Fatal hemangioblastoma: a case report and literature review
Wenjie Zhang, Xu Zhang, Chang Ge, Cao Yang, Rui Li, Jingxuan Xu

TL;DR
A rare case of fatal hemangioblastoma is reported, highlighting the poor prognosis of ruptured tumors and the need for better treatment guidelines.
Contribution
A comprehensive case report and literature review of 30 patients with fatal or ruptured hemangioblastomas, providing insights into clinical features and outcomes.
Findings
Spontaneous rupture of hemangioblastomas is rare and associated with high mortality despite surgical intervention.
Among 30 patients, 23% died within one month, with causes including hemorrhage, tumor progression, and respiratory failure.
Most tumors originated in the cerebellum, and surgical resection was the primary treatment, though prognosis remained poor in ruptured cases.
Abstract
Hemangioblastoma (HB) is a benign tumor of the central nervous system (CNS), typically associated with a favorable prognosis following aggressive surgical resection. Spontaneous rupture and bleeding of these tumors are exceptionally rare, with only a small number of fatal cases reported. The rarity of such cases has impeded reliable epidemiological studies, underscoring the need to investigate the risk factors associated with HB-related mortality. A patient presented with a 12-hour history of headache and rapidly became comatose approximately 30 minutes after admission. Neuroimaging revealed a large, solitary tumor located in the cerebellar vermis, medulla, and C1 segment of the spinal cord, with spontaneous rupture resulting in severe intracerebral hemorrhage. Despite emergency resuscitation and subsequent surgical resection, the patient unfortunately succumbed to their condition.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
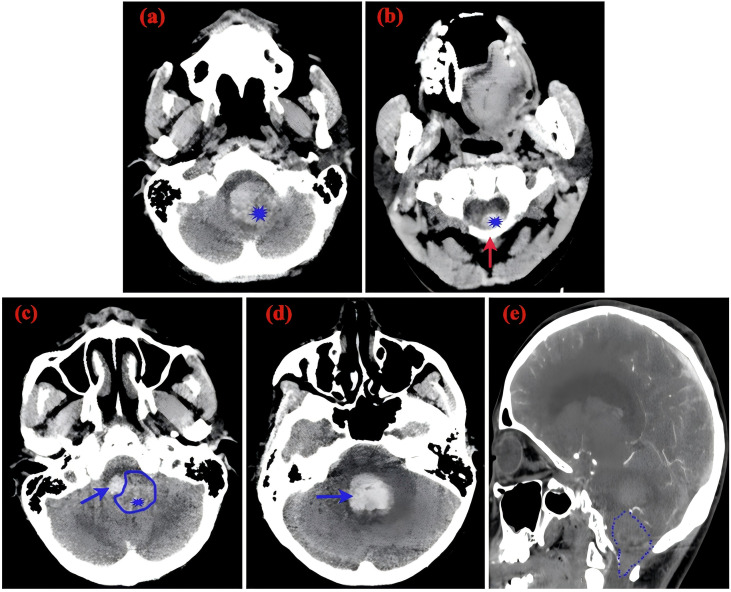 Figure 1
Figure 1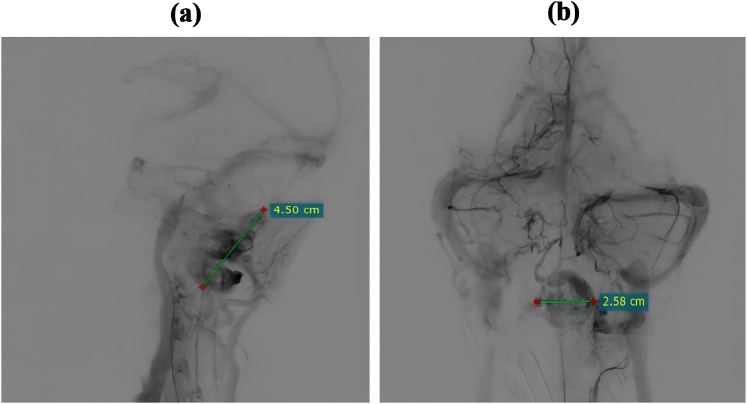 Figure 2
Figure 2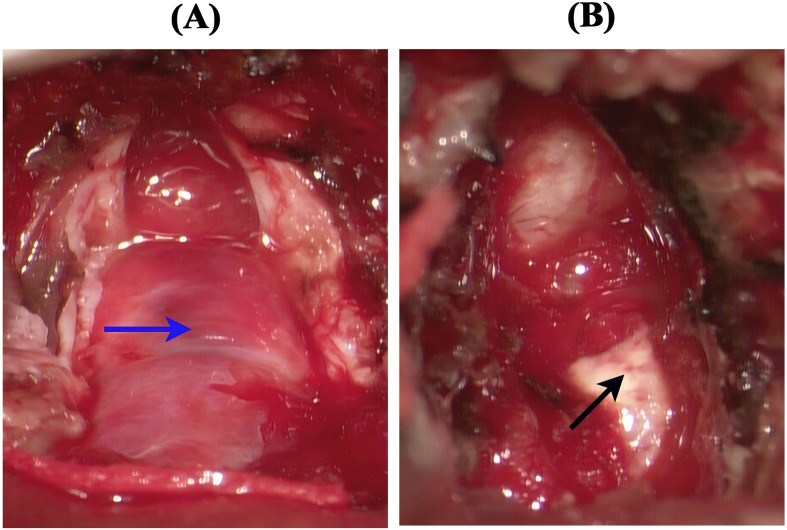 Figure 3
Figure 3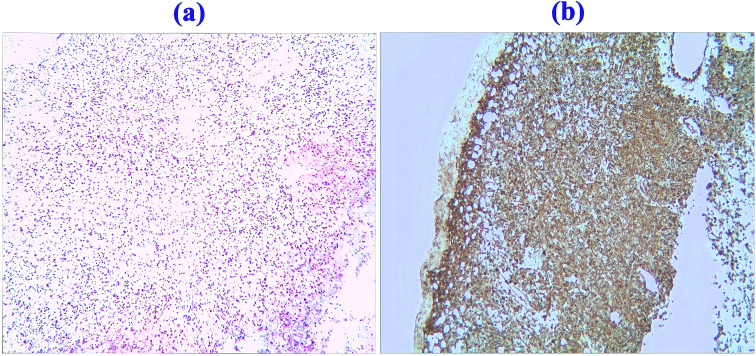 Figure 4
Figure 4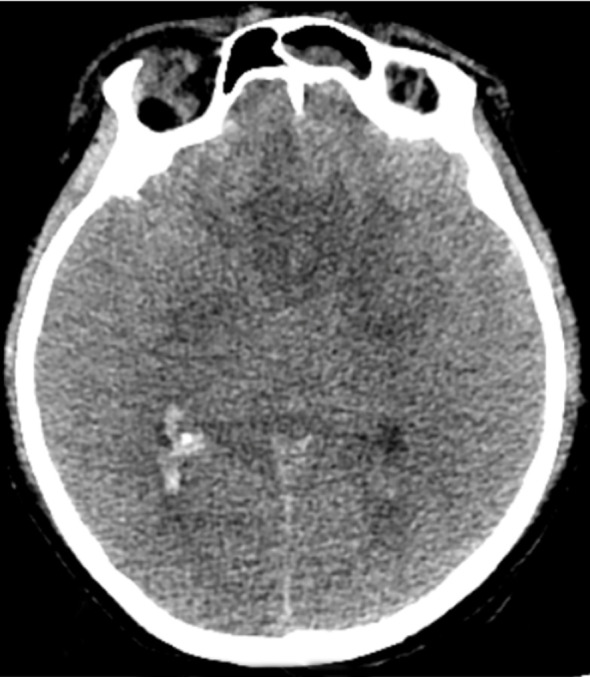 Figure 5
Figure 5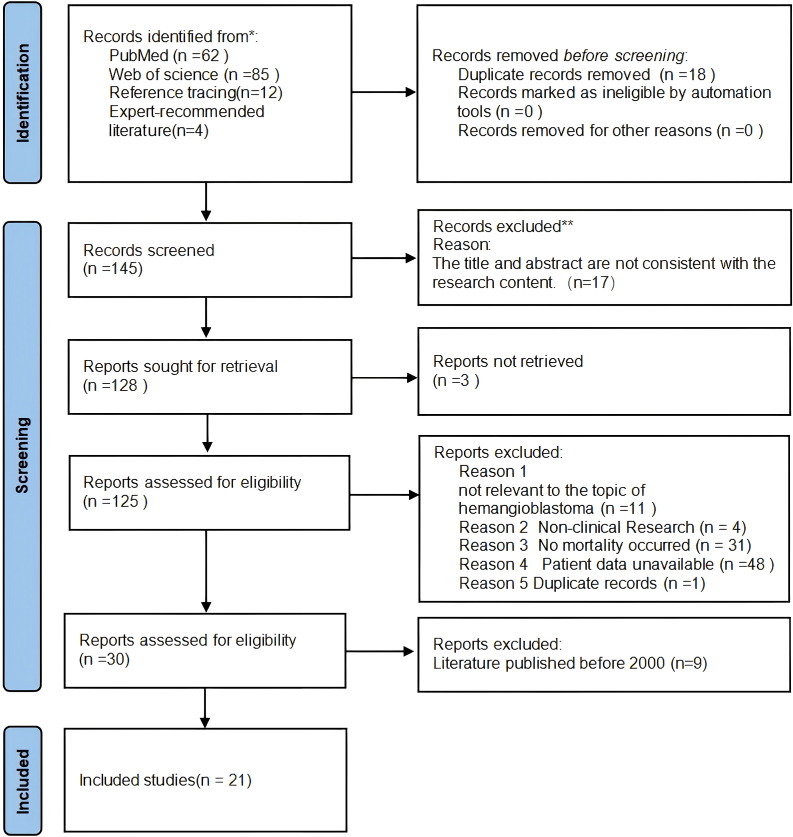 Figure 6
Figure 6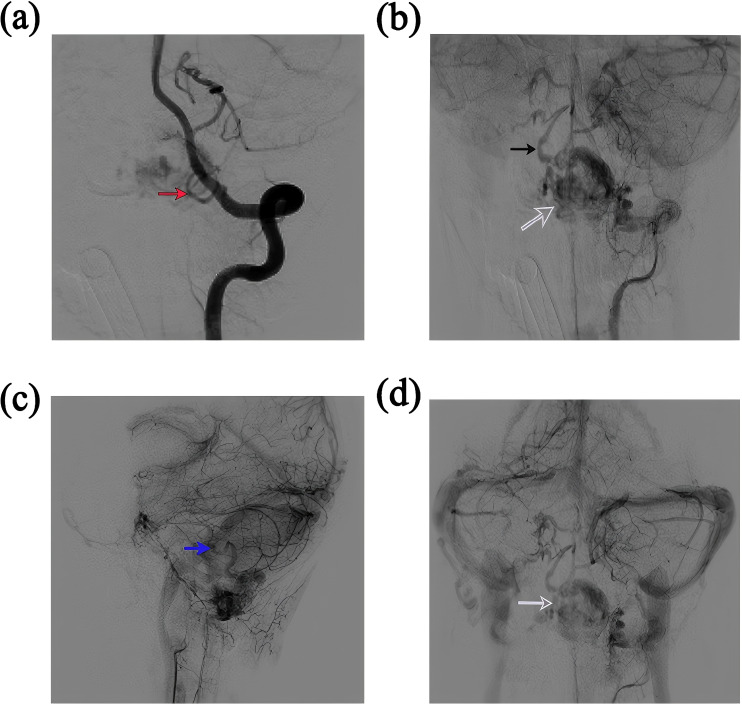 Figure 7
Figure 7| Time | DOI/PMID | Sex | DA | RT (mons) | OS (mons) | M D(cm) | IS | RS | TT | Surgery | VHL | Bleeding | MC | Embolization | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2010 | 10.1007/s00701-010-0669-7 | M | 49 | N/A | 4 | 2.8 | CPA | CPA, Peri-Luschka foramen | Solid | No | No | Yes | Cerebral herniation secondary to post-radiation hemorrhage | No | |
