Lipid-lowering medication reduces more target lesion than non-target lesion revascularizations: a cohort study
Elina Mantyniemi, Mitja Laaperi, Pasi Karjalainen, Juha Sinisalo

TL;DR
Long-term follow-up shows that statin use reduces repeat procedures at the original stent site more than new sites in heart disease patients.
Contribution
Identifies statin adherence as a factor reducing target lesion revascularization more effectively than non-target lesion revascularization.
Findings
Statin adherence lowers odds of target lesion revascularization compared to non-target lesion revascularization.
Diabetes and longer stent length increase odds of target lesion revascularization.
Target lesions occurred earlier than non-target lesions during follow-up.
Abstract
Factors related to the very long-term progression of atherosclerosis after stent implantation remain unclear. To define factors predicting disease progression as either target lesion (TL) or a new site target lesion (NTL) coronary stenosis. In a tertiary hospital, between June 2006 and March 2008, a prospective cohort registry of consecutive patients assigned to a coronary angiogram (n = 5294) was collected. Patients who underwent percutaneous coronary stenting (n = 1970 patients) were followed for ten years. Of them (1335/67.8%) had acute coronary syndrome (ACS) and (635/32.2%) chronic coronary syndrome (CCS). New ischemic lesions were categorized as TL or NTL. During a median of 9.5 years follow-up, 639 (32.4%) patients had a cardiovascular event, including 253 (12.8%) cardiovascular deaths. Repeat percutaneous coronary interventions were more frequent in CCS than in ACS patients…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
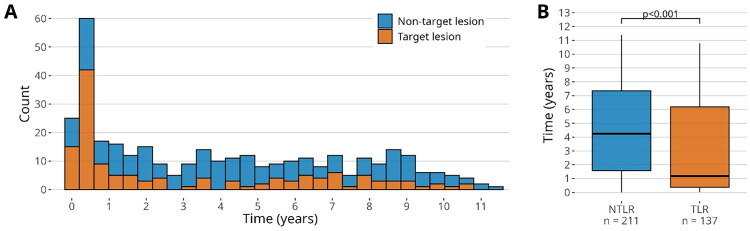 Figure 1
Figure 1| Variable | All | ACS | CCS | |
|---|---|---|---|---|
| Age | 64.8 (56.2–73.8) | 64.0 (55.6–73.8) | 65.8 (57.8–73.9) | 0.021 |
| Sex (women) | 624 (31.7%) | 422 (31.6%) | 202 (31.8%) | 0.970 |
|
| ||||
| Diabetes | 366 (18.6%) | 201 (15.1%) | 165 (26.0%) | <0.001 |
| Dyslipidaemia | 1393 (70.7%) | 850 (63.8%) | 543 (85.5%) | <0.001 |
| Hypertension | 1282 (65.1%) | 836 (62.6%) | 446 (70.2%) | 0.001 |
| Peripheral vascular disease | 138 (7.0%) | 88 (6.7%) | 50 (7.9%) | 0.373 |
| Atrial fibrillation | 102 (5.2%) | 89 (6.7%) | 13 (2.0%) | <0.001 |
| Previous PCI | 256 (13.0%) | 112 (8.4%) | 144 (22.7%) | <0.001 |
| Smoking: Current | 607 (30.8%) | 471 (35.6%) | 136 (21.4%) | <0.001 |
| Smoking: Previous | 641 (32.5%) | 389 (29.4%) | 252 (39.7%) | <0.001 |
|
| ||||
| none | 627 (31.8%) | 2 (0.1%) | 625 (98.4%) | <0.001 |
| STEMI | 577 (29.3%) | 577 (43.2%) | ||
| NSTEMI | 624 (31.7%) | 619 (46.4%) | 5 (0.8%) | |
| UAP | 142 (7.2%) | 137 (10.3%) | 5 (0.8%) | |
|
| ||||
| Triglycerides mmol/L | 1.20 (0.91–1.67) | 1.21 (0.93–1.68) | 1.16 (0.87–1.67) | 0.056 |
| Lp(a) mg/L | 9.9 (4.9–23.1) | 10.3 (5.2–22.9) | 9.4 (4.6–25.2) | 0.243 |
| HDL mmol/L | 1.18 (1.01–1.40) | 1.16 (1.01–1.37) | 1.21 (1.02–1.47) | 0.014 |
| LDL mmol/L | 2.82 (2.20–3.49) | 3.03 (2.43–3.67) | 2.46 (1.99–3.03) | <0.001 |
| Cystatin C mg/L | 1.21 (1.03–1.47) | 1.18 (1.00–1.45) | 1.25 (1.07–1.51) | <0.001 |
