Exploring psychiatrists’ perspectives on supporting parents with mental health Challenges: A mixed-methods study
Mireille Jasmin, Geneviève Piché, Aude Villatte, Andrea Reupert, Marie-Ève Clément, Anne Dorothee Müller, Marianne Fournier-Marceau, Darryl Maybery, Marie-Hélène Morin, Stéphane Richard-Devantoy, Gerard Hutchinson, Gerard Hutchinson, Gerard Hutchinson

TL;DR
This study explores how psychiatrists support parents with mental health issues and identifies barriers and facilitators to family-focused care.
Contribution
The study provides new insights into psychiatrists' practices and attitudes toward family-focused care for parents with mental illness.
Findings
Most psychiatrists are reluctant to provide family-focused support due to individual-focused care and stigma.
Facilitators include professional autonomy, personal experience, and confidence in family meetings.
Recommendations include training and guidelines to improve family-focused psychiatric care.
Abstract
Parenting responsibilities can be particularly challenging for patients receiving mental health services, often resulting in a range of negative impacts on children. Incorporating a family-focused approach into the usual care of parents with mental illness has been recommended to promote patient recovery while supporting the well-being of children and the entire family unit. This study aimed to document the family-focused practices undertaken by psychiatrists working with parents who have a mental illness and to explore potential facilitators and barriers to these practices. A sequential explanatory mixed-method design was used, combining