| 2025 | 10.1016/j.esmoop.2025.105109 | M | 58 | N/A | 9 days(Post-recurrence therapy) | 5.2 | N/A | Cerebellum | Cystic-solid | No | Yes | Yes | Belzutifan-associated spontaneous hemorrhage | No | |
| 2023 | 10.1200/PO.23.00066 | F | 62 | N/A | 3 days(Post-recurrence therapy) | 1.6 | Medulla | Medulla | Solid | No | Yes | Yes | Belzutifan-associated spontaneous hemorrhage | N/A | |
| 2016 | 10.1007/s00701-016-2798-0 | F | 46 | 68 | 106 | N/A | Cerebellum | Multiple subarachnoid space,spinal cord | Solid | Total | No | No | Death | No | |
| M | 53 | 136 | 215 | N/A | Cerebellum | Interpeduncular,prepontine,CPA,cisterma magna | Cystic | Total | No | No | Death | No | |||
| M | 51 | 64 | 69 | N/A | Cerebellum | Pons,midbrain,insula,parietal lobe | N/A | Total | No | No | Death | No | |||
| 2002 | 10.3171/jns.2002.96.4.0775 | F | 43 | 84 | 102 | 3.3 | Cerebellum | Brain stem, spinal cord | Solid | Total | No | No | Respiratory failure, Aspergillus sepsis | No | |
| F | 47 | 72 | 120 | N/A | Cerebellum | Cerebellum,medulla,spinal cord | Cystic | Total | No | No | Respiratory failure | No | |||
| M | 34 | 84 | 121 | 3.5 | Cerebellum | CPA、Cerebrospinal fluid, cervical, thoracic, and lumbar spinal cord, optic chiasm | Cystic-solid | Total | No | No | Stem tumor progression | No | |||
| M | 41 | 96 | 120 | 3.5 | Cerebellum | Occipital lobe, Brain stem, Cervicobulbar junction, Dorsal aspect of the entire spinal cord | Cystic-solid | Total | No | No | Sudden death | No | |||
| 2003 | PMID: 12699568 | M | 30 | 252 | 264 | N/A | Cerebellum | Whole spine | N/A | Total | Yes | No | Death | No | |
| 2005 | 10.1007/s11060-004-2244-7 | F | 29 | 264 | N/A | N/A | Cerebellum | Brain stem,cerebellum,spinal cord | N/A | Total | No | No | Death | No | |
| 2006 | 10.1016/j.clineuro.2006.12.007 | F | 23 | 624 | N/A | 2.4 | Foramen, magnum | Brain stem,spinal cord | Solid | Total | No | No | Death | No | |
| 2007 | 10.1007/s11060-006-9321-z | F | 17 | 168 | 171 | N/A | Cerebellum | Whole spine | N/A | Total | Yes | No | Death | No | |
| 2009 | 10.3346/jkms.2009.24.4.755 | M | 41 | 120 | 132 | N/A | Cerebellum | Suprasellar,medulla,spinal cord | Solid | Total | No | No | Death | No | |
| 2008 | 10.3174/ajnr.A1360 | M | 43 | 144 | 168 | N/A | Cerebellum | Suprasellar cistern,whole spine | N/A | Total | Yes | No | |||
| 2011 | 10.1007/s00701-010-0827-y | F | 46 | 132 | N/A | N/A | Cerebellum | Hypothalamus,temporal lobes,stem, whole spine, | solid | Total | Yes | No | Death | No | |
| 2011 | 10.1007/s11060-010-0244-3 | F | 28 | 84 | 156 | N/A | Cerebellum | Cerebellum,brain stem,whole spine | N/A | Total | Yes | No | Death | No | |