| NT-proBNP ng/L | 406 (152–1258) | 644 (226–1716) | 217 (109–528) | <0.001 |
|
| ||||
| BMS | 1267 (64.3%) | 918 (82.7%) | 349 (73.6%) | |
| DES | 249 (12.6%) | 152 (13.7%) | 97 (20.5%) | <0.001 |
| BMS and DES both | 68 (3.5%) | 40 (3.6%) | 28 (5.9%) | |
| Average stent length in mm | 18 (12–24) | 18 (15–24) | 20 (12–28) | 0.545 |
| | ||||
| during 1st year | 1518 (77.1%) | 1025 (76.8%) | 493 (77.6%) | 0.714 |
| overall adherence | 1146 (58.2%) | 747 (56.0%) | 399 (62.8%) | 0.004 |
|
| ||||
| during 1st year | 1278 (64.9%) | 884 (66.2%) | 394 (62.0%) | 0.078 |
| overall adherence | 1210 (61.4%) | 824 (61.7%) | 386 (60.8%) | 0.727 |
|
| ||||
| Death | 635 (32.2%) | 425 (31.8%) | 210 (33.1%) | 0.619 |
| CV-Death | 253 (12.8%) | 165 (12.4%) | 88 (13.9%) | 0.391 |
| CV-event | 530 (26.9%) | 364 (27.3%) | 166 (26.1%) | 0.637 |
| Stroke | 216 (11.0%) | 144 (10.8%) | 72 (11.3%) | 0.772 |
| Myocardial infarction | 364 (18.5%) | 252 (18.9%) | 112 (17.6%) | 0.549 |
|
| ||||
| TL-Restenosis | 137 (39.4%) | 85 (41.7%) | 52 (36.1%) | 0.351 |
| NTL-stenosis | 212 (60.7%) | 119 (58.3%) | 92 (63.9%) | 0.312 |
| CABG | 14 (0.7%) | 13 (1.0%) | 1 (0.2%) | 0.084 |
| Variable | NTL and TL | NTL | TL | |
|---|---|---|---|---|
| Age | 64.0 (55.4–71.9) | 63.0 (55.1–71.6) | 65.1 (56.1–72.9) | 0.396 |
| Sex (women) | 103 (29.5%) | 59 (27.8%) | 44 (32.1%) | 0.461 |
|
| ||||
| Diabetes | 81 (23.2%) | 42 (19.8%) | 39 (28.5%) | 0.082 |
| Dyslipidaemia | 253 (72.5%) | 158 (74.9%) | 95 (69.3%) | 0.313 |
| Hypertension | 238 (68.2%) | 148 (69.8%) | 90 (65.7%) | 0.491 |
| Peripheral vascular disease | 31 (8.9%) | 14 (6.6%) | 17 (12.4%) | 0.095 |
| Atrial fibrillation | 13 (3.7%) | 5 (2.4%) | 8 (5.8%) | 0.165 |
| Smoking: Current | 96 (27.5%) | 61 (28.9%) | 35 (25.5%) | 0.369 |
| Smoking: Previous | 129 (37.0%) | 72 (34.1%) | 57 (41.6%) | |
|
| ||||
| none | 138 (39.5%) | 90 (42.5%) | 48 (35.0%) | 0.266 |
| STEMI | 76 (21.8%) | 47 (22.2%) | 29 (21.2%) | |
| NSTEMI | 107 (30.7%) | 62 (29.2%) | 45 (32.8%) | |
| UAP | 28 (8.0%) | 13 (6.1%) | 15 (10.9%) | |
|
| ||||
| Triglycerides mmol/L | 1.23 (0.93–1.76) | 1.25 (0.96–1.85) | 1.17 (0.88–1.68) | 0.075 |
| Lp(a) mg/L | 11.5 (5.6–32.5) | 11.9 (6.0–35.6) | 10.1 (5.3–24.6) | 0.291 |
| HDL mmol/L | 1.17 (1.00–1.40) | 1.15 (0.98–1.39) | 1.22 (1.03–1.41) | 0.094 |
| LDL mmol/L | 2.74 (2.15–3.39) | 2.74 (2.20–3.47) | 2.77 (2.07–3.18) | 0.197 |
| Cystatin C mg/L | 1.23 (1.04–1.47) | 1.24 (1.08–1.50) | 1.17 (1.00–1.38) | 0.023 |
| NT-proBNP ng/L | 296 (124–861) | 292 (134–853) | 330 (118–885) | 0.820 |
|
| ||||
| BMS | 207 (59.3%) | 129 (72.9%) | 78 (72.2%) | 0.031 |
| DES | 55 (15.8%) | 39 (22.0%) | 16 (14.8%) | |
| BMS and DES both | 23 (6.6%) | 9 (5.1%) | 14 (13.0%) | |
| Average stent length in mm | 20 (15–30) | 18 (12–26) | 20 (16–32) | 0.026 |
|
| ||||
| | ||||
| during 1st year | 274 (78.5%) | 175 (82.5%) | 99 (72.3%) | 0.032 |
| overall adherence | 214 (61.3%) | 133 (62.7%) | 81 (59.1%) | 0.573 |
|
| ||||
| during 1st year | 236 (67.6%) | 149 (70.3%) | 87 (63.5%) | 0.228 |
| overall adherence | 234 (67.0%) | 149 (70.3%) | 85 (62.0%) | 0.138 |
|
| ||||
| Death | 98 (28.1%) | 57 (26.9%) | 41 (29.9%) | 0.620 |
