Vaccine preferences and their role for vaccine confidence and uptake: a meta-ethnography
Jeniffer Landicho, Thea Andrea Bravo, Jonas Wachinger, Catherine Silvestre, Kate Bärnighausen, Kerry Scott, Till Bärnighausen, Shannon A. McMahon, Mark Donald C. Reñosa

TL;DR
This study explores how people's preferences for vaccine characteristics influence their confidence and willingness to get vaccinated.
Contribution
The paper introduces a meta-ethnographic synthesis of qualitative data on vaccine preferences using the 4Ps marketing framework.
Findings
Vaccine preferences are shaped by perceived product quality, safety, and origin.
Convenience of vaccination locations and delivery methods is a key factor in vaccine acceptance.
Promotional strategies and information sources significantly influence vaccination decisions.
Abstract
Vaccine confidence and uptake are influenced by individuals’ preferences regarding vaccine composition, quality, or administration pathways. However, literature synthesizing available qualitative insights into individuals’ vaccine preferences remains limited. We therefore conducted a meta-ethnographic systematic review of the qualitative literature on vaccine preferences to identify opportunities for enhancing vaccine confidence and uptake. We implemented a comprehensive search strategy and screened 5,528 studies across seven research databases published between 2001 and 2023. We identified and synthesized 97 qualitative articles to delineate factors influencing consumers’ vaccine preferences. Our findings revealed four primary domains shaping individuals’ vaccine preferences: Product, Place, Price, and Promotion. First, individuals’ preferences for vaccines often hinge on perceived…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
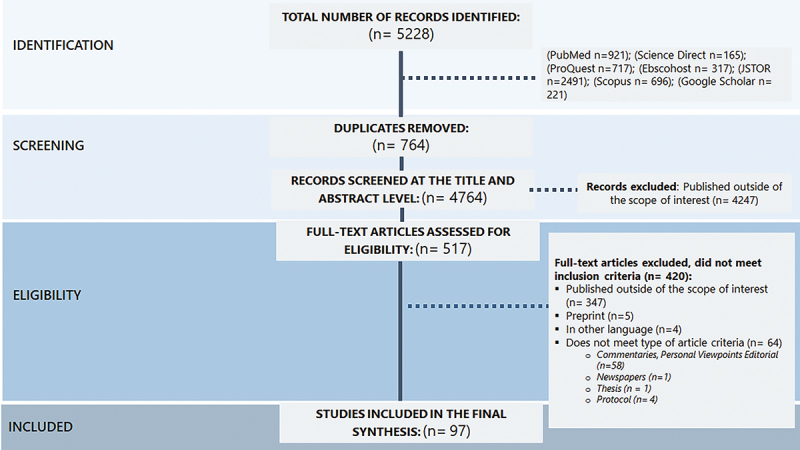 Figure 1
Figure 1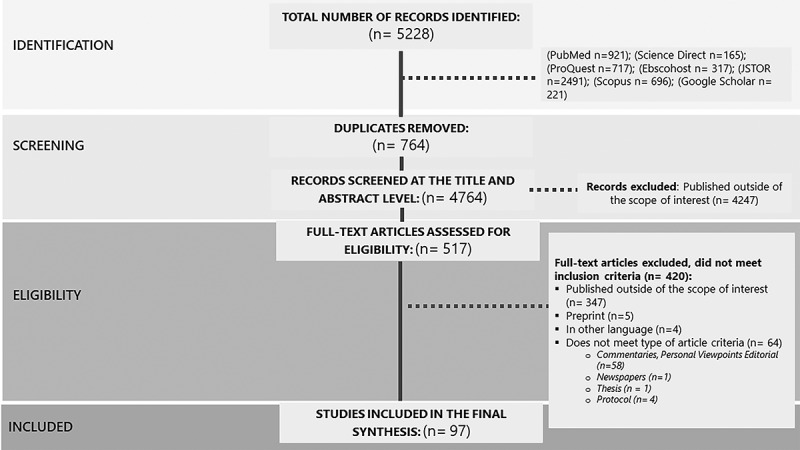 Figure 2
Figure 2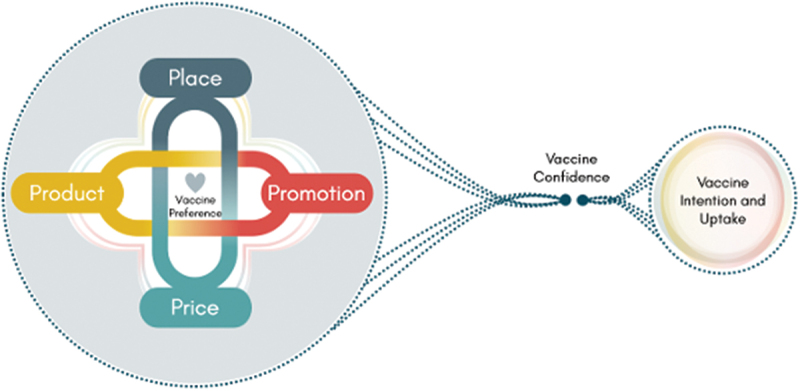 Figure 3
Figure 3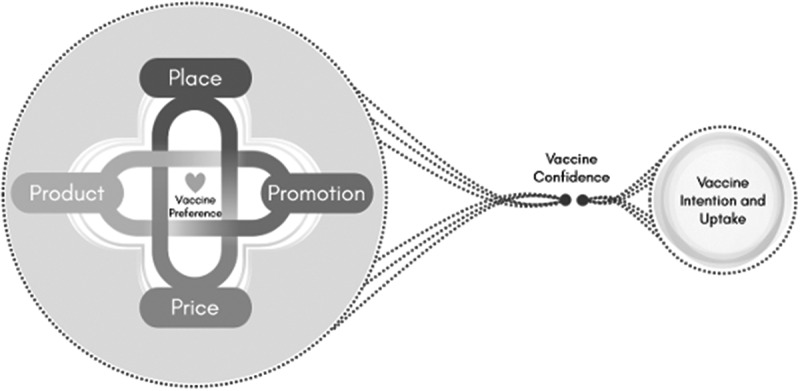 Figure 4
Figure 4- —Bill & Melinda Gates Foundation
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVaccine Coverage and Hesitancy · Influenza Virus Research Studies · Bacterial Infections and Vaccines
Background
Vaccination stands as a cornerstone of public health, having saved an estimated 154 million lives worldwide since 1974 by preventing infectious diseases such as hepatitis, diphtheria, tetanus, pertussis, measles, and polio [1–3]. Vaccination programs are instrumental in advancing global health goals, including the Millennium Development Goals 4 and 5 (reducing child mortality and improving maternal health) and the Sustainable Development Goal 3, (ensuring healthy lives and well-being for all [4–6]. More specifically, from 1990 to 2013, under-five mortality fell by 49%, aided in part by improved immunization coverage, including a 74% reduction in measles deaths from 2000 to 2013 [5]. During the same period, maternal mortality has also dropped by 45% [5,7,8].
