Emergency Department–Initiated Buprenorphine for Opioid Use Disorder: A Systematic Review of Treatment Engagement and Emergency Care Utilization
Mosab A Alabas, Abdulmajeed A Alshahrani, Saeed M Almobty, Ibrahim A Alaqeel, Mohammed S Alhomaidi, Mohammed S Alfuwis, Yasser A Alshammari, Laura M Damanhouri, Abdulmalek S Alyahya, Fawaz A Alshehri

TL;DR
Starting buprenorphine treatment for opioid addiction in emergency departments helps patients engage in ongoing care, but its effect on reducing emergency visits depends on social factors and support services.
Contribution
This study systematically reviews evidence on ED-initiated buprenorphine's impact on treatment engagement and ED use for opioid use disorder.
Findings
ED-initiated buprenorphine increases treatment engagement within 30 days compared to referral alone.
Impact on reducing ED return visits is mixed and context-dependent.
Social determinants and supportive services influence treatment outcomes.
Abstract
Emergency departments (EDs) represent a critical point of contact for individuals with opioid use disorder (OUD). Initiation of buprenorphine, a medication for OUD, in the ED has been proposed as a strategy to improve engagement in ongoing treatment and reduce recurrent emergency care utilization; however, evidence across these outcomes has not been comprehensively synthesized. This systematic review aimed to qualitatively summarize the effectiveness of ED-initiated buprenorphine in improving treatment engagement and reducing subsequent ED utilization among adults with OUD. A systematic search of major biomedical databases identified randomized and observational studies evaluating buprenorphine initiation in the ED and reporting outcomes related to treatment engagement or return ED visits. Data were extracted using a standardized approach, and methodological quality was assessed using a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
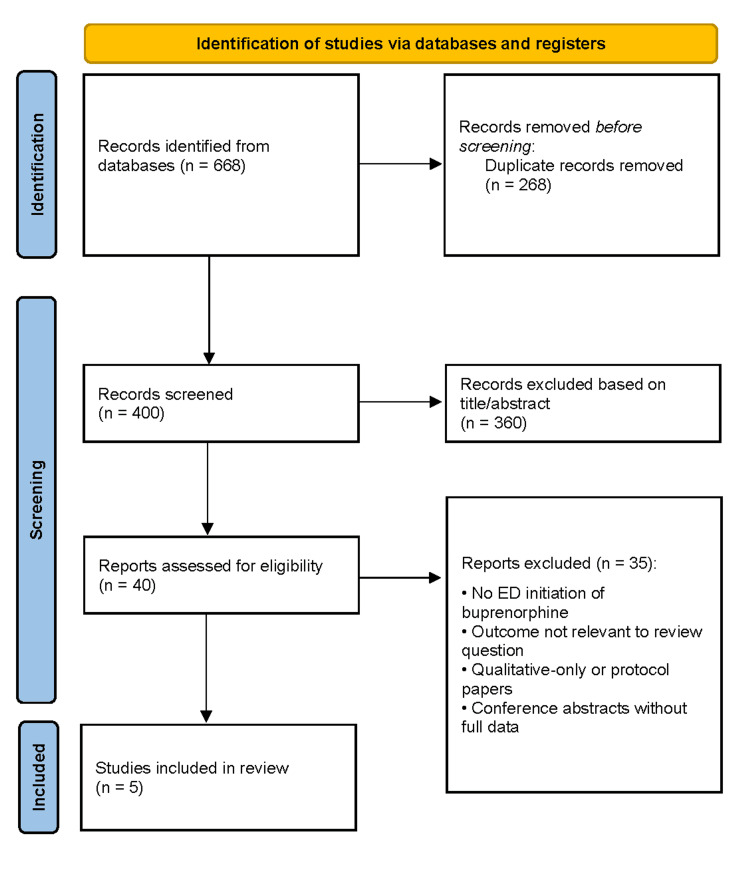 Figure 1
Figure 1| Study ID | Country | Study design | Setting (ED type / sites) | Population | Sample size | Inclusion criteria | Intervention (ED-initiated buprenorphine details) | Comparator/control | Follow-up duration | Primary outcome | Outcome type | 30-day ED return visits (Yes/No) | 30-day ED return visit data | 30-day treatment engagement (Yes/No) | 30-day treatment engagement data | Key quantitative results | Statistical analysis | Adjustments/confounders | Main conclusions | Limitations |
| Chambers et al. [ | USA | Retrospective cohort | Four EDs in Rhode Island | Adults treated in the ED for opioid overdose, not engaged in OUD treatment, were discharged home | 1,008 | ED-treated opioid overdose; not in OUD treatment at index visit; discharged home | Buprenorphine initiated in or from the ED (administered in ED or prescribed at discharge) | No buprenorphine initiation / other ED services | 30 days | Engagement in OUD treatment | Treatment engagement | No | Not reported | Yes | 146/1,008 (14%) | ED buprenorphine initiation associated with higher 30-day engagement (aOR 5.86; 95% CI 2.70–12.71) | Multivariable conditional logistic regression | Age, sex, race/ethnicity, insurance, calendar year, prior overdose, ED site | ED initiation is strongly associated with increased treatment engagement. | Observational design; low buprenorphine initiation rate; ED utilization not assessed |
| Kilaru et al. [ | USA | Retrospective cohort | Nationwide EDs (claims-based) | Adults treated in the ED for nonfatal opioid overdose, discharged home | 6,451 | ED visit for nonfatal opioid overdose; commercially insured; discharged home | Post-ED receipt of MOUD (buprenorphine or naltrexone); ED initiation not directly measured | No MOUD receipt | Up to 90 days | Receipt of OUD treatment | Treatment engagement | No | Not reported | Yes | 16.6% received OUD treatment | MOUD receipt uncommon; Black patients had a lower adjusted probability (ARD −5.9%) | Multivariable logistic regression with predictive margins | Age, sex, race/ethnicity, region, overdose type, prior mental health treatment | Engagement after overdose is low, with demographic disparities. | ED initiation not directly measured; limited to commercially insured patients |
