Analgesic Strategies in Adult Intensive Care Units: A Systematic Review of Opioid and Non-opioid Approaches
Majed M Madkhali, Hussain M Al Qibti, Mohammed A Al-Arim, Muaid A Alfaifi, Maram M Fageehi, Ohoud M Masmali, Fawziah M Jali, Abdulelah Y Beati, Leena M Almobty, Moath A Alqanbar, Shaima M Alabdullah, Khaled A Hakami

TL;DR
This review compares opioid and non-opioid pain management strategies in adult ICU patients, finding that multimodal and non-GABA approaches improve outcomes and reduce complications.
Contribution
The study provides a systematic evaluation of analgesic and sedative strategies in adult ICUs, emphasizing non-GABA and multimodal approaches.
Findings
Dexmedetomidine improves sedation quality and reduces delirium compared to benzodiazepines and propofol.
Protocolized sedation strategies increase ventilator-free days and reduce ICU length of stay.
Multimodal approaches reduce opioid use and nausea while maintaining hemodynamic stability.
Abstract
Effective analgesia and sedation are critical components of care in adult intensive care units, with strategies ranging from opioid and non-opioid regimens to multimodal and protocol-guided approaches. This systematic review was conducted in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Evidence was synthesized from randomized controlled trials and observational studies across PubMed, Cochrane Library, Scopus, and Web of Science through October 2025, evaluating sedative and analgesic interventions - including opioid, non-opioid, alpha-2 agonist, and protocolized approaches - in adult intensive care unit (ICU) populations. The methodological quality of the chosen studies was assessed using the Modified Downs and Black checklist. A total of 11 eligible studies demonstrated that dexmedetomidine provided comparable or superior…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
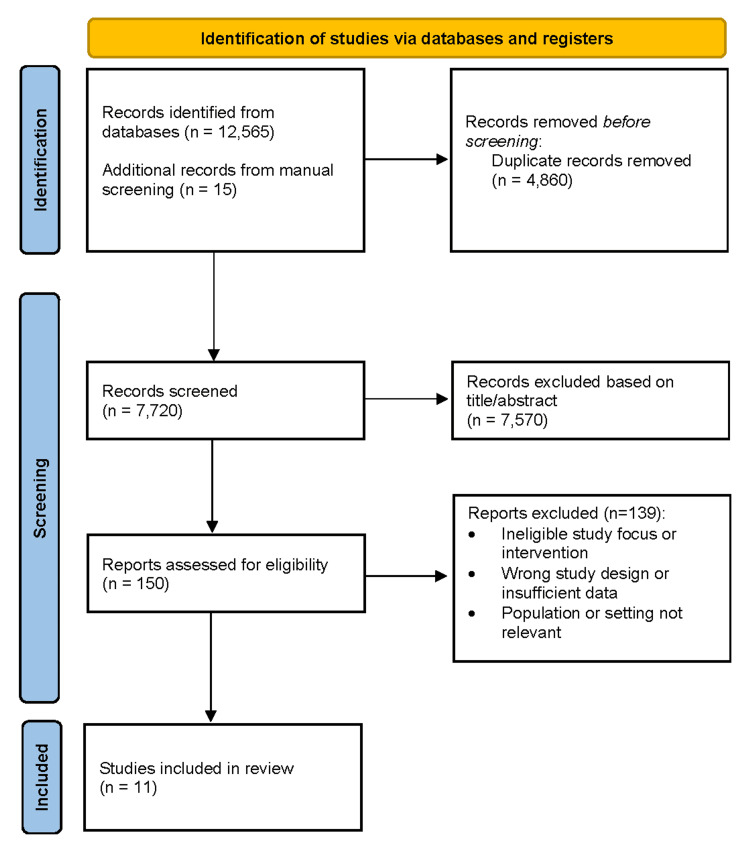 Figure 1
Figure 1| Author | Country / Setting | Study Design | Sample Size | Population Characteristics | Intervention (Type, Dose, Duration) | Comparator | Outcomes Measured | Key Findings / Results | Safety / Adverse Events |
| Burry et al. [ | Canada / 51 ICUs | Prospective, multicenter observational study | 712 mechanically ventilated adults (3,620 patient-days) | Critically ill adults on MV ≥24 h; median age 61; APACHE II ≈19.6; mixed medical-surgical | Observational data collection; recorded opioid, sedative, NMBD, antipsychotic use; sedation/pain/delirium assessment tools, protocols, DISs | None | Frequency/type/route of analgesics, sedatives, antipsychotics, NMBDs; secondary: assessment tool and protocol use, predictors | Opioid use 84.8% (fentanyl 54.3%, morphine 35%), sedatives 62.2% (midazolam most), antipsychotics 9.6%, NMBDs 18.3%, DIS 42%; predictors identified for drug/protocol use | Accidental device removal 4.6%; 75% during DIS; no major sedation-related AEs |
| Mehta et al. [ | Canada & USA / 16 tertiary ICUs | Multicenter RCT (SLEAP) | 423 analyzed (214 DIS + protocolized sedation, 209 protocolized sedation) | Mechanically ventilated adults expected ≥48 h; excluded cardiac arrest, TBI, NM blockade, palliative intent | Protocolized sedation + DIS: opioid/benzodiazepine titration to light sedation, daily stops | Protocolized sedation only | Time to successful extubation, ICU/hospital LOS, sedative/opioid doses, delirium (ICDSC ≥4), unintentional device removal, mortality, nurse workload | Median time to extubation 7 days both; ICU/hospital LOS similar; delirium ~53%; sedative/opioid use higher with DIS; nurse workload higher (VAS 4.22 vs 3.80, p=0.001) | Unintentional device removal similar (4.7% vs 5.8%); no increase in serious AEs; more agitation and sedative requirement with DIS |