Despite these remarkable gains, public trust in vaccines has been increasingly undermined: already prior to the COVID-19 pandemic, vaccine hesitancy and controversies posed significant threats to public health [9]. In 2019, the World Health Organization (WHO) identified vaccine hesitancy–defined as the reluctance or refusal to vaccinate despite vaccine availability–as one of the top ten global health problems [10]. The challenge of vaccine hesitancy is especially acute in low- and middle-income countries (LMICs), where fragile health systems and resource limitations compound the risks associated with vaccination coverage [11–13].
Efforts to strengthen vaccination programs and improve vaccine uptake require a nuanced understanding of the factors shaping individual decision-making. While vaccine hesitancy, confidence, and uptake are distinct constructs, they are closely related [14–17]. Vaccine confidence generally refers to trust in vaccines, the systems that deliver them, and the motivations of policymakers and individuals [17–19]. Low confidence may contribute to hesitancy, which in turn may lead to reduced uptake [20]. However, several studies have shown that vaccine hesitancy is additionally shaped by a range of factors beyond confidence, including past experiences with health services, perception of disease risks, and how information is communicated. Contextual influences such as historical, political, and socio-cultural, also play a role in how individuals perceive and engage with vaccines [21–24].
Vaccine uptake, meanwhile, can be influenced by practical access barriers, even when confidence is high [25]. Existing systematic reviews have elucidated various barriers affecting vaccination uptake [26–29], including individual preferences regarding vaccination design and delivery [27,30]. These studies span diverse vaccine contexts—such as childhood immunizations [26,27], global perspectives on routine vaccination [28], influenza vaccines [29], and HPV vaccination [30]—and highlight the role of individual experiences and service design in shaping decisions. However, these reviews tend to center on barriers or determinants of uptake rather than vaccine preferences per se, and are predominantly quantitative in nature. In contrast, preferences [31]—understood as people’s stated or inferred inclinations toward certain attributes—represent an emerging area of interest in the vaccination literature. Despite their increasing salience in public discourse, vaccine preferences remain undertheorized and underexplored within the academic literature.
In this article, we define vaccine preferences as individuals’ stated or inferred inclinations toward particular attributes of vaccines (e.g. brand, delivery method, dosing schedule, site of administration), shaped by both personal and contextual factors [32,33]. These preferences reflect affective, cognitive, and social processes, and are often embedded in cultural expectations, past experiences, and media messaging [34]. While many studies use discrete choice experiments or survey methods to assess the relative importance of specific vaccine attributes [30,33,35–38], preferences are not static; rather, they are dynamic, subjective experiences, and culturally mediated–evolving through complex interactions with societal norms, personal experiences, and environmental influences [39].
This nuanced perspective on preferences, rooted in disciplines such as social psychology and anthropology [34], emphasizes that preferences extend beyond a mere evaluation of product features [30,35,36,40,41]. Understanding individuals’ preferences necessitates a deeper examination of how individuals develop, negotiate and articulate their desires within broader cultural and social contexts. Such an approach would offer a comprehensive insight into how people constructs, mediate and express these preferences in their everyday lives.
In the context of vaccination, preferences are influenced by geographical location, cultural background, religious beliefs, education, media messaging, and service delivery options among others [21]. For example, in many Muslim-majority countries, vaccine content and the influence of religious leaders significantly determined community decisions and attitudes toward vaccination [42]. During the COVID-19 pandemic, vaccine brand preference became a significant phenomenon in several countries–sometimes driven by perceived efficacy, nationalism, rumors, and misinformation [43–46]. Additionally, vaccine brand preferences were influenced by vaccine presentations in diverse social media content [46,47]. When these preferences were unmet or ignored, public confidence and trust in the vaccination program was often undermined–even when vaccines were accessible and free [45]. In this way, vaccine preferences may serve as signals or expressions of deeper sentiments–such as trust, fear, or exclusion–that intersect with vaccine confidence and shape hesitancy [24]. Conversely, when available vaccine options align with people’s preferences, this may reinforce confidence and increase uptake. Understanding preferences requires more than mapping feature rankings; it calls for contextualized, qualitative insights into how individuals interpret and express what matters to them in relation to vaccination.
In this article, we present findings from a meta-ethnographic systematic review of available qualitative literature that examines how individuals experience, negotiate, and articulate preferences related to vaccines and vaccination. Rather than assuming preferences directly cause or prevent hesitancy, we explore how preferences interact with broader social and institutional factors to shape vaccine intention and, in some cases, uptake. Recognizing and addressing individuals’ vaccine preferences is crucial for informing policies and improving immunization programs, and ensuring vaccination efforts are responsive, trusted, and contextually grounded.
Methods
We conducted a meta-ethnographic systematic review informed by Noblit and Hare [48]. Meta-ethnography is useful for synthesizing qualitative research and creating frameworks to analyze and understand the results from various studies [49,50]. Unlike other qualitative synthesis approaches, which may focus more on aggregating themes or describing patterns, meta-ethnography enables the interpretive translation of concepts across primary studies. This results in new understandings or frameworks that are more explanatory and conceptually rich–an approach especially appropriate for complex, value-laden topics such as vaccine preferences, where context and meaning shape individual decisions [51,52].
Our review followed a seven-step framework [48]: 1. Getting started; 2. Deciding what is relevant to the initial interest; 3. Reading the studies; 4. Determining how the studies are related; 5. Translating studies into one another; 6. Synthesizing translation; and 7. Expressing the synthesis. In the following sub-section, we outline how we performed each of these steps within our study.
Getting started
JL and MDCR began with a brainstorming session to ‘identify the intellectual interest’ within the area of vaccine preferences [48]. Preliminary research questions were sent to the broader team for evaluation of relevance and acceptability. Following a series of discussions and iterative refinement, we finalized the overall question, which was to examine vaccine preferences from the perspective of the public.