| 2012 | 10.1007/s11060-011-0752-9 | M | 31 | 60 | 75 | N/A | Cerebellum | Cerebellum,brain stem,multiple spine | N/A | Total | No | No | Death | No | |
| 2014 | 10.4103/2152-7806.142321 | F | 45 | 91 | 120 | N/A | Cerebellum | Multiple brain and spine | Cystic | Total | No | No | Death | No | |
| 2007 | 10.3171/jns.2007.106.6.994 | M | 49 | No | Intraoperative | N/A | CPA | No | N/A | No | N/A | Post-embolization hemorrhage | Coma,Death | Yes | |
| F | 25 | No | one hour postoperative | N/A | Vermis | No | N/A | No | N/A | Post-embolization hemorrhage | Coma,Death | Yes | |||
| M | 71 | No | Intraoperative | N/A | CPA | No | N/A | Total | N/A | Post-embolization hemorrhage | Coma,surgery,Death | Yes | |||
| 2010 | 10.1136/jnis.2010.004366 | M | N/A | No | Within several days postoperative | 3.8 | Cerebellum | No | N/A | Subtotal Resection | No | No | Intracranial abscess,Hydrocephalus,re-hemorrhage | Yes | |
| 2024 | 10.3390/curroncol31070293 | M | 56 | No | 16 | 2 | Cerebellum | No | Cystic-solid | Total | No | No | Recurrence | N/A | |
| 2009 | 10.1007/s10143-008-0166-0 | M | 26 | No | 3 days | 2.0 | Pons, medulla | No | N/A | Total | yes | No | Intracranial abscess, Pneumonia | No | |
| M | 56 | No | 3 | 2.0 | Medulla | No | N/A | Total | No | No | Pneumonia | No | |||
| 2010 | 10.1007/s00701-010-0668-8 | M | 33 | No | 16 | 3.5 | Medulla | No | Solid | Total | No | No | Pneumonia,Death | No | |
| 2016 | 10.1007/s00701-016-2834-0 | M | 33 | No | 7 days | N/A | Medulla | No | Solid | Total | Yes | No | Pneumonia | No | |
| 2025 | Present Case | F | 21 | No | 8 days | 4.5 | Vermis, medulla, Atlas | No | Solid | Total | No | Yes | Intracranial abscess,Stem compression | No | |
| Clinical characteristics | n (%), mean ± SD, max/min/mdn |
|---|---|
| Sex | |
| M | 18 (60.00%) |
| F | 12 (40.00%) |
| DA | 40.94 ± 13.44 (Years) |
| OS | |
| ≤1 month | 7 (23.33%) |
| >1 month | 18 (60.00%) |
| N/A | 5 (17.00%) |
| RT | |
| Recurrence | 17 (%) 146.06 ± 136.64 (Mons.) |
| N/A | 3 (10.00%) |
| No recurrence | 10 (33.33%) |
| MD | |
| Available | 13 (43.33%) Max:5.2cm, Min:1.6cm, Midian:3.3cm |
| N/A | 17 (56.67%) |
| IS | |
| Cerebellum | 18 (60%) |
| Medulla | 8 (26.67) |
| Multiple | 3 (10%) |
| N/A | 1 (3.33%) |
| TT | |
| Cystic | 3 (10%) |
| Solid | 10 (33.33%) |
| Cystic-Solid | 4 (13.33%) |
| N/A | 13 (43.33%) |
| Surgery | |
| Yes | Total: 24 (80.00%), Subtotal: 2 (6.67%) |
| No | 5 (17.00%) |
| VHL | |
| Yes | 9 (30.00%) |
| No | 18 (60.00%) |
| N/A | 3 (10.00%) |
| Bleeding | |
| Yes | 7 (23.33%) |
| No | 23 (76.67%) |
| MC | |
| Hemorrhage | 6 (20%) |
| Tumor progression | 3 (10%) |
| Infection | 6 (20%) |
| Respiratory failure | 1 (3.33%) |
