Rescue endoscopic ultrasound-guided hemostasis for massive gastric cancer bleeding after transcatheter arterial embolization
Hao Zhuang, Jialiang Huang, Duanmin Hu, Guilian Cheng

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
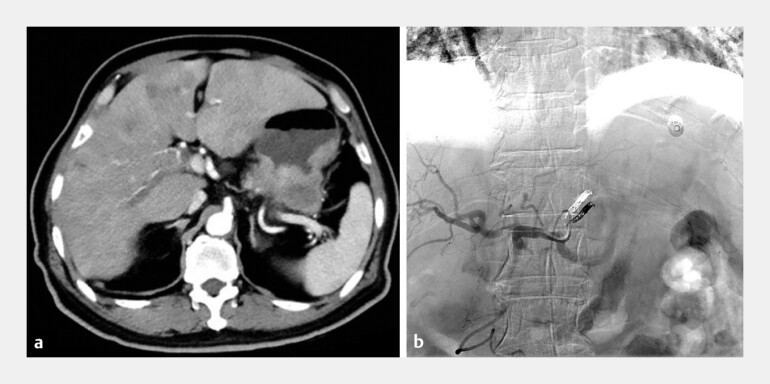 Fig. 1
Fig. 1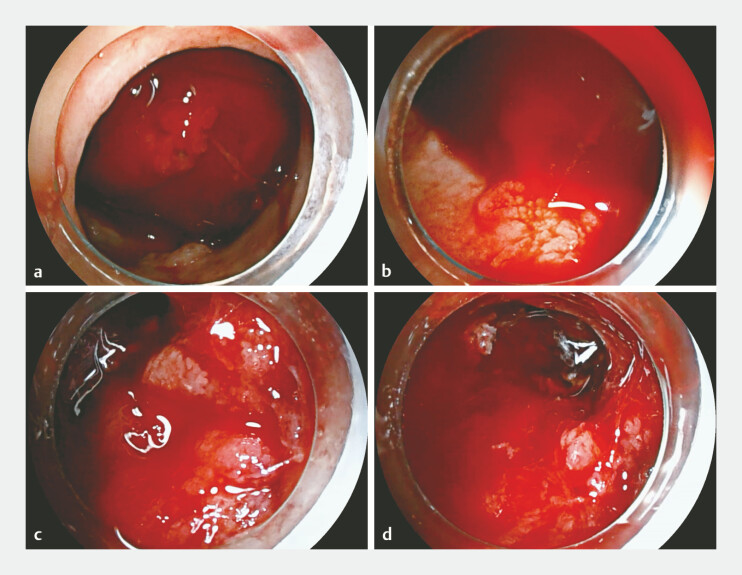 Fig. 2
Fig. 2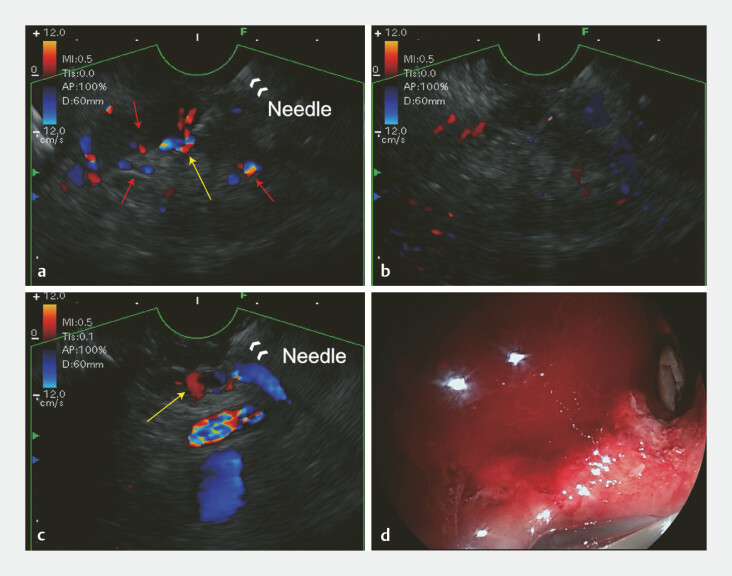 Fig. 3
Fig. 3- —Project of Suzhou Science and Technology Development Plan (Applied Basic Research – Medical and Health Technology Innovation)
- —Project of State Key Laboratory of Radiation Medicine and Protection
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastrointestinal Bleeding Diagnosis and Treatment · Vascular Anomalies and Treatments · Gastric Cancer Management and Outcomes
A 66-year-old man was admitted for massive gastrointestinal bleeding due to advanced gastric cancer with liver metastasis. He had undergone transcatheter artery embolization (TAE) of the left gastric artery for initial tumor hemorrhage 1 month prior ( Fig. 1 ). Given the poor efficacy of conventional endoscopic therapy to diffuse tumor bleeding 1 and the patient refused surgery, emergency endoscopic ultrasound (EUS)-guided hemostasis was performed after careful communication with the patient and his family.
