Impact of social vulnerability on glycemic control and diabetes technology use in youth with type 1 diabetes
Nicholas R. Banull, Melanie Bryan, Stephen I. Stone, Hope Shimony, Amanda Ingram, Ana María Arbeláez

TL;DR
This study shows that access to diabetes technology can reduce the impact of social vulnerability on blood sugar control in young people with type 1 diabetes.
Contribution
The study demonstrates that diabetes technology use reduces glycemic disparities linked to race and socioeconomic status in youth with type 1 diabetes.
Findings
Black patients, Medicaid recipients, and those with higher social vulnerability used diabetes technology less frequently.
Insulin pump or CGM use was associated with lower HbA1c levels, especially in disadvantaged groups.
Higher DKA rates were linked to older age, higher HbA1c, Black racial identity, and insulin pump use.
Abstract
Diabetes technology has been shown to improve glycemic control in people with type 1 diabetes (T1DM). Despite their benefits, these technologies are used less frequently by youth from lower socioeconomic backgrounds and racial minorities worldwide. This study aimed to examine the relationship between social vulnerability, disparities in diabetes technology use, and glycemic control in youth with T1DM. This retrospective billing code analysis included 1,460 patients with T1DM, aged ≤ 23 years old, who were seen at a large academic diabetes center in the Midwest between January 2020 and April 2022, before the expansion of insurance coverage for diabetes technology in Missouri. We analyzed data on number of visit encounters, use of a continuous glucose monitor (CGM), use of an insulin pump, area of deprivation index (ADI) score, age, sex, race, and type of insurance. A predictive multiple…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
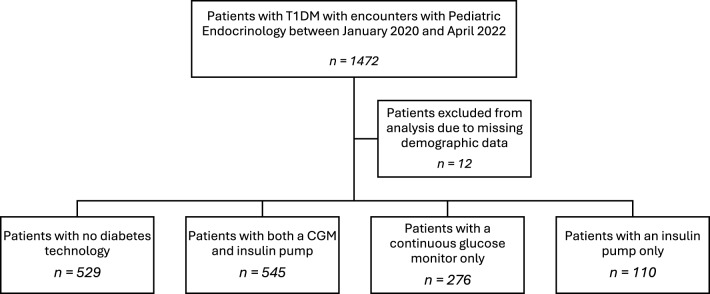 Figure 1
Figure 1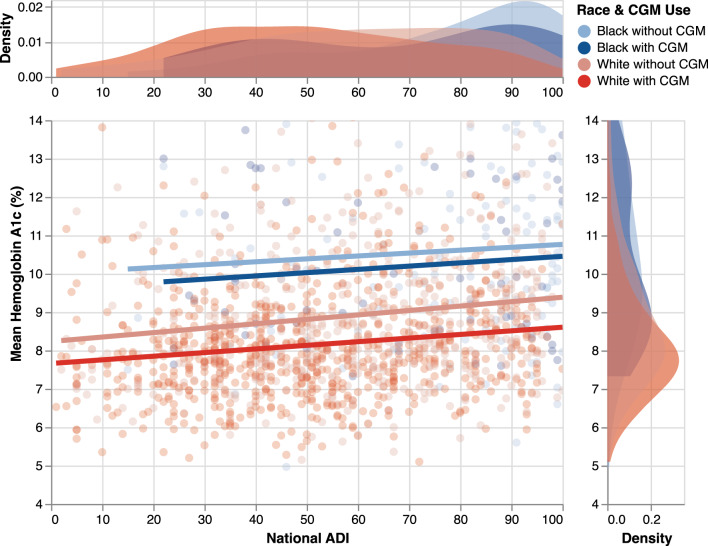 Figure 2
Figure 2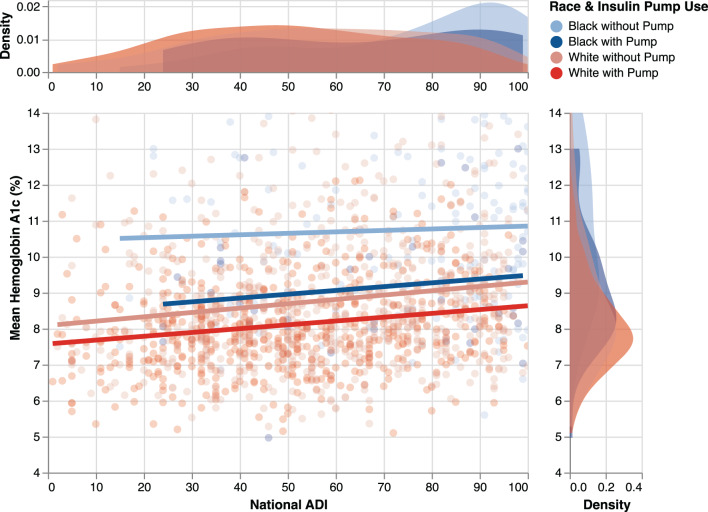 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDiabetes Management and Research · Diabetes and associated disorders · Diabetes Management and Education
Background
Advancements in diabetes technology, particularly continuous glucose monitors (CGMs) and continuous subcutaneous insulin infusion (CSII) via insulin pumps, have been shown to improve glycemic control in youth with type 1 diabetes mellitus (T1DM) [1, 2] when compared with multiple daily injections [3]. These devices have been shown to increase time in the target glucose range, lower rates of hypoglycemia, and reduce admissions for diabetic ketoacidosis (DKA) [3–5].
Despite these significant benefits, the use of CGMs, insulin pumps, and closed-loop insulin delivery systems in children worldwide remains low due to cost and barriers to adopting this technology. Although the uptake of these devices is increasing in the US, their usage is notably less frequent among children from lower socioeconomic backgrounds and among ethnic and racial minorities [6–14]. This disparity in the use of diabetes technology may contribute to the well-documented differences in clinical outcomes for Hispanic and non-Hispanic Black individuals with T1DM as compared to their White peers [15]. Furthermore, research indicates that racial disparities in diabetes outcomes persist even after controlling for socioeconomic status, suggesting that mistrust, implicit bias, and systemic racism may have an impact on diabetes outcomes for non-White individuals with T1DM [16, 17].