| Unspecified mortality | 14 (46.67%) |
| Embolization | |
| Yes | 4 (13.33%) |
| No | 23 (76.67%) |
| N/A | 3 (10.00%) |
- —Xinjiang Medical University10.13039/501100004880
- —Science and Technology Department of Xinjiang Uygur Autonomous Region10.13039/100016079
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer, Hypoxia, and Metabolism · Glioma Diagnosis and Treatment · Neuroblastoma Research and Treatments
Introduction
Hemangioblastomas (HB) are benign, highly vascularized neoplasms comprising approximately 2% of intracranial tumors and 3–4% of spinal tumors (1). These lesions predominantly localize to the cerebellum (2), though spinal cord and brainstem involvement occurs in 5% of cases (3). Approximately 20–30% of HB are associated with von Hippel-Lindau (VHL) disease (4). Clinical manifestations primarily stem from secondary intracranial hypertension, encompassing symptoms such as headache, nausea, vomiting, ataxia, and dizziness (3). Intracranial hemangioblastomas generally exhibit favorable prognosis following complete surgical resection, with 5-year survival rates surpassing 90% (5) (6). Hemorrhagic complications are infrequent in this pathology (7). A comprehensive literature review conducted in 2010 identified only 44 documented instances of spontaneous hemorrhage (4). Subsequent research by Ene et al. (2015) reported 53 cases and estimated the incidence of central nervous system hemangioblastomas at 1.41 per million person-years (6) (8). The annual hemorrhage rate among affected individuals is approximately 0.24% (9). Despite this, spontaneous bleeding events remain sparsely documented in global literature.
Current understanding suggests that tumors smaller than 1.5 cm (in size) carry almost no risk of spontaneous bleeding, whereas those larger than 2.3 cm present a significantly increased risk of spontaneous bleeding (7) (9). Ongoing debates persist regarding the mortality rate and prognostic outcomes following spontaneous hemorrhage, as limited short-term mortality data are available (10) (11) (12) (13). Epidemiological studies face challenges due to the scarcity of reported spontaneous hemorrhage cases (8). The present study reports a rare fatal case of spontaneous hemangioblastoma rupture-associated hemorrhage. The tumor exhibited a large, solid morphology, posteriorly situated near the left medulla oblongata. It extended superiorly to the cerebellar vermis and inferiorly to the C1 spinal cord segment. To our knowledge, no prior literature has described a life-threatening event resulting from foramen magnum region hemangioblastoma spontaneous rupture.