an online survey and individual interviews. Family-focused practices were reported by 27 psychiatrists through the French version of the Family-Focused Mental Health Practice Questionnaire. Follow-up qualitative individual interviews were conducted…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
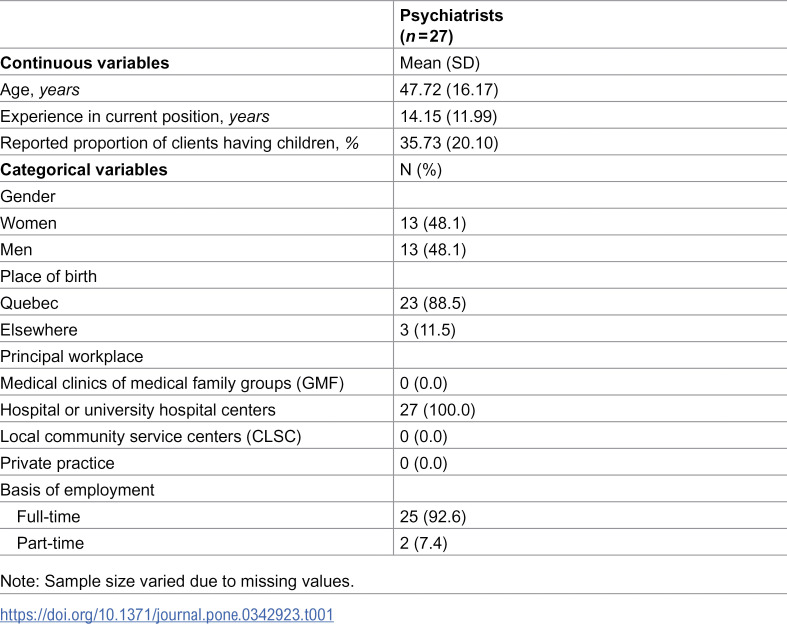 Figure 1
Figure 1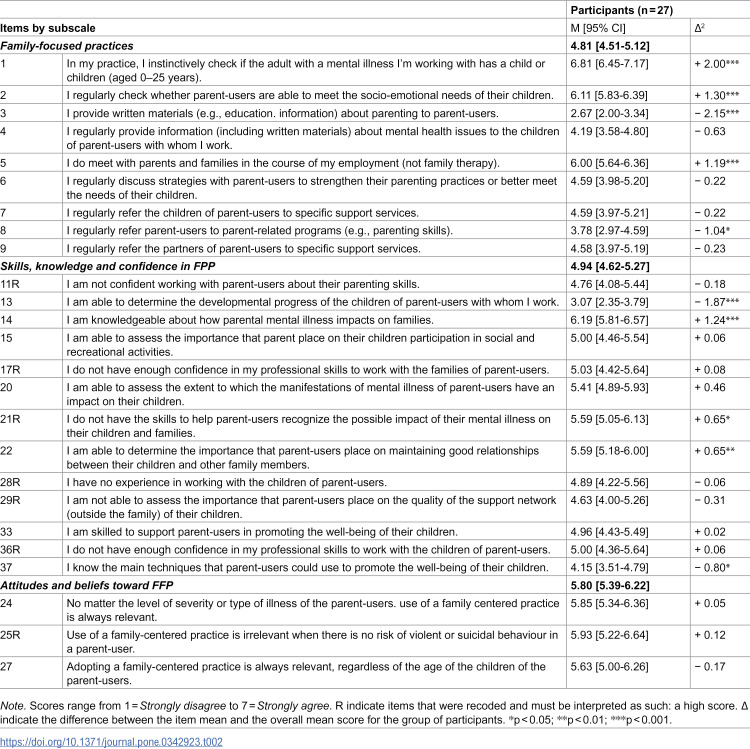 Figure 2
Figure 2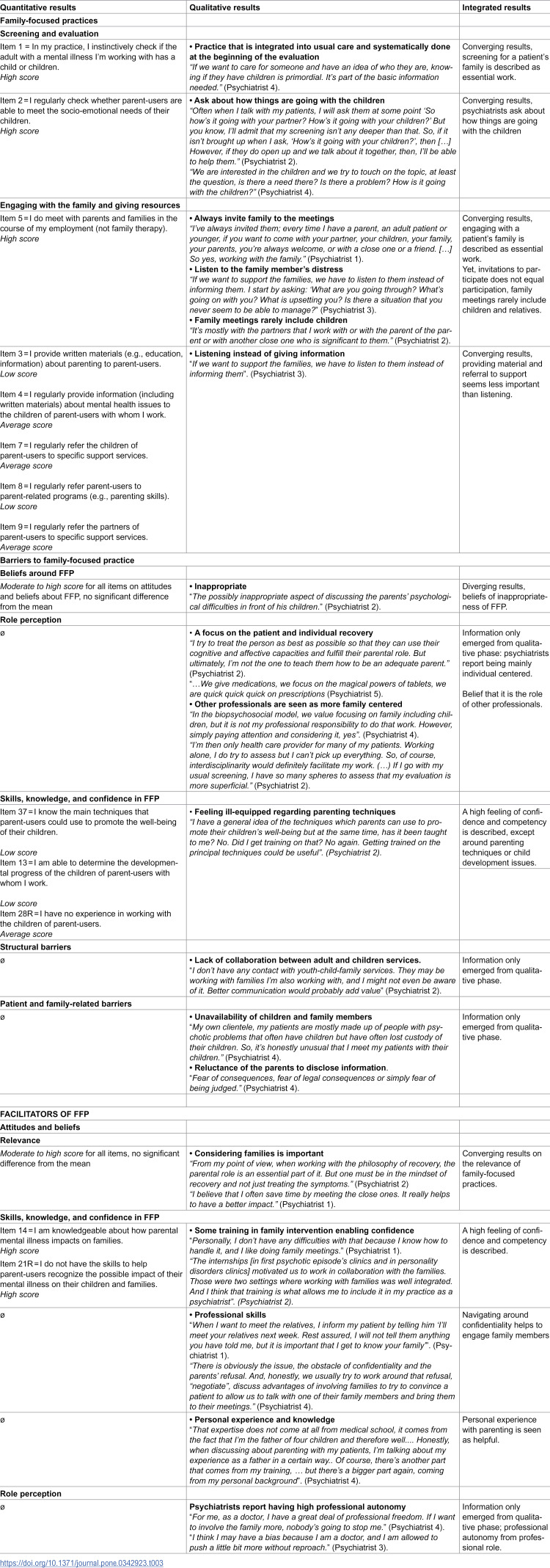 Figure 3
Figure 3- —http://dx.doi.org/10.13039/501100000155Social Sciences and Humanities Research Council of Canada
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMaternal Mental Health During Pregnancy and Postpartum · Family Caregiving in Mental Illness · Family Support in Illness
Background
Many psychiatric patients are parents, with estimates ranging from 20–38.5% in various services [1,2]. Thus, an important aspect of psychiatric care and recovery involves patients who are parents. The mental health of these parents affects not only themselves but also their children’s development and family well-being, often impairing parents’ ability to meet children’s emotional and educational needs [3]. Parents may experience guilt and concern about these impacts [4]. Identifying, acknowledging, and supporting patients’ parenting role is key to recovery, as embedding parenting into treatment encourages adherence to medication and motivates parents to “get better” for the sake of their children [5], while also boosting their confidence in parenting [6]. Parenthood also fosters identity, connectedness, and hope, crucial elements of recovery [7–9].
