, and reports from significant others (68–88). However, only five (of the 21) studies clearly reported that recent use was evaluated prior to the delivery of TMS (70, 74, 75, 81, 85). The remaining studies did not specify whether cocaine use was assessed prior to each TMS session. Future studies that clarify this parameter would benefit the field of TMS research.
Among the studies of TMS in CUD, we found two reports of a seizure (75, 85). Madeo et al. (75) performed an observational study (n = 248) and reported that one participant experienced a seizure following cocaine use. The authors reported that 66 days had passed since the first TMS session, but the precise time between the most recent TMS session and the seizure was not published (although the authors stated that TMS had not recently been delivered). Martinotti et al. (85) performed a randomized, sham-controlled study (n = 80) and reported a seizure-like episode in one participant in the active TMS group. The event occurred following intravenous cocaine use, but the proximity to the TMS session was not reported. Moreover, both studies were limited in their description of seizure-like activity and appeared to rely on self-report (75, 85).
Steele et al. (74) reported a transient neurological event of uncertain etiology in an open-label pilot study (n = 19) where a participant experienced rhythmic right-hand supination and pronation at the wrist. The event began 10–15 minutes following TMS and persisted for about 3 minutes (74, 89). The episode resolved within 1 hour, and no further TMS sessions were administered. Steele et al. (90) also reported a new-onset tremor in a participant with CUD who received sham intermittent theta burst stimulation.
Taken together, this data suggests that seizure is uncommon in studies using TMS in CUD. This finding is consistent with a recent meta-analysis, which reported a seizure prevalence of 2.32 per thousand participants receiving active TMS for individuals with CUD (91). However, clinical studies that describe the temporal association between cocaine use and the delivery of TMS, and the time between TMS and serious adverse events, such as seizure, would further demonstrate the safety of this intervention.
CUD and motor threshold
Previous TMS studies have shown that participants with CUD have a higher motor threshold compared to controls (63, 66, 92, 93). Hanlon et al. (93) investigated the mechanism behind this using intracortical facilitation and functional MRI. The findings suggest that cocaine use is associated with reduced cortical facilitation, which may increase motor threshold and alter motor cortex BOLD signal, potentially mediated by glutamate and GABA signaling (93).
It remains unknown whether the elevated motor threshold seen in CUD varies with the amount of use or the duration of abstinence. Some TMS in CUD studies measured motor threshold prior to each session (59, 61, 74), which would address this potential variability. Alternatively, a recent study obtained a UDS prior to each TMS session, and the motor threshold was reassessed in the event of a newly positive result (NCT04907357). Either of these approaches would be expected to accommodate possible changes in cortical excitability.
Discussion
Pharmacological treatment for CUD has been elusive, despite numerous clinical trials (3, 4). Additional treatments are needed, and research investigating TMS for CUD shows that this intervention reduces craving and cocaine use (6, 7, 94). Although pivotal clinical trials are still needed, there is a strong rationale for pursuing TMS as a therapy.
Given the potential benefit of TMS, there is a need to characterize the risk of seizure in CUD (95). To this end, we reviewed the research on cocaine exposure and seizure risk, which showed that patients requiring urgent medical care due to recent, high dose cocaine use were at risk for seizure. Outside of this scenario, there are no published reports of increased seizure rates among individuals with CUD. This suggests that CUD itself does not increase seizure risk – although this absence of documentation is not definitive.
With respect to TMS, the following steps, outlined in Figure 2, would be expected to mitigate seizure risk:
Decision tree for administering TMS in individuals with CUD.
An assessment of cocaine use prior to sessions
This can be done with a urine drug screen, although it would remain positive for 2–4 days, well after cocaine has cleared the plasma (33). An additional method is to establish a collaborative dialogue with individuals regarding their patterns of use, combined with observation for signs and symptoms of acute intoxication. In this approach, TMS sessions could be timed to avoid cocaine plasma levels above negligible amounts. The half-life of cocaine is about 90 minutes, meaning that plasma levels should be cleared by about 7.5 hours.
An evaluation of cocaine toxicity
Individuals who use cocaine generally avoid toxic doses, but miscalculations can occur. A toxic dose (also called overdose) can include seizure in addition to other serious adverse events. An assessment of overdose should include both recent and past events, which may require a clinical evaluation. Additionally, psychoeducation on the risks associated with overdose, and the need for medical care, can serve as a form of harm reduction.