| Skains et al. [ | USA | Retrospective chart review | Single urban academic ED | Adults discharged from the ED with a primary OUD diagnosis | 169 | ICD-10 OUD diagnosis; discharged from ED | Buprenorphine/naloxone prescribed at discharge (53.8%); often co-prescribed with naloxone | No buprenorphine prescription | 30 days, 90 days, 1 year | Repeat ED utilization | ED utilization | Yes | Opioid-related ED visits at 30 days lower (37.5% vs 62.5%, P=0.04); adjusted IRR 0.56 (95% CI 0.33–0.96) | No | Not reported | Reduced ED utilization at 30 days, sustained to 1 year | Bivariate analyses; Poisson regression | Age, domicile status | ED-initiated buprenorphine reduces repeat ED utilization. | Single center; outside-system visits not captured |
| D’Onofrio et al. [ | USA | Randomized controlled trial | Single urban academic ED | Adults with opioid dependence presenting to the ED | 329 | DSM-IV opioid dependence; not in treatment; medically stable | ED-initiated buprenorphine/naloxone with referral | Referral alone; brief intervention + referral | 30 days | Engagement in addiction treatment | Treatment engagement | Yes | No significant difference (P = .51) | Yes | 78% vs. 37% vs 45% | Significantly higher engagement and reduced illicit opioid use | χ² tests; mixed-model analyses | Randomization stratified by sex, cocaine use, opioid type | ED-initiated buprenorphine improves short-term engagement. | Single site; short follow-up; bundled intervention |
| Childers et al. [ | USA | Observational descriptive cohort | Single urban academic ED (California Bridge) | Adults with OUD identified in the ED | 210 | OUD; accepted referral for outpatient MAT | Buprenorphine in ED (80.8%); discharge prescription (67.6%); care navigation | No comparator | 30 days | Engagement in addiction treatment | Treatment engagement | No | Not reported | Yes | 95/210 (45.2%) | Housing status predicted engagement (aOR 2.49; 95% CI 1.20–5.20) | Univariable and multivariable logistic regression | Age, sex, race/ethnicity, housing, mental health, insurance | High engagement despite high homelessness. | No comparator; single center |
| Study ID | Reporting (10) | External validity (3) | Internal validity – bias (7) | Internal validity – confounding (6) | Power (1) | Total score (27) | Overall quality |
| Chambers et al. [ | 9 | 3 | 6 | 3 | 1 | 22 | Good |
| Kilaru et al. [ | 8 | 2 | 5 | 4 | 1 | 20 | Good |
| Skains et al. [ | 8 | 2 | 6 | 4 | 1 | 21 | Good |
| D’Onofrio et al. [ | 9 | 2 | 7 | 6 | 1 | 25 | High |
| Childers et al. [ | 8 | 2 | 5 | 4 | 1 | 20 | Good |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOpioid Use Disorder Treatment · Substance Abuse Treatment and Outcomes · HIV, Drug Use, Sexual Risk
Introduction and background
Opioid use disorder (OUD) remains a major public health challenge, with persistently high rates of opioid-related morbidity and mortality despite the availability of effective treatments [1]. Emergency departments (EDs) serve as a key point of contact for individuals with OUD, particularly during episodes of overdose or acute withdrawal [2]. Many patients rely on EDs for episodic care and experience frequent repeat visits due to poor linkage to ongoing treatment, contributing to fragmented care and increased strain on emergency services [3]. Reducing recurrent ED utilization among this population is therefore an important clinical and health system priority [4].
