Association of serum methylglyoxal with endothelial dysfunction in patients with type 2 diabetes
Shanshan Yu, Xinyan Jin, Yuanying Xu, Zhao Liu, Jun Lu, Jie Gao, Wenjun Sha, Tao Lei

TL;DR
This study shows that higher levels of methylglyoxal in the blood are linked to worse blood vessel function in people with type 2 diabetes, suggesting it could be a useful early warning sign.
Contribution
The study identifies serum methylglyoxal as an independent and clinically relevant biomarker for endothelial dysfunction in type 2 diabetes.
Findings
Higher serum methylglyoxal levels were significantly associated with endothelial dysfunction in 76% of type 2 diabetes patients.
Methylglyoxal showed a strong negative correlation with flow-mediated dilation, even after adjusting for age and sex.
Methylglyoxal demonstrated good predictive power with an AUC of 0.785 for identifying endothelial dysfunction.
Abstract
To explore the correlation between serum Methylglyoxal (MGO) and endothelial dysfunction in patients with type 2 diabetes mellitus, and to evaluate the clinical value of MGO in the development of diabetes mellitus and its complications. In this cross-sectional study, we enrolled 250 patients diagnosed with T2MD. Based on flow-mediated dilation (FMD) measurements, the patients were categorized into normal endothelial function group (FMD ≥6.4%, n = 61) and endothelial dysfunction group (FMD <6.4%, n = 189). Analysis of the relationship between MGO and FMD was conducted via Spearman’s correlation, partial correlation, and multiple logistic regression. An ROC curve analysis was utilized to quantify the predictive performance of MGO for endothelial function. Endothelial dysfunction was observed in 189 (76%) patients with type 2 diabetes. Patients with endothelial dysfunction had higher…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
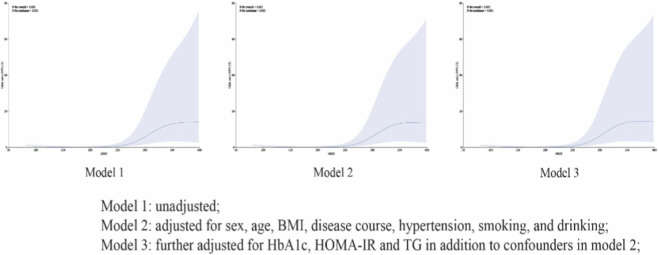 FIGURE 1
FIGURE 1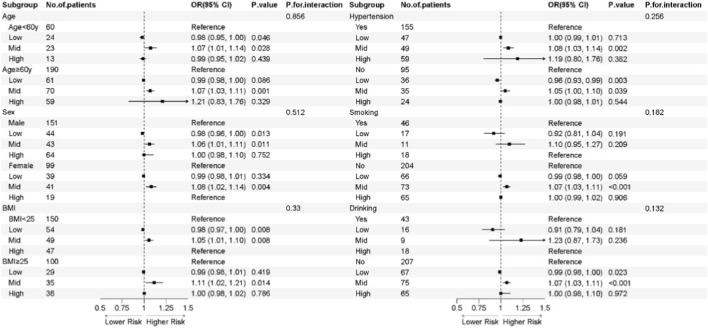 FIGURE 2
FIGURE 2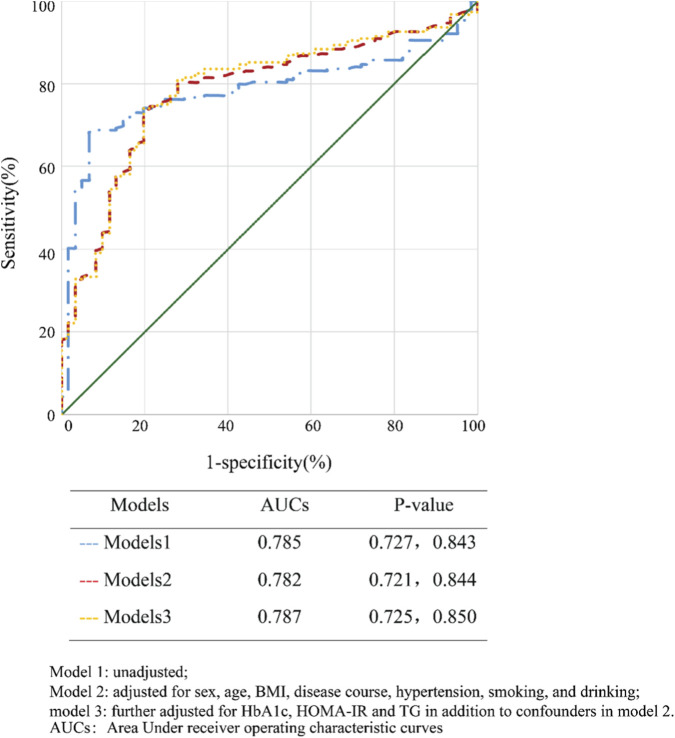 FIGURE 3
FIGURE 3| Variables | All (n = 250) | Nonendothelial dysfunction (n = 61) | Endothelial dysfunction (n = 189) | p for trend |
|---|---|---|---|---|
| Gender, male | 151 (60.4) | 31 (50.8) | 120 (63.5) | 0.078 |
| Age, years | 66.0 (60, 71) | 63.0 (54.0, 70.0) | 67.0 (60.5, 71.0) | <0.001 |
| Duration of diabetes, years | 10.0 (3, 20) | 6.0 (2.5, 15.0) | 10.0 (4, 20.0) | <0.001 |
| Current smoker, % | 46 (18.4) | 12 (19.7) | 34 (18) | 0.768 |
| Current drinkers, % | 43 (17.2) | 9 (14.8) | 34 (18) | 0.560 |
| BMI, kg/m2 | 24.2 (22.5, 26.7) | 23.9 (21.8, 25.8) | 24.4 (22.6, 26.9) | <0.001 |
| SBP, mmHg | 130 (125, 140) | 130 (124, 139) | 130 (125, 140) | <0.001 |
| DBP, mmHg | 80 (77, 88) | 80 (79, 90) | 80 (77, 88) | <0.001 |