| CV-Death | 52 (14.9%) | 33 (15.6%) | 19 (13.9%) | 0.779 |
| CV-event | 181 (51.9%) | 115 (54.2%) | 66 (48.2%) | 0.318 |
| Stroke | 31 (8.9%) | 21 (9.9%) | 10 (7.3%) | 0.520 |
| Myocardial infarction | 174 (49.9%) | 112 (52.8%) | 62 (45.3%) | 0.203 |
| CV death | CV event | |||
|---|---|---|---|---|
| Variable | OR (95%CI) | P-value | OR (95%CI) | P-value |
|
| ||||
| Age (per 10 yr) | 1.62 (1.32–2.01) | <0.001 | 1.14 (0.99–1.31) | 0.073 |
| Sex: female | 0.97 (0.63–1.47) | 0.880 | 1.02 (0.75–1.38) | 0.894 |
| Atrial fibrillation | 1.20 (0.60–2.31) | 0.603 | 1.31 (0.73–2.30) | 0.361 |
| Diabetes | 2.18 (1.43–3.31) | <0.001 | 1.54 (1.11–2.13) | 0.009 |
| BMI | 1.07 (1.03–1.11) | <0.001 | 1.04 (1.01–1.07) | 0.009 |
| Smoking: current | 1.10 (0.63–1.91) | 0.745 | 0.87 (0.61–1.24) | 0.444 |
| Smoking: ex-smoker | 1.42 (0.91–2.23) | 0.123 | 0.89 (0.65–1.23) | 0.495 |
| NTproBNP (logaritmized) | 1.63 (1.41–1.90) | <0.001 | 1.14 (1.03–1.26) | 0.010 |
| CystatinC | 1.21 (0.86–1.68) | 0.275 | 1.15 (0.88–1.49) | 0.307 |
| Stent length (per 10 mm) | 1.15 (1.00–1.31) | 0.043 | 1.07 (0.96–1.18) | 0.209 |
| Statin adherence ≥80% | 0.31 (0.17–0.58) | <0.001 | 0.33 (0.21–0.51) | <0.001 |
| Antihypertensive med. | 1.11 (0.41–3.48) | 0.852 | 0.44 (0.26–0.77) | 0.004 |
|
| ||||
| Age (per 10 yr) | 1.06 (0.87–1.29) | 0.564 | 1.03 (0.75–1.42) | 0.865 |
| Sex: female | 1.23 (0.77–1.96) | 0.392 | 1.65 (0.86–3.18) | 0.132 |
| Atrial fibrillation | 2.57 (0.84–8.65) | 0.105 | ||
| Diabetes | 1.61 (0.97–2.66) | 0.063 | 2.07 (1.04–4.15) | 0.038 |
| BMI | 0.98 (0.93–1.02) | 0.313 | 0.96 (0.91–1.03) | 0.256 |
| Smoking: current | 0.84 (0.52–1.37) | 0.493 | 1.12 (0.54–2.32) | 0.752 |
| Smoking: ex-smoker | 1.37 (0.88–2.13) | 0.168 | ||
| NTproBNP (logaritmized) | 1.02 (0.87–1.20) | 0.808 | 0.90 (0.72–1.12) | 0.346 |
| CystatinC | 0.57 (0.31–0.97) | 0.046 | 0.59 (0.30–1.10) | 0.111 |
| Stent length (per 10 mm) | 1.31 (1.09–1.58) | 0.004 | 1.26 (1.02–1.55) | 0.031 |
| Statin adherence ≥80% | 0.30 (0.19–0.47) | <0.001 | 0.45 (0.21–0.95) | 0.036 |
| Antihypertensive med. | 0.29 (0.18–0.48) | <0.001 | 0.67 (0.30–1.52) | 0.338 |
- —State Research Funding for Helsinki University Hospital
- —Matti Schmidt testament fund
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer, Lipids, and Metabolism · Sarcoma Diagnosis and Treatment · Gastrointestinal Tumor Research and Treatment
Introduction
During the first year after coronary stenting ischemic events are mostly related to stent thrombosis or restenosis [1–3]. The rate of stent failure declines after one year to 1–2% per year [3–6]. The rate of stent-related repeat revascularization appears to be higher among CCS patients compared to patients presenting with ST-elevation myocardial infarction (STEMI) [7]. While the development of drug-eluting stents (DES) has reduced the incidence of in-stent restenosis [1,5,6,8–10], patients still experience recurrent ischemic events due to either stent-related complications or the natural progression of atherosclerotic disease. The role of procedural factors such as stent length, vessel size, calcification, and bifurcation lesions in long-term outcomes after percutaneous coronary intervention (PCI) has been widely studied [1,3,5,6,11]. However, less is known about the long-term progression of coronary artery disease.