| Su et al. [ | China / Peking University First & Third Hospitals | Randomized, double-blind, placebo-controlled clinical trial | 700 (350 DEX, 350 placebo) | Adults ≥65 yrs ICU post non-cardiac surgery; excluded neuro disorders, severe cardiac dysfunction, dialysis, coma | DEX 0.1 µg/kg/h IV continuous (~14–16 h); no loading dose | Placebo (normal saline) | Delirium incidence (CAM-ICU, days 1–7), time to extubation, ICU/hospital LOS, complications, 30-day mortality, pain (NRS), sleep, hemodynamics | Delirium 9% vs 23% (OR 0.35, p<0.0001); time to extubation 4.6 vs 6.9 h; ICU LOS 20.9 vs 21.5 h; non-delirium complications 15% vs 21%; improved pain and sleep (all p<0.001) | Bradycardia 17% vs 13% NS; hypotension 33% vs 26% NS; tachycardia lower (7% vs 14%, p=0.002); hypertension and hypoxemia lower; no sedation-related serious events |
| Riker et al. [ | Multinational / 68 ICUs (USA, Australia, Argentina, Brazil, New Zealand) | Prospective, double-blind RCT (SEDCOM) | 366 analyzed (244 DEX, 122 midazolam) | Adult medical/surgical ICU patients expected MV >24 h; mean age 62; APACHE II ≈19; 75% sepsis; excluded trauma, pregnancy, severe hepatic/cardiac disease | DEX 0.2–1.4 μg/kg/h IV up to 30 days; titrated to RASS −2 to +1; optional loading 1 μg/kg; fentanyl PRN | Midazolam 0.02–0.1 mg/kg/h IV; titrated to the same sedation target; fentanyl PRN | % time within RASS target, delirium prevalence/duration, MV duration, ICU LOS, nurse interaction, 30-day mortality | Sedation similar (77.3% vs 75.1%); delirium lower with DEX (54% vs 76.6%); time to extubation 3.7 vs 5.6 days; delirium-free days higher; communication improved | Bradycardia 42% vs 19% (5% required intervention); tachycardia less frequent; hypertension needing treatment less; infections lower; no rebound HTN or severe withdrawal |
| Jakob et al. [ | Europe / 44 ICUs (MIDEX), 31 ICUs (PRODEX) | Two multicenter, double-blind, phase 3 RCTs | MIDEX: 500 (249 Dex, 251 Midazolam); PRODEX: 498 (251 Dex, 247 Propofol) | Mechanically ventilated adults needing light–moderate sedation >24 h; excluded severe neuro disorders, bradycardia <50 bpm, high vasopressor need | DEX 0.2–1.4 µg/kg/h IV continuous; daily sedation stops, spontaneous breathing trials | MIDEX: Midazolam 0.03–0.2 mg/kg/h IV; PRODEX: Propofol 0.3–4 mg/kg/h IV | % time within target RASS, duration of mechanical ventilation, ICU/hospital LOS, pain communication, arousability (VAS), delirium (CAM-ICU), 45-day mortality | Sedation efficacy: Dex non-inferior; ventilation shorter vs midazolam (123 vs 164 h, p=0.03); extubation shorter vs both; improved patient communication; lower neurocognitive events vs propofol | Bradycardia higher with DEX (14% vs 5% midazolam, 3.7% vs 0.8% propofol); hypotension was higher vs. midazolam (20.6% vs 11.6%), similar vs. propofol; no increase in serious AEs overall |