| Hypertension (%) | 155 (62) | 29 (47.5) | 126 (66.7) | 0.007 |
| FPG, mmol/L | 7.13 (5.78,10.06) | 6.84 (5.91, 10.68) | 7.20 (5.63, 9.85) | <0.001 |
| HbA1c, % | 9.3 (7.9,11.1) | 9.5 (7.9–11.5) | 9.2 (7.6–10.9) | <0.001 |
| FCP, pmol/L | 0.7 (0.43,1.04) | 0.67 (0.47, 0.93) | 0.71 (0.42, 1.04) | <0.001 |
| F-INS, pmol/L | 74.39 (50.75, 132.6) | 72.5 (49.39,157.5) | 74.97 (50.84,125.7) | <0.001 |
| HOMA-IR, mmol/L*mU/L | 25.66 (15.26, 50.4) | 25.97 (15.25,60.3) | 25.47 (15.06,47.61) | <0.001 |
| TC, mmol/L | 4.41 (3.55, 5.36) | 4.80 ± 1.35 | 4.34 (3.53, 5.28) | <0.001 |
| TG, mmol/L | 1.41 (1.06, 2.21) | 1.31 (0.97, 1.79) | 1.44 (1.06, 2.30) | <0.001 |
| HDL-C, mmol/L | 1.08 (0.92, 1.32) | 1.14 ± 0.27 | 1.11 (0.82, 1.34) | <0.001 |
| LDL-C, mmol/L | 2.61 (1.93, 3.5) | 3.02 ± 1.15 | 2.49 (1.89, 3.28) | <0.001 |
| MGO, Pg/ML | 269.66 (214.00, 314.81) | 216.68 (199.32, 235.83) | 289.56 (236.44, 326.81) | <0.001 |
| FMD (%) | 5.3 (3.78,6.3) | 7.4 (6.85, 8.55) | 4.7 (3.2, 5.7) | 0.033 |
| Variables | Spearman’s correlation | Partial correlation | ||
|---|---|---|---|---|
|
|
|
|
| |
| Sex (male) | 0.192 | 0.002 | - | - |
| Age (years) | −0.266 | <0.001 | - | - |
| BMI (kg/m2) | −0.90 | 0.154 | −0.131 | 0.039 |
| Disease course (years) | −0.191 | 0.002 | −0.117 | 0.067 |
| SBP (mmHg) | −0.051 | 0.426 | −0.023 | 0.720 |
| DBP (mmHg) | 0.024 | 0.707 | −0.015 | 0.809 |
| Smoking (%) | −0.049 | 0.437 | 0.018 | 0.779 |
| Drinking (%) | −0.068 | 0.282 | 0.009 | 0.887 |
| HbA1c (%) | 0.078 | 0.222 | 0.085 | 0.182 |
| HOMA-IR | −0.009 | 0.881 | −0.141 | 0.026 |
| TC (mmol/L) | 0.223 | <0.001 | 0.083 | 0.193 |
| TG (mmol/L) | −0.050 | 0.435 | −0.095 | 0.135 |
| HDL-C (mmol/L) | 0.111 | 0.079 | 0.036 | 0.574 |
| LDL-C (mmol/L) | 0.221 | <0.001 | 0.093 | 0.143 |
| MGO (pg/mL) | −0.611 | <0.001 | −0.36 | <0.001 |
| | Model 1 | Model 2 | Model 3 | |||
|---|---|---|---|---|---|---|
| Or (95%CI) | P Value | Or (95%CI) | P Value | Or (95%CI) | P Value | |
| MGO per 10 pg/mL | 1.099 (1.06,1.14) | <0.001 | 1.096 (1.05,1.14) | <0.001 | 1.096 (1.05,1.14) | <0.001 |
| MGO tertiles | ||||||
| Tertile 1 | 1 (REF) | — | 1 (REF) | — | 1 (REF) | — |
| Tertile 2 | 4.57 (2.82–7.40) | <0.001 | 4.44 (2.68–7.35) | <0.001 | 4.41 (2.65–7.32) | <0.001 |
| Tertile 3 | 3.18 (1.63–6.21) | <0.005 | 3.28 (1.64–6.55) | <0.005 | 3.22 (1.60–2.50) | <0.005 |
|
| 37.67 (8.68–163) | <0.001 | 32.95 (7.41–146) | <0.001 | 32.66 (7.34–145) | <0.001 |
| per SD | 2.67 (1.78–4.01) | <0.001 | 2.60 (1.70–3.97) | <0.001 | 2.61 (1.69–4.02) | <0.001 |
- —Shanghai Municipal Health Commission10.13039/100017950
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAdvanced Glycation End Products research · Fatty Acid Research and Health · Antioxidant Activity and Oxidative Stress
Introduction
1
