Endoscopic ultrasound-guided gallbladder drainage in situs inversus totalis using a loop formation technique
Sho Kitagawa, Narito Murakoshi, Naoki Shiga

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
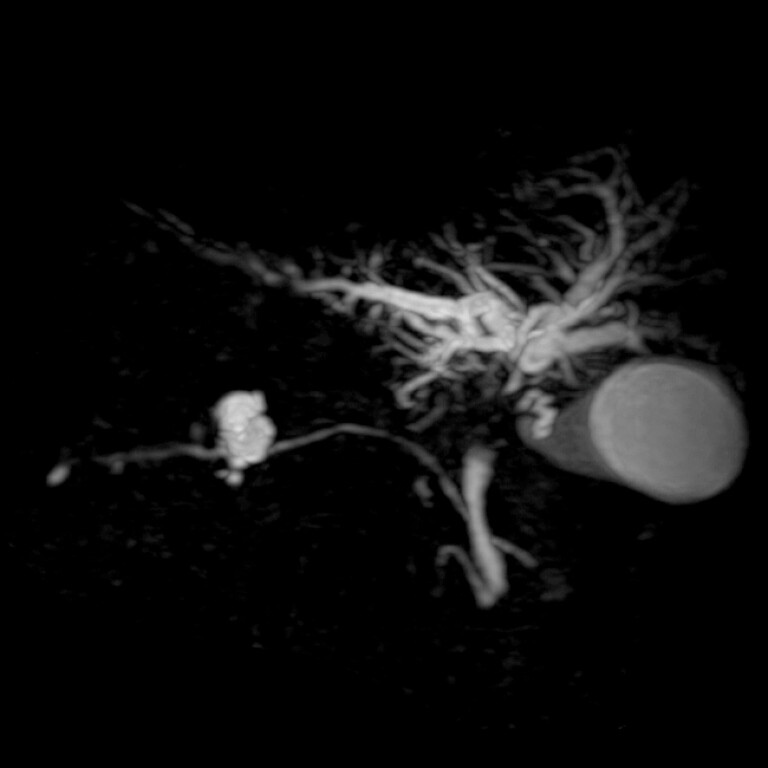 Fig. 1
Fig. 1 Fig. 2
Fig. 2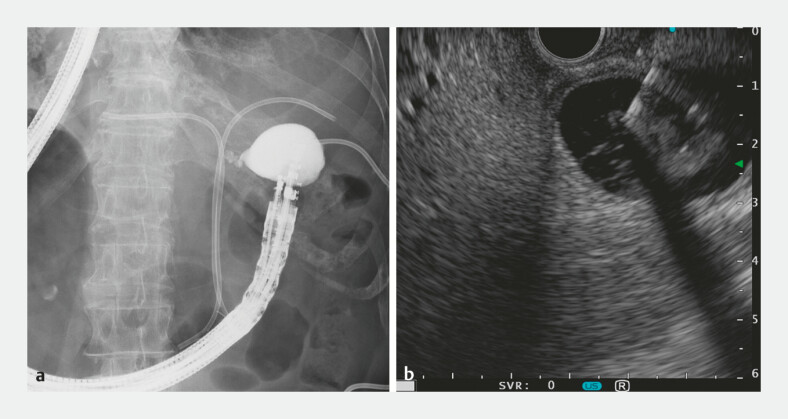 Fig. 3
Fig. 3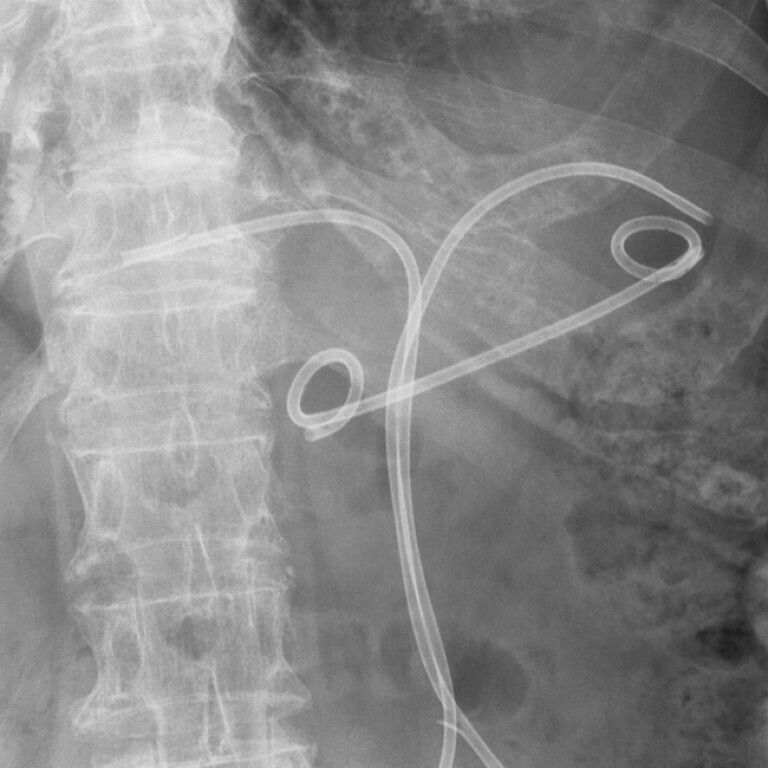 Fig. 4
Fig. 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntestinal Malrotation and Obstruction Disorders · Pediatric Hepatobiliary Diseases and Treatments · Biliary and Gastrointestinal Fistulas
Endoscopic retrograde cholangiopancreatography in patients with situs inversus totalis (SIT) is technically challenging because of the mirror-image anatomy, with ergonomic difficulties and scope instability often necessitating procedural modifications 1 2 3 . Endoscopic ultrasound (EUS) in patients with SIT also requires an accurate anatomical orientation within the mirror-image setting, with only a limited number of case reports published 2 4 5 . Herein, we present a case of EUS-guided gallbladder drainage (EUS-GBD) in a patient with SIT, highlighting the technical modifications employed to overcome these challenges.