Children of parents with mental illness face increased risks of mental health issues [10–12] and psychosocial challenges [13]. They often take on caregiving responsibilities for their parents [14] while struggling with the emotional “rollercoaster” of their family life [15]. These children express a strong need to receive information from healthcare professionals about their parents’ conditions [16] and to discuss their experiences [17].
Thus, there is a need for a family-focused approach in mental health services that goes beyond treating adult patients alone by addressing the needs of the entire family. Family-focused practices emphasize a whole-family perspective, fostering collaborative partnerships, being family-centered, and supporting families in the care and development of individuals [18]. This approach promotes a systemic view, recognizing the reciprocal effects of symptoms on parenting and family functioning [19,20]. Such practices and family-oriented interventions have been shown to improve outcomes for individuals with mental illness, including reduced relapse and hospitalizations rates [21–23]. They also enhance parental efficacy [24], strengthen parent‒child relationships, promote resilience and coping in children [25–27] and reduce the risk of intergenerational transmission of mental illness [28].
Canadian policy frameworks increasingly emphasize family involvement in mental healthcare. The Mental Health Strategy for Canada (2019) encourages institutions to engage families in prevention, diagnosis, treatment, service planning, and evaluation. This represents a local and global shift toward a relational recovery model and a “family-centered” approach, in contrast to a traditional individualized, symptom-centered model of care [29]. However, the current mental healthcare system in Canada faces significant challenges, including long wait times, resource shortages, and disparities in access, particularly in rural and underserved areas. The separation between specialized mental health services and general primary care, as well as between child and adult services [30], has created barriers to providing timely, integrated care, which is considered a facilitator for adopting a more family-focused practice [31].
In collaboration with other professionals, psychiatrists, who play a central role in managing complex mental illnesses [32,33], are encouraged to involve families not only in treatment planning to support patient recovery but also in providing them with resources and support to help them cope with caregiving challenges [34]. Given the key role they play within mental health services [32,33], it is important to ascertain how psychiatrists support families in navigating mental health challenges. In two large-scale quantitative studies, psychiatrists reported providing higher levels of support to patients’ families and children than other professional groups [35,36], including providing information on mental illness to children, parenting advice to parents, and referral resources. However, findings from two qualitative studies reveal a more limited involvement. In Laser et al study (38), psychiatrists mainly addressed parenting concerns in two contexts: arranging child care arrangements during hospital admissions and discussing potential pregnancies in relation to psychiatric medication [37]. In Cognard & Wendland, psychiatrists acknowledged the importance of the mother‒child relationship, but focused primarily on assessing maternal mental health and caregiving capacity, rather than offering direct family support [38]. Across both studies, concerns about confidentiality, lack of training, and unclear protocols were cited as key barriers to engaging in family-focused practices.
In Canada, as elsewhere, addressing the needs of family members is considered essential [39]. Psychiatrists are well-positioned to offer this support, making their involvement a critical opportunity to better integrate family-focused care. However, few studies have explored how psychiatrists perceive their role in addressing the parenting needs of patients with mental illness and the strategies they might employ to support these families. Prior research highlights a discrepancy between psychiatrists’ self-reported levels of family support, as reported in quantitative studies, and the relatively limited, assessment-focused involvement observed in qualitative research. This discrepancy highlights the disconnect between what psychiatrists report in structured surveys and how they describe their involvement with families in qualitative interviews, which may also imply that quantitative and qualitative methods assess different facets of family-focused practices. Few studies have specifically examined psychiatrists’ practices. Most studies focus on other mental health professionals, such as nurses, pediatricians and family physicians [40–42]. This study aims to address these gaps by investigating first how psychiatrists in Quebec, Canada, support parents with a mental illness and their families, and second, the factors that encourage or hinder their engagement in family-focused practices. The findings will deepen our understanding of psychiatrists’ contributions to supporting families in navigating mental health challenges, with recommendations provided to strengthen family-focused approaches to psychiatric care.