Diabetes mellitus (DM) is a chronic metabolic disease, which is caused by the defect of islet function secretion or the impairment of other biological functions (Tufail et al., 2025). According to the data of the International Diabetes Federation (IDF) in 2025, the number of diabetes patients aged 20 to 79 in the world is as high as 589 million, and is expected to increase to 853 million by 2050, accounting for 13% of the global population.In 2024, more than 3.4 million people died of diabetes and its complications worldwide, accounting for 9.3% of the total number of deaths worldwide (Cai et al., 2024). Diabetes mellitus has emerged as a major global public health challenge that poses a serious threat to human health. In addition, the total healthcare expenditure related to diabetes and its complications in the world exceeded $1 trillion for the first time in 2024, posing a serious challenge to the global health system (International Diabetes Federation, 2025).
Type 2 diabetes is characterized by multiple metabolic disorders characterized by chronic glucose homeostasis imbalance, increased oxidative conditions, and disturbances in carbohydrate, fat, and protein metabolism (Twarda-Clapa et al., 2022). Methyl glyoxal (MGO) is an α-oxaldehyde, a highly reactive acyclic dicarbonyl compound produced during the oxidation of sugars, and a by-product of glucose, lipid, and amino acid metabolism (Abidi et al., 2018). They react readily with lysine and arginine residues of lipids, nucleic acids, and proteins to form advanced glycation end products (Advanced Glycated Endproducts, AGEs); Hyperglycemia, decreased glucose utilization, and phosphotriose isomerase deficiency lead to increased plasma MGO levels and decreased levels of the reducing product glutathione, which together cause oxidative stress and damage vascular endothelial function, thereby inducing a variety of complications, mainly vascular disease (Vašková et al., 2025).
Vascular complications of diabetes involve heart, brain, kidney, retina and other important organs, which is the leading cause of death and disability in diabetic patients (Sallam and Laher, 2020). Clinical studies have shown that the age of atherosclerosis in diabetic patients is younger, the severity is higher, and the scope of lesions is wider. Atherosclerosis is the core manifestation of diabetic vascular lesions, and endothelial dysfunction is the initiating factor of atherosclerosis. The three affect each other (Lee et al., 2023). As a highly efficient glycation agent with 20,000 times higher reactivity than glucose, MGO can induce the growth of necrotic core of plaque in diabetic atherosclerosis patients, which makes the plaque prone to rupture and accelerates the development of diabetic complications (Schalkwijk et al., 2023; Hanssen et al., 2018).