Deciding what is relevant to the initial interest
After the primary question was finalized, JL, TAB and MDCR convened to outline core concepts and main keywords to be used to develop the search string strategy. To create the initial search strings, we combined Medical Subject Headings (MeSH) and Non-MeSH terms such as ‘Vaccine Preference’, ‘Vaccine Attributes’, ‘Vaccine Acceptability’, ‘Qualitative studies’ and ‘Qualitative Research’. The keywords were combined using Boolean operators like ‘AND’, ‘OR’, and ‘NOT’. We tested the validity of our initial search string strategy by conducting a pilot search on PUBMED and ScienceDirect to refine our search strategy and identify any remaining issues. We evaluated the number of search result and assessed their relevance to the study. Afterward, we extracted the MESH terms from the identified relevant studies. We chose to adopt the broader subject heading so that all terms nested under it would be included in the search, resulting in a comprehensive coverage of relevant literature, which is detailed in Supplementary Table S1.
After the search string strategy was finalized, JL executed the final search strings across six primary research databases including PubMed, ScienceDirect, ProQuest, EBSCOhost, JSTOR, and Scopus. To further enhance the comprehensiveness of our search, a secondary search was conducted using Google Scholar to capture grey literature and additional relevant studies. TAB then independently re-ran the final search strings across five research databases to validate the search results, confirming consistency and accuracy. The results from each search string of JL were exported and tabulated per research database using Endnote (version 8.2) and Microsoft Excel (version 2019), facilitating efficient documentation and removal of duplicate references.
After JL removed duplicates, the MS Excel sheet was shared with the other members of the research team. JL, TAB and CS independently screened the titles and abstracts of papers retrieved from the seven research databases (both primary and secondary databases) based on pre-defined eligibility criteria (see Table 1). Further, we performed a reference listing of all included articles to identify additional publications that may have been missed in our initial search combinations.Table 1.Inclusion and exclusion criteria.CriterionInclusionExclusionLiterature focus(1) Original research(2) Research involved qualitative methods(3) Findings included qualitative insights on vaccine preferences(1) Quantitative studies(2) Systematic reviews(3) Studies without ethical approval(4) Review articles, commentaries, conference or seminar papers and/or personal viewpoints(5) Articles that are abstract only and/or no retrievable full text(6) Books/Theses/Dissertation(7) Vaccine preference studies on veterinary vaccinesTime periodLanguageJanuary 2001* – August 2023English *Reflects the timepoint when several new vaccines (varicella and other conjugated vaccines) were introduced for the general public, sparking debates about vaccine preferences.
Reading the studies
To familiarize ourselves with the content of the studies, JL and TAB read and re-read all included studies. Using printed copies of the studies, we manually highlighted and annotated key information using markers and highlighters. This collaborative, hands-on approach enabled close engagement with the data and supported the identification of relevant concepts and contextual elements. An evidence table was developed to systematically extract and record pertinent contextual data from each study.
To enhance process rigor, MDCR reviewed four studies and compared their observations with those of JL and TAB. This step helped to validate the coding and data extraction approach before the two lead authors proceeded to apply the same process across all remaining included studies.
JL and TAB assessed the quality of all included studies using the Consolidated Criteria for Reporting Qualitative Studies (COREQ). This appraisal focused on evaluating the transparency and rigor of study reporting but did not inform study inclusion or exclusion. Instead, it was used to support a more nuanced interpretation of the findings during synthesis.
Determining how studies are related
We performed manual coding to highlight and compare relevant statements (i.e. all key metaphors, ideas, and/or concepts and their relations) across articles. These statements were tabulated in the excel sheets with reflexive notes or memos to help us bridge some nuances or confusion with the data and support us in the finalization of the codebook.
To promote reflexivity and ensure that the coding accurately reflected the core content and interpretations of the included studies, we employed several strategies. First, we engaged in regular discussions as a research team to reflect on our positionalities, disciplinary backgrounds, and potential biases that could influence the interpretation of the data. These reflexive discussions were particularly important given our interdisciplinary team, which included public health researchers and social scientists. Second, to assess the trustworthiness of our thematic coding and promote intersubjectivity, four articles were randomly selected and independently coded by JL and MDCR. The results were then compared with the codes and themes generated via a meeting. Discrepancies were discussed, and convergence across interpretations was used to refine the codebook iteratively. This dual process of reflexive dialogue and collaborative coding contributed to a more nuanced and transparent analysis. This process supported us in the finalization of the codebook.
Translating the studies into one another
We employed a layered approach to generate new and higher-order interpretations that drew on both first- and second-level analysis. At the first level, JL, TAB, and MDCR extracted illustrative participant quotes from the included studies, which served as our primary data. These quotes were systematically coded, and similar codes were clustered to identify patterns and develop emerging concepts across studies. To complement this, JL and MDCR also engaged in second-level analysis by considering the themes, categories, and interpretations offered by the original study authors. This allowed us to compare not only what participants said, but also how study authors understood and contextualized those views. This dual-level approach enabled us to surface both the direct expressions of vaccine preferences and the broader interpretive insights embedded in the primary literature.
The coded data, accompanying analytical memos, and emerging themes were then compared across all included studies to identify patterns and variations in how vaccine preferences were described. This process allowed us to gain an overview of how key elements of vaccine preferences emerged and interacted across diverse settings and populations. Each theme was carefully reviewed to ensure conceptual clarity, distinctiveness, and coherence. To further strengthen transparency and rigor, we held collaborative team discussions throughout the analysis process. These discussions helped guide interpretative decisions, drawing upon existing literature and our own contextual knowledge, and informed our decision to map the inductively developed insights in the later stages of analysis.
Synthesizing translations and expressing the synthesis
Our analysis followed an iterative and layered process. We began with an inductive thematic analysis to identify patterns and themes emerging directly from the data, allowing participant perspectives to shape the initial structure of our findings. As these core themes became well-established, we observed that many of them related to the characteristics of the vaccine itself, the information available about it, associated costs, and vaccination access.
To further deepen our interpretation and enhance analytical coherence with existing literature, we then organized the emerging themes into analytical categories using Borden and McCarthy’s ‘4Ps of Marketing Mix’ framework, as a secondary, deductive lens [53]. This framework facilitates the identification of crucial factors that contribute to the attractiveness of a product or service (in our case, vaccines and vaccination programs) to clients, focusing on the 4Ps–Product, Place, Price, and Promotion. We mapped the inductively derived themes onto the 4Ps domains, enabling us to organize the findings in a way that preserved the originality of participants’ insights while providing a structured, theory-informed basis for understanding the broader drivers of vaccine preferences [54].
Results
Characteristics and data sources of included studies
We performed a comprehensive review of literature published between January 2021 and August 2023, identifying a total of 5,228 studies. After removing 764 duplicates, we screened titles and abstracts of 4,764 and reviewed the full text of 517 studies. After screening and assessing study eligibility, our final sample consisted of 97 qualitative studies as shown in Figure 1. Figure 1.PRISMA diagram of articles identified and selected.