One mechanism underlying very late stent restenosis has been described as in-stent neoatherosclerosis. Pathophysiological pathways differ to some extent from atherosclerotic process in native vessels. Atherosclerotic plaque formation involves lipoproteins, particularly low-density lipoprotein cholesterol (LDL-C), which is considered the main risk factor for atherosclerotic disease. Transcytosis of LDL-C particles into the tunica intima of the arterial wall triggers an immune response, leading to smooth muscle cell proliferation, extracellular matrix accumulation, and the formation of atherosclerotic plaque. Intensive lipid-lowering treatment has been shown to impede plaque progression and lower the risk of cardiovascular events [12]. Early in-stent restenosis is thought to result from mechanical disruption of the endothelial lining during PCI, which serves as the initiating factor [13]. Findings from intravascular imaging and histological studies suggest that chronic inflammation and endothelial dysfunction contribute to late in-stent neoatherosclerosis, ultimately resulting in very late stent restenosis. In-stent neoatherosclerosis occurs earlier after DES implantation than after BMS implantation, which may reflect differences in the underlying pathophysiological mechanisms [14].
Furthermore, previous studies indicate that while DES substantially reduced in-stent restenosis (ISR) burden compared to bare metal stent (BMS), in-stent neo-atherosclerosis appears to be more common after DES implantation than after BMS implantation [14,15]. This phenomenon has been explained by multiple mechanisms, including drug-driven suppression of neo-intimal growth and incomplete re-endothelization. There are implications that high low-density lipoprotein cholesterol concentration may be independently related to neo-atherosclerosis progression [16,17]. This suggests that good adherence to lipid-lowering medication could prevent very late stent restenosis.
In this article, we aim to define factors related to new ischemia-causing stenosis in the previously stented target lesion (TL) vs. new lesions (NTL), with a particular focus on statin adherence, given our extensive follow-up period and access to medication purchase data.
Methods
Patients and study design
The prospective Corogene (Genetic Predisposition of Coronary Artery Disease) cohort was collected in Helsinki University Central Hospital, Finland, between March 2006 and March 2008, consisting of 5294 consecutive patients assigned to coronary angiography [18]. A subset of patients who underwent percutaneous coronary stenting (n = 1970) was selected for this study. The primary indication for angiography was more often ACS (n = 1335) than CCS (n = 635). Patients with a history of coronary artery bypass grafting (CABG) were excluded. Patients with previous PCI were included in the study; however, restenosis in those lesions were not included. Patients who did not receive a stent on the index procedure were excluded from the analysis.
