Conservative management of gastric ulcer penetration using a polyglycolic acid sheet: a case report
Toshiyuki Wakatsuki, Tatsuhiro Go, Jun Harada, Hiroki Numoto, Yuta Nanimoto, Tomoko Sato

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
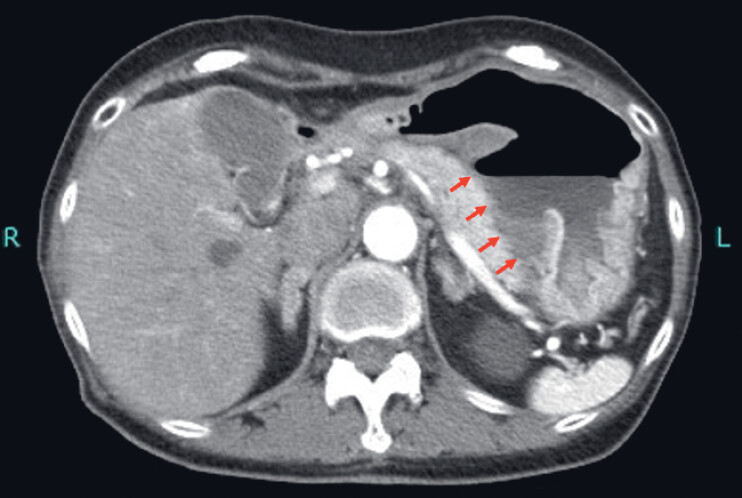 Fig. 1
Fig. 1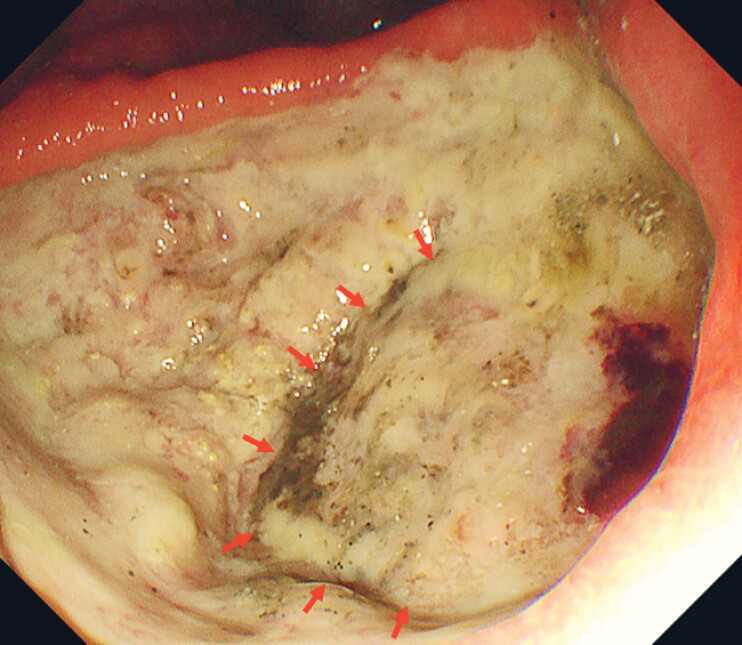 Fig. 2
Fig. 2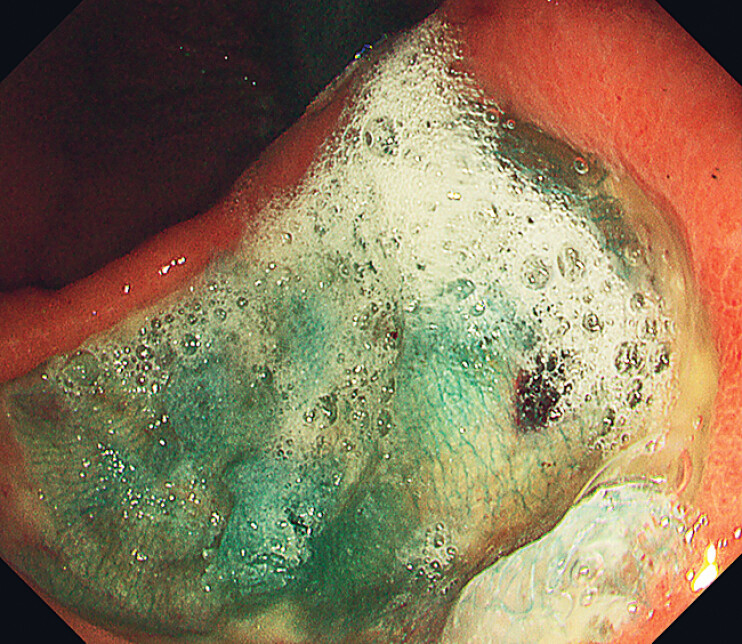 Fig. 3
Fig. 3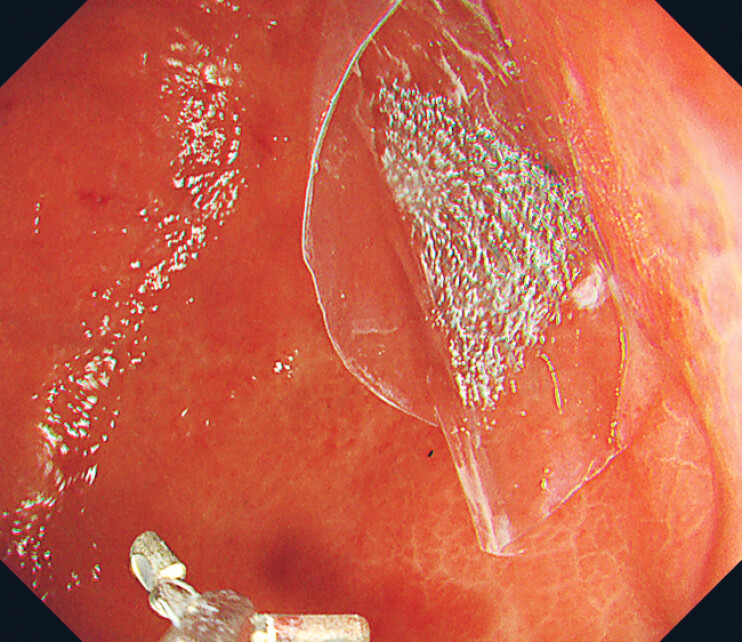 Fig. 4
Fig. 4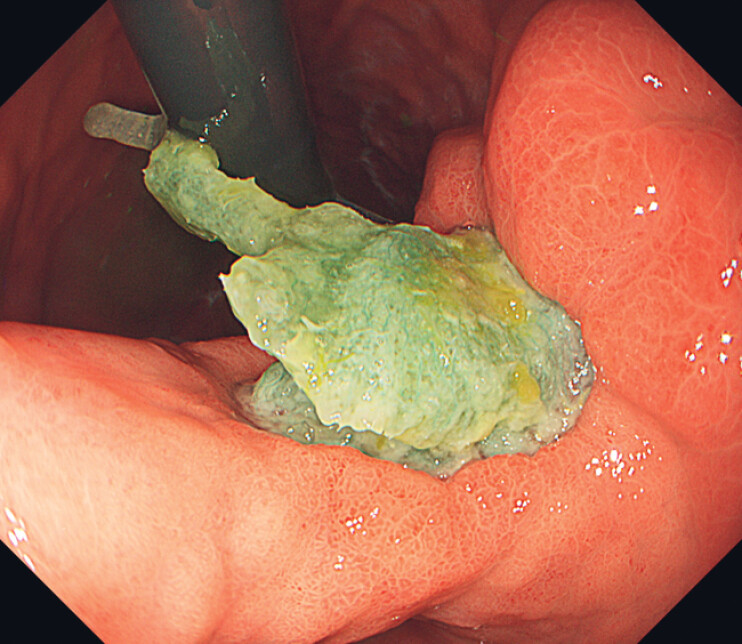 Fig. 5
Fig. 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHelicobacter pylori-related gastroenterology studies · Gastric Cancer Management and Outcomes · Gallbladder and Bile Duct Disorders
A 76-year-old woman was admitted with loss of appetite. Physical examination revealed no abnormalities, but blood tests showed mild anemia. Computed tomography revealed a gastric ulcer penetrating into the pancreas ( Fig. 1 ), without free air in the abdominal cavity. Esophagogastroduodenoscopy revealed an active gastric ulcer on the lesser curvature of the gastric angle and pancreatic tissue visible at the ulcer base, confirming penetration ( Fig. 2 ). She was diagnosed with gastric ulcer penetrating the pancreas and managed conservatively. A polyglycolic acid (PGA) sheet and fibrin glue were applied; custom-made oriented polypropylene (OPP) bags were used to deliver a PGA sheet into the stomach and cover the ulcer base ( Fig. 3 and Fig. 4 ; Video 1 ). We prepared original OPP bags for delivery by cutting commercialized ballpoint pen packs into 40-mm pieces. PGA sheets shrink in size and lose adhesive strength when exposed to saliva or mucus. Using OPP bags allows large PGA sheets to be stored in envelopes during transport, enabling rapid delivery and fixation in the stomach without exposing them to saliva or mucus. The bags were removed after the procedure. Ten days later, endoscopic examination revealed a reduction in ulceration, epithelial regeneration, and residual PGA sheets ( Fig. 5 ). Oral intake was resumed, and the patient was discharged 2 weeks later.