Therefore, based on the universality and harmfulness of diabetic vascular complications, it is very important to evaluate and prevent the early vascular injury of diabetes. The assessment of endothelial function is based on the traditional invasive percutaneous quantitative coronary angiography, but it has limitations in clinical screening (Baltu et al., 2019). Flow-mediated dilation (FMD) of the brachial artery is a new noninvasive technique for assessing vascular endothelial function.In terms of assessment results, FMD is highly correlated with the gold standard quantitative coronary angiography, and has become a good indicator for replacing coronary angiography (Flammer et al., 2012). Studies have shown that a 1% reduction in FMD increases the risk of cardiovascular events by 13% (Hashimoto et al., 2021; Welters et al., 2017).
Vascular disease caused by diabetes mellitus involves heart, brain and other important organs, which is the main cause of death and disability in diabetic patients (Khan and Jandeleit-Dahm, 2025). Related studies have shown that vascular endothelial damage caused by endothelial dysfunction is an important factor in vascular disease (Pasut et al., 2025; Ji et al., 2025). MGO promotes endothelial dysfunction through oxidative stress and inflammation (Wan et al., 2024). Therefore, elucidating the relationship between MGO and endothelial dysfunction holds important clinical implications for preventing diabetic vascular complications.This study was to investigate the correlation between MGO and endothelial dysfunction in type 2 diabetes mellitus, to evaluate the clinical value of MGO in diabetes mellitus and its complications, and to provide a basis for early clinical diagnosis of diabetic vascular lesions.
Materials and methods
2
Object of study
2.1
In this cross-sectional study, 273 patients diagnosed with T2MD were recruited in the Department of Endocrinology, Putuo Hospital, Shanghai University of Traditonal Chinese Medicine from 1 January 2024 to 22 November 2024. The diagnostic criteria were in line with the diagnostic criteria of diabetes mellitus issued by WHO in 1999. Exclusion criteria: patients with diabetic ketoacidosis; patients with severe hepatic and renal dysfunction; patients with malignant tumors; patients with severe anemia, infection or trauma, and autoimmune diseases; patients during pregnancy and lactation; and patients with cognitive dysfunction or psychiatric disorders.
In order to achieve the aim of research, we excluded patients with following conditions: (1) diabetic ketoacidosis (n = 5), (2) severely liver and kidney dysfunction (n = 8) (3) and patients with malignant tumors (n = 10). Ultimately, 250 patients were collected for this ivestiggation. Finally, 250 patients were enrolled. According to the results of FMD, the patients were divided into normal endothelial function group (FMD ≥6.4%, n = 61) and endothelial dysfunction group (FMD <6.4%, n = 189).
Ethical approval for this study was granted by the Institutional Review Board of Putuo Hospital, Shanghai University of Traditional Chinese Medicine. All procedures were performed in full compliance with the ethical standards of the revised Helsinki Declaration. Written informed consent was obtained from all individual participants prior to any study procedures, and all personally identifiable information was held in strict confidence.
Anthropometric and laboratory measurement
2.2
Diagnostic criteria for type 2 diabetes: (1) typical diabetic symptoms (polydipsia, polyuria, polyphagia, unexplained weight loss) plus random blood glucose ≥11.1 mmol/L; (2) Fasting blood glucose ≥7.0 mmol/L or blood glucose ≥11.1 mmol/L 2 h after glucose loading (3) Glycosylated hemoglobin ≥6.5% (4) Patients without typical symptoms of diabetes should be reexamined another day for confirmation.
The general clinical data and laboratory biochemical indicators of the patients in the two groups were collected, and the concentration of MGO in the serum of the patients was measured. Clinical information including age, gender, height, weight, course of diabetes, smoking history, drinking history, history of hypertension were collected and BMI was calculated. After fasting for 12 h, 3–5 mL venous blood was drawn on an empty stomach the next morning, and glycosylated hemoglobin, FPG, TC, TG, HDL-C, LDL-C and fasting insulin were detected by Roche cobas8000 automatic biochemical analyzer. The HOMA-IR calculation formula was (fasting blood glucose * fasting insulin)/22.5. Glycosylated hemoglobin (HbA1c) was detected by BC -5390 glycosylated hemoglobin analyzer (Premier Hb9210) and high performance liquid chromatography.