| Reade et al. [ | Australia and New Zealand / 15 ICUs | Double-blind, multicenter RCT (DahLIA) | 71 analyzed (39 DEX, 32 placebo) | Mechanically ventilated adults with agitated delirium (CAM-ICU +, MAAS ≥5), ready for extubation but restrained; excluded dementia, TBI, α₂-agonist therapy | DEX 0.5 μg/kg/h IV, titrated 0–1.5 μg/kg/h to RASS −2 to +1; max 7 days; optional bolus | Placebo (normal saline); standard sedation/antipsychotics per clinician | Ventilator-free hours within 7 days, time to extubation, delirium resolution, ICU/hospital LOS, antipsychotic/sedative use, mortality | Ventilator-free hours 144.8 vs 127.5 h (Δ=17 h, p=0.01); time to extubation 21.9 vs 44.3 h; delirium resolution 23.3 vs 40 h; antipsychotic use less; opioid/propofol use reduced | Bradycardia 5% vs 0%; mild hypotension; rare agitation-related AEs; no increase in reintubation/self-extubation |
| Kawazoe et al. [ | Japan / 8 ICUs | Open-label, multicenter RCT (DESIRE Trial) | 201 (100 DEX, 101 Control) | Adult ICU patients with sepsis requiring MV ≥24 h; mean age 69 ± 14 yrs; 63% male; median APACHE II 23; 71% shock on admission | DEX 0.2–1.4 µg/kg/h IV; target RASS 0 (day) to −2 (night); additional agents as needed | No DEX; sedation with midazolam, propofol, fentanyl per protocol | 28-day mortality, ventilator-free days (VFDs), SOFA, ICU LOS, delirium/coma-free days, sedation quality, CRP, procalcitonin, renal outcomes | 28-day mortality 22.8% vs 30.8% (HR 0.69, p=0.20); VFDs 20 vs 18; sedation improved with DEX (17–58% vs 20–39%, p=0.01); subgroup APACHE II ≥23: lower mortality (HR 0.39, p=0.03) | Bradycardia 7% vs 2% (NS); mild hypotension; ACS 1% both; no serious sedation-related events |
| Pandharipande et al. [ | USA / Vanderbilt and Washington Hospital Center | Double-blind RCT (MENDS trial) | 103 analyzed (52 DEX, 51 lorazepam) | Adult medical/surgical ICU patients needing MV >24 h; median age 60; APACHE II 29; excluded severe neuro, alcohol withdrawal, hepatic failure | DEX 0.15–1.5 µg/kg/h IV up to 120 h; no loading dose | Lorazepam 1–10 mg/h IV | DCFDs, % time at target RASS, ventilator-free days, ICU/hospital LOS, 28-day and 12-month mortality, neurocognitive outcomes, costs | DCFDs 7 vs 3 (p=0.01); coma prevalence 63% vs 92%; target sedation 80% vs 67%; 28-day mortality 17% vs 27% | Bradycardia 17% vs 4% (one treated); hypotension similar; self-extubation 8% vs 4%; no hemodynamic compromise or severe toxicity |
| He et al. [ | China / Surgical ICU, Third Affiliated Hospital of Sun Yat-Sen University | Prospective single-center RCT | 120 (60 per group) | Adult ICU patients (18–80 yrs) with hepatic or renal dysfunction requiring fiberoptic bronchoscopy | Remimazolam besylate (initial 5 mg IV; 2.5 mg q15min × ≤5 if needed) | Propofol (1.5 mg/kg IV load; 0.5 mg/kg q15min × ≤5 if needed) | Sedation success, time to target sedation (RASS −3 to 0), recovery time, hemodynamic events, liver/renal function | Both groups achieved target sedation in ~5 min; remimazolam required fewer rescue doses (3.3% vs 16.7%, p=0.03); cumulative sedative dose was lower (5 mg vs 100 mg, p<0.001); recovery time was similar | Hypotension 3.3% vs 20% (p=0.01); bradycardia, tachycardia, hypoxemia not different; no severe adverse events |
| Smit et al. [ | Netherlands / 8 mixed medical–surgical ICUs | Multicenter, double-blind, placebo-controlled RCT | 132 (65 haloperidol, 67 placebo) | Adult ICU patients (mean 64 ± 15 yrs, 68% male) with delirium (CAM-ICU + or ICDSC ≥4); excluded neurological disease, dementia, psychosis | Haloperidol IV 2.5 mg q8h (1 mg if ≥80 yrs), titrated up to 5 mg q8h; duration up to 14 days | Placebo (IV saline) | Delirium- and coma-free days (DCFDs), secondary: sedative/antipsychotic use, agitation, self-extubation, mobility, sleep, 28-day mortality, post hoc: falls, hallucinations, memory, QoL | No difference in DCFDs (9 vs 9, aRR 0.98, p=0.87); haloperidol had less benzodiazepine use (57% vs 73%, aOR 0.41, p=0.03); trends toward fewer agitation events and falls (9% vs 27%, aOR 0.32, p=0.03) | Adverse events rare; QTc prolongation 5% vs 9%, arrhythmia 6% vs 2%, NS; slight BP drop after first dose (−12 mmHg, p=0.001); no extrapyramidal differences |