This study aimed to assess the relationship between social vulnerability, disparities in diabetes technology use, and clinical outcomes in youth with Type 1 diabetes (T1DM). Understanding the mechanisms that drive these disparate outcomes is crucial to providing more equitable, comprehensive, and appropriate care to all children with T1DM and their families.
Methods
Participants and data collection
A retrospective data analysis was conducted using billing data from patients with T1DM, who were under 23 years old, and had been seen at Washington University Pediatric Diabetes Clinics between January 2020 and April 2022. Patients with an E10 International Statistical Classification of Diseases and Related Health Problems, Tenth Revision (ICD-10) diagnosis, corresponding to T1DM, were included in the study. Although this time frame encompasses the COVID-19 pandemic, patient care for those with T1DM was not interrupted at this academic center during the study period. However, some visits were switched to virtual appointments from in-office visits from March 2020 to July 2020. This change was made to ensure that patients met the annual visit requirements set by the American Diabetes Association guidelines and to prevent any interruption in their care.
Outcome variables
The primary outcome variables were glycated hemoglobin (HbA1c), which reflects chronic glycemic control, and rates of diabetic ketoacidosis (DKA). Each encounter included in this study corresponded to a HbA1c measurement. Mean HbA1c was estimated by calculating the average of all HbA1c measurements for each individual patient over the two-year study period including HbA1c measures at diagnosis. DKA occurrences were determined by the number of inpatient admissions in DKA for each patient over the two-year study period. Current Procedural Terminology (CPT) codes and demographic variables were extracted from the electronic medical health record (EMHR) to assess potential covariates that could have influenced clinical outcomes. These covariates included age, sex, race, social disparity, insurance, number of visit encounters, use of an insulin pump, and/or a continuous glucose monitor. Individuals were considered pump or CGM users if they had utilized the respective technology for more than one month at any point during the study period. Throughout the study, all patients in the practice using CGM used real-time continuous glucose monitors (rtCGM). Social disparity was assessed using the Area Deprivation Index (ADI), which provides an objective comparison of relative socioeconomic conditions of neighborhoods across the United States, based on census data from the 2018 American Community Survey. The ADI takes into account demographic and socioeconomic factors that affect a community’s ability to respond to external stressors, such as neighborhood household income, housing quality, education, and employment. The ADI scores were calculated using patients’ home addresses and The Neighborhood Atlas® software from the University of Wisconsin [18]. Higher ADI scores indicate a higher level of social deprivation.