Baseline clinical characteristics of the patient. a Enhanced computed tomography (CT) confirmed the tumor extending from the cardia to the gastric body with several slightly enhanced metastasis in the liver. b Digital subtraction angiography (DSA) post-TAE observed successfully occlusion in downstream of the left gastric artery. TAE, transcatheter artery embolization.
Under general anesthesia with tracheal intubation, esophagogastroduodenoscopy (EGD) was first performed and revealed a huge tumor extending from the cardia to gastric body, with active bleeding point distributing across the tumor base ( Fig. 2 ). A linear-array echoendoscope with color Doppler was then employed and observed multiple offending microvascular within submucosa. At the convergence point of these microvascular, a large vessel was identified as the dominant feeding vessel, providing major blood flow to the branches. Under EUS guidance, the feeding vessel was punctured with a standard 22-gauge needle. The intravascular location of the needle was confirmed by the injection of 0.5 mL of injection, followed by the administration of 1mL of cyanoacrylate, which resulted in the immediate disappearance of flow signals in the feeding vessel and its branches. Another large feeding vessel was identified at the gastric body and successfully embolized following the same procedure. After operation, repeat >EGD confirmed that no sustained bleeding occurred during 10-minute observation ( Fig. 3 , Video 1 ). The patient was discharged on postoperative day 8 without adverse events or complications. No recurrent bleeding occurred within 1 month follow-up.
Esophagogastroduodenoscopy (EGD) revealed diffuse active bleeding from the gastric tumor. a The huge tumor mixed with the blood clot occupied the whole gastric lumen. b – d Multiple active bleeding points distributed across the base of cancer.
EUS-guided cyanoacrylate injection for massive gastric cancer bleeding. a Color Doppler identified a feeding vessel (yellow arrow) providing blood to offending microvascular (red arrow) and EUS-guide cyanoacrylate injection was performed with a 22-gauge needle. b Blood flow signals of the feeding vessel and its branches immediately disappeared after injection. c Another feeding vessel (yellow arrow) was identified and successfully embolized with the same procedure. d No further active bleeding appeared during 10-minute EGD observation. ECD, esophagogastroduodenoscopy; EUS, endoscopic ultrasound.
EUS-guided cyanoacrylate injection for massive gastric cancer bleeding after TAE. EUS, endoscopic ultrasound; TAE, transcatheter artery embolization.Video 1
EUS-guided hemostasis reported success rates of 78–100% in nonvariceal refractory bleeding 2 3 . Han Chaoqun et al. reported a successful case of EUS-guided lauromacrogol injection for refractory gastric cancer bleeding 4 . To our knowledge, rescue EUS-guided hemostasis for massive gastric cancer recurrent bleeding after TAE have not been reported before.
Endoscopy_UCTN_Code_TTT_1AS_2AB
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mullady DK Wang AY Waschke KAAGA Clinical Practice Update on Endoscopic Therapies for Non-Variceal Upper Gastrointestinal Bleeding: Expert Review Gastroenterology 20201591120112810.1053/j.gastro.2020.05.09532574620 · doi ↗ · pubmed ↗
- 2Uribarri-González LPérez-Aguado G Arrubla Gamboa AEUS-guided therapy of nonvariceal refractory bleeding: A prospective observational study Endosc Ultrasound 20221133633710.4103/EUS-D-21-0016935708360 PMC 9526097 · doi ↗ · pubmed ↗
- 3De Angelis CG Cortegoso Valdivia P Rizza S Endoscopic Ultrasound-Guided Treatments for Non-Variceal Upper GI Bleeding: A Review of the Literature J Clin Med 2020986632245209 10.3390/jcm 9030866 PMC 7141529 · doi ↗ · pubmed ↗
- 4Han C Ling X Liu JA new therapy for refractory gastric cancer bleeding: endoscopic ultrasound-guided lauromacrogol injection Endoscopy 202254 E 151E 15210.1055/a-1398-519633862653 · doi ↗ · pubmed ↗