Following the index procedure, patients were monitored for up to ten years or until the occurrence of PCI, CABG or death. Ischemia-driven revascularizations, indicated by recurrent angina or myocardial ischemia during follow-up, were systematically analyzed. Subsequent angiograms were compared with the index procedure to define the location of a new ischemic lesion, that is, TL or NTL. Segments 5 mm proximal and 5 mm distal to the stent were considered as stent affected, as proposed by the Academic Research Consortium [19] and were included in stent lesion. Stenosis outside this range were considered new lesions. Stent(s) used in the procedure were bare metal stents or drug-eluting stents based on the decision of the invasive cardiologist. The combined stent length is reported without possible overlapping for multiple stents. Patients who did not undergo a subsequent PCI after the index procedure were excluded, including those who experienced an ischemic event but were managed conservatively or underwent CABG.
National registries in Finland can be merged at the patient level with a unique social security number. This enables the acquisition of data on medication purchases from The Social Insurance
Institution of Finland (SII), follow-up data from the Hospital Discharge Registry of the Finnish
(HILMO) Institute for Health and Welfare based on ICD-codes and causes of death from Statistics of Finland [20]. The validity of the diagnostic codes has been studied previously [21]. The follow-up started in March 2006 and January 2006 for SII’s medication purchase data and HILMO’s discharge data, respectively. The follow-up for these data registries lasted until the end of December 2017 or until CABG or the patient’s death, whichever occurred first.
Baseline characteristics, clinical, laboratory, and angiographic findings were collected from the hospital records. Baseline clinical characteristics included traditional risk factors, including age, sex, previous or current smoking, chronic kidney disease, hypertension, diabetes, obesity and atrial fibrillation. Echocardiograms were reviewed when available. Biomarkers, including N-terminal prohormone B-type natriuretic peptide (NT-proBNP), lipoprotein (a) Lp(a), high-sensitivity C-reactive protein (hCRP) and cystatin-C values, were incorporated into the analysis. Angiographic data was evaluated by two interventional cardiologists (M.E and S.J) independently. Analyses were based on the first recorded re-procedure during the follow-up period to avoid duplicate entries.
Medications were pooled into pharmacological groups based on Anatomical Therapeutic Chemical (ACT) codes [22]: antithrombotic agents (ATC code B01), antihypertensive agents (ATC codes C03, C07, C08, C09) and lipid modifying agents (ATC code C10). In Finland, SII reimburses medication purchases up to 3 months at a time (maximally 100 days covered). Medication adherence was defined as days covered on a yearly basis. The follow-up was divided into periods of 365 days beginning from patient discharge and until the end of the follow-up or patient death, whichever occurred first. A period of 365 days was considered adherent if the patient had purchased medication covering ≥ 292 days (80%) within that period and the interval between first and last purchase was ≥180 days. This correlates to an adherence rate of 80%, which is generally considered a measure of good adherence [23,24].
The principal investigator had unrestricted access to the data, maintained the database, prepared all drafts of the manuscript with all authors, and vouched for the integrity of the study.
Ethics approval
All patients provided written informed consent. The Helsinki University Central Hospital Ethics
Committee approved the research protocol for the study (registry numbers 426/E5/05, 205/E0/2007, HUS/152/2016, and HUS/1203/2016). This study complies with the 1964 Declaration of Helsinki and subsequent revisions.
Clinical endpoints
The primary objective was to determine the rate and location of new ischemic events in relation to target lesion stenting, and to differentiate factors related to the course of disease progression.
Secondary outcomes were major adverse cardiovascular events (MACE) defined as cardiovascular death, stroke, or repeat PCI.
Statistical analysis
Data were reported as medians with interquartile ranges (IQRs) for continuous variables and as counts with percentages for categorical variables. Pairwise comparisons were conducted using the Mann–Whitney U-test for continuous variables in relation to outcomes, and the Chi-squared test for categorical variables in relation to outcomes. Logistic regression models were fitted to assess associations with different outcomes. Statistical significance was defined as a p-value <0.05. All analyses were performed using R software, version 4.5.0.
Results
A total of 1970 patients were included in the study. Among the study population, 1335 patients presented with acute coronary syndrome (ACS) and 635 patients with chronic coronary syndrome (CCS). The majority of the patients were males. There were more patients diagnosed with diabetes and dyslipidaemia in the CCS group. Current smoking was more common among
ACS patients. The majority (71.0%) of implanted stents were BMS. Most DES (21.3%) were first-generation devices. Second-generation DES were used in 5.2% of cases, and in 2.4% of cases the stent type was unknown. The median length of stents was 20 (IQR 16–30) mm in ACS group and 20 (IQR 12–29) mm in CCS group (p = 0.161 between groups). Baseline characteristics are summarized in Table 1(A,B).