An 85-year-old woman with SIT was referred for internalization of gallbladder drainage. She had previously undergone percutaneous transhepatic gallbladder drainage for cholecystitis caused by cystic duct obstruction secondary to hilar cholangiocarcinoma ( Fig. 1 and Fig. 2 ). EUS-GBD was performed with the patient in the prone position and the endoscopist standing on the right side of the table. Initially, the conventional mirror-image approach required the counter-clockwise rotation of the scope. However, this maneuver forced the endoscopist to extend the left hand away from the patient, resulting in an ergonomically compromised posture in which the endoscopist had to turn away from the patient. To address this issue, we deliberately rotated the scope counter-clockwise by 360 degrees to form a loop near the endoscopist’s hand. This technique allowed the EUS-GBD to be performed while maintaining a comfortable position facing the patient. In contrast to patients with normal anatomy, where the optimal visualization of the gallbladder from the duodenal bulb is typically achieved by slight scope withdrawal, the reversed anatomy in SIT renders the scope prone to slipping out, thereby precluding such maneuvers. Consequently, forward pressure had to be maintained throughout the procedure. Notably, loop formation contributed to scope stability, facilitating the successful placement of a 7Fr double-pigtail stent using the standard EUS-GBD technique ( Fig. 3 and Fig. 4 , Video 1 ).
Magnetic resonance cholangiopancreatographic images showing hilar biliary strictures and cystic duct obstruction secondary to hilar cholangiocarcinoma in an 85-year-old woman with situs inversus totalis.
Computed tomographic images obtained before percutaneous transhepatic gallbladder drainage showing a distended gallbladder with wall thickening, consistent with acute cholecystitis.
Endoscopic ultrasound-guided gallbladder drainage in situs inversus totalis. a Fluoroscopic and b endoscopic ultrasound images demonstrating the puncture of the gallbladder.
An abdominal radiograph showing the indwelling endoscopic ultrasound-guided gallbladder stent following the removal of the percutaneous drainage catheter.
Endoscopic ultrasound-guided gallbladder drainage in situs inversus totalis using a loop formation technique.Video 1
Endoscopy_UCTN_Code_TTT_1AS_2AH
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Venu RP Geenen JE Hogan WJERCP and endoscopic sphincterotomy in patients with situs inversus Gastrointest Endosc 1985313383404043687 10.1016/s 0016-5107(85)72220-1 · doi ↗ · pubmed ↗
- 2Nasser J Sarmini MT Vozzo CERCP and EUS technique in situs inversus totalis: preparing for a left-sided plot twist Video GIE 2022736737036238805 10.1016/j.vgie.2022.05.008PMC 9551618 · doi ↗ · pubmed ↗
- 3Ding B Wang J Wei X Efficacy and safety of ERCP in patients with situs inversus totalis: multicenter case series and literature review BMC Gastroenterol 20222249736451092 10.1186/s 12876-022-02593-3PMC 9714160 · doi ↗ · pubmed ↗
- 4Togliani T Pilati S Mantovani N Extrahepatic cholangiocarcinoma in a patient with situs inversus totalis diagnosed by endoscopic ultrasound Endoscopy 201345 E 229E 23023945923 10.1055/s-0033-1344327 · doi ↗ · pubmed ↗
- 5Luo S Wang LS Li DF Linear array endoscopic ultrasonography for a patient with situs inversus totalis Endoscopy 202355 E 412E 41336758627 10.1055/a-1990-0753 PMC 9911293 · doi ↗ · pubmed ↗