Methods
This study used a sequential explanatory mixed-method design. This approach was used to develop a nuanced description and interpretation of the phenomenon, in which qualitative data further contextualize and enrich the quantitative results [43]. Phase I involved the completion of the Family-Focused Mental Health Practice Questionnaire (FFMHPQ-FR) [44], which aims to document psychiatrists’ family-focused practices. Phase II included individual interviews with selected Phase I participants to explore psychiatrists’ perspectives on their family-focused practices and the factors that support and hinder them. Phase III of this study sought to integrate the quantitative and qualitative data collected in Phases I and II. Guidelines for the Good Reporting of A Mixed Methods Study (GRAMMS) [45] were used.
This study was approved by the Research Ethics Board of the Université du Québec en Outaouais (#2021–1167) and the Comité d’Éthique de la Recherche Sectorielle en Santé des Populations et Première Ligne du CIUSSS de la Capitale-Nationale (# MP-13-2021-2135). All participants signed an online information and consent form before completing the online questionnaire and before participating in the interviews.
Recruitment
Recruitment for Phase I was conducted across all regions of the Province of Quebec, Canada, from 15/03/2021–08/02/2022. Various strategies were used (e.g., emails to managers of main workplaces and professional associations, advertisements on social media). Participants were required to meet the following criteria: 1) be psychiatrists; 2) currently work with adults with mental illness; 2) have direct contact with clients; and 3) be fluent in French. The only exclusion criterion was working exclusively with children with mental illness. Recruitment for Phase II took place from 15/06/2023–15/08/2023. A few months after Phase I, the psychiatrists who had participated in that phase were invited by email to take part in Phase II. Of the 27 psychiatrists contacted, five agreed to participate (two women and three men).
Participants
Twenty-seven psychiatrists completed the online survey (Table 1). Gender distribution was equal, and most participants (88.5%) were born in Quebec. The average age was 47.1 years (range 29–81), with an average of 14.2 years of experience (range 1–48). All psychiatrists worked in hospital settings (100.0%), providing second- or third-line services such as psychiatric emergencies, inpatient care, or outpatient clinics. On average, they estimated that 35.7% of their clients had parenting responsibilities (range: 5–75%), aligning with rates reported in similar contexts [46]. In Phase II, five participants took part in individual interviews (two women and three men), with ages ranging from 37 to 81 years and an average of 22 years of experience.
Table 1: Participants' sociodemographic and professional background characteristics.
Measures
The French version of the FFMHPQ [47] (FFMHPQ-FR) were used to measure psychiatrists’ practices, knowledge and confidence when working with families that have a parent with a mental illness. The FFMHPQ-FR, previously translated and validated, showed good psychometric properties [44]. The three subscales used in this study were 1) Family-focused practices; 2) professionals’ perceived skills, knowledge, and confidence; and 3) professionals’ attitudes and beliefs toward FFP. The participants rated their answers on a 7-point Likert scale (from 1 = strongly disagree to 7 = strongly agree). The questionnaire took 10–15 minutes to complete and included questions about participants’ professional background and work context (e.g., experience, workplace, and proportion of clients with children).
Semi-structured online interviews were conducted via Microsoft Teams using a guide developed from the research aims, Phase I preliminary results, and the literature. The interview guide (see Supplementary File) explored psychiatrists' experience working with parents with mental illness (e.g., What is it like for you to work with adults who have a mental illness and also have a parenting role? In your opinion, what is your role in accompanying parents with mental illnesses? How, if at all, is it different from working with adults who do not have children?). Interviews lasted 38–66 minutes (average, 47 minutes) and were audio-recorded.
Data analyses
Participants could choose “refuse to answer” or “not applicable”, which were coded as missing answers and treated with mean value imputation by item [48]. Across all 38 items, the rate of valid responses was 99.0%. Quantitative analysis was performed using SPSS 27 software (IBM Corp., 2020). Basic assumptions for the parametric techniques were verified (e.g., normal distribution) [49]. One sample t-tests compared item scores to subscale means, identifying items significantly above or below average. Higher scores indicated more family-focused practices or facilitating factors, whereas lower scores reflected fewer family-focused practices or hindering factors. Statistical significance was set at P < 0.05.
Qualitative data were analyzed using NVivo 14 through thematic content analysis, based on Braun and Clarke’s six phases [50]: familiarization, coding, theme generation, review, refinement, and reporting. Weekly team meetings ensured consensus on codes and themes.