| de Wit et al. [ | USA / Virginia Commonwealth University Medical Center, Medical ICU | Prospective RCT | 74 (36 DIS, 38 SA) | Adult mechanically ventilated ICU patients; excluded severe neurocognitive dysfunction, tracheostomy, NM blockade | DIS until awake/agitated; resumed at half prior dose | SA: nurse-driven sedation algorithm (RASS −2 to −3) | Total duration of mechanical ventilation, 28-day ventilator-free days, ICU/hospital LOS, SOFA, sedation depth, agitation, sedative/analgesic use, mortality | SA reduced mechanical ventilation (3.9 vs 6.7 days, p=0.0003), ICU LOS (8 vs 15 days, p<0.0001), hospital LOS (12 vs 23 days, p=0.01); more ventilator-free days; DIS group had more agitation | Early hypertension, tachycardia, patient–ventilator asynchrony during DIS; more withdrawals due to agitation; no major drug-related AEs |
| Author | Reporting (0–10) | External Validity (0–3) | Internal Validity – Bias (0–7) | Internal Validity – Confounding (0–6) | Power (0–2) | Total (0–28) | Quality Level | Notes / Comments |
| Burry et al. [ | 9 | 3 | 6 | 4 | 2 | 24 / 28 | Good | Prospective observational multicenter Canadian ICU study. Strong data quality and generalizability; limited by observational design and potential confounding. |
| Mehta et al. [ | 10 | 3 | 7 | 6 | 2 | 28 / 28 | Excellent | SLEAP multicenter RCT of DIS + protocolized sedation. Strong internal validity, validated tools, and high statistical power. |
| Su et al. [ | 10 | 3 | 7 | 6 | 2 | 28 / 28 | Excellent | Large multicenter double-blind RCT; clear randomization, power analysis, and outcome definition. Reduced delirium observed with dexmedetomidine. |
| Riker et al. [ | 10 | 3 | 7 | 6 | 2 | 28 / 28 | Excellent | SEDCOM multicenter double-blind RCT (dexmedetomidine vs midazolam). Perfect reporting; large sample; validated outcomes; minimal bias. |
| Jakob et al. [ | 10 | 3 | 7 | 6 | 2 | 28 / 28 | Excellent | MIDEX/PRODEX phase-3 RCTs of dexmedetomidine vs midazolam/propofol. Methodologically outstanding; high power and strong internal validity. |
| Reade et al. [ | 10 | 3 | 7 | 5 | 2 | 27 / 28 | Excellent | DahLIA double-blind RCT adding dexmedetomidine to standard care for agitated delirium. High rigor; early stop slightly reduced power. |
| Kawazoe et al. [ | 10 | 3 | 6 | 5 | 2 | 26 / 28 | Good–Excellent | DESIRE open-label multicenter RCT in septic ICU patients. Robust design and outcomes but lack of blinding slightly reduces bias control. |
| Pandharipande et al. [ | 10 | 3 | 7 | 6 | 2 | 28 / 28 | Excellent | MENDS double-blind RCT (dexmedetomidine vs lorazepam). Excellent design, blinding, and validated delirium metrics (CAM-ICU). |
| He et al. [ | 10 | 3 | 7 | 5 | 2 | 27 / 28 | Excellent | High-quality RCT of remimazolam vs propofol for ICU bronchoscopy. Excellent reporting and design; minor limitation: no adjusted multivariate analysis. |
| Smit et al. [ | 10 | 3 | 7 | 6 | 2 | 28 / 28 | Excellent | EuRIDICE RCT of haloperidol for ICU delirium. Double-blind, multicenter, rigorous protocol. Early termination slightly reduced power, but internal validity remained strong. |