Statistics
Descriptive statistics were calculated for all variables, including mean, standard deviation, and median. Univariate analysis was performed to identify potential influencing factors on HbA1c. Variables were included in a predictive multiple linear regression model based on either statistical significance or clinical relevance. To assess for normality, distribution of unstandardized residuals and normalized Q-Q plots were analyzed. Multicollinearity was assessed by calculating variance inflation factors using a linear regression model. Poisson regression was initially performed on non-normally distributed outcome variables to assess for overdispersion. Negative binomial regression with a log link was performed using DKA as an output variable and estimated using fisher scoring with maximum likelihood and type III Wald Chi-Square tests. Results were considered statistically significant if p < 0.05 in two-tailed tests. Analyses were conducted using the statistical package SPSS© Version 27. Graphics were produced using Adobe Illustrator, SPSS, and Vega-Altair [19]. This study was approved by Washington University’s Human Research Protection Office Committee and waiver of consent was granted.
Results
Between January 2020 and April 2022, a total of 1,472 unique patients with T1DM were seen at the Department of Pediatric Endocrinology Diabetes outpatient clinics at Washington University in St. Louis (see Fig. 1). Twelve patients were excluded from the analysis due to missing demographic data or an inability to calculate ADI, for a total of 1,460 patients included in this study. These patients had 7,410 encounters during the analysis period.Fig. 1. Total number of patients included in the study after excluding for missing data. The distribution of patients using different diabetes technologies is also shown
Descriptive statistics
Population characteristics are summarized in Table 1. The mean age was 13.27 (SD = 4.4) years, and 54.6% of the patients being male. The patients’ racial composition was 84.6% White, 13.2% Black, and 2.2% other. 66.4% of patients were on managed care insurance, 26.5% were on Medicaid, and 7.1% were on other types of insurance. The overall ADI score for the cohort was 57.0 (SD = 24.7.) The mean ADI of Black patients was 73.80 (SD = 23.6), while white patients had a mean ADI of 54.38 (SD = 23.9). 37.3% of patients used pump and CGM, 7.5% used pump only, 18.9% used CGM only, and 36.2% did not use diabetes technology.Table 1. Characteristics of study participantsNo Technology (n = 529)CGM Only (n = 276)Pump Only (n = 110)Pump and CGM (n = 545)Total (n = 1460)Age0–1 y2 (66.7)1 (33.3)0031–5 y32 (36.8)22 (25.3)4 (4.6)29 (33.3)875–11 y144 (36.4)60 (15.2)34 (8.6)157 (39.8)39511–18 y304 (35.6)165 (19.3)67 (7.8)318 (37.2)85418–25 y47 (38.8)28 (23.1)5 (4.1)41 (33.9)121Mean Age (σ)13.3 (3.3)13.5 (4.6)13.4 (4.1)13.2 (4.2)13.3 (4.4)SexMale307 (38.5)156 (19.6)52 (6.5)282 (35.3)797Female222 (33.5)120 (18.1)58 (8.7)263 (39.7)663InsuranceCommercial1 (16.7)005 (83.3)6Managed Care270 (27.8)192 (19.8)67 (6.9)440 (45.4)969Managed Medicaid216 (55.8)66 (17.1)34 (8.8)71 (18.3)387Medicaid21 (60)6 (17.1)3 (8.6)5 (14.3)35Medicare1 (100)0001No Coverage2 (40)1 (20)2 (40)05Other13 (26.0)10 (20)3 (6.0)24 (48.0)50Self-Pay5 (71.4)1 (14.3)1 (14.3)07RaceAmerican Indian or Alaska Native2 (50)01 (25)1 (25)4Asian6 (35.3)3 (17.6)2 (11.8)6 (35.3)17Black or