Following the qualitative data analysis, three co-authors conducted an integration phase to combine the quantitative and qualitative findings. This process was presented via a joint display figure, which highlights new insights that go beyond those revealed by the quantitative and qualitative results individually.
Results
Quantitative findings
Table 2 presents the means and confidence intervals of the scores of the 27 psychiatrists regarding their level of family-focused practices, skills and knowledge, and attitudes toward family-focused practices. It also presents items that are significantly above and below the mean.
Table 2: Item-by-item analysis.
The results from the family-focused practices subscale showed large variability across items. Psychiatrists reported that they ‘agree’ to ‘strongly agree’ about checking if their patient has a child and checking if their patient can meet their children’s needs but reported that they ‘disagree’ to ‘slightly disagree’ in providing written materials about parenting to their patients.
The results regarding psychiatrists’ self-reported skills, knowledge, and confidence in family-focused practices also revealed variability. While psychiatrists generally agree that they are skilled and knowledgeable about the impact of parental mental illness on families and the importance of social support networks, they slightly disagreed about their knowledge of key techniques that patients could use to promote their children’s well-being and their own ability to assess the overall development of their children.
The items on the ‘Professionals’ attitudes and beliefs toward the FFP subscale did not vary significantly. Psychiatrists generally agreed on all the items pertaining to the relevance of family-focused practices.
Qualitative findings
The participants confirmed that screening for parental status was integrated into their usual care and was systematically performed, highlighting its significance as a source of information. Psychiatrists also described assessing parents’ capacity to respond to their children’s needs. Nonetheless, although they mentioned their willingness to address parenting concerns, this focus was underlined as limited, especially when parents were not actively engaging in or furthering discussions on their parenting role.
Psychiatrists also reported making concerted efforts to include family members in their sessions, particularly during evaluation meetings and discharge planning, and reported that part of their role was to listen to their patients’ relatives. At the same time, psychiatrists specified that family meetings rarely include children (Table 3).
Table 3: Integrative results from Phases I and II.
Barriers to family-focused practice
Some professionals expressed hesitation about involving children, citing concerns about the appropriateness of discussing parents’ psychological difficulties in their presence. This may reflect underlying beliefs about the unsuitability of family-focused approaches in such contexts, with discomfort rooted in confidentiality issues and the sensitive nature of psychiatric information.
Psychiatrists noted that other professional groups might be better suited for family-focused interventions, emphasizing that although they valued working with the family, “…it is not my professional responsibility to do that work’ (Psychiatrist 4). Most participants acknowledged their predominant focus on individual-centered care, which often took priority over broader family-oriented approaches.
While psychiatrists generally felt confident in their skills, many reported feeling ill-equipped and lacking specific training in discussing parenting techniques and child development, which they belief would be beneficial to improve their practice.
Participants also identified a significant structural barrier in the form of limited collaboration between adult and child services. This fragmentation hindered their ability to effectively refer patients’ children to appropriate support and constrained their understanding of the family’s broader needs.
Some barriers related to patients and their families were underlined. Several participants noted that they rarely met their patients' children, often due to the children’s unavailability because of school or because parents “have often lost custody of their children.” (Psychiatrist 4). Additionally, parental self-stigma emerged as a significant obstacle, with some psychiatrists reporting that patients were hesitant to disclose information about their children out of “fear of consequences, fear of legal consequences, or simply fear of being judged”. (Psychiatrist 4).
Facilitators of family-focused practice
Participants emphasized the importance of recognizing the parental role of their patients and involving families in patient care, highlighting the significant benefits of a family-focused approach. They reported feeling confident in their ability to work with patients’ families, attributing this in part to the training they had received.
Despite challenges related to patient reluctance to involve family members, psychiatrists identified several professional skills, such as negotiation, that helped them navigate and overcome parental hesitancy. Additionally, some participants noted that their own personal experience as parents enhanced their capacity to connect with and support other parents.
Professional autonomy also emerged as a key facilitator, providing psychiatrists with the flexibility to tailor their practice. As one psychiatrist remarked, “As a doctor, I have a great deal of professional freedom. If I want to involve the family more, nobody’s going to stop me” (Psychiatrist 4).