Of the included studies, 65% were conducted in high-income countries (HICs), including the USA (n = 19), UK (n = 13), Canada (n = 10), the Netherlands (n = 4), New Zealand (n = 2), Switzerland (n = 2), Australia (n = 7), Spain (n = 1), Poland (n = 1), and Sweden (n = 1). Studies conducted in upper-middle-income countries accounted for 9% of the total while those in low- and middle- income countries (LMICs) represented 14%. Low-income Countries (LICs) were represented in 4% of the included articles, specifically Uganda (n = 3) and Sierra Leone (n = 1). Additionally, six (6%) of the included studies used a multi-country setting, such as HICs and LMICs or more specific pairings such as LMICs and LICs, or HICs and upper middle-income countries (UMICs). These countries were categorized following the World Bank Classification, which categorizes countries into four income groups based on the previous year’s Gross National Income per capita [55].
Forty-six percent of the included studies employed a descriptive qualitative study (n = 45) followed by an exploratory qualitative study (n = 28; 29%). Remaining studies were either cross-sectional qualitative, phenomenology, grounded theory, or other types of qualitative study design. To identify and recruit the study participants, 73% of the included studies used purposive sampling (n = 71), Respondent groups included parents, adolescents, the elderly, healthcare providers, and policymakers. Additionally, three studies specifically included indigenous peoples, and two studies involved religious leaders. Data collection methods across included studies were interviews (n = 52) and focus-group discussions (n = 24), with many studies (n = 21) using a combination of both methods and other techniques such as observation and qualitative surveys. Thematic analysis (n = 57) was the most common analytical approach, followed by content (n = 12) and framework analysis (n = 12). For a detailed description of the included studies, please refer to Supplementary Table S2.
Quality of included studies
Across COREQ domains related to research team composition and reflexivity, 26 out of 97 studies reported the researcher’s credentials, and 31 studies indicated the researchers’ occupation at the time of research implementation. Additionally, 38 studies specified the researcher’s experience and training in conducting qualitative research (see Supplementary Table S3).
Many of the included studies (n = 64) described their methodological orientations and theoretical frameworks and provided details on participant involvement and selection processes. However, only 29 studies reported reasons why approached individuals declined to participate or dropped out prematurely, and nine studies did not specify how participants were approached. Data saturation was discussed in 46 studies. In terms of data analysis, 69 studies reported the number of coders, with 51 of these articles providing descriptions of the coding tree. Most studies (n = 63) used qualitative data analysis software such as NVivo, Atlas.ti, and MAXQDA.
Key findings
We identified various themes via the synthesis of included studies, which we organized based on the core concepts of the 4Ps: Product, Place, Price, and Promotion [53]. While many studies primarily focused on discussions surrounding HPV and COVID-19 vaccines, our analysis highlights the broader complexities of vaccine confidence and uptake across different vaccines, including routine childhood vaccines, HPV, COVID-19 vaccines, and other adult vaccines. Figure 2 illustrates these complexities, emphasizing how preferences and decision-making are influenced by a range of factors. Figure 2.Vaccine preferences among the general public.
A large proportion of identified preferences centered on the product (i.e. the vaccine) itself, encompassing considerations of quality, safety, composition, and administration details e.g. dosage). Additionally, the location or place of vaccination (e.g. government or private health facilities), including timing and availability, influenced respondents’ vaccine decision-making. Fewer articles highlighted strong preferences related to vaccination price, with considerations commonly focusing on the cost of new vaccines not (yet) covered by governments or insurers, and indirect expenses such as transportation costs or lost income from missed work. In comparison, the promotion of vaccines featured more prominently in the identified articles, particularly in terms of vaccine information considerations and the preferred sources for this information.4PsVaccine PreferencesFactors influencing preferenceArticle Reference/CountryProductVaccine QualityExtensive product research and qualityassurance testingAustralia [74] Canada [62] Canada [75] HongKong SAR [57] Hongkong SAR [61] Hongkong SAR [69] India [72] Malaysia [56] New Zealand [58] The Netherlands [59] Uganda [63] United Kingdom [60] United Kingdom [73] United States [64] United States [65] United States [66] United States [67] United States [68] United States [70] United States [71] Demonstrate high efficacy with favorable safety and tolerability profileAustralia [74] Australia [91] Australia [102] Canada [62] Canada [77] Canada [83] Canada [84] Canada [88] China [101] Haiti [85] Hongkong SAR [61] HongKong SAR [69] India [97] India [100] Multi-country [121] Multi-country [95] Nigeria [82] Tanzania [96] The Netherlands [78] The Netherlands [92] Uganda [90] Uganda [99] United Kingdom [79] United Kingdom [80] United Kingdom [81] United Kingdom [87] United Kingdom [98] United States [67] United States [76] United States [89] United States [93] United States [94] United States [71] United States [103] Venezuela [86] Clinically effective with extended duration of protectionAustralia [91] Canada [83] Canada [84] China [104] Haiti [85] HongKong SAR [57] Nigeria [82] Sierra Leone [110] Switzerland [107] Switzerland [109] The Netherlands [59] The Netherlands [92] The Netherlands [105] Uganda [90] United Kingdom [79] United Kingdom [98] United States [65] United States [76] United States [94] United States [71] United States [108] Vietnam [106] Production, Packaging, Composition, and AdministrationWith Careful consideration of ethical standards and cultural values in the design and manufacturingHongKong SAR [113] Indonesia [114] Malaysia [56] Multi-country [115] New Zealand [58] Sweden [111] The Netherlands [92] United Kingdom [79] United Kingdom [112] Desire to minimize the frequency and volume of vaccine administrationAustralia [91] Canada [116] HongKong SAR [57] Malaysia [56] Tanzania [96] United Kingdom [117] United Kingdom [118] United States [76]PlaceAdequate supply of vaccines andaccessibility of service delivery pointWith adequate supply of vaccinesMexico [119] Panama [120] United Kingdom [73] Accessible service delivery pointAustralia [91] Canada [75] Canada [124] Multi-country [121] Tanzania [123] United States [65] Zambia [122] Assurance of privacyand preference for well-trained healthcare providersPrivateUnited States [125] Well trained health care providerCanada [116] Mexico [119] United Kingdom [117] United States [108] United States [125]PriceVaccination costOr Preference for affordable vaccination options and trusted vaccine brandsAffordable Vaccination cost (High prices i.e not free or affordable price, covered by insurance)Canada [62] Canada [116] Côte d’Ivoire [129] HongKong SAR [57] Hongkong SAR [61] India [72] India [128] India [130] Malaysia [56] Multi-country [121] Multi-country [127] Nigeria [82] The Netherlands [59] United States [65] United States [66] United States [67] United