Buprenorphine is an evidence-based medication for the treatment of OUD that reduces illicit opioid use, overdose risk, and mortality [5]. Initiating buprenorphine during acute ED encounters offers a critical opportunity to engage patients at a time of heightened vulnerability and potential readiness for change [6]. Although regulatory, logistical, and educational barriers historically limited buprenorphine use in emergency settings, evolving policies and growing clinical experience have increasingly supported the feasibility of ED-initiated buprenorphine as a bridge to longitudinal addiction care [7].
Existing randomized and observational studies demonstrate that ED-initiated buprenorphine improves short-term engagement in addiction treatment compared with referral or brief intervention alone [8]. However, its impact on downstream healthcare utilization, particularly repeat ED visits, is less well defined. Recurrent ED presentations among individuals with OUD are common and are associated with higher healthcare costs, disrupted continuity of care, and increased risk of adverse outcomes, making ED return visits a clinically meaningful outcome when evaluating ED-based interventions [9].
Despite expanding implementation of ED-initiated buprenorphine programs, evidence regarding their effect on short-term ED utilization remains heterogeneous. Reported outcomes vary based on patient characteristics, availability of follow-up care, and the presence of adjunctive services such as naloxone distribution or peer support. In addition, differences in study design, outcome definitions, and follow-up duration complicate the interpretation of the existing literature [10].
This systematic review aims to critically examine and qualitatively synthesize available evidence on ED-initiated buprenorphine among patients with OUD, with a focus on treatment engagement and short-term ED return visits. By consolidating current findings, this review seeks to inform emergency clinicians, health system leaders, and policymakers about the effectiveness of ED-initiated buprenorphine as a strategy to improve care continuity and reduce recurrent ED utilization.
Review
Methodology
Literature Search Strategy
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [11]. A comprehensive electronic search was performed in PubMed, Scopus, Web of Science, and the Cochrane Library from database inception through the final search date. The search strategy combined controlled vocabulary and free-text terms related to ED care, buprenorphine or buprenorphine/naloxone initiation, and opioid use disorder, along with terms capturing treatment engagement and ED utilization outcomes. The initial search was developed in PubMed and adapted for each database to account for differences in indexing and syntax. Searches were limited to human studies and original research articles. Reviews, editorials, commentaries, protocols without outcome data, conference abstracts without full results, and clearly non-relevant publications were excluded.
Eligibility Criteria
Eligibility criteria were defined a priori using a population-intervention-outcome framework. Studies were included if they evaluated adult patients with OUD treated in an ED and assessed buprenorphine initiation during the ED visit or at discharge. Eligible studies were required to report post-ED outcomes, including engagement in addiction treatment, repeat ED visits, or related follow-up measures within a defined time frame. Randomized controlled trials and observational studies, including prospective or retrospective cohort designs and chart reviews, were eligible. Studies conducted in any geographic or clinical setting were considered. Exclusion criteria included studies not involving ED-initiated buprenorphine, those limited to non-ED settings, studies focused solely on provider attitudes or implementation without patient-level outcomes, qualitative-only studies, case reports, narrative reviews, and non-English publications.
Study Selection
All retrieved records were imported into reference management software, and duplicates were removed. Study selection was performed in two stages. First, titles and abstracts were screened to exclude clearly irrelevant studies. Second, full-text articles of potentially eligible studies were reviewed against predefined inclusion and exclusion criteria. Reasons for exclusion at the full-text stage were documented, and the selection process was summarized using a flow diagram to ensure transparency and reproducibility.