Discussion
This study explored how psychiatrists support parents with mental illness and the factors influencing their family-focused care. Results revealed moderate engagement in such practices, contrasting with previous studies reporting higher levels [35,36]. Nevertheless, our findings reveal considerable variability in psychiatrists’ support for patients and families, consistent with prior qualitative research [37].
Primarily, our results suggest that psychiatrists are generally proficient at identifying whether patients have children, an important finding given the commonly observed gaps in recording parental status within mental health services [51,52]. Recognizing parenting status is a fundamental first step in family-focused care and should be routinely integrated into intake assessments across mental health services [53].
However, psychiatrists in our study reported a limited or superficial focus on providing parenting support or directly engaging with patients’ children. While they recognized the value of involving family members, including children, this involvement was primarily seen as a means to improve symptom management and recovery, rather than to support the family’s understanding or coping with mental illness. This aligns with findings from a recent study of adults who grew up with a parent with mental illness, who felt they were “involved but not included” by professionals, serving as sources of information without sufficient support or inclusion in care decisions [54]. Similarly, psychiatrists here recognized the impact of parental mental illness on families but, consistent with Cognard and Wendland study [38], expressed low confidence in discussing parenting skills or assessing children’s developmental needs. Although most reported attempting to address children’s needs, such screening rarely extended beyond surface-level engagement.
Furthermore, although some psychiatrists invited family members to meetings, children were seldom included. This echoes results from studies involving various professionals, where concrete support for family members, especially children, was limited [2,52]. A Canadian study from two decades ago similarly found that while service providers acknowledged whole-family needs, few felt equipped to engage all family members effectively [55]. Cognard and Wendland (38) also highlighted a mother-centered approach shaped by limited skills and training, offering minimal direct support for family cohesion or parenting. Such gaps, widely noted among nonphysician professionals as well [56,57,58], underscore an urgent need for resources and training to better equip psychiatrists in addressing child development and parenting concerns during follow-up care for parents with mental illness.
Unlike other studies [36], psychiatrists in our sample did not identify service availability or workload as major barriers. Instead, they emphasized their professional autonomy and independence. Nevertheless, consistent with prior research [37], many expressed reluctance to discuss parental mental illness in front of children due to concerns about appropriateness and confidentiality. Other reasons for limited involvement with patients’ children included issues concerning children’s unavailability due to school schedules, loss of custody, parental self-stigma, and fear of possible legal consequences.
While some participants took pride in their skills and enjoyed conducting family meetings, others acknowledged their practice remained predominantly individual-centered. This narrow focus represents a significant gap, as addressing parenting can strongly motivate recovery, whereas ignoring parenting stress can harm overall well-being [59]. The emphasis on individual care, which overlooks family dynamics, likely reflects a structural barrier that fragments care between adult and child services rather than addressing the family unit holistically. Growing evidence supports integrated approaches, such as mother-baby units, that yield better outcomes for both parents and children [60,61]. Moreover, although psychiatrists are trained in the biopsychosocial model and recovery care, some feel that “other professionals may be better suited” to support patients’ families. As Linden noted [62], psychiatrist training often prioritizes psychopharmacology, with limited emphasis on therapeutic communication, complicating the integration of family support into psychiatric care.
Implications for practice
Previous research highlights challenges professionals face when discussing parenting and sensible issues with parents who have a mental illness and their families [63,64]. Although psychiatrists in our study routinely identified parenting status, many could benefit from additional training to build confidence and skills in addressing parenting concerns. This learnable skill [65] is essential for helping parents balance mental health and parenting responsibilities, ultimately improving outcomes for both parents and their children. Integrating specific family-focused strategies into clinical training would better equip psychiatrists to have these sensitive conversations, fostering a more supportive, inclusive environment for families. Evidence shows that training professionals in family-focused care like Let’s Talk about Children and The Parenting Well effectively enhances family-focused practices [59,66].
Moreover, acknowledging psychiatrists’ practice limitations underscores the need for a more integrated, multidisciplinary approach to address family issues comprehensively. Psychiatrists should collaborate closely with social workers, psychoeducators, psychologists, nurses and child welfare professionals. Such collaboration allows psychiatrists to concentrate on mental health treatment while ensuring the broader needs of families, especially children, are addressed. Some professionals, such as social workers, may be better positioned to offer direct support to children by responding to their needs, providing information, and engaging parents in their caregiving roles. Nonetheless, psychiatrists’ unique role in patient care requires them to remain actively involved in identifying parenting status, assessing parenting concerns, including family members in care plans, and making appropriate referrals to psychosocial or child services. The value of multidisciplinary, interagency, and collaborative care models for families coping with mental illness has been well documented [31,39].