| de Wit et al. [ | 9 | 2 | 6 | 5 | 2 | 24 / 28 | Good | RCT comparing DIS vs nurse-driven algorithm. Well-reported but single-center, small sample, moderate generalizability. |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntensive Care Unit Cognitive Disorders · Anesthesia and Sedative Agents · Patient Safety and Medication Errors
Introduction and background
Effective analgesia and sedation are central to modern intensive care, shaping physiological stability, patient comfort, and clinical outcomes. Pain, agitation, and delirium frequently coexist in the intensive care unit (ICU), contributing to prolonged mechanical ventilation and increased morbidity [1,2]. Despite the availability of structured guidelines, substantial variation in practice persists, reflecting ongoing uncertainty about the optimal use of different analgesic and sedative agents [1].
Benzodiazepines and opioids have long been the foundation of ICU sedation and analgesia, yet prolonged exposure to these agents is associated with delirium, respiratory depression, and delayed recovery [3-10]. These concerns have driven a shift toward minimizing deep sedation and promoting early awakening, leading to increasing interest in newer sedatives and multimodal approaches that aim to provide cooperative sedation with fewer neurocognitive and hemodynamic complications [3-7,9].
Recent clinical trials have evaluated alternative agents and protocolized strategies designed to individualize analgesia and sedation. Agents such as dexmedetomidine, propofol, and remimazolam have been studied for their potential to reduce delirium and facilitate earlier extubation [3-9]. At the same time, nurse-driven algorithms, daily sedation interruption, and multimodal analgesic regimens incorporating non-opioid adjuvants have been adopted to reduce oversedation and limit opioid exposure [2].
However, evidence across studies remains heterogeneous, with inconsistent findings regarding effects on delirium, mechanical ventilation duration, ICU length of stay, and other key outcomes [1,3-10]. Differences in study design, patient characteristics, sedation targets, and outcome definitions further challenge interpretation and implementation in clinical practice [9]. Important gaps also remain in understanding how these pharmacologic strategies interact with the ICU environment, illness severity, and concurrent therapies [11].
Given these uncertainties, a comprehensive synthesis of current evidence is needed to clarify the relative effectiveness and safety of opioid and non-opioid analgesic and sedative strategies in critically ill adults. This systematic review evaluates their impact on pain control, delirium, sedation quality, duration of mechanical ventilation, recovery outcomes, and adverse events, to inform evidence-based clinical practice and identify priorities for future research [1-11].
Review
Methods
Literature Search Strategy
This systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [12]. A comprehensive search of PubMed, the Cochrane Library, Web of Science, and Scopus was conducted to identify studies evaluating analgesic and sedative strategies in adult ICU patients (Appendix). Searches included all available literature up to October 2025 and focused on outcomes such as pain control, delirium, sedation depth, duration of mechanical ventilation, recovery, and mortality.