Data Extraction and Quality Appraisal
Data were extracted using a standardized, pilot-tested form. Extracted variables included study design, setting, population characteristics, sample size, intervention details, comparator conditions, follow-up duration, and reported outcomes related to treatment engagement and ED utilization. Methodological quality was assessed using a modified version of the Downs and Black checklist [12,13], a validated tool for evaluating both randomized and nonrandomized studies of healthcare interventions. The modified checklist assesses study quality across key domains, including reporting quality, external validity, internal validity related to bias, internal validity related to confounding, and statistical power, with a maximum possible score of 27 points. Higher scores indicate better methodological quality. Quality assessments were used to inform interpretation of findings and to highlight methodological strengths and limitations across the included studies, rather than as criteria for study exclusion.
Results
Study Selection
The database search yielded 668 records. After removal of duplicates, 400 unique records underwent title and abstract screening, of which 360 were excluded for lack of relevance, inappropriate study design, or absence of relevant outcomes. Forty full-text articles were reviewed in detail, and 35 were excluded due to lack of ED-initiated buprenorphine, absence of treatment engagement or utilization outcomes, qualitative-only designs, or insufficient data. Five studies met the inclusion criteria and were included in the qualitative synthesis and quality assessment (Figure 1) [1-5].
PRISMA flow diagram of study selectionPRISMA flow diagram illustrating the identification, screening, eligibility assessment, and inclusion of studies in the systematic review. The diagram details the number of records identified through database searching and other sources, records screened after removal of duplicates, full-text articles assessed for eligibility, and studies included in the final qualitative and/or quantitative synthesis, with reasons for exclusion at each stage.
Study Characteristics
All included studies were conducted in the United States and comprised one randomized controlled trial and four observational studies, including retrospective cohort studies and chart reviews. Study settings ranged from single urban academic EDs to multisite and nationwide claims-based analyses. Adult patients presenting with opioid overdose, dependence, or withdrawal were included, with sample sizes ranging from 169 to 6,451 participants. Most studies focused on patients not engaged in treatment at the index ED visit and discharged home. Follow-up periods ranged from 30 to 90 days, with one study assessing ED utilization outcomes up to one year. Interventions included ED-administered buprenorphine, buprenorphine or buprenorphine/naloxone prescriptions at discharge, and facilitated linkage to outpatient care. Comparators included referral-only approaches, brief interventions, or no comparator in descriptive cohorts. Primary outcomes were treatment engagement and repeat ED utilization (Table 1).
Quality Assessment
Methodological quality, assessed using the Modified Downs and Black checklist, ranged from good to high across studies, with total scores between 20 and 25 out of a possible 27. Reporting quality was consistently strong, and external validity was moderate to high. Internal validity related to bias and confounding was generally robust, particularly in the randomized trial [4], while observational studies demonstrated appropriate adjustment strategies. All studies met criteria for sufficient statistical power (Table 2).
Qualitative Synthesis
Across studies, ED-initiated buprenorphine was consistently associated with improved short-term engagement in OUD treatment. In the randomized trial, treatment engagement at 30 days was substantially higher among patients receiving ED-initiated buprenorphine compared with referral or brief intervention alone [4]. Observational studies reported similar trends, with buprenorphine initiation in or from the ED independently associated with higher odds of treatment engagement within 30 days [1,5]. Follow-up treatment rates varied across cohorts but were consistently higher among patients receiving buprenorphine during the ED encounter or at discharge [1,2,5].
Evidence regarding ED utilization outcomes was mixed. The randomized trial found no significant differences in ED use at 30 days between intervention groups [4]. By contrast, one observational study reported reduced opioid-related ED return visits at 30 days among patients prescribed buprenorphine, with adjusted analyses demonstrating reductions in all-cause ED visits at 30 days, 90 days, and one year [3]. Non-opioid-related ED visits appeared to be more strongly associated with demographic and social factors than with buprenorphine exposure [3].
Several studies evaluated the influence of adjunctive ED-based services. Behavioral counseling in the ED was associated with increased treatment engagement in one study, whereas referral alone and naloxone distribution were not [1]. Naloxone provision was associated with reduced opioid-related ED return visits in another study, independent of buprenorphine prescription [3]. Social determinants, including housing instability, insurance status, race, age, and sex, were consistently associated with disparities in treatment engagement and follow-up across studies, even after adjustment for clinical factors [1,2,5].