To better support psychiatrists in engaging with families, especially in complex cases involving intersecting family challenges, mental health services could implement interagency family case consultation teams [31]. These teams, comprising experts from various areas (e.g., child services, adult services, community services, youth protection), may provide valuable insights into the complex dynamics families face. Research shows that such interprofessional and interagency support enhances practitioners’ confidence in supporting families, improves child safety perceptions, and leads to better clinical outcomes [5,31,67,68].
Strengths and limitations of the study
A key strength of this study is its focus exclusively on psychiatrists’ contributions to supporting families facing mental health challenges, a perspective not previously explored in depth. The mixed-methods design, integrating both qualitative and quantitative data, provides a comprehensive understanding of the topic. However, the study has limitations. The relatively small sample size and overrepresentation of older, more experienced psychiatrists, who typically report higher family-focused practices, may limit the generalizability of findings. Reliance on self-reported data and interviews also introduces potential social desirability bias. Future research could build on these findings by including patient perspectives and reviewing intake records to more objectively verify psychiatrists’ family-focused practices.
Conclusion
While psychiatrists recognize the importance of parenting in mental illness, many hesitate to offer comprehensive support due to barriers like individual-focused practice, stigma, consent challenges, and poor coordination between adult and child services. Facilitators such as professional autonomy, personal experiences, and confidence in conducting family meetings help promote family-focused care. To address these barriers, integrated multidisciplinary approaches and targeted training on parenting challenges and psychoeducation for children are needed. Equipping psychiatrists with these tools can foster family-inclusive care and improve outcomes for parents and their families.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Maybery D, Reupert AE. The number of parents who are patients attending adult psychiatric services. Curr Opin Psychiatry. 2018;31(4):358–62. doi: 10.1097/YCO.0000000000000427 29847344 · doi ↗ · pubmed ↗
- 2Ruud T, Maybery D, Reupert A, Weimand B, Foster K, Grant A, et al. Adult mental health outpatients who have minor children: prevalence of parents, referrals of their children, and patient characteristics. Front Psychiatry. 2019;10:163. doi: 10.3389/fpsyt.2019.00163 31001149 PMC 6456127 · doi ↗ · pubmed ↗
- 3Reupert AE, J Maybery D, Kowalenko NM. Children whose parents have a mental illness: prevalence, need and treatment. Med J Aust. 2013;199(3 Suppl):S 7-9. doi: 10.5694/mja 11.11200 25369850 · doi ↗ · pubmed ↗
- 4Hine RH, Maybery DJ, Goodyear MJ. Identity in recovery for mothers with a mental illness: A literature review. Psychiatr Rehabil J. 2018;41(1):16–28. doi: 10.1037/prj 0000215 27732035 · doi ↗ · pubmed ↗
- 5Stolper H, van Doesum K, Henselmans P, Bijl AL, Steketee M. The patient’s voice as a parent in mental health care: a qualitative study. Int J Environ Res Public Health. 2022;19(20):13164. doi: 10.3390/ijerph 192013164 36293747 PMC 9603497 · doi ↗ · pubmed ↗
- 6Moltrecht B, Lange AMC, Merrick H, Radley J. Whole-family programmes for families living with parental mental illness: a systematic review and meta-analysis. Eur Child Adolesc Psychiatry. 2024;33(9):3203–46. doi: 10.1007/s 00787-024-02380-3 38393370 PMC 11424744 · doi ↗ · pubmed ↗
- 7PichéG, Davidson G, Dunkley-Smith A, Grant A, Yates S, Maybery D. Exploring past research to move forward: a scoping review of aims, outcomes, and recommendations in parental mental illness qualitative research. Front Public Health. 2024;12:1427432. doi: 10.3389/fpubh.2024.1427432 39478750 PMC 11521813 · doi ↗ · pubmed ↗
- 8Hine RH, Maybery DJ, Goodyear MJ. Identity in Personal Recovery for Mothers With a Mental Illness. Front Psychiatry. 2019;10:89. doi: 10.3389/fpsyt.2019.00089 30906268 PMC 6418025 · doi ↗ · pubmed ↗