Following the index procedure, 639 (32.4%) patients had at least one cardiovascular event, including 253 (12.8%) cardiovascular deaths. Of the patients 348 (17.7%) required repeat ischemia-driven revascularization at least once during follow-up. PCI was more frequent in CCS than in ACS patients (144 (22.7%) vs. 204 (15.3%), p = 0.001). On the contrary, CABG was borderline more frequent in ACS than in CCS (13 (1.0%) vs. 1 (0.2%), p = 0.084).
Repeat revascularization occurred more frequently at new target lesions (NTLR) in 212 cases (60.7%) than at target lesions (TLR) in 137 cases (39.3%). Time to TLR was significantly earlier than time to NTLR (1.2, IQR 0.4–6.2 years vs 4.3, IQR 1.6–7.3 years, p < 0.001) (Figure 1). Risk factors associated with repeat revascularization included advanced age, higher NT-proBNP levels and multiple stents (Table 2(A)).
(A) Incidence non-target lesion and target lesion revascularizations during follow-up. (B) Box plot of time interval to revascularization. NTLR = new target lesion revascularization, TLR = target-lesion revascularization. Compared using Mann-Whitney U test.
**: **
Adherence to statin medication declined with time, as expected, but remained at a relatively high level even after 9 years (Supplementary Figures 1 and 2). During the first year after PCI 76.8% of patients in ACS group and 77.5% in CCS group had good adherence to statin medication (≥80% days covered) (p = 0.800 between groups). During the whole follow-up period 55.8% of patients in the ACS group and 63.3% in the CCS group had good adherence to statin medication (p = 0.002). The most prescribed statin was simvastatin (54.7%), followed by atorvastatin (27.7%) and rosuvastatin (7.5%). Most patients (74.4%) were receiving moderate-intensity, while 11.6% remained high-intensity, and the rest were on low-intensity statin therapy. During follow-up, statin therapy could have been modified by switching to other statins or adjusting the dose, either to intensify treatment or to reduce side effects (Supplementary Figures 3 and 4). Antihypertensive medication was used less conscientiously during the first year after PCI with 66.3% (ACS) and 61.8% (CCS) of patients adhering ≥80% to prescribed dosing. Adherence to antihypertensive medication persisted over the years. Among ACS patients 61.7% and 60.7% among CCS patients had good adherence to blood pressure lowering medication throughout the whole 10-year period. Adherence to anticoagulants was 74.7% (ACS) and 73.9% (CCS) during the first year of follow-up. We did not calculate antithrombotic adherence, since the period it was used varied due to multiple reasons, such as the stent type, usage of anticoagulation, and whether patient had ACS or CCS [25]. These findings are in accordance with previous studies investigating long-term medication adherence among Swedish patients after CABG [26].
Multivariate logistic regression models identified several risk factors associated with TLR compared to NTLR, including statin adherence, cumulative stent length, and diabetes (Table 2(B)).
High adherence to statin therapy (≥ 80% of time) significantly reduced the likelihood of TLR versus NTLR. Conversely, increased stent length and the presence of diabetes were associated with a greater risk of TLR compared to NTLR (Table 2(B)).
Discussion
Main findings of this study are: (1) good adherence to statin therapy significantly reduces target lesion (TL)–related events more than non–target lesion (NTL)–related events; (2) both TL- and NTL-related ischemic events continue to occur for at least 10 years following initial coronary stenting; and (3) NTL-related events accounted for the majority of these repeat revascularizations.
Coronary atherosclerosis concerns the whole coronary tree, and despite secondary prevention measures, atherosclerosis will continue to advance in stented and non-stented locations. Longterm follow-ups have shown that non-target lesion events are more frequent than target lesion events [27,28]. The reason for that may be simply the fact that non-stented coronary volume is larger, and, therefore, the probability of new events is also higher. Accordingly, this study showed that new target lesion-related events accounted for most of these repeat revascularizations.