Case report
A 21-year-old female patient presented with an abrupt onset of headache, accompanied by nausea and severe projectile vomiting, persisting for 12 hours. Initial assessment revealed preserved consciousness, but neurological examination documented a progressive exacerbation of headache intensity. Admission to the hospital occurred 12 hours after symptom onset, followed by rapid progression to deep coma within 30 minutes. Physical examination disclosed bilateral 2-mm fixed pupils with sluggish light reflex. Cranial computed tomography (CT) demonstrated a solid tumor and bleeding in the foramen magnum region, with the lesion predominantly on the left side, compressing the medulla. Hemorrhagic extension into the ventricular system and subarachnoid space resulted in fourth ventricle cast formation (Figure 1). The clinical diagnosis was established as: occupying lesion in the foramen magnum region; acute obstructive hydrocephalus. Emergency bilateral lateral ventricular puncture and external drainage were performed, with an intraoperative intracranial pressure (ICP) measurement of 200 mm H_2_O. Subsequent digital subtraction angiography (DSA) showed the upper margin extending to the lower third of the cerebellar hemisphere, and the lower margin reaching the inferior border of the posterior arch of the atlas. The lesion measured 4.5 x 2.58 cm in the sagittal plane (Figure 2). Emergency resection of the lesion was performed by opening the foramen magnum, exposing the posterior arch of the atlas, and conducting a posterior fossa decompressive craniectomy. During surgery, a firm, gray-yellow, and red solid tumor was observed, with clear boundaries and a surrounding capsule. The tumor was completely resected in segments (Figure 3). Pathological examination showed a highly vascularized tumor with abundant capillaries and a rich population of stromal cells. The stromal cells exhibited an epithelial-like appearance with transparent and microvacuolated cytoplasm. Immunohistochemistry revealed positivity for Vimentin (+), CD31 (+), CD34 (+), and focal positivity for NSE (+) (Figure 4).
CT scans(a) Slightly hyperdense mass in the cerebellar vermis, indicated by the blue asterisk (), accompanied by a hyperdense hemorrhagic lesion on the right. (b) Slightly hyperdense mass extending inferiorly to the cervical spinal cord at the C1 segment (blue asterisk); the red arrow denotes the lamina of the atlas (C1). (c) Slightly hyperdense mass in the cerebellar vermis (blue asterisk) and hemorrhage within the fourth ventricle (blue arrow). (d) Blue arrow denotes hemorrhage within the fourth ventricle. (e) Sagittal view of original CTA image demonstrating the size and location of the tumor (highlighted in blue).*
Digital subtraction angiography (DSA) prior to craniotomy. (a) Lateral view demonstrating the abnormal vascular lesion with a maximum diameter of 4.5 cm. (b) Anteroposterior (AP) view illustrating the transverse diameter of the vascular lesion measuring 2.58 cm.
Surgical images. (A) The blue arrow indicates a solid mass with an intact capsule, bright red in color and containing abundant blood vessels. (B) The black arrow indicates the removal of the tumor from the dorsal side of the medulla, exposing the normal brainstem tissue below.
Pathological specimens and immunohistochemistry. (a) Histological section stained with hematoxylin and eosin (H&E, ×100) illustrating hemangioblastoma (HB), characterized by abundant stromal cells with clear, vacuolated cytoplasm, focal nuclear atypia, and intermixed capillary vessels. (b) Immunohistochemical staining showing positivity for Vimentin (+), CD31 (+), CD34 (+), S-100 (+), focal positivity for NSE (+), and a low proliferative index (Ki-67 ~1%). Negative staining was observed for CD68 (−), GFAP (−), Olig-2 (−), Synaptophysin (−), and Chromogranin A (CgA, −). These findings support the diagnosis of hemangioblastoma.
Timeline of disease progression
The patient remained in a persistent state of profound coma (Glasgow Coma Scale [GCS] score of 3), accompanied by the absence of spontaneous ventilation, which necessitated endotracheal intubation and mechanical ventilation. On the second postoperative day, serum sodium levels showed a continuous upward trend, reaching a peak of 173.5 mmol/L (normal range: 135–145 mmol/L), requiring bedside hemodialysis. At 04:00 on the third postoperative day, bilateral mydriasis (left: 5 mm, right: 4 mm), accompanied by absent pupillary light reflexes, was observed. Cranial computed tomography (CT) revealed significant cerebral edema with obliteration of sulcal contours and multiple hypodense lesions affecting both cerebral hemispheres and the genu of the corpus callosum. These imaging findings were consistent with cerebral ischemia. Despite the administration of nimodipine, mannitol, edaravone, dipyridamole, and corticosteroids—after the patient's family refused surgical craniectomy decompression—transcranial Doppler (TCD) revealed elevated blood flow velocities in the bilateral middle cerebral, anterior cerebral, and vertebrobasilar arteries, indicating vasospasm. The patient’s clinical deterioration continued, with repeated serum analyses showing neuronal-specific enolase levels exceeding 300 ng/mL (reference range: 0–16.3 ng/mL). Ultimately, the patient succumbed to terminal cerebral edema (Figure 5), refractory intracranial hypertension, and brainstem dysfunction on the eighth postoperative day, with electroencephalography confirming brain death. An autopsy was not performed due to the family's refusal.
The patient suddenly developed cerebral vasospasm on the second day after surgery, with obvious swelling of the entire brain, disappearance of the cerebral sulci, and low-density lesions in both cerebral hemispheres and the knee of the corpus callosum, indicating cerebral ischemia.
Literature review
Materials and methods
This descriptive systematic review aims to systematically collect and summarize published case reports and case series on fatal outcomes of hemangioblastoma (HB).
Eligibility criteria
Literature published after 2000 on fatal hemangioblastoma (HB) patients was reviewed, providing comprehensive information. Studies were considered for inclusion only if they reported data on at least three specific criteria. These included tumor size, age at initial diagnosis, overall survival (and cause of death), primary or recurrence site, the Von Hippel-Lindau (VHL) disease status, and the primary treatment modality (surgery or embolization).
