Handmade snare technique for grasping and repositioning biliary stents via the endoscopic ultrasound-guided hepaticojejunostomy route
Daisuke Namima, Hideki Kamada, Yoshio Shimizu, Naoki Fujita, Hiroki Yamana, Kiyoyuki Kobayashi, Hideki Kobara

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
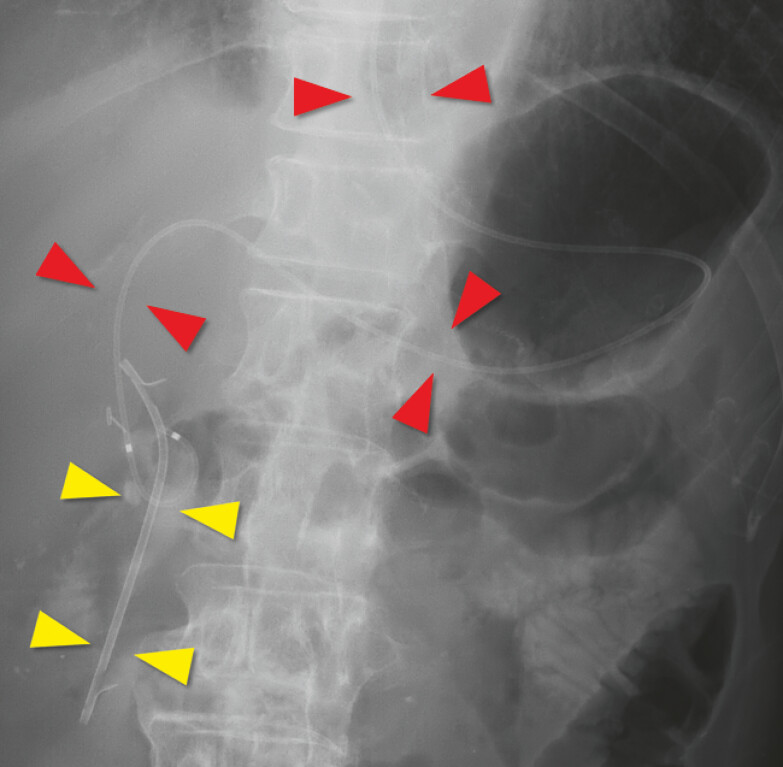 Fig. 1
Fig. 1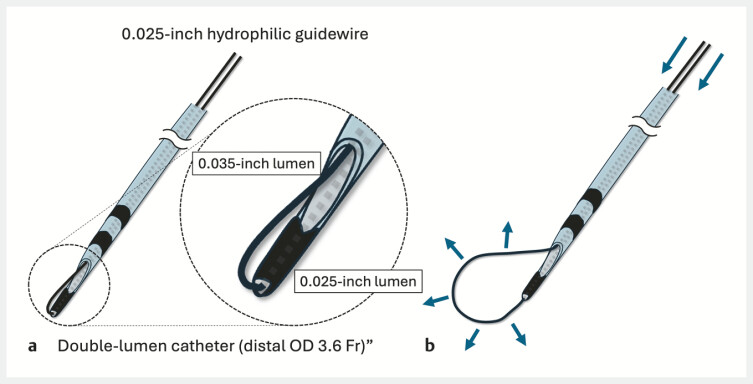 Fig. 2
Fig. 2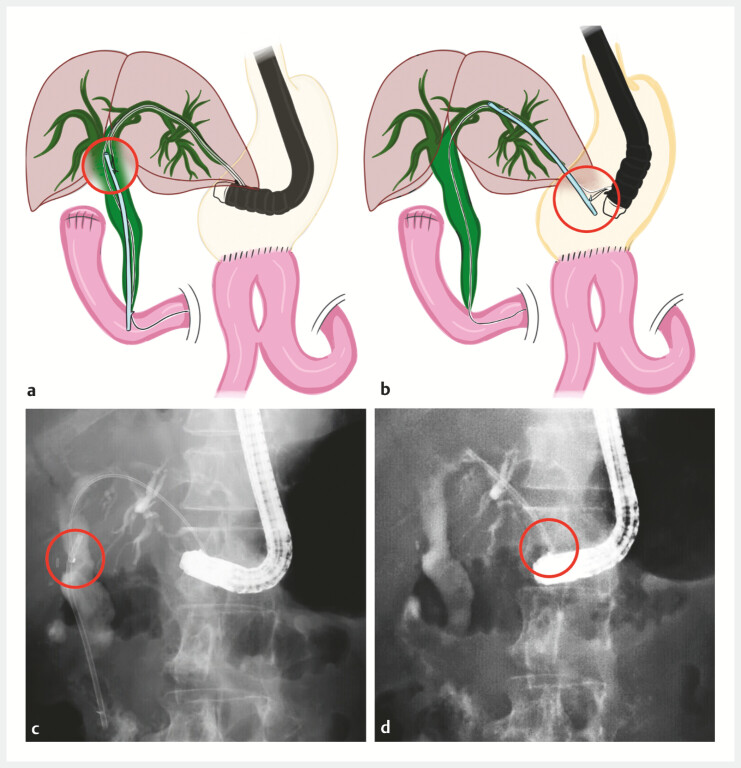 Fig. 3
Fig. 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGallbladder and Bile Duct Disorders · Organ Transplantation Techniques and Outcomes · Esophageal and GI Pathology
Endoscopic ultrasound-guided hepaticogastrostomy/hepaticojejunostomy (EUS-HGS/HJS) is an established alternative to endoscopic retrograde cholangiopancreatography (ERCP) in patients with surgically altered anatomy 1 2 . When combined with antegrade transpapillary stenting (AGS), dual-route biliary drainage can be secured 3 4 ; however, troubleshooting often requires balloon-assisted endoscopy.