States [126] Preferences to trusted vaccine brandsAustralia [74] Australia [132] China [104] Côte d’Ivoire [129] Hongkong SAR [61] Multi-country [127] Poland [131] Singapore [134] United Kingdom [117] United States [135] Vietnam [133] Preference for Cost-effective vaccine that reduce financial and healthcare burdenCost-effectiveness of the vaccinesCanada [77] India [100] India [128] India [136] Multi-country [121] United States [67] Reduction of secondary costassociated with vaccinationSecondary costs associated with vaccinationAustralia [138] India [130] United States [137] Zambia [122]PromotionPreferred content of Vaccine information, sources and channelsComprehensive informationon the value of vaccinesCanada [116] HongKong SAR [69] India [128] Malaysia [56] Mexico [119] Panama [120] Spain [141] The Netherlands [59] United Kingdom [70] United Kingdom [73] United Kingdom [139] United Kingdom [143] United States [67] United States [70] United States [94] United States [140] United States [142] Vietnam [106] Zambia [122] Trusted messengersin conveying vaccine informationAustralia [102] Australia [144] Australia [145] Canada [83] Canada [84] Canada [88] Canada [147] Haiti [85] Hongkong SAR [61] HongKong SAR [69] HongKong SAR [113] India [128] Indonesia [114] Malaysia [56] Multi-country [121] Multi-country [146] Panama [120] United Kingdom [98] United States [67] United States [140] United States [142] Vietnam [106] Zambia [122] Preferredmode of delivery and channel of informationCanada [75] Canada [148] The Netherlands [59] United States [89] United Kingdom [117] United States [135] United States [140] Freedom of choice versus mandatory vaccinationRespect for autonomy of individual and freedom of choiceAustria [150] Canada [62] HongKong SAR [113] Multi-country [127] New Zealand [149] The Netherlands [78] Poland [131] United Kingdom [87] United States [64] Preference for Mandatory vaccinationUnited States [67]
Product
Vaccine quality
Extensive product research and quality assurance testing
In most studies (91 out of 97), participants highlighted their preference for a vaccine that was of high quality (commonly defined in terms of vaccine efficacy and effectiveness in preventing disease) and safe (commonly defined as the absence of or minimal side effects).
Across studies, participants emphasized the critical role of safety in evaluating the vaccine quality, especially for new vaccines. For instance, in a study on parents’ refusal of childhood vaccination in Malaysia, one participant emphasized a need for vaccine safety ‘to be guaranteed through adequate testing and research, until doctors can give the assurance that it is 100% safe’ [56]. Studies conducted in Hong Kong, New Zealand, and the Netherlands also highlighted concerns among parents and young adults regarding the insufficient investigation of new vaccines before their introduction to the global market [57–59]. Similar suspicions and concerns arose during emergencies when vaccines were perceived to be manufactured and deployed prematurely without adequate scientific scrutiny, as observed with the AH1N1 vaccine [57]. In a UK study exploring COVID-19 and COVID-19 vaccination beliefs, a participant voiced concerns regarding the rapid development of vaccines: ‘They’ve made it so quick we don’t know the side effects it’s going to have in the future’ [60]. The uncertainties surrounding new vaccines often led participants to prefer waiting and assessing the vaccine’s effects on others first [70–75,127]. Studies conducted in Hong Kong SAR, Canada, Uganda, and the U.S. indicated a prevailing preference to wait until long-term studies were available [61–67], which could identify limitations and possible side effects before broader roll-out [59,60,65,68,69]. Participants expressed concerns about the need for more studies on vaccines to address potential risks, as illustrated by a participant’s comment: ‘Do more studies on the vaccine. Sometimes they say the vaccine is good, and then a few years after that you hear someone died because of it or it is making things worse’ [67].
Demonstrate high efficacy with favorable safety and tolerability profile
Participants across studies consistently preferred vaccines with few to no side effects and high efficacy [61,62,67,69,71,76–87,102,121]. Many individuals set high standards for vaccines, voicing a preference for 100% efficacy, as evidenced in a Canadian study among Indigenous People [62]. Moreover, several studies underscored participants’ preference for vaccines with demonstrated long-term vaccination efficacy [76] and effectiveness in preventing vaccine-preventable disease [69,74,77–80,121]. If the vaccine is effective in preventing infections, some participants showed a willingness to accept short-term side effects (e.g. fever, injection site pain and scarring, stomach flu, dizziness, and fatigue) [61,67,69,76,82–89,103], highlighting complex trade-offs between immediate discomfort and long-term benefits. On the other hand, individuals who had either experienced the diseases firsthand or were more susceptible to diseases expressed willingness to accept vaccines with lower effectiveness [84,90–96], suggesting that their direct experience may make them open to any level of protection. However, concerns about severe side effects–such as death, deformities, disabilities, and vaccine effects on unborn children–were significant barriers to vaccine uptake [63,67,97–101].
Clinically effective with extended duration of protection
Participants across settings consistently emphasized that a high-quality vaccine is one that effectively prevents disease and offers protection [57,59,65,68,76,79,82–85,90–92,94,98,104–108]. For instance, in Vietnam, a parent of a fully vaccinated girl stressed the importance of vaccines for rural residents who cannot afford healthcare [106], while a Swiss participant described vaccination as essential, saying ‘vaccinating is life’ [107,109]. Parents, especially those with children in school, expressed that vaccinating their children alleviates their anxieties, as vaccines help mitigate the risks of preventable diseases. Beyond individual-level factors, some participants also recognized the broader societal benefits of vaccination, particularly its role in disease eradication [71,96,98,99,110].
Production, packaging, composition and administration good manufacturing product
Designed and manufactured with consideration of ethical standards and cultural values
Participants’ perspectives on vaccine content and manufacturing methods including parenteral containers and dosage forms differed considerably across studies and countries [103,115,130,151]. In the Netherlands, Sweden, and the UK, participants expressed fears about the potential use of harmful substances such as chemicals, metals, microchips, or viruses in vaccine production [92,111,112]. Participants from Malaysia, New Zealand, and Hong Kong voiced concerns about injecting ‘foreign’ substances into their bodies, perceiving potential harm [56,58,113]. Other participants questioned the cleanliness of the vaccine production process based on their religious beliefs, raising worries about the use of animals or aborted fetuses in an exploitative manner [56]. Muslim participants in clinical trials in Malaysia and the UK strongly preferred ‘halal vaccines’ that guaranteed the absence of any pig-derived fragments [56,79]. Similarly, participants in Indonesia sought approval from ulamas (Muslim scholars recognized for their expertise in Islamic law and theology) to ensure the acceptability and purity of the vaccine products [114].