Computed tomography revealed a gastric ulcer penetrating into the pancreas (red arrow) with no free air within the abdominal cavity.
Esophagogastroduodenoscopy revealed an active gastric ulcer in the lesser curvature of the gastric angle. A region deeper than the base of other ulcers was observed, raising suspicion of penetration into pancreatic tissues (red arrow).
PGA sheets were used to cover the ulcers and were fixed in place with fibrin glue. PGA, polyglycolic acid.
PGA sheets were delivered into the stomach using the Original OPP bags. OPP, oriented polypropylene; PGA, polyglycolic acid.
Ten days after the removal of the OPP bags, endoscopic examination revealed a reduction in ulceration, epithelial regeneration, and residual PGA sheets. OPP, oriented polypropylene; PGA, polyglycolic acid.
Endoscopic polyglycolic acid sheet application for gastric ulcer perforation.Video 1
Peptic ulcers can penetrate the bowel wall without causing free perforation or leakage into the peritoneal cavity, leading to atypical symptoms due to the involvement of adjacent organs. Although surgical intervention is usually required, conservative management was feasible in our case because there were no inflammatory findings or free air in the abdominal cavity. To our knowledge, this is the first reported case of a gastric ulcer penetrating the pancreas successfully treated with a PGA sheet to promote wound healing, resulting in favorable recovery. Previous reports have demonstrated the effectiveness of PGA sheets in treating gastrointestinal fistulas 1 2 3 , serving as a scaffold for tissue regeneration and inducing the growth of granulation tissue that covers perforations 4 . In cases of peptic ulcer penetration without free air, the endoscopic application of PGA sheets may be an alternative to surgery.
Endoscopy_UCTN_Code_TTT_1AO_2AN Endoscopy_UCTN_Code_TTT_1AO_2AO Endoscopy_UCTN_Code_CCL_1AB_2AC_3AZ
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Takimoto K Hagiwara A Filling and shielding for postoperative gastric perforations of endoscopic submucosal dissection using polyglycolic acid sheets and fibrin glue Endosc Int Open 20164 E 661E 66410.1055/s-0042-10586727556075 PMC 4993898 · doi ↗ · pubmed ↗
- 2Nakano Y Takao T Morita Y Endoscopic plombage with polyglycolic acid sheets and fibrin glue for gastrointestinal fistulas Surg Endosc 2019331795180130251142 10.1007/s 00464-018-6454-z · doi ↗ · pubmed ↗
- 3Kawabata H Sone D Yamaguchi K Filling of Polyglycolic Acid Sheets for Closure of Gastrointestinal Fistulas With an Easily Deliverable Technique Using a Guidewire Gastroenterol Res 2020139610010.14740/gr 1284 PMC 733185632655725 · doi ↗ · pubmed ↗
- 4Kroez M Lang W Dickneite G Wound healing and degradation of the fibrin sealant Beriplast P following partial liver resection in rabbits Wound Repair Regen 20051331832310.1111/j.1067-1927.2005.130315.x 15953052 · doi ↗ · pubmed ↗