Oncological safety and preventive impact of nipple-sparing mastectomy in patients with BRCA1/2 mutation: multicentre study of the Korea Robot-endoscopy Minimal Access Breast Surgery Study Group (KoREa-BSG)
Hong-Kyu Kim, Dong Seung Shin, Sung Yoon Jang, Soong June Bae, Eun Young Kim, Chihwan David Cha, Hyung Seok Park, Jeeyeon Lee, Jun-Hee Lee, Eun-Shin Lee, Jung Eun Choi, Soo Youn Bae, Hee-Chul Shin, Dongwon Kim, Moo Hyun Lee, Yong-Yeup Kim, Sang-Ah Han, Janghee Lee

TL;DR
Nipple-sparing mastectomy is a safe and effective option for BRCA1/2 mutation carriers, with similar recurrence rates and reduced risk of contralateral breast cancer.
Contribution
Demonstrates NSM's oncological safety and preventive impact in BRCA1/2 carriers, particularly in Asian populations.
Findings
Ipsilateral local recurrence rates were similar between BRCA1/2 carriers and non-carriers.
Contralateral breast cancer occurred in 4.5% of BRCA1/2 carriers who did not undergo risk-reducing NSM.
No contralateral breast cancer cases were observed in patients who underwent risk-reducing NSM.
Abstract
Nipple-sparing mastectomy (NSM) is a surgical option offering both oncological safety and cosmetic benefits. However, the oncological safety of NSM in carriers of BRCA1/2 pathogenic variants/likely pathogenic variants (PV/LPV) with breast cancer and the role of risk-reducing mastectomy remain underexplored, especially in Asian populations. This study evaluated the safety and effectiveness of NSM in BRCA1/2 PV/LPV carriers and assessed the preventive impact of contralateral risk-reducing NSM (RRNSM) on cancer incidence. This multicentre retrospective study included women aged 20–80 years who underwent NSM for therapeutic or risk-reducing purposes and received germline BRCA1/2 tests between May 2006 and June 2022 across 19 institutions in Korea. Patients with distant metastasis at diagnosis were excluded. Information on demographics, the clinical characteristics of patients and tumours,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
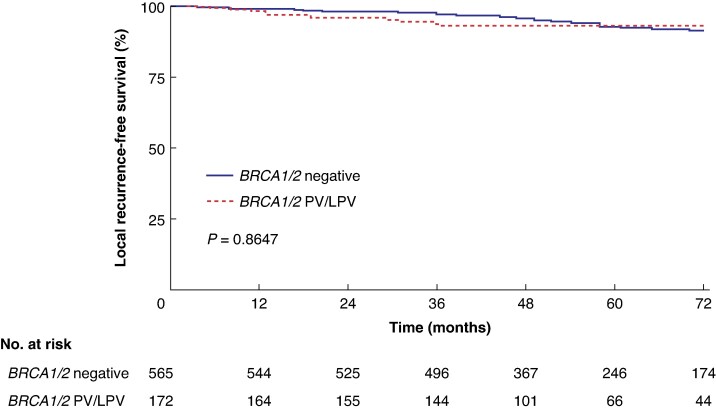 Fig. 1