Desire to minimize the frequency and volume of vaccine administration
Several studies highlighted preferences related to vaccine dosage, intervals, and administration schedules [103,130]. In a Tanzanian study on the acceptability of dosage reduction for HPV vaccines, nearly all girls preferred receiving the vaccine in a single dose [96]. Similarly, a Canadian study on attitudes toward a hypothetical HIV vaccine revealed that most participants preferred a single injection without booster follow-ups [116]. In Hong Kong, a mother mentioned her husband’s refusal to allow their daughter to receive additional vaccinations due to concerns about excessive injections [57]. Similarly, parents in the UK voiced concerns about children receiving multiple injections within a short period [117].
In addition to a preference for receiving a single-dose vaccine, preferences also emerged regarding combining multiple vaccines into a single injection, while participants also acknowledged potential challenges. In Australia, young women desired vaccines that could protect against multiple diseases but recognized the complexity of producing combined vaccines [91]. This assumption was mirrored in an American study among HIV high-risk groups where participants acknowledged that, while theoretically preferred, a single-dose vaccine protecting from all HIV subtypes might not be realistic or adequate as it might make developing the vaccine even more challenging [76]. In the UK, parents also expressed concerns about the limitations of the influenza vaccine, recognizing that it only protects against the prevailing strain in a given year and not against all potential strains [118]. In contrast to this, a Malaysian parent expressed a preference to avoid combination vaccines [56].
Place
Adequate supply of vaccines and accessibility of service delivery point
A study conducted among ethnic minority and White British groups revealed that they preferred to receive vaccines in community health care settings like hospitals, and other places that they deemed safe [73]. However, in a study on maternal vaccination in Mexico and Panama, participants mentioned occasions when public hospitals experienced vaccine shortages, prompting a desire to access both government and private health facilities [119,120]: ‘they (public hospitals) ran out of vaccines. They tell you to come back later or try other hospitals -or you can go to a private one’ [119]. Participants across several studies in the U.S., Greece, the UK and Canada [65,91,121,124] emphasized the importance of conveniently accessible vaccination locations: ‘You shouldn’t have to drive any longer than 20 minutes to access a vaccine’ [91].
In Zambia and Canada, participants proposed implementing door-to-door vaccination programs to target individuals who are sick or have disabilities [75,122]. Additionally, parents of teenagers eligible for HPV vaccination expressed a preference for school-based immunization programs due to their straightforward logistics [123].
Assurance for privacy and preference for well-trained healthcare providers
Some participants in the U.S. expressed privacy concerns [125] and reservations about the level of training received by healthcare workers (HCWs) in public vaccination settings [108]. Similarly, parents in the U.S. preferred not to have their children vaccinated at community pharmacies, citing concerns about the clinical expertise of pharmacists [108]. Participants in Canada, Mexico and the U.S. preferred receiving vaccines at the clinic run by their healthcare providers [116,119,125]. In the UK, members of Polish and Romanian communities raised concerns about the qualification of nurses administering the vaccines, as vaccines in Poland are exclusively administered by medical doctors [117].
Price
Affordable vaccination option and trusted vaccine brands
Participants expressed hesitancies to avail of vaccines due to high prices, particularly if their income was limited [57,59,127]. In both Hong Kong and the U.S., participants with multiple children preferred to know the required dosage regimen beforehand due to concerns about potential expense [57,66,126]. Several studies concluded that vaccines should generally be given for free [62,72,82,121], or at least at an affordable price [57,65,82,128,129], irrespective of citizenship or life situation [116]. Purchasing vaccines could be quite costly, causing some people to decline, especially if they believe they are already immune to these diseases [57,61].
Respondents in the U.S. studies indicated that vaccine coverage through health insurance would serve as a significant driver for uptake [66,67,126]. Furthermore, participants in Malaysia preferred life-long governmental compensation to those who suffered from severe vaccination side effects to alleviate fears of catastrophic healthcare expenditure following vaccination [56]. Brand preferences also influenced the vaccination costs. Participants in various studies expressed preferences for specific vaccine brands or types not commonly available in public health facilities due to concerns about the quality of the vaccines [74,117,127,129,131], i.e. people have to pay more because they want a specific vaccine which is not covered by the government [57]. Brand-conscious people wanted to know which vaccine brands were more suitable [61,104,135] and this was particularly evident during the COVID-19 pandemic, where preferences were shaped by perceptions of certain brands as safer, more effective, or more trustworthy than others [132–135].
Preference for a cost-effective vaccine that reduces financial and healthcare burden
Participants in studies across Canada, Australia, the U.S., and India expressed a willingness to spend money on vaccines that would protect them from diseases [67,77,121,128]. They preferred the upfront cost of vaccination over potentially higher expenses associated with disease management and treatment at a later time [67,100]. This perspective on the cost-effectiveness of vaccination was echoed by a community member in India, where antenatal influenza vaccination was seen to prevent disease and reduce healthcare costs: ‘If she is vaccinated prior and her immunity increases, then she won’t suffer from these diseases. That means it will not increase the financial burden for healthcare, and patient’s expenses are saved’ [136].
Reduction of secondary costs associated with vaccination
Participants across studies in India, Zambia, U.S., and Australia also voiced preferences regarding vaccination schedules that minimize indirect costs [122,130,137,138]. In Zambia, a study was conducted to investigate the impact of vaccines in informal settlements. The study found that while most participants preferred following conventional vaccination schedules, some individuals, particularly men, expressed a preference for receiving vaccines on Saturdays and Sundays, when they were not required to work [122].
Promotion
Preferred content of vaccine information, sources and channels
Vaccine information influences an individual’s decisions regarding vaccine uptake and acceptance, as highlighted in several studies [85,87,92,120,125,128,131,141–144,152]. To make informed decisions, participants in the U.S., Mexico and Panama expressed a desire for comprehensive information about the value of vaccination [70,94,119,120]. They preferred to know details such as the type of vaccine, how it works, diseases it prevents, dosage regimen, side effects, benefits, and risks [56,59,69,106,116,122,139,140]. Participants emphasized the importance of receiving accurate and transparent information, with one British participant suggesting: ‘ … I think it would make it easier if it was true information, stating that it was for this strain of flu and this is what’s happened to people that have had it and people that haven’t had it’ [139]. This sentiment was echoed by a Haitian participant who regretted consenting to her child receiving the HPV vaccine due to feeling uninformed at the time [67].