There has long been an expectation that coronary interventions could provide a definitive solution for coronary stenosis. While these procedures are lifesaving in the setting of acute coronary syndrome, significantly reducing mortality and the incidence of myocardial infarctions [29], their primary benefit in chronic coronary syndrome is symptom relief. The initial assumption that a stented coronary segment would be permanently ‘cured’ has not been fully realized, with stent restenosis remaining a major challenge.
Multiple interrelated factors are linked to stent restenosis: clinical factors include diabetes mellitus, elevated low-density lipoprotein levels, chronic kidney disease, heart failure, older age, and female sex; anatomic factors include vessel size and lesion characteristics; procedural factors include stent under expansion, and malposition; and stent-related factors include stent length, stent type and structure [11,28,30–32]. Likewise, in this study, we found that longer stents and diabetes were significant risk factors for stent restenosis.
Stents can also promote hypersensitivity and inflammatory reactions, which were more prominent in first-generation DES than BMS or second-generation DES^3^. These reactions explain the increased risk of late and very late stent thrombosis with first-generation DES [1,5]. With BMS, late lumen loss tends to peak 6–8 months after implantation and then decreases over time. The same trend could be seen in this study. Conversely, with DES, there is a slower but ongoing neointimal accumulation. Despite the substantial improvements in DES technologies, in-stent restenosis and the need for TLR still occur at 1%-2% per year, even with contemporary DES platforms3. This has been shown to continue for at least 5 years [7,10,27,30,33,34]. However, the literature extending beyond that is sparse [27,31,33]. The current study represents one of the longest follow-up periods published in TLR vs NTLR literature, extending the finding that TL restenosis continues for at least 10 years after initial coronary stenting. In our population, it is evident that atherosclerosis continues to progress also in native NTL sites despite the use of statins.
Adherence to evidence-based pharmacological therapies plays a crucial role in mitigating adverse events in both stable coronary artery disease and post-acute ischemic episodes [30,32,34–38]. We had extensive data on medication use throughout the follow-up period, and the extended 10-year follow-up allowed a comprehensive examination of the progression of coronary artery disease in both natural and stented segments in a real-world setting. Statins protected from all end points including target-lesion revascularizations, especially when used ≥80% of the time. This underscores the importance of lifetime adherence to lipid-lowering therapy, especially in diabetic patients with long or multiple stents. High-intensity LDL-lowering therapy may even promote plaque regression and stabilization, as observed in several coronary imaging studies [12]. However, its effect on long-term cardiovascular outcomes requires additional research. One example of that is proprotein convertase subtilisin/kexin type 9 inhibitor or its gene silencing, which may stabilize LDL cholesterol levels better than statins and that way prevent atherosclerosis progression [39].
Statin therapy after PCI can reduce the risk of repeat revascularization [40]. Less is known about the statin effect on TLR vs NTLR. One study shows that statins reduce TLR in sirolimus stents, but not in BMS [41]. Small, randomized studies have previously shown that statin does not reduce TLR vs target vessel revascularizations, however, no such studies on TLR vs NTLR have been published [42–44]. It should be noted that the target vessel means the same coronary artery where the initial stent is located, but the non-target lesion is a broader concept, including all locations and coronaries, but not the stent spot, and 5 mm proximal and 5 mm distal to the stent. In the present study, NTLR was more frequent than TLR, and good adherence to statin therapy reduced TLR more than NTLR.
Statins are known to reduce the risk of plaque rupture in native coronaries [45,46]. The direct evidence that statins will also reduce plaque rupture in in-stent neoatherosclerosis is lacking.
Neoatherosclerosis is frequently observed in patients with very late stent thrombosis, i.e. more than one year after stenting. This phenomenon is significantly associated with the implantation of drug-eluting stents. Furthermore, in-stent plaque rupture often occurs in patients with neoatherosclerosis and previous myocardial infarction [47]. Aligning with this finding, in the present study TLR was more frequent in ACS patients than in CCS patients. It is plausible that in-stent plaque rupture can be prevented with statin in a similar manner to native coronaries. The observed finding that statins reduce TLR may be attributed to statins’ pleiotropic effects, reducing neo-atherosclerosis through various mechanisms. Statin therapy reduces coronary inflammation [45]. However, there is also evidence that statins reduce stent-induced inflammation. In a porcine model, statin-coated stents were used, and they decreased neointimal hyperplasia [48].