African American116 (60.1)41 (21.2)11 (5.7)25 (13.0)193Other Pacific Islander3 (33.3)3 (33.3)03 (33.3)9Other2 (50)1 (25)01 (25)4White400 (32.4)228 (18.5)96 (7.8)509 (41.2)1233**Mean HbA1c % (σ)**9.4 (2.2)8.8 (1.9)8.7 (1.4)8.1 (1.3)8.7 (1.9)**Mean ADI (σ)**64.0 (24.3)55.0 (23.7)59.4 (23.33)50.3 (23.9)56.8 (24.7)**Mean Number of DKA Admissions (σ)**0.77 (2.0)0.82 (1.7)0.83 (1.5)0.53 (1.6)0.69 (1.8)EncountersTotal Encounters2028 (27.4)1650 (22.3)564 (7.6)3168 (42.8)7478Mean Encounters (σ)3.8 (2.8)6.0 (2.8)5.1 (4.8)5.8 (2.2)5.1 (3.0)
The mean number of encounters per patient was 5.1 over the study period (SD = 3.0). Each patient encounter was associated with a corresponding HbA1c result. The overall mean HbA1c was 8.72% (SD = 1.9) for all patient encounters. For White patients, the mean HbA1c was 8.5% (SD = 1.7); while Black patients had a mean HbA1c of 10.5% (SD = 2.3). Patients without diabetes technology had a mean HbA1c of 9.4% (SD = 2.2). The mean HbA1c for patients using a CGM was 8.8% (SD = 1.9), for those using an insulin pump was 8.7% (SD = 1.4), and patients using both a CGM and an insulin pump had a mean HbA1c of 8.1% (SD = 1.3)
The mean number of DKA admissions per patient was 0.69 (SD = 1.8). White patients had a mean of 0.52 (SD = 1.4) DKA admissions, while Black patients averaged 1.79 (SD = 3.1) DKA admissions. For patients without diabetes technology, the mean number of DKA admissions was 0.77 (SD = 2.0), for those using an insulin pump it was 0.83 (SD = 1.6), and for those using a CGM it was 0.82 (SD = 1.7). Patients utilizing both a CGM and an insulin pump had a mean number of 0.53 (SD = 1.6) DKA admissions.
Multivariable regression analysis
HbA1c
Unstandardized residuals did not demonstrate a normal distribution for HbA1c (Kolmogorov-Smirnov p < 0.001). Given large sample size, multiple linear regression was performed using HbA1c as an outcome variable. Univariate linear regression analysis showed that ADI, insulin pump use, CGM use, simultaneous use of both pump and CGM, race, and insurance were all statistically significant predictors of HbA1c levels. As shown in Table 2, multiple linear regression demonstrated that higher ADI, Black racial identity, and Medicaid insurance were significantly associated with increased HbA1c levels, whereas insulin pump and CGM usage were significantly associated with lower HbA1c levels. The multiple linear regression model was significant with an adjusted R^2^ value of 0.206, and ANOVA analysis found F (11,1459) = 35.5, p < 0.001. (Figs. 2, 3).Table 2. Multiple linear regression using mean HbA1c as output variableUnstandardized CoefficientsStandardized Coefficients95% CI for BetaBStd. ErrorBetatpLowerUpperAge0.0140.010.0321.3740.17−0.0060.034ADI0.0060.0020.0782.9970.0030.0020.01Male Sex0.1340.0890.0351.5070.132−0.040.309Number of Encounters0.0030.0160.0050.1940.846−0.0280.034RaceBlack/African American1.3860.1420.2489.781 < 0.0011.1081.664Other−0.3280.303−0.025−1.080.28−0.9220.267InsuranceMedicaid0.660.1150.1545.75 < 0.0010.4350.886Other0.1020.1760.0140.5810.561−0.2430.448Diabetes TechnologyCombined Pump and CGM Use−0.0540.217−0.014−0.250.803−0.4810.372Insulin Pump Use−0.410.179−0.1082.2890.022−0.762−0.059CGM Use−0.3450.132−0.091−2.610.009−0.604−0.086Fig. 2Linear regression plot of mean HbA1c (%) by national area deprivation Index and stratified by patients’ CGM usage and race. The kernel density plot (distribution of observations) of HbA1c is shown to the right, and the kernel density plot of the ADI scores is shown aboveFig. 3Linear regression plot of mean HbA1c (%) by national area deprivation Index and stratified by patients’ insulin pump usage and race. The kernel density plot (distribution of observations) of HbA1c is shown to the right, and the kernel density plot of the ADI scores is shown above