Trusted messengers were identified as crucial in conveying vaccine information effectively [83,146]. Yet, who was considered a trusted source varied considerably even within populations. Studies in Canada, the UK, and Vietnam found that participants sought information from healthcare providers, while others preferred information from newspapers, social media, and mainstream media [73,88,98,106]. Participants valued HCWs who patiently explained vaccine purposes while emphasizing both the benefits and potential side effects, such as symptoms and complications of the underlying disease [56,61,140,145]. Participants across several studies expressed reliance on medical doctors for health decisions due to trust and confidence in their expertise [67,69,83–85,88,102,113,120,121,142,144,146,147].
Additionally, community volunteers and religious authorities were also recognized as trusted sources of vaccine information [128]. In Zambia, community volunteers supported vaccination efforts by addressing community concerns, easing fears, and creating spaces where people could openly discuss their reservations [122]. Participants also emphasized the importance of involving church leaders in vaccine information dissemination, recognizing their trusted role within the community and their ability to reach the congregation effectively [114,122].
Meanwhile, in the Netherlands, participants preferred traditional methods of information delivery, such as face-to-face consultations and the distribution of vaccine leaflets [59]. Canadian HCWs identified multiple channels for advertising information, including school-based campaigns, large banners, smartphone and television messaging, and vaccine reminder systems [148]. Some studies also highlighted preferences for vaccine information in multiple languages and presented in accessible language without scientific jargon [59,75,89,117,135,140].
Freedom of choice on mandatory and optional vaccines
Across the included studies, many participants regarded childhood vaccinations as mandatory, aligning with their country’s national immunization program [59,131]. However, when it came to optional vaccines–such as the HPV vaccine, which was not required for school entry–some participants expressed a preference for exercising their personal autonomy and making their own vaccination decisions [64]. In the U.S., African American women felt that the HPV vaccine should not be mandatory [67]. The freedom of choice was also echoed for maternal vaccination from a participant from the Netherlands [78] who nevertheless acknowledged that freedom of choice should not always prevail. While several studies found strong preference for autonomy in decision-making [64,67,78,87,150], with many arguing that mandatory vaccination would juxtapose with freedom of choice [113,127,149], there was no concensus with optional vaccines, indicating complexity and challenges associated with balancing individual autonomy and public health objectives.
Discussion
Our article synthesizes qualitative studies examining general populations’ vaccine preferences. Our findings outline vaccine preferences across all four domains of the 4Ps framework: Product, Place, Price, and Promotion. Product-associated preferences relate to vaccine quality, safety, and specific brands or origins, particularly for new vaccines. Place-associated preferences underscore the importance of vaccination settings, such as a doctor’s clinic or community health center, and the perceived competence of the vaccine administrator. Price-related considerations, particularly affordability and cost-effectiveness, play a crucial role in shaping vaccine acceptance, especially for new vaccines, as they significantly influence the level of trust and willingness to adopt. Promotion preferences included specific side-effect information dissemination, one-on-one methods of communication, and the involvement of credible messengers (e.g. physicians).
Our findings align with earlier systematic reviews that have explored ethical considerations in vaccine development and vaccination process [153] and factors influencing acceptance [33,154]. In our meta-ethnography, the quality and safety of vaccines emerged as primary preferences for vaccination. However, individuals often seemed to set an exceptionally high bar for vaccine quality, efficacy, and safety without actually considering the broader public health benefits [155]. Specifically, participants often prioritized the perceived risks of potential side effects from vaccines over the dangers of remaining unvaccinated [58,156,157], particularly for novel vaccines. Consequently, when individuals receive a vaccine (and endure the side effects) but later contract the infection, they tend to perceive that the vaccine has failed, reinforcing their skepticism. This asymmetry in risk perception is critical for understanding vaccine hesitancy and poses an opportunity for public health messaging [14]. Although vaccinated individuals may still contract the infection, the critical point is that they are substantially less likely to develop severe disease or require hospitalization [158,159]–a distinction that is essential for the public to have a clear comprehension of and trust in vaccines [160,161].
Our findings also highlight that individuals who opted for vaccination often emphasize the direct benefits for themselves or their children, such as protection during pregnancy or against HPV [157]. In contrast, societal benefits–including protecting others, reducing community disease burden or contributing to herd immunity–were mentioned less frequently. Although a study expanded the view of vaccine safety to include minimizing side effects and supporting overall health [162], the prevailing emphasis remained on individual rather than the societal health gains. While demand-creation approaches are broadly necessary to close vaccination gaps, our findings suggest that promotional messages highlighting personal protection may resonate more strongly with individuals than appeals to societal benefits [157]. Nonetheless, balancing these perspectives remains critical, particularly for novel vaccines such as COVID-19, which were recommended for entire populations–even those at low personal risks–precisely because of their population-level value [163].
The public’s confidence in the scientific basis of vaccination may not extend to new or innovative vaccines, even if these are based on well-established technologies [155]. This may indicate a more general doubt or lack of trust in the advancement of healthcare, especially when it pertains to novel or unfamiliar products [141]. Notably, in our meta-ethnography, vaccine composition, particularly vaccine ingredients, was a major consideration for novel vaccines, as individuals sought assurances that vaccine would not conflict with their cultural or religious beliefs. This aligns with a study conducted in Islamic-majority countries [42], where individual concerns about safety and religious compatibility outweighed attention to broader societal considerations. This aspect highlights the importance of transparency in presenting clinical trial data and stages of vaccine development, particularly in regions with diverse cultural and religious contexts. Communicating the continuity and shared principles between established and new vaccines, along with the critical role vaccines play in averting serious disease, could potentially narrow this divide.
In terms of vaccine development and composition, our review also highlighted a general preference for single-type vaccines over combined ones. The idea of receiving multiple shots within a short period of time to deliver different vaccines, as well as the concept of booster shots for the same vaccine, were often unpopular. This preference presents a significant challenge for vaccine developers, as reducing the number of shots typically necessitates combining vaccines into a single vial, and booster shots often are essential for maintaining vaccine effectiveness. Importantly, the reasons underlying the preference for fewer shots varied: in some cases, concerns centered on safety or discomfort, financial constraints, or the indirect costs of repeated clinic visits. These variations did not clearly align with specific country settings but rather appeared across individual- and structural-levels. While disentangling these influences was beyond the scope of this review, we emphasize that preferences should be understood as embedded within broader determinants of health-seeking behavior. Further research is recommended to explore the underlying causes and identify potential strategies to navigate trade-offs. Additionally, these findings highlight the need to refine public messaging strategies that more effectively communicates the benefits and safety of combined vaccines and multiple-shots vaccines.