The search strategy incorporated both Medical Subject Headings (MeSH) and free-text terms related to analgesia, sedation, critical care, adult populations, and common clinical outcomes. Equivalent search structures were adapted for each database. Searches were limited to English-language human studies and restricted to original research, including randomized controlled trials (RCTs), controlled clinical trials, and observational studies.
Eligibility Criteria
Study eligibility was defined using the Population-Exposure-Comparator-Outcome (PECO) framework [13]. Eligible studies included adults admitted to an ICU for medical or surgical conditions requiring analgesia, sedation, or mechanical ventilation. Exposures of interest included opioid-based or non-opioid regimens such as dexmedetomidine, propofol, benzodiazepines, haloperidol, remimazolam, and multimodal strategies. Studies were required to include a comparator group and report at least one clinically relevant outcome, including pain ratings, delirium incidence or duration, sedation adequacy, ventilator-free days, length of stay or mortality.
Eligible designs included RCTs, controlled clinical trials, and prospective observational studies. Studies were excluded if they involved pediatric populations; focused solely on perioperative or procedural sedation; lacked relevant clinical outcomes; or were review articles, case reports, conference abstracts, editorials, or animal studies. Only full-text publications in English were included.
Study Selection
All identified records were imported into EndNote (Clarivate, Philadelphia, PA) for organization and duplicate removal. Study selection occurred in two stages. First, two reviewers independently screened titles and abstracts based on the inclusion and exclusion criteria. Second, full-text articles of potentially eligible studies were reviewed in detail. Disagreements were resolved through discussion or consultation with a third reviewer.
Data Extraction and Quality Appraisal
Two reviewers independently extracted data using a standardized form. Extracted variables included study characteristics, patient demographics, type and dose of interventions, comparator regimens, and reported clinical outcomes such as sedation adequacy, delirium, mechanical ventilation duration, pain control, and recovery indicators. Differences in extraction were resolved by consensus, with third-reviewer arbitration when needed.
Methodological quality and risk of bias were assessed using the Downs and Black Checklist, which evaluates reporting quality, external validity, internal validity, and study power [14]. Studies were rated as excellent, good, fair, or poor based on their total score. Most included studies demonstrated high methodological quality, supporting reliable interpretation and synthesis of findings.
Results
Study Selection
Database searches identified 12,580 records, with an additional 15 records found through manual screening. After removal of duplicates, 7,720 unique studies were assessed by title and abstract, and 7,570 were excluded as irrelevant. Full texts of 150 articles were evaluated, resulting in 11 studies [1-11] that met all inclusion criteria. These studies demonstrated acceptable methodological quality and were included in the qualitative synthesis. The selection process is summarized in the PRISMA flow diagram (Figure 1).
PRISMA flow diagram of the study selection processThe flow diagram summarizes the selection of studies for inclusion in the systematic review following PRISMA recommendations [12]. It details the number of records identified, screened, and assessed for eligibility, as well as the studies included in the final analysis, with exclusions at each stage and corresponding reasons documented.
Characteristics of Included Studies
The 11 included studies consisted of nine RCTs, one prospective single-center trial, and one multicenter observational study conducted across multiple continents. Sample sizes ranged from 71 to 700 patients. Most studies enrolled adults requiring mechanical ventilation or postoperative monitoring in mixed medical-surgical ICUs, while others focused on subgroups such as sepsis [5], agitated delirium [4,7], or organ dysfunction [6]. Methodological rigor was generally high, with defined inclusion criteria, standardized sedation targets, and validated measures for sedation, delirium, and recovery (Table 1).
Interventions encompassed pharmacologic regimens and protocolized sedation strategies. Dexmedetomidine was evaluated in six major trials [3,4,6-8], and remimazolam in one study [9], typically compared with benzodiazepines or propofol under light-to-moderate sedation targets assessed by the Richmond Agitation-Sedation Scale (RASS). One study assessed haloperidol, an antipsychotic medication [10], and two examined protocol-based sedation: a nurse-implemented algorithm versus daily interruption [11] and protocolized sedation with or without daily interruption [2]. An observational study described real-world sedative, opioid, and antipsychotic use across Canadian ICUs [1].