Limitations
The study cohort represents a large prospective material from a single center. However, the number of repeated revascularizations is moderate. Larger material in multiple centers is needed to confirm our findings. Since the study enrollment period, procedural techniques and pharmacologic therapies have advanced. In this cohort, bare metal stents were predominantly used, and clopidogrel was the primary antithrombotic agent following stenting, unlike current practice, using more contemporary DES technologies, and frequently ticagrelor for post-ACS management.
In cases of death or conservatively managed ischemic events, the exact location of potential coronary stenoses was not determined, which may have influenced the proportions and endpoints related to target lesions (TL) and new target lesions (NTL).
The study population represents prospectively collected registry data. Therefore, medication adherence has been obtained from purchase history, but the actual use of the medication cannot be determined. Additionally, the use of acetylsalicylic acid is not known since it is mostly bought over the counter. Because follow-up relies on registry data, we lack detailed information on several clinically relevant aspects. Moreover, no patient-level data are available beyond the index hospitalization; for example, LDL levels during follow-up are unknown.
Conclusion
Ischemic events related to both TL and NTL persist for at least 10 years following initial coronary stenting. Notably, the majority of repeat revascularizations during this period are driven by NTL-related events. Achieving over 80% adherence to statin therapy provides significantly greater protection against TLR compared to NLR.
Previous long-term lipid-lowering randomized controlled trials in stented patients with imaging data could help validate our findings. Stent trials with extended follow-up and varied lipid-lowering regimens may also offer insights into in-stent neoatherosclerosis. Ultimately, the most robust approach to confirm the reproducibility of our results would be a dedicated randomized controlled trial incorporating intravascular imaging and long-term follow-up.
Supplementary Material
Supplementary_material.docx
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sarno G, Lagerqvist B, Nilsson J, et al. Stent thrombosis in new-generation drug-eluting stents in patients with STEMI undergoing primary PCI: a report from SCAAR. J Am Coll Cardiol. 2014;64(1):16–24. doi: 10.1016/j.jacc.2014.04.022.24998123 · doi ↗ · pubmed ↗
- 2Cutlip DE, Chauhan MS, Baim DS, et al. Clinical restenosis after coronary stenting: perspectives from multicenter clinical trials. J Am Coll Cardiol. 2002;40(12):2082–2089. doi: 10.1016/s 0735-1097(02)02597-4.12505217 · doi ↗ · pubmed ↗
- 3Giustino G, Colombo A, Camaj A, et al. Coronary in-stent restenosis: JACC state-of-the-art review. J Am Coll Cardiol. 2022;80(4):348–372. doi: 10.1016/j.jacc.2022.05.017.35863852 · doi ↗ · pubmed ↗
- 4Donisan T, Madanat L, Balanescu DV, et al. Drug-eluting stent restenosis: modern approach to a classic challenge. Curr Cardiol Rev. 2023;19(3):e 030123212355. doi: 10.2174/1573403 X 19666230103154638.36597603 PMC 10280993 · doi ↗ · pubmed ↗
- 5Tada T, Byrne RA, Simunovic I, et al. Risk of stent thrombosis among bare-metal stents, first-generation drug-eluting stents, and second-generation drug-eluting stents: results from a registry of 18,334 patients. JACC Cardiovasc Interv. 2013;6(12):1267–1274. doi: 10.1016/j.jcin.2013.06.015.24355117 · doi ↗ · pubmed ↗
- 6Palmerini T, Biondi-Zoccai G, Della Riva D, et al. Stent thrombosis with drug-eluting and bare-metal stents: evidence from a comprehensive network meta-analysis. Lancet. 2012;379(9824):1393–1402. doi: 10.1016/S 0140-6736(12)60324-9.22445239 · doi ↗ · pubmed ↗
- 7Fokkema ML, James SK, Albertsson P, et al. Outcome after percutaneous coronary intervention for different indications: long-term results from the Swedish Coronary Angiography and Angioplasty Registry (SCAAR). Euro Intervention. 2016;12(3):303–311. doi: 10.4244/EIJY 15M 10_07.26485732 · doi ↗ · pubmed ↗
- 8Bangalore S, Kumar S, Fusaro M, et al. Short- and long-term outcomes with drug-eluting and bare-metal coronary stents: a mixed-treatment comparison analysis of 117 762 patient-years of follow-up from randomized trials. Circulation. 2012;125(23):2873–2891. doi: 10.1161/CIRCULATIONAHA.112.097014.22586281 · doi ↗ · pubmed ↗