A 65-year-old man with surgically altered anatomy and multiple comorbidities presented with septic shock due to choledocholithiasis-related cholangitis. Emergency EUS-HJS was performed to achieve rapid decompression because definitive stone extraction was not feasible at that time. A plastic stent was placed antegradely across the papilla (AGS), and an endoscopic nasobiliary drainage (ENBD) tube was added ( Fig. 1 ).
A fluoroscopic image showing an antegrade plastic stent placed across the papilla with its distal end in the duodenum (yellow arrowheads) and an endoscopic nasobiliary drainage tube traversing the endoscopic ultrasound-guided hepaticogastrostomy route (red arrowheads).
Two weeks later, ENBD cholangiography confirmed stone clearance, and internalization was planned because fistula maturation was uncertain and reintervention without balloon-assisted endoscopy was desirable at the receiving hospital; stent exchange via the HJS route was planned if cholangitis recurred. A standard guidewire was advanced via the ENBD and left in place as a rescue wire in case the stent migrated completely into the bowel; the ENBD tube was removed. A handmade snare was advanced through the HJS tract alongside the rescue wire. As previously reported 5 , the snare was constructed by inserting both ends of a 0.025-inch flexible hydrophilic guidewire commonly used for ERCP in Japan (Radifocus; Terumo, Japan) into the two lumens of a double-lumen catheter (Uneven Double Lumen Cannula; Piolax Medical Devices, Japan; distal outer diameter: 3.6 Fr). Due to the limited wire length, the proximal end of the catheter was cut to externalize both wire ends, creating a soft loop with the wire exiting from the two distal holes ( Fig. 2 ). The loop was used to grasp the stent flap and reposition the stent to the HJS anastomosis; patency was confirmed ( Fig. 3 , Video 1 ).
Schema of the handmade snare constructed from an uneven double-lumen catheter. a The two ends of a guidewire are inserted through the two lumens of the catheter to form a distal snare loop. The loop is kept closed so that it does not interfere with insertion. b Pushing the guidewires from the proximal side advances and opens the snare loop, forming a grasping device.
Repositioning a plastic stent via the endoscopic ultrasound-guided hepaticogastrostomy or hepaticojejunostomy (HGS/HJS) route using the handmade snare. In all panels, the grasping portion of the plastic stent is indicated by red circles. a Schema showing the distal end of the plastic stent across the papilla being grasped with the handmade snare advanced through the endoscopic ultrasound-guided HGS/HJS route. b Schema showing the plastic stent being pulled back and repositioned to the HGS/HJS anastomosis. c A fluoroscopic image corresponding to ( a ), showing grasping of the plastic stent with the handmade snare. d A fluoroscopic image corresponding to ( b ), showing the plastic stent relocated to the HGS/HJS anastomosis.
Handmade snare–assisted repositioning of an antegrade transpapillary plastic stent via the endoscopic ultrasound-guided hepaticojejunostomy (EUS-HJS) route, achieving internalization and preserving biliary access without balloon-assisted enteroscopy.Video 1
This HJS-based technique provides a simple approach for transpapillary stent management without the need for balloon-assisted endoscopy.
Endoscopy_UCTN_Code_CCL_1AF_2AF_3AB Endoscopy_UCTN_Code_TTT_1AR_2AZ
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Nakai Y Kogure H Isayama H Endoscopic Ultrasound-Guided Biliary Drainage for Benign Biliary Diseases Clin Endosc 20195221221910.5946/ce.2018.18830866611 PMC 6547351 · doi ↗ · pubmed ↗
- 2Jirapinyo P Lee LS Endoscopic Ultrasound-Guided Pancreatobiliary Endoscopy in Surgically Altered Anatomy Clin Endosc 20164951552910.5946/ce.2016.14427894187 PMC 5152780 · doi ↗ · pubmed ↗
- 3Ogura T Masuda D Imoto AEUS-guided hepaticogastrostomy combined with fine-gauge antegrade stenting: a pilot study Endoscopy 20144641642124573771 10.1055/s-0034-1365020 · doi ↗ · pubmed ↗
- 4Kumbhari V Tieu AH Khashab MAEUS-guided biliary drainage made safer by a combination of hepaticogastrostomy and antegrade transpapillary stenting Gastrointest Endosc 2015811015101610.1016/j.gie.2014.10.01925484328 · doi ↗ · pubmed ↗
- 5Kamada H Kobara H Kobayashi K Endoscopic retrieval of a migrated pancreatic stent using a handmade catheter with a guidewire loop Endoscopy 201951 E 7E 930406631 10.1055/a-0751-2569 · doi ↗ · pubmed ↗