Outcome measures included sedation quality, delirium incidence or duration, ventilator-free days, ICU or hospital length of stay, and adverse events [2,5]. Dexmedetomidine and remimazolam generally produced effective light sedation with favorable hemodynamic and cognitive profiles compared with γ-aminobutyric acid (GABA)-ergic sedatives [7,9]. Antipsychotics modestly reduced agitation without shortening delirium duration, while algorithm-based sedation shortened ventilation and ICU stay compared with daily interruption. Reported adverse events were mostly mild and related to drug dosing [2-8]. Overall, the included studies reflect a shift toward individualized, non-opioid, and protocol-guided sedation strategies aimed at reducing delirium and accelerating recovery [2-8].
Quality Assessment
Study quality assessed using the Modified Downs and Black Checklist ranged from 24 to 28, indicating good to excellent methodological rigor. Eight studies achieved an excellent rating, and three were rated good. Reporting quality was consistently high, with clear intervention descriptions and outcome definitions. External validity was strongest in large multicenter trials enrolling diverse ICU populations. Internal validity was robust in double-blind RCTs such as those by Su et al. [3], Jakob et al. [5], and Pandharipande et al. [8], whereas open-label designs [1,6] had moderate confounding risk. All studies demonstrated adequate statistical power with appropriate sample size calculations and prespecified endpoints, supporting confidence in the reliability of findings (Table 2).
Results on Pain and Sedation Quality
Both opioid and non-opioid regimens achieved effective sedation, but notable differences emerged in interaction quality and depth control. Dexmedetomidine consistently produced comparable or superior sedation to midazolam and propofol, with better communication and fewer episodes of coma or oversedation in SEDCOM and MIDEX/PRODEX [4,5], and more coma-free days than lorazepam in Pandharipande et al. [8]. Remimazolam provided equivalent sedation to propofol with faster onset, lower cumulative dose, and fewer hypotensive events [9]. Protocol-based sedation outperformed daily interruption; nurse-implemented algorithms resulted in less agitation and shorter ventilation than interruption alone [11], and protocolized sedation did not benefit from added interruption [2]. Real-world practice showed high opioid use but inconsistent sedation assessment across centers [1].
Results on Delirium Outcomes
Non-opioid α₂-agonist sedation showed consistent advantages in delirium reduction. Dexmedetomidine significantly decreased delirium incidence in postoperative elderly patients [3] and increased delirium-free days in multiple trials [4,5,8]. In agitated delirium, adjunctive dexmedetomidine accelerated symptom resolution and increased delirium-free time [7]. Antipsychotics showed mixed effects; haloperidol had no impact on delirium duration but reduced agitation and rescue benzodiazepine use [10].
Results on Recovery and Clinical Outcomes
Dexmedetomidine was associated with shorter time to extubation compared with midazolam and propofol in several studies [4,5,7]. However, mortality benefits were not demonstrated; in septic patients, dexmedetomidine did not reduce 28-day mortality or ventilator-free days overall, although benefits were suggested in patients with higher illness severity [6]. Protocolized sedation and antipsychotics showed neutral effects on length of stay or mortality [2,10]. Daily sedation interruption alone resulted in longer ventilation and higher mortality in one study [11]. Remimazolam provided efficient procedural recovery comparable to propofol [9].
Results on Safety and Adverse Effects
Adverse effects varied by drug. Dexmedetomidine caused predictable bradycardia and hypotension but fewer hypertensive or tachycardic episodes than conventional sedatives [4,5]. Low-dose prophylactic dexmedetomidine reduced hemodynamic instability without excess hypotension [3], and bradycardia was typically mild [6]. Remimazolam demonstrated lower hypotension rates than propofol and no organ toxicity [9]. Haloperidol was well tolerated with few serious events [10]. Protocol-based approaches did not introduce pharmacologic risks but were associated with agitation-related complications such as device removal in some cases [1,11].
Discussion
This systematic review summarizes contemporary evidence on analgesic and sedative strategies in adult intensive care units, highlighting a clear transition from traditional opioid- and benzodiazepine-heavy regimens toward multimodal, non-opioid, and protocol-guided approaches. Across the included studies, light and cooperative sedation emerged as a consistent theme associated with improved clinical trajectories, including reduced delirium, earlier liberation from mechanical ventilation, and better patient interaction without compromising safety.