Search strategy and data extraction
A literature search was conducted using the Web of Science and PubMed databases (without time restrictions). The search terms used were "Hemangioblastoma/mortality", "Hemangioblastoma", "fatal", and "death", with English as the selected language. Animal studies were excluded. Two independent reviewers assessed the article content. Some information was obtained by contacting the authors, and any data that could not be retrieved were recorded as N/A. Data collection and quality assessment were independently performed by two reviewers. In the event of disagreements between the reviewers, an additional reviewer was consulted to reach a consensus. Reference lists were also manually searched to identify additional citations. To ensure comprehensive literature coverage, we also included articles recommended by field experts. The study identification process was conducted in accordance with the PRISMA guidelines, with details provided in the flow diagram (Figure 6).
Literature selection flowchart. .
Two reviewers independently assessed the methodological quality of the included studies. As the literature consisted primarily of case reports and small case series, we employed the Joanna Briggs Institute (JBI) critical appraisal checklist for case reports. Disagreements during quality assessment were resolved by consensus or by consultation with a third reviewer. The extracted data and quality assessment results for all included studies are summarized in Table 1.
Diagnosis
Upon definitive diagnosis of a hemangioblastoma, exclusion of von Hippel-Lindau (VHL) disease is imperative, irrespective of patient age, personal/family history, or tumor localization. Compared to sporadic cases, VHL disease demonstrates heightened familial aggregation and recurrence rates, thereby necessitating rigorous long-term surveillance. This autosomal dominant disorder arises from germline mutations in the VHL tumor suppressor gene (3p25.3) (3) (14), manifesting as multisystem neoplasms, including central nervous system and retinal hemangioblastomas, renal cell carcinoma, bilateral pheochromocytomas, pancreatic cysts, endolymphatic schwannomas, and epididymal cystadenomas (15) (16) (17). In the present case, the tumor exhibited solitary morphology, with no documented family history, absence of retinal vascular anomalies, and unremarkable bilateral renal ultrasonography. Consequently, this lesion was classified as an isolated hemangioblastoma.
However, the final diagnosis of VHL requires genetic testing for germline mutations in peripheral blood leukocytes, with diagnostic accuracy approaching 100% (7, 18). Genetic testing was not performed as consent from the patient's family was not obtained. Recent studies have confirmed that VHL gene alterations can be detected in the vast majority of hemangioblastomas, establishing VHL inactivation as a central event in tumor formation (19). Biallelic VHL inactivation in hemangioblastomas leads to insufficient degradation of HIF-1α, resulting in inappropriate transcription of effectors expressed under hypoxic conditions, such as vascular endothelial growth factor (VEGF) or platelet-derived growth factor B (PDGF-B), which promote tumor formation (20).
Research indicates that approximately 50% of individuals with a mutation in the VHL gene will develop a hemangioblastoma within 30 years of diagnosis (3) (14). Therefore, Suh et al. recommend screening the families of all patients presenting with an isolated hemangioblastoma for VHL mutations to facilitate early identification of at-risk relatives (21).
Differential diagnosis
Hemangioblastoma must be differentiated from the following conditions: meningioma, metastatic tumors, cystic astrocytoma, medulloblastoma, ependymoma, perivascular tumors, and arteriovenous malformations (AVM). The peak incidence occurs between the ages of 20 and 40. Hemangioblastomas are typically solitary but may be multiple. They can present as large cysts with small nodules or as solid masses. Imaging of hemangioblastomas typically shows large cysts with small nodules, significant and uniform enhancement of the wall nodules, and tortuous blood vessels inside or around the tumor. Pathology reveals a tumor containing numerous foamy cells and abundant capillaries, with positive staining for inhibin α, CD31, and CD34.
Pathology
Hemangioblastoma comprises two principal components: vascular elements and stromal cells (22). The histological appearance of hemangioblastomas is consistent across various anatomical sites within the central nervous system (16) (23) (24) (25). Figure 4 shows a dense reticulum network interspersed between the stromal cells and vascular channels. This histological pattern is characteristic of hemangioblastoma (2) (3) (15) (23). In histopathological practice, hemangioblastoma should be differentiated from angiomatous meningioma and metastatic renal cell carcinoma. Useful immunohistochemical markers for this differentiation include positive staining for S100, inhibin-α, and neuron-specific enolase (NSE), and typically negative staining for epithelial markers (2) (3) (15) (25).
Imaging examination
MRI is invaluable for localizing tumors, characterizing their histopathology, and guiding surgical planning (26) (27) (28) (29) (30) (31) (32) (33). However, the prolonged duration of MRI examinations often prevents critically ill patients from undergoing this modality. In this case, the patient was unable to undergo cranial MRI due to life-threatening cerebral hemorrhage. CT remains the first-line diagnostic tool for cerebral hemorrhage but has inferior resolution for solid tumors (29). On CT, cystic components of hemangioblastomas appear as hypodense regions, whereas solid components appear as isodense or mildly hyperdense areas (30). In our case, CT revealed hemorrhage in the medulla oblongata, cerebellar subarachnoid space, occipital cistern, bilateral ventricles, and third/fourth ventricles. Isodense shadows in the posterior medulla oblongata and cerebellar vermis suggested solid tumors. No cystic components were observed, leading to a diagnosis of solid hemangioblastoma. CTA failed to show any significant aneurysms. Digital subtraction angiography (DSA) provides high-resolution visualization of normal and pathologic vascular structures and demonstrates high sensitivity in delineating tumor nodules (3) (12). Hemangioblastomas are highly vascularized, and DSA can reveal the number and distribution of tumor vessels, including feeding arteries and draining veins (31). Such information facilitates preoperative surgical planning, thereby mitigating intraoperative hemorrhage and reducing postoperative morbidity (26) (32) (33) (34). The patient’s DSA showed tumor enhancement during the arterial phase, complete parenchymal phase tumor contour visualization, and prolonged venous phase contrast retention, revealing a tumor volume of 4.5 × 2.58 cm. Angiography further revealed a feeding artery originating from the posterior spinal artery and an abnormally dilated draining vein (Figure 7).