A motor threshold assessment
Previous studies on TMS indicate that seizure risk is mitigated using a careful assessment of motor threshold, especially in the setting of medication changes (8, 9). Thus, checking motor threshold at each TMS session or rechecking when the individuals’ pattern of cocaine use changes would also be expected to reduce risk.
Overall, TMS has been investigated as a potential treatment for CUD, with promising results and few serious adverse events. Among these publications, there have been two reports of seizures, although both cases occurred following cocaine use – and not in temporal proximity to the TMS session (although the precise time frame was not reported). At the same time, it is notable that most studies did not clearly report whether recent cocaine use was assessed prior to the TMS sessions. This omission limits our ability to interpret the temporal relationship between recent cocaine use and TMS outcomes. Incorporating systematic assessment of recent cocaine use prior to TMS delivery in future studies would benefit the field and allow further documentation of the safety of TMS in CUD.
As with any treatment study, all participants, including CUD participants, should have a clinical evaluation that is specific to the population and study needs. The information provided here, while generally applicable in the design of future TMS studies, cannot replace clinical oversight and monitoring, which is important for research using TMS for any indication.
Limitations
Our review of the literature has several limitations. As noted, there is substantial heterogeneity across studies in TMS protocols, approaches to assessing recent cocaine use, and methods for reporting seizure-like activity. These discrepancies hinder our ability to understand how TMS, cocaine use, and seizure events are related in terms of timing and sequence. In addition, a recent meta-analysis (91) that included several of the cocaine studies discussed here found a high risk of bias in these studies.
Furthermore, our publication did not review the efficacy of TMS for CUD, nor the occurrence of adverse events other than seizure. For these topics, we refer the reader to systematic reviews of TMS in SUD (6, 96) and substance use and to Blyth et al. (91), who reviewed the overall risk of adverse events in this patient population.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kampman KM . The treatment of cocaine use disorder. Sci Adv. (2019) 5:eaax 1532. doi: 10.1126/sciadv.aax 1532, PMID: 31663022 PMC 6795516 · doi ↗ · pubmed ↗
- 2Brandt L Chao T Comer SD Levin FR . How can we optimally channel therapeutic optimism to advance pharmacotherapy research on cocaine use disorder? Addiction. (2021) 116:715–7. doi: 10.1111/add.15423, PMID: 33538068 · doi ↗ · pubmed ↗
- 3Substance Abuse and Mental Health Services Administration. 2021 National Survey on Drug Use and Health (NSDUH): annual national report. Rockville (MD): Center for Behavioral Health Statistics and Quality (2023).
- 4Schwartz EK Wolkowicz NR Aquino JPD Mac Lean RR Sofuoglu M . Cocaine use disorder (CUD): current clinical perspectives. Subst Abus Rehabil. (2022) 13:25–46. doi: 10.2147/sar.s 337338, PMID: 36093428 PMC 9451050 · doi ↗ · pubmed ↗
- 5Goldstein RZ . Continuous theta burst stimulation of the medial prefrontal cortex reduces drug cue reactivity with a potential for improving outpatient treatment outcomes in cocaine use disorder. Biol Psychiatry: Cognit Neurosci Neuroimaging. (2025) 10:557–9. doi: 10.1016/j.bpsc.2025.04.007, PMID: 40483007 · doi ↗ · pubmed ↗
- 6Amerio A Baccino C Breda GS Cortesi D Spiezio V Magnani L . Effects of transcranial magnetic stimulation on cocaine addiction: A systematic review of randomized controlled trials. Psychiatry Res. (2023) 329:115491. doi: 10.1016/j.psychres.2023.115491, PMID: 37783092 · doi ↗ · pubmed ↗
- 7Harmelech T Hanlon CA Tendler A . Transcranial magnetic stimulation as a tool to promote smoking cessation and decrease drug and alcohol use. Brain Sci. (2023) 13:1072. doi: 10.3390/brainsci 13071072, PMID: 37509004 PMC 10377606 · doi ↗ · pubmed ↗
- 8Stultz DJ Osburn S Burns T Pawlowska-Wajswol S Walton R . Transcranial magnetic stimulation (TMS) safety with respect to seizures: A literature review. Neuropsychiatr Dis Treat. (2020) 16:2989–3000. doi: 10.2147/ndt.s 276635, PMID: 33324060 PMC 7732158 · doi ↗ · pubmed ↗