Measurement of FMD: Subjects were instructed to fast for at least 4 h before the test and to abstain from smoking, alcohol, caffeine, or antioxidant vitamins for at least 12 h before the test.Patients were asked to rest in a sitting position in a quiet, dark, air-conditioned room (22 °C–25 °C) for at least 5 min before their blood pressure was measured by sphygmomanometry (Yoshida et al., 2010). FMD measurements were then performed after the patient was in the same room, resting in the prone position for at least 15 min. Ultrasound measurements were performed according to the guidelines for ultrasound assessment of brachial artery FMD. Calculation formula: FMD (%) = [maximum vessel diameter (mm)-vessel diameter at rest (mm)]/vessel diameter at rest (mm) * 100%.
After the whole blood sample was collected and kept at room temperature for 2 h, it was centrifuged for 15 min with a centrifuge at a speed of 2000 rpm. The supernatant of the blood sample was taken and packed into 1.5 mL EP tubes and stored in a refrigerator at a low temperature of −80 °C. Serum MGO concentrations were measured using a human MGO enzyme-linked immunosorbent assay (ELISA) kit (Fusheng Industrial Co., Ltd., China), all in strict accordance with the instructions.
Statistical methods
2.3
Statistical analyses were conducted using SPSS for Windows version 27.0. The Kolmogorov–Smirnov test evaluated the distribution of all continuous variables; those with a normal distribution were presented as mean ± standard deviation (®x ± s). Continuous variables that did not follow a normal distribution were reported as median (lower quartile, upper quartile) [M (QL, QU)], while categorical variables were expressed as counts and percentages (n [%]). Group differences were assessed using the Mann–Whitney U test for continuous variables and the chi-square test for categorical variables. Spearman’s correlation and multivariable logistic regression analyses were performed to examine the relationship between FMD and MGO. Additionally, the ROC curve was employed to evaluate the sensitivity and specificity of MGO in predicting endothelial dysfunction.
Results
3
Clinical data characteristics of patients from both groups were included
3.1
Table 1 presents the fundamental clinical characteristics of the patients who were ultimately enrolled. This study included a total of 189 patients diagnosed with endothelial dysfunction. The individuals in the endothelial dysfunction group were clearly older than those in the group without endothelial dysfunction. (67 vs. 63, p < 0.001). Patients with endothelial dysfunction had significantly higher MGO levels than those without endothelial dysfunction (289.56 (236.44, 326.81) vs. 216.68 (199.32, 235.83), p < 0.001). No significant differences were observed between the study groups regarding gender, smoking status, alcohol consumption, and disease duration.
Spearman correlation analysis of correlation between FMD and MGO and other indicators
3.2
Table 2 presents the relationship between FMD and MGO, along with other clinical indicators. Spearman’s correlation analysis revealed a significant negative relationship between FMD and MGO. (R = −0.611, p < 0.001). Additionally, endothelial function was positively correlated with gender (R = 0.192, p = 0.002), TC (R = 0.223, p < 0.001) and LDL-C (R = 0. 221, p < 0.001); And there was a negative correlation with age (R = −0.266, p < 0.001) and course of disease (R = −0.191, p = 0.002). We found that the indicators MGO (r′ = −0.36, p < 0.001) still remained the negative association with FMD afer controlling the variables sex and age, but the correlation coefficient between MGO and FMD decreased. Nevertheless, the correlation between endothelial function and course of disease, TC and LDL-C disappeared following the two variables fixed, and there was a negative correlation between endothelial function.
Logistic regression analysis of influencing factors of endothelial dysfunction in patients with type 2 diabetes mellitus
3.3
Following analysis, MGO was identified as an independent risk factor for endothelial dysfunction in individuals with T2DM. Table 3 demonstrates a significant negative association of endothelial function with per 10% increase in MGO concentration in the univariable analysis (Model 1) (OR 1.099, 95% CI 1.06–1.14). This association remained significant after adjusting for sex, age, BMI, course of disease, hypertension, smoking, and alcohol consumption (OR 1.096, 95% CI 1.05–1.14), as well as further adjustment for HbA1c, HOMA-IR, and TG (OR 1.096, 95% CI 1.05–1.14). In Model 1, the risk of endothelial dysfunction peaked in the Tertile two of MGO levels (ORs = 4.57, 95% CI, 2.82–7.40) compared with the Tertile 1, the odds ratio slightly attenuated in the Tertile 3 (ORs = 3.18, 95% CI, 1.63–6.21). In Model 2, the adjusted ORs were 4.44 (95% CI: 2.68–7.35) for the second tertile and 3.28 (95% CI: 1.64–6.55) for the third tertile (p for trend<0.01)). These associations persisted in Model 3, with corresponding ORs of 4.41 (95% CI: 2.65–7.32) and 3.22 (95% CI: 1.60–6.50) (p for trend<0.01). In model 1, a one standard deviation (SD) rise in MGO (PG/mL) corresponded to a 2.67 -fold higher risk of endothelial dysfunction (95% CI 1.78–4.01). After controlling for sex, age, BMI, disease duration, hypertension, smoking status, alcohol consumption, HbA1c, HOMA-IR, and triglyceride levels, the association remained significant and materially unchanged, with odds ratios of 2.60 (95% CI: 1.70–3.97) in Model two and 2.61 (95% CI: 1.69–4.02) in Model 3.