DKA
Unstandardized residuals for DKA did not demonstrate a normal distribution (Kolmogorov-Smirnov p < 0.001). Poisson regression demonstrated deviance Value/df of 1.433, a Pearson Chi-Square Value/df of 1.842, and AIC of 3272.02, suggestive of overdispersion and a poor model fit. Negative binomial regression demonstrated a deviance Value/df of 0.805, a Pearson Chi-Square Value/df of 1.036, and AIC of 2885.9. As shown in Table 3, the negative binomial regression demonstrated that age, HbA1c, number of encounters, Black/African American racial identity, and Medicaid insurance were associated with significantly increased rates of DKA (p < 0.001, p < 0.001, p < 0.001, p = 0.01, p = 0.001, respectively). Additionally, insulin pump use was associated with increased rates of DKA (p = 0.03). However, both combined CGM and insulin pump use and CGM use were not associated with lower rates of DKA (p = 0.06, p = 0.344, respectively).Table 3. Negative binomial regression with DKA occurrences as outcome variable95% CI for exp (b)BStd. ErrorSig.exp (b)LowerUpperAge0.0500.011 < 0.0011.0511.0281.075National ADI0.0010.0020.7071.0010.9971.005Male Sex−0.0120.0930.8970.9880.8231.187Mean HbA1c0.2610.025 < 0.0011.2981.2361.362Number of Encounters0.1280.013 < 0.0011.1361.1081.165RaceOther Race0.3140.3020.2991.3690.7572.476Black/African American0.3360.1310.0101.4001.0821.810InsuranceOther Insurance0.5820.1690.0011.7901.2872.491Medicaid Insurance0.3910.1150.0011.4781.1801.851Diabetes TechnologyCombined Pump + CGM Use−0.4050.2170.0620.6670.4361.021Pump Use0.3860.1780.0301.4711.0392.085CGM Use0.1260.1330.3441.1340.8741.472
Discussion
In this study, Black patients exhibited approximately 2% higher HbA1c and higher rates of Diabetic Ketoacidosis (DKA) compared to White patients, validating the impact of racial and socioeconomic disparities in glycemic control in youth with T1DM. HbA1c levels in this cohort were influenced by technology use, race, insurance, and higher social adversity as indicated by higher Area Deprivation Index (ADI) scores. While Black patients had higher rates of Medicaid use and higher ADI scores compared to White patients, the relationship between HbA1c levels and race remained independent of socioeconomic and insurance status. Interestingly, unlike findings from other studies, lower socioeconomic status and CGM use did not emerge as statistically significant predictors of DKA [20]. This data suggests that targeted interventions designed to improve HbA1c, such as the use of continuous glucose monitors in marginalized communities, could still positively influence DKA admission rates. Even though our study population was more disadvantaged than the national average, both this study and others indicate that the factors contributing to racial disparities in glycemic control among youth with T1DM go beyond ADI, insurance type and technology use. Other studies have suggested that factors influenced by institutional racism may be involved [6, 14].