Limitations
This review has several limitations. The small number of eligible studies and substantial heterogeneity in study design, outcome definitions, and follow-up durations limited the ability to perform a quantitative meta-analysis and constrained direct comparisons across studies. Most included studies were conducted in academic EDs in the United States, which may limit generalizability to nonacademic, rural, or international settings. Variation in intervention components, comparator conditions, and availability of follow-up services further complicates the interpretation of observed effects. In addition, many studies were observational in nature and therefore subject to residual confounding and selection bias. Future research should prioritize standardized outcome measures, longer follow-up periods, and comparative evaluation of different ED buprenorphine delivery models, including extended-release formulations and structured warm-handoff programs. Rigorous assessment of equity-focused interventions is also needed to ensure that the benefits of ED-initiated buprenorphine are realized across diverse patient populations.
Conclusions
This systematic review demonstrates that ED-initiated buprenorphine is consistently associated with improved short-term engagement in treatment for OUD, particularly within the first 30 days after the index ED visit. Initiating buprenorphine in or from the ED appears more effective than referral-based or nonpharmacologic approaches alone in facilitating linkage to ongoing addiction care. By contrast, the effect of ED-initiated buprenorphine on subsequent ED utilization is less consistent and varies according to follow-up duration, outcome definitions, accompanying interventions, and social determinants of health. While some studies report reductions in opioid-related or all-cause return visits, these findings are not uniform across settings or time frames. Overall, the evidence supports ED-initiated buprenorphine as a key component of evidence-based care for OUD, while underscoring the importance of integrated care models that combine pharmacologic treatment with behavioral support, harm reduction strategies, and reliable outpatient follow-up to achieve sustained improvements in patient and health system outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1An evaluation of the association between specific post-overdose care services in emergency departments and subsequent treatment engagement J Am Coll Emerg Physicians Open Chambers LC Hallowell BD Samuels EA Daly M Baird J Beaudoin FL 04202310.1002/emp 2.12877 PMC 983328136643599 · doi ↗ · pubmed ↗
- 2Incidence of treatment for opioid use disorder following nonfatal overdose in commercially insured patients JAMA Netw Open Kilaru AS Xiong A Lowenstein M 03202010.1001/jamanetworkopen.2020.5852 PMC 725418232459355 · doi ↗ · pubmed ↗
- 3Impact of emergency department-initiated buprenorphine on repeat emergency department utilization West J Emerg Med Skains RM Reynolds L Carlisle N Heath S Covington W Hornbuckle K Walter L 101010172420233816518110.5811/westjem.60511 PMC 10754187 · doi ↗ · pubmed ↗
- 4Emergency department-initiated buprenorphine/naloxone treatment for opioid dependence: a randomized clinical trial JAMA D'Onofrio G O'Connor PG Pantalon MV 1636164431320152591952710.1001/jama.2015.3474 PMC 4527523 · doi ↗ · pubmed ↗
- 5Emergency department-initiated buprenorphine treatment in a population with a high rate of homelessness: an observational study J Emerg Med Childers R Castillo EM Cronin AO Swee S Lasoff D 1291356420233680643410.1016/j.jemermed.2022.12.004 · doi ↗ · pubmed ↗
- 6Opioid prescribing behavior in the emergency department during routine orthopedic manipulations Am Surg Medline A Wham R Kim G Staley C Steck A Boissonneault A Schenker ML 237623828920233552285110.1177/00031348221091957 · doi ↗ · pubmed ↗
- 7Continued opioid use and adverse events following provision of opioids for musculoskeletal pain in the emergency department: a systematic review and meta-analysis Drugs Chen Q Maher CG Han CS Abdel Shaheed C Lin CC Rogan EM Machado GC 152315358320233776854010.1007/s 40265-023-01941-1PMC 10624756 · doi ↗ · pubmed ↗
- 8Opioid and benzodiazepine use in the emergency department and the recognition of delirium within the first 24 hours of hospitalization J Psychosom Res Lee S Okoro UE Swanson MB Mohr N Faine B Carnahan R 11070415320223495904010.1016/j.jpsychores.2021.110704 PMC 9348903 · doi ↗ · pubmed ↗