To further investigate the dose-response relationships, restricted cubic spline (RCS) analyses were performed to assess the continuous associations between MGO levels and endothelial dysfunction in patients with type 2 diabetes. The restricted cubic spline (RCS) analysis demonstrated a significant relationship between MGO levels and endothelial dysfunction in patients with type 2 diabetes (P overall<0.001). The risk of endothelial dysfunction increased with rising MGO levels and reached a plateau beyond the second tertile (P non-linearity<0.001) (Figure 1). And Similar results were obtained when adjusting for gender, age, BMI, course of disease, hypertension, smoking and alcohol consumption (model 2), and HbA1c, HOMA-IR, C-reactive protein, and TG (model 3).
Restricted Cubic Spline (RCS): Association of MGO levels with the risk of endothelial dysfunction. Notes: The dose-response relationship was characterized using restricted cubic spline. P non-linearity<0.001 indicates a significant deviation from linearity. Model 1: unadjusted; Model 2: adjusted for sex, age, BMI, disease course, hypertension, smoking, and drinking; Model 3: further adjusted for HbA1c, HOMA-IR and TG in addition to confounders in model 2; OR: odds ratio; 95% CI: 95% confidence interval.
Subgroup analyses were performed using Model one to evaluate potential effect modifications by various demographic and clinical characteristics. These findings are visually summarized in the forest plot (Figure 2), with subgroups stratified by age, sex, BMI category, hypertension status, smoking status, and alcohol consumption. The stability of the main association was further supported by consistent effect sizes observed across all predefined subgroups, with no statistically significant interactions observed (all P-interaction >0.05). These findings provide additional evidence supporting the negative association between MGO levels and risk of endothelial function.
Subgroup analysis for the risk of endothelial dysfunction. Notes: The forest plot displays the odds ratios (OR) and 95% confidence intervals for the risk of endothelial dysfunction across various subgroups. The squareas represent the point estimates of the OR, and the horizontal lines indicate the 95% CI. P interaction values were calculated to evaluate the consistency of the association across different sstrata. OR: odds ratio; 95% CI: 95% confidence interval.
Receiver operating curve for MGO predicting endothelial dysfunction
3.4
Based on the regression models, ROC curves were constructed to evaluate the predictive performance of MGO for endothelial dysfunction in patients with type 2 diabetes (Figure 3). In the fully adjusted model (Model 3), which included sex, age, BMI, disease duration, hypertension, smoking status, alcohol consumption, HbA1c, HOMA-IR, and triglyceride levels, the area under the receiver operating characteristic curve (AUC) was significantly greater compared to both Model 2 (0.787 vs. 0.782; p < 0.001) and Model 1 (0.787 vs. 0.785; p < 0.001). Furthermore, the AUC of Model one was also significantly higher than that of Model 2, which was further adjusted for gender, age, BMI, disease duration, hypertension, smoking, and alcohol consumption.
Receiver operating characteristic (ROC) curves for MGO Predicting Endothelial Dysfunction. Notes: Model 1: unadjusted; Model 2: adjusted for sex, age, BMI, disease course, hypertension, smoking, and drinking; Model 3: further adjusted for HbA1c, HOMA-IR and TG in addition to confounders in model 2; AUCs: Area Under receiver operating characteristic curves.