Angiographic characteristics of the lesion. (a) The red arrow distinctly indicates an early-phase vascular hemangioma supplied by the posterior spinal artery originating from the vertebral artery. (b) The black arrow identifies a prominent draining vein that becomes visible in the late arterial to early capillary phase, a key angiographic feature distinguishing arteriovenous malformations (AVMs) from other solid tumors. White arrows highlight the dense capillary bed characteristic of solid tumors. (c) The parenchymal phase demonstrates delayed contrast washout within the tumor tissue. (d) During the venous phase, clear staining of the solid tumor components effectively delineates the size and anatomical location of the lesion.
However, solid hemangioblastomas often mimic arteriovenous malformations (AVMs) (12), which necessitates careful differentiation. Angiographically, AVMs lack a true capillary bed, whereas hemangioblastomas display microvascular networks that resemble normal capillary beds (4) (7). Such histopathological similarities may impart improved hemodynamic tolerance to hemangioblastomas, leading to a markedly lower bleeding risk compared to AVMs (23) (35).
Surgical treatment
Surgical treatment remains the gold standard for hemangioblastoma, with complete resection critical for a favorable prognosis (26) (36) (37). The surgical strategy for resecting solid hemangioblastomas differs from that for other tumors and should follow the principles used for arteriovenous malformations. This requires first occluding the feeding arteries while preserving the draining vein until the tumor is fully removed, a technique that prevents tumor collapse or rupture (36) (38). The vascular network of a hemangioblastoma lacks contractile elements. Therefore, the tumor should be removed en bloc whenever possible to avoid uncontrollable hemorrhage (38).
For hemangioblastomas located in the brainstem, surgical resection remains the primary and most effective treatment modality. For hemorrhagic hemangioblastoma (HB), treatment should combine tumor resection with hemorrhage control (4). Mortality significantly increases with intraoperative bleeding (39). Studies have indicated that the mortality rate for surgery in the brainstem region is 25% (12). The brainstem’s complex anatomy poses unique challenges, especially in emergencies. Inadequate surgical planning may lead to brainstem injury, while unavoidable intraoperative bleeding further elevates the risk of poor outcomes (6) (36) (39). Some argue that total resection, rather than piecemeal resection, may reduce the risk of recurrence. Additionally, good prognosis can be achieved even without preoperative embolization (40).
Selective preoperative embolization of feeding arteries, followed by complete tumor excision, is the evidence-supported strategy of choice for mitigating intraoperative bleeding risks and facilitating resection of large solid tumors. Post-embolization reduction in tumor vascularity enhances the likelihood of complete removal while notably decreasing intraoperative hemorrhage (4) (38) (39). Xu demonstrated improved hemorrhage control post-embolization in solid tumors and advocated for preoperative embolization in large solid tumors (9) (38).
However, critics argue that preoperative embolization poses notable risks, including cerebellar infarction, tumor swelling, and enhanced tissue rigidity, which may complicate surgical dissection. Despite these risks, embolization remains clinically safe and effective for brainstem and spinal cord tumors (41) (42). Current literature lacks systematic evidence on the feasibility of preoperative embolization for hemangioblastomas with spontaneous hemorrhage. In our case, the patient presented with severe preoperative symptoms of tumor hemorrhage, which indicated a guarded prognosis. The clinical utility of preoperative embolization in such scenarios remains inconclusive, necessitating further investigation into its potential therapeutic role.
For asymptomatic patients or those unsuitable for craniotomy, long-term observation or radiation therapy may be considered (38) (43). A study showed that stereotactic radiosurgery (SRS) for hemangioblastomas resulted in 7 deaths due to disease progression among 98 patients. A favorable prognosis was observed in cases where the tumor volume was less than 3.2 mL (44).
Complications
Solid tumors, larger tumor sizes, and lesions near nerve roots are more likely to hemorrhage spontaneously. The primary reasons are as follows:
Solid tumors possess a denser vascular network than cystic lesions and lack cyst walls for structural support, rendering vessels fragile under conditions like hypertension or trauma (7) (45) (46).Large hemangioblastomas (those exceeding 2 cm in diameter) have fragile vasculature, which may increase the risk of spontaneous hemorrhage (9) (47).Gläsker et al. attributed the higher bleeding tendency of nerve-root-associated hemangioblastomas to their anatomical relationship with nerve roots, where compression may induce rupture (48).
The present case is consistent with the characteristics previously described. Furthermore, this case represents the largest documented solid hemangioblastoma located in the brainstem.
Subarachnoid hemorrhage secondary to rupture of a brain or spinal cord hemangioblastoma is rare (8) and must be distinguished from aneurysm-related subarachnoid hemorrhage (7). While clinically significant vasospasm frequently complicates aneurysm-related cases (49) (50) (45), this phenomenon has not been documented in hemangioblastoma-associated subarachnoid hemorrhage. Delayed cerebral ischemia resulting from cerebral vasospasm is a leading cause of morbidity and mortality following subarachnoid hemorrhage (51) (52).
The review found that patient mortality was mainly due to hemorrhage, tumor progression, pulmonary infection, and respiratory failure. Hemorrhage occurred spontaneously, following targeted drug therapy, or as a consequence of embolization.