Non-GABA-based sedatives, particularly alpha-2 agonists, demonstrated favorable sedation profiles characterized by greater arousability and fewer episodes of deep sedation or coma. These properties appear to support more effective neurological assessment and may facilitate participation in care processes such as spontaneous breathing trials and early mobilization. Remimazolam also showed promise as an alternative sedative, achieving adequate sedation with fewer hemodynamic disturbances in selected ICU settings. Together, these findings suggest that sedative choice plays an important role in balancing comfort, safety, and recovery.
Beyond pharmacologic selection, this review underscores the importance of how sedation is delivered. Protocolized and nurse-driven strategies were associated with more consistent sedation targeting and improved efficiency compared with approaches relying solely on daily sedation interruption. These results indicate that structured implementation, regular reassessment, and alignment of analgesia and sedation goals may be as important as the agents themselves in optimizing outcomes.
Several limitations should be acknowledged. The included studies were heterogeneous in terms of patient populations, clinical settings, sedation targets, and outcome definitions, limiting direct comparison and precluding quantitative meta-analysis. Some trials focused on specific subgroups, such as postoperative or septic patients, which may affect generalizability. In addition, long-term outcomes, including cognitive function and quality of life after ICU discharge, were not consistently evaluated.
Conclusions
This review highlights a clear shift in ICU practice away from deep benzodiazepine-based sedation toward multimodal, non-opioid, and protocol-guided strategies. Among available agents, dexmedetomidine offers the strongest evidence for improving sedation quality, reducing delirium, and accelerating recovery while maintaining a favorable safety profile. When combined with structured pain and sedation protocols, these approaches can meaningfully improve patient outcomes and ICU efficiency. Future research should prioritize long-term cognitive outcomes, economic impact, and integration of non-pharmacologic therapies to further optimize comfort and recovery in critically ill adults.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Analgesic, sedative, antipsychotic, and neuromuscular blocker use in Canadian intensive care units: a prospective, multicentre, observational study Can J Anaesth Burry LD Williamson DR Perreault MM 6196306120142478856410.1007/s 12630-014-0174-1 · doi ↗ · pubmed ↗
- 2Daily sedation interruption in mechanically ventilated critically ill patients cared for with a sedation protocol: a randomized controlled trial JAMA Mehta S Burry L Cook D 1985199230820122318050310.1001/jama.2012.13872 · doi ↗ · pubmed ↗
- 3Dexmedetomidine for prevention of delirium in elderly patients after non-cardiac surgery: a randomised, double-blind, placebo-controlled trial Lancet Su X Meng ZT Wu XH 1893190238820162754230310.1016/S 0140-6736(16)30580-3 · doi ↗ · pubmed ↗
- 4Dexmedetomidine vs midazolam for sedation of critically ill patients: a randomized trial JAMA Riker RR Shehabi Y Bokesch PM 48949930120091918833410.1001/jama.2009.56 · doi ↗ · pubmed ↗
- 5Dexmedetomidine vs midazolam or propofol for sedation during prolonged mechanical ventilation: two randomized controlled trials JAMA Jakob SM Ruokonen E Grounds RM 1151116030720122243695510.1001/jama.2012.304 · doi ↗ · pubmed ↗
- 6Effect of dexmedetomidine added to standard care on ventilator-free time in patients with agitated delirium: a randomized clinical trial JAMA Reade MC Eastwood GM Bellomo R 1460146831520162697564710.1001/jama.2016.2707 · doi ↗ · pubmed ↗
- 7Effect of dexmedetomidine on mortality and ventilator-free days in patients requiring mechanical ventilation with sepsis: a randomized clinical trial JAMA Kawazoe Y Miyamoto K Morimoto T 1321132831720172832241410.1001/jama.2017.2088 PMC 5469298 · doi ↗ · pubmed ↗
- 8Effect of sedation with dexmedetomidine vs lorazepam on acute brain dysfunction in mechanically ventilated patients: the MENDS randomized controlled trial JAMA Pandharipande PP Pun BT Herr DL 2644265329820071807336010.1001/jama.298.22.2644 · doi ↗ · pubmed ↗