Discussion
4
The latest IDF shows that as of 2024, China is the country with the largest number of diabetes patients aged 20-79, up to 148 million, and is expected to continue to grow to 168.3 million by 2050. The total expenditure related to diabetes is 168.9 billion US dollars, accounting for 16.6% of the global expenditure, which poses a great challenge to the medical system and medical consumption. The prevalence of diabetes mellitus is increasing year by year, and the risk of cardiovascular and cerebrovascular diseases in patients with type 2 diabetes mellitus is 72% higher than that in patients without diabetes mellitus, which aggravates the occurrence of macrovascular and microvascular diseases and leads to the rising mortality of diabetes mellitus and its complications (Tufail et al., 2025). Vascular endothelial cells play an important role in regulating vasoconstriction, vasodilation and local inflammation. Chronic hyperglycemia can directly damage endothelial cells and lead to endothelial dysfunction. Compared with glucose, MGO has higher glycosylation reactivity, which can more rapidly produce glycosyl compounds with extracellular proteins, lipids and DNA, form AGEs and reduce the production of nitric oxide. Induces inflammation and oxidative stress, resulting in vasoconstriction and abnormal cell growth, which in turn leads to endothelial dysfunction (Tufail et al., 2025). Endothelial dysfunction is a key factor in the initiation and promotion of diabetic angiopathy, and it is also one of the foundations of diabetic angiopathy. Therefore, it is very important to study endothelial function for the maintenance of cardiovascular homeostasis and the prevention and treatment of diabetic angiopathy. As a new technique for detecting endothelial function based on flow-mediated vasodilation (FMD) of brachial artery, it has the characteristics of easy operation, high accuracy, non-invasive and wide application. Related studies have shown that FMD can be used as an index to evaluate the functional status of vascular endothelium.
Studies have shown that patients with type 2 diabetes have higher plasma levels of MGO, which leads to an increased risk of cardiovascular events and mortality (McTiernan et al., 2019). In this study, the serum MGO level in type 2 diabetic patients with vascular endothelial dysfunction was higher than that in patients without endothelial dysfunction. In addition, patients in the endothelial dysfunction group were older than those in the non-endothelial dysfunction group. Age is an independent risk factor for the progressive decline of endothelial function. The decline of endothelial function with age is caused by the increase of apoptosis and the decrease of regeneration ability of endothelial cells during aging (Ahmed et al., 2024; Tomiyama and Yamashina, 2014).
Our study demonstrated that MGO levels were significantly elevated in patients with endothelial dysfunction compared to those with normal endothelial function. This finding was further supported by a robust inverse correlation between MGO concentrations and endothelial function (measured by FMD), suggesting a direct detrimental role of MGO in vascular homeostasis. In the multivariable logistic regression analysis, MGO emerged as an independent risk factor for endothelial dysfunction, even after adjusting for traditional cardiovascular confounders. For every 10% increase in MGO, the risk of endothelial dysfunction in type 2 diabetes increased by 9.9%, and for every standard deviation increase in MGO, the risk of endothelial dysfunction increased by 2.67 times.
Intriguingly, the risk of endothelial dysfunction did not increase in a strictly linear fashion. We observed that the odds ratio for the second tertile (T2) was higher than that for the third tertile (T3). This non-monotonic trend was fully validated by the restricted cubic spline (RCS) analysis, which illustrated a non-linear dose-response relationship characterized by a plateau effect beyond the T2 threshold. Such a pattern suggests a potential ‘saturation effect,' wherein the pathological impact of MGO on the vascular endothelium may reach a maximal threshold at moderate-to-high concentrations, after which further elevation in MGO does not lead to a proportional increase in risk. Furthermore, the results of our subgroup analysis, visualized through forest plots, confirmed that this negative association remained consistent across diverse clinical strata. These findings collectively underscore the robust and independent role of MGO as a critical mediator of endothelial impairment.
Endothelial dysfunction is caused by many factors, among which diabetes and obesity play a leading role. In patients with dyslipidemia, high low-density lipoprotein cholesterol in the blood is prone to oxidation reaction, forming ox-LDL, which can directly damage endothelial cells, make cells produce excessive reactive oxygen species, further damage the structure of endothelial cells, and impair their function (Kweon et al., 2025; Suraj-Prażmowska et al., 2025). In people with overweight BMI, visceral fat can release free fatty acids and proinflammatory factors to directly damage endothelial cells, or induce excessive production of mitochondrial ROS. Superanions combine with NO to produce peroxynitrite, thus reducing the bioavailability of NO (Rivera et al., 2025). Insulin is an anabolic hormone and a potent vasoactive hormone that regulates vascular tone and tissue perfusion, and insulin resistance is a key factor in the development of type 2 diabetes and its associated cardiovascular complications (Gomez Toledo et al., 2025; Matsuzawa and Lerman, 2014). MGO directly impairs the glucose uptake of islet beta cells, reduces insulin clearance, produces insulin glycosylation, or increases the proliferation and expansion of adipose tissue, reduces capillarization, and eventually leads to insulin resistance. Insulin resistance reduces NO-dependent vasodilation mediated by insulin in arteries and arterioles, increases vascular tension, reduces tissue perfusion, accelerates the formation of atherosclerosis, impairs endothelial structure and function, and eventually leads to endothelial dysfunction (Penna and Pagliaro, 2025; Horton et al., 2025).