Despite the demonstrated benefits of diabetes technology in improving patient outcomes for T1DM, many patients in the United States and around the world still lack access to these technologies. Prescription and usage of diabetes technology are influenced by various factors, including availability, affordability, differences in coverage among payor systems in different states, preferences of patients and their families, and their trust in the healthcare system, among others [21, 22]. Process barriers may also impact a patient or family’s willingness or ability to access diabetes technology. In our clinical practice, CGMs are typically initiated at diagnosis after discussion of insurance coverage and out-of-pocket costs with families. Pump therapy can be initiated as early as one month after diagnosis and requires participation of patients and/or caregivers in a brief pump course and knowledge assessment.
This study was conducted at a time when insurance coverage for diabetes technologies was limited in our state. This may explain why only 56% of the patients in this study were using a CGM and 45% had an insulin pump. This allowed us to ascertain the effects of limited technology access in underserved communities as it occurs in many regions around the world. Thus, as we continue to advocate for improved access and coverage of diabetes technology for all patients, this study suggests that the impact of such access may be even more significant for the most vulnerable patients.
This and other studies indicate that racial and socioeconomic disparities in technology usage exist among youth with T1DM [6–14]. However, further research is needed to effectively evaluate the trends and motivations behind diabetes technology prescription from all involved parties and to better understand the factors that contribute to the successful use of such technology. Prior studies suggest that provider bias may lead to racial disparities in diabetes technology use, with Black patients facing lower rates of device initiation and higher rates of device discontinuation [17, 23]. However, children from racial and socially disadvantaged backgrounds remain significantly under-represented in clinical trials for FDA-approved modern diabetes technologies. This critical gap underscores the urgent need to study diverse populations of children with T1DM to better understand how these technologies impact these underserved patients. Our cohort included youth from various racial and socioeconomic backgrounds, reflecting the makeup of the 2022 US population, and a the percentage of patients identifying as Black was slightly higher than typically reported among T1DM populations [24]. Therefore, this study provides a valuable opportunity to examine the relationship between social vulnerability and diabetes outcomes, as well as how the use of diabetes technology, such as CGM or Continuous subcutaneous insulin infusion via insulin pump (CSII) affects diabetes outcomes across different populations.
CSII offers several advantages over multiple daily injections including a reduction in the disease burden of patients with T1DM and is associated with better glycemic control in numerous studies [25, 26]. While insulin pump usage has been rising substantially among young individuals with T1DM, adoption rates for diabetes technology in many vulnerable populations remain notably lower than the national average [14]. This study indicated lower usage of CGM and pumps among black patients, which may be related to insurance coverage at the time of the study. Although we acknowledge that improvements in glycemic control may be driven by more individualized insulin dosing, prompt pump adaptation to temporary changes in insulin sensitivity, and increased user satisfaction [27] provided by diabetes technology, our findings showed that the use of insulin pumps or CGMs alone is associated with a lower HbA1c levels, even after accounting for other variables. Furthermore, these data suggest that while insulin pump or CGM use is associated with lower HbA1c levels in all patients with T1DM, this difference was especially notable in patients with higher ADI scores and in Black patients.
Prior studies have noted both increases and decreases in rates of DKA in patients with insulin pump use [28, 29]. This study found an association between insulin pump use and increased DKA occurrences. Insulin pump use has a theoretical higher risk of DKA as CSII exclusively uses short acting insulin, which if disrupted and unrecognized could lead to poorer short term glycemic control and DKA. Additionally, insulin pump therapy has been shown to be more expensive to patients and their families than insulin injection, which may lead to increased difficulty adhering to insulin therapy [30]. Rates of DKA in individuals with insulin pump use in existing diabetes literature may vary due to availability of CSII closed loop systems. During our study period, legislation may have influenced availability of these systems. Our study population was significantly more disadvantaged than the national average and may be exposed to additional social determinants of health that are not able to be encumbered by our study design, leading to increased rates of DKA admissions associated with insulin pump use.