While many studies have primarily focused on discussions surrounding HPV and COVID-19 vaccines [41,60,61,64–68,82,83,85,91,96,111,116,123,126,140,156,159,163–165], our findings underscore the contested and context-specific nature of vaccination narratives [166]. Vaccine preferences are shaped by multiple, intersecting factors, including individual’s current condition, prior experiences with vaccination, government implementation strategies, and broader public discourses (e.g. vaccine-related controversies) [167]. Our review not only identifies specific preferences but also sheds light on how these preferences are formed. For many, decisions are rooted in perceptions of vaccine quality and accessibility; however, uncertainties around novel vaccines were magnified by inconsistent and often conflicting public health messaging, which in turn eroded confidence [166]. Traditional and social media played a role in this process, as people actively sought information on safety profiles and potential side effects–a finding also observed in other systematic reviews [27,33]. The COVID-19 pandemic intensified the fragility of vaccine confidence, as misinformation spread rapidly and undermined acceptance of new vaccines [157]. Taken together, these findings underscore the importance of rebuilding trust through clear, transparent, and consistent communication strategies that addresses both safety concerns and misinformation, thereby reinforcing the foundations of vaccination programs [168].
In addition to identifying specific vaccination preferences, our review also provides insights into how such preferences are shaped by contextual factors. In LMICs, accessibility and vaccine availability often emerged as paramount considerations, with individuals’ choices closely tied to whether vaccines could be obtained easily and reliably. By contrast, studies from HICs suggested that location of vaccination was rarely a primary concern, except in circumstances where privacy or convenience became salient. Consistent with findings from other studies [165,169], vaccine supply is a critical factor influencing vaccine uptake across settings. Fewer studies directly explored perceptions of vaccine price (and its associated secondary costs) as a determinant of uptake [170,171]. Since a majority of routine vaccines are typically included in government immunization programs, the uptake of vaccines excluded from these programs will, among other factors, depend on their price. Some studies indicate that efforts to overcome the barrier of vaccination accessibility due to cost are yielding beneficial results [82,91,121]. Therefore, the discussion of vaccine equity and supply chain sustainability warrants further evaluation.
Finally, our analysis highlights expressed vaccine preferences but does not always capture the underlying reasons that shape them. For example, the preference for single-dose over multi-dose vaccines may stem from very different concerns depending on context–ranging from accessibility, affordability to work-related opportunity costs or broader socio-cultural factors. Preferences, therefore, should not be interpreted as root causes of hesitancy or acceptance, but rather as proximal expressions of deeper structural and contextual dynamics. While our synthesis captures vaccine preferences across these domains, our findings suggest that these preferences are not necessarily direct underlying drivers of vaccine hesitancy or uptake or confidence, but rather as expressions of how individuals navigate broader structural and contextual factors. Understanding preferences offers valuable insight into how individuals articulate their priorities when navigating vaccination decisions, even if these do not align neatly with the fundamental drivers of uptake or confidence. Future research is needed to further disentangle these interactions and clarify the mechanisms linking preferences with actual vaccination behaviors.
Review strengths and limitations
This meta-ethnographic review provides evidence regarding the general population’s vaccine preferences, drawing on comprehensive searches across several databases with extensive search strings and overseen by a biomedical librarian (JL). However, some limitations must be considered. First, the literature search was restricted to studies published up to June 2023. This cut-off reflected the fixed timeline of the project and resource constraints, rather than an intentional exclusion of more recent work. Consequently, newer evidence published after this date could not be captured. Second, while our iterative methodology during literature extraction enabled a systematic examination of vaccine preferences and their relationship with confidence and uptake, the transferability of our findings may be constrained by the large number of studies conducted in HICs, the underrepresentation of vulnerable or marginalized groups, and variation in qualitative approaches used to explore vaccine preferences. Finally, as many studies were conducted in higher-income contexts, interpreting our results across more diverse settings remain challenging given the strong influence of context on perceptions.
Conclusion
This meta-ethnographic review underscores the need to adopt a holistic approach when considering vaccination preferences in relation to intentions and uptake. Our findings suggest that policymakers and vaccine program managers must address contextual nuances and engage in collaborative efforts with diverse agencies to meet evolving vaccine preferences. Notably, there are significant gaps in the literature, particularly concerning vaccine preferences in LMICs. We hope for our findings to stimulate discussions on effectively integrating the general public’s vaccine preferences into existing vaccination programs, bridging the gap between preferences and actionable interventions.
Supplementary Material
Supplementary Table 3_COREQ.pdf
Supplementary Table 2_Characteristics of Included Studies_Clean Copy_26 Aug 2025.docx
Supplementary Table 1_Summary of Research Databases.pdf
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1CDC. Ten great public health achievements — United States, 2001–2010. 2011. 619–22.21597455 · pubmed ↗
- 2WHO. Raising awareness of immunization. World Health Organization. Available from: https://www.who.int/westernpacific/activities/raising-awareness-of-immunization
- 3Shattock AJ, Johnson HC, Sim SY, et al. Contribution of vaccination to improved survival and health: modelling 50 years of the expanded programme on immunization. Lancet. 2024;403:2307–2316. doi: 10.1016/S 0140-6736(24)00850-X 38705159 PMC 11140691 · doi ↗ · pubmed ↗
- 4WHO. Millennium development goals (MD Gs). World Health Organization; 2018. Available from: https://www.who.int/news-room/fact-sheets/detail/millennium-development-goals-(mdgs)
- 5World Health Organization. Organisation mondiale de la S. Millennium Development Goals (MD Gs). World Health Organization; 2018.
- 6Alliance GTV. Millennium development goals: gavi contributed to the eight millennium development goals 2020. updated 2020 Feb 18 [cited 2025 Jun 2]. Available from: https://www.gavi.org/our-alliance/global-health-development/millennium-development-goals#:~:text=MDG%205:%20improve%20maternal%20health,low%2Dincome%20countries%20were%20vaccinated
- 7Nations U. The millennium development goals report 2015. New York: United Nations; 2015.
- 8Maternal Immunization. Protected together. International Vaccine Access Center. 2020 [cited 2025 Jun 2]. Available from: https://immunizationevidence.org/maternal-immunization-protected-together/?utm_source=chatgpt.com