This study has limitations. First, this study is a single-center cross-sectional study with a small sample size. Second, Information regarding antidiabetic, antihypertensive, lipid-lowering, or antioxidant medications with an effect on vascular endothelial function, such as GLP-1, SGLT-2, ACEI, and CCB, were uanavailable. Thirdly, serum factors that reflect endothelial function, such as nitric oxide, endothelin-1, and endothelin-nitric oxide synthase, were not examined in this study. Fourthly, in the present study, plasma MGO levels were quantified using ELISA. While this method is more widely accessible and prevalent in clinical settings, we acknowledge that Liquid Chromatography-Mass Spectrometry (LC-MS) remains the ‘gold standard' for MGO measurement, as highlighted by Hanssen (Hanssen et al., 2018). Consequently, we aim to adopt this more precise methodology in our prospective investigations to further validate the current findings.
Conclusion
5
To sum up, this study shows that there is a correlation between elevated serum MGO levels and endothelial function (measured by FMD), which can be used as a new indicator to evaluate endothelial function in patients with type 2 diabetes mellitus, and provide a new basis for clinical prevention of diabetic angiopathy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Abidi M. Khan M. S. Ahmad S. Kausar T. Nayeem S. M. Islam S. (2018). Biophysical and biochemical studies on glycoxidatively modified human low density lipoprotein. Arch. Biochem. Biophys. 645, 87–99. 10.1016/j.abb.2018.02.019 29524430 · doi ↗ · pubmed ↗
- 2Ahmed B. Rahman A. A. Lee S. Malhotra R. (2024). The implications of aging on vascular health. Int. J. Mol. Sci. 25 (20), 11188. 10.3390/ijms 252011188 39456971 PMC 11508873 · doi ↗ · pubmed ↗
- 3Baltu F. Sarici A. M. Yildirim O. Mergen B. Bolat E. (2019). Investigation of vascular endothelial dysfunction in the patients with age-related macular degeneration. Cutan. Ocul. Toxicol. 38 (1), 29–35. 10.1080/15569527.2018.1504056 30037291 · doi ↗ · pubmed ↗
- 4Cai S. S. Zheng T. Y. Wang K. Y. Zhu H. P. (2024). Clinical study of different prediction models in predicting diabetic nephropathy in patients with type 2 diabetes mellitus. World J. Diabetes 15 (1), 43–52. 10.4239/wjd.v 15.i 1.43 38313855 PMC 10835501 · doi ↗ · pubmed ↗
- 5Flammer A. J. Anderson T. Celermajer D. S. Creager M. A. Deanfield J. Ganz P. (2012). The assessment of endothelial function: from research into clinical practice. Circulation 126 (6), 753–767. 10.1161/CIRCULATIONAHA.112.093245 22869857 PMC 3427943 · doi ↗ · pubmed ↗
- 6Gomez Toledo A. Golden G. J. Cummings R. D. Malmstr Malmström J. Esko J. D. (2025). Endothelial glycocalyx turnover in vascular health and disease: rethinking endothelial dysfunction. Annu. Rev. Biochem. 94 (1), 561–586. 40132227 10.1146/annurev-biochem-032620-104745 · doi ↗ · pubmed ↗
- 7Hanssen N. M. J. Westerink J. Scheijen JLJM van der Graaf Y. Stehouwer C. D. A. Schalkwijk C. G. (2018). Higher plasma methylglyoxal levels are associated with incident cardiovascular disease and mortality in individuals with type 2 diabetes. Diabetes Care 41 (8), 1689–1695. 10.2337/dc 18-0159 29784769 · doi ↗ · pubmed ↗
- 8Hashimoto H. Maruhashi T. Yamaji T. Harada T. Han Y. Takaeko Y. (2021). Smoking status and endothelial function in Japanese men. Sci. Rep. 11 (1), 95. 10.1038/s 41598-020-80012-x 33420173 PMC 7794366 · doi ↗ · pubmed ↗