Although this is not a clinical trial and we are limited to draw definitive conclusions regarding the direct impact of pump or CGM use on glycemic control, this study suggests that the use of DM technology might mitigate the effects of social vulnerability on glycemic outcomes. This study also indicates that pump usage alone could eliminate racial disparities in improving A1c levels among youth with T1DM. While we recognize the clinical advantages of automated insulin delivery systems, we also note that access to these systems is limited both globally around the world and within the US. Consequently, our analysis focused on the independent use of pumps and CGMs rather than their combined use. Additionally, we recognize that our study methodology prevented an assessment of impact of CGM metrics such as time in range and wear time; however, we used HbA1c as an appropriate and standard method for assessing glycemic control because it reflects the average blood glucose over time and predicts diabetes complications. We expect a wide variability in how patients approach technology among the patients included in this populational study; but our results still demonstrate the positive association between technology use and glycemic control across the socioeconomic spectrum. Despite limitations on generalizability to areas with no technology delivery gaps, these data emphasize the need for national and global advocacy to reduce disparities in diabetes care delivery, particularly within payer systems that impose high eligibility requirements for access to diabetes technology. Moreover, this data challenges prescribing practices that require patients to achieve glycemic control benchmarks without technological assistance prior to gaining access to such technology. Lastly, we recognize that due to the study’s time frame, we are unable to determine the potential influence of the COVID-19 pandemic on glycemic control and the uptake of diabetes technology in this population.
Conclusions
This study highlights the disparities in the use of diabetes technology and glycemic control among disadvantaged and socially vulnerable populations. Although hybrid closed-loop systems are becoming more commonly used, many patients worldwide still lack access to this technology. This study highlights that both insulin pump and CGM use alone can effectively lower HbA1c levels across all groups, with greater improvements observed in patients of lower socioeconomic background. Therefore, further research is needed to better understand the factors contributing to disparities in diabetes technology usage. This understanding can lead to new interventions aimed to mitigate and address the racial and socioeconomic inequalities faced by youth with type 1 diabetes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lee MY, Tanenbaum ML, Maahs DM, Prahalad P. Overcoming barriers to diabetes technology in youth with type 1 diabetes and public insurance: cases and call to action. Case Rep Endocrinol. 2022, 2022;9911736. 10.1155/2022/9911736.10.1155/2022/9911736 PMC 890409435273814 · doi ↗ · pubmed ↗
- 2Tremblay ES, Bernique A, Garvey K, Astley CM. A retrospective cohort study of racial/ethnic and socioeconomic disparities in initiation and meaningful use of Continuous glucose monitoring among youth with type 1 diabetes. J Diabetes Sci Technol. Published online July 3, 2023: 19322968231183985. 10.1177/19322968231183985.10.1177/19322968231183985 PMC 1153105237394962 · doi ↗ · pubmed ↗
- 3S M, O E, N N, et al. Inequities in health outcomes in children and adults with type 1 diabetes: data from the T 1D exchange quality improvement collaborative. Clin Diabetes: A Publ Of The Am Diabetes Assoc. 2021;39(3). 10.2337/cd 21-0028.10.2337/cd 21-0028 PMC 832900934421203 · doi ↗ · pubmed ↗
- 4Sm O, Sh G. Social determinants of health and structural inequities-root causes of diabetes disparities. Diabetes Care. 2021;44(1). 10.2337/dci 20-0060.10.2337/dci 20-006033571949 · doi ↗ · pubmed ↗
- 5M AB, Nk S, As B, R E. Insulin pumps in children - a systematic review. World J Clin Pediatrics. 2022;11(6). 10.5409/wjcp.v 11.i 6.463.10.5409/wjcp.v 11.i 6.463PMC 968568036439904 · doi ↗ · pubmed ↗
- 6Blackman SM, Raghinaru D, Adi S, et al. Insulin pump use in young children in the T 1D Exchange clinic registry is associated with lower hemoglobin A 1c levels than injection therapy. Pediatr Diabetes. 2014;15(8):564–72. 10.1111/pedi.12121.10.1111/pedi.1212124494980 · doi ↗ · pubmed ↗