Discussion
Hemangioblastoma is a benign central nervous system (CNS) tumor that typically has an excellent prognosis following complete surgical resection. Nevertheless, spontaneous rupture and hemorrhage, though rare, can result in severe and potentially life-threatening complications. This study investigates the clinical characteristics, therapeutic challenges, and prognostic factors associated with fatal hemangioblastoma to provide insights for improved clinical management.
The clinical and demographic characteristics of the cohort are presented in Table 2. The mean age at initial diagnosis within the study population was 40.94 years. The median maximum tumor diameter was 3.3 cm, with the majority being solid tumors (10 of 15 cases). Tumors were most commonly located in the cerebellum (18 cases) and the medulla (8 cases). Notably, the median tumor diameter in this group exceeded the previously reported threshold (2.3 cm) associated with an increased risk of bleeding, suggesting that tumor volume plays an important role in bleeding and prognosis. Furthermore, the solid composition of these tumors and their location in critical deep regions, such as the posterior fossa and brainstem, increase both treatment complexity and clinical risk.
Complete surgical resection remains the definitive treatment for hemangioblastoma (53). In our cohort, a complete resection was achieved in 80% of cases (24/30). However, surgical difficulty and perioperative risk increase substantially for ruptured tumors, particularly large, solid tumors in critical locations like the brainstem. The significant intraoperative hemorrhage in our index case highlights the characteristic hypervascularity and complex vascular architecture of these tumors. While preoperative selective arterial embolization can reduce intraoperative bleeding and facilitate resection (54), its optimal timing and safety during acute, life-threatening hemorrhage remain unclear. In our case, rapid clinical deterioration precluded embolization. Future studies should assess whether timely embolization in acute presentations can improve hemorrhage control and outcomes.
In this series, 7 patients (23%) died within one month postoperatively from causes such as re-bleeding, tumor progression, infection, and respiratory failure. In the index case, severe hypernatremia and global cerebral edema developed. This suggests the combined stress of hemorrhage and surgery can disrupt critical regulatory systems, triggering systemic complications. Furthermore, postoperative imaging and transcranial Doppler (TCD) monitoring revealed cerebral vasospasm and subsequent ischemia, a dangerous complication of subarachnoid hemorrhage. Therefore, for hemorrhagic hemangioblastomas, management must extend beyond resection to include meticulous perioperative care of vasospasm, electrolyte balance, intracranial pressure, and systemic status to reduce complication-related mortality.
In summary, while spontaneous rupture and hemorrhage of hemangioblastoma are rare, they are associated with high mortality and require urgent clinical attention. High-risk features may include large tumor size, solid morphology, and location in the posterior fossa or brainstem. Surgically, resection remains definitive, but the approach must balance radical removal with neurological preservation. This decision should be individualized based on tumor location, vascular anatomy, and patient status, and should consider preoperative embolization. Postoperatively, vigilant monitoring and aggressive management of complications such as cerebral vasospasm, elevated intracranial pressure, and endocrine-metabolic disturbances are critical. Future multi-center collaboration and larger case series are needed to better define prognostic factors and establish standardized protocols for the emergency and perioperative management of hemorrhagic hemangioblastomas.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Jejurkar MA Lagad SG Ranjan R . Recurrence of sporadic intracranial cerebellar hemangioblastoma: case report and literature review. Neurol India. (2021) 69:508–10. doi: 10.4103/0028-3886.314560, PMID: 33904491 · doi ↗ · pubmed ↗
- 2Igari Y Hosoya T Hayashizaki Y Usui A Kawasumi Y Usui K . Sudden death due to a cystic lesion in the cerebellum. Forensic Sci Int. (2014) 245:e 25–8. doi: 10.1016/j.forsciint.2014.10.017, PMID: 25459277 · doi ↗ · pubmed ↗
- 3Hussein MR . Central nervous system capillary haemangioblastoma: the pathologist's viewpoint. Int J Exp Pathol. (2007) 88:311–24. doi: 10.1111/j.1365-2613.2007.00535.x, PMID: 17877533 PMC 2517334 · doi ↗ · pubmed ↗
- 4de San Pedro JR Rodríguez FA Níguez BF Sánchez JF López-Guerrero AL Murcia MF . Massive hemorrhage in hemangioblastomas Literature review. Neurosurgical Rev. (2010) 33:11–26. doi: 10.1007/s 10143-009-0217-1, PMID: 19672640 · doi ↗ · pubmed ↗
- 5Liao T Huang Z Ma C . Spontaneous massive intraventricular hemorrhage due to hemangioblastoma in a child. Asian J Surg. (2024) 47:4638–40. doi: 10.1016/j.asjsur.2024.07.298, PMID: 39117543 · doi ↗ · pubmed ↗
- 6Yin X Duan H Yi Z Li C Lu R Li L . Incidence, prognostic factors and survival for hemangioblastoma of the central nervous system: analysis based on the surveillance, epidemiology, and end results database. Front Oncol. (2020) 10:570103. doi: 10.3389/fonc.2020.570103, PMID: 33014882 PMC 7509109 · doi ↗ · pubmed ↗
- 7Marvin E Akhter AS Coppens JR . Recurrent hemorrhage in hemangioblastoma involving the posterior fossa: Case report. Surg Neurol Int. (2017) 8:122. doi: 10.4103/sni.sni_91_17, PMID: 28713626 PMC 5502298 · doi ↗ · pubmed ↗
- 8Ene CI Morton RP Ferreira Jr M Sekhar LN Kim LJ . Spontaneous hemorrhage from central nervous system hemangioblastomas. World Neurosurg. (2015) 83:1180.e 13–7. doi: 10.1016/j.wneu.2015.02.009, PMID: 25727302 · doi ↗ · pubmed ↗