Fig. 1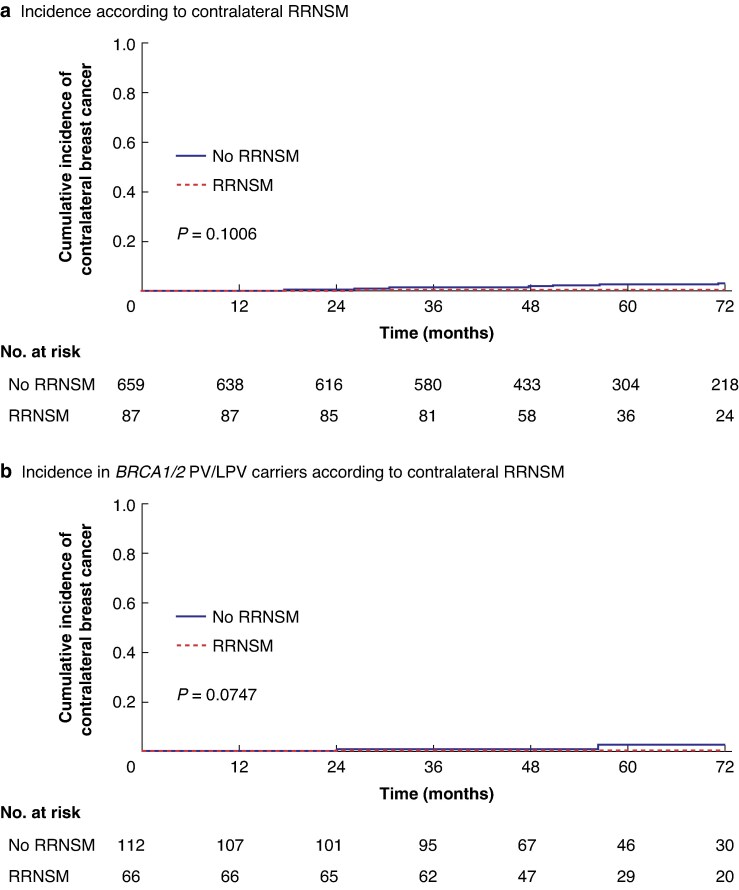 Fig. 2
Fig. 2| All patients ( |
|
| |
|---|---|---|---|
|
| |||
| Unilateral NSM (Group A) | 659 | 547 (91.0%) | 112 (60.2%) |
| Unilateral TM + contralateral RRNSMA (Group B) | 9 | 3 (0.5%) | 6 (3.2%) |
| Unilateral NSM + contralateral RRNSMA (Group C) | 78 | 18 (3.0%) | 60 (32.3%) |
|
| |||
| Bilateral NSM | 39 | 33 (5.5%) | 6 (3.2%) |
|
| 2 | 0 (0.0%) | 2 (1.1%) |
| AResults of contralateral RRNSM ( | 87 | 21 | 66 |
| Benign tumour after contralateral RRNSM | 85 | 20 | 65 |
| Incidental cancer after contralateral RRNSM | 2 | 1 | 1 |
| BResults of bilateral RRNSM ( | 2 | 0 | 2 |
| Benign tumour after bilateral RRNSM | 2 | 0 | 2 |
| Incidental cancer after bilateral RRNSM | 0 | 0 | 0 |
| Variables |
|
|
|
|---|---|---|---|
| Age at operation (years), median (i.q.r.) | 39 (35–46) | 37 (34–42) | 0.002 |
| Follow-up duration (months), median (i.q.r.) | 59.6 (44.8–83.8) | 55.4 (42.3–76.6) | 0.092 |
|
| 0.024 | ||
| pTis | 134 (22.3%) | 40 (21.7%) | |
| pT1 | 290 (48.3%) | 102 (55.4%) | |
| pT2 | 143 (23.8%) | 34 (18.5%) | |
| pT3 | 26 (4.3%) | 2 (1.1%) | |
| pT4 | 2 (0.3%) | 0 (0.0%) | |
| Unknown | 6 (1.0%) | 6 (3.3%) | |
|
| 0.216 | ||
| pN0 | 435 (72.4%) | 124 (67.4%) | |
| pN1 | 125 (20.8%) | 44 (23.9%) | |
| pN2 | 23 (3.8%) | 6 (3.3%) | |
| pN3 | 12 (2.0%) | 4 (2.2%) | |
| Unknown | 6 (1.0%) | 6 (3.3%) | |
|
| 0.001 | ||
| No | 9 (1.5%) | 13 (7.1%) | |
| SLNB | 455 (75.7%) | 124 (67.4%) | |
| SLNB followed by ALND | 122 (18.6%) | 39 (21.2%) | |
| ALND | 25 (4.2%) | 8 (4.3%) | |
|
| <0.001 | ||
| Positive | 473 (78.7%) | 103 (56.0%) | |
| Negative | 102 (17.0%) | 60 (32.6%) | |
| Unknown | 26 (4.3%) | 21 (11.4%) | |
|
| 0.003 | ||
| Positive | 128 (21.3%) | 22 (12.0%) | |
| Negative | 383 (63.7%) | 120 (65.2%) | |
| Unknown | 90 (15.0%) | 42 (22.8%) | |
|
| <0.001 | ||
| HR+/HER2− | 338 (56.2%) | 70 (38.0%) | |
| HR+/HER2+ | 80 (13.3%) | 15 (8.2%) | |
| HR−/HER2+ | 48 (8.0%) | 7 (3.8%) | |
| HR−/HER2− | 45 (7.5%) | 50 (27.2%) | |
| Unknown | 90 (15.0%) | 42 (22.8%) | |
|
| <0.001 | ||
| < 20% | 390 (64.9%) | 87 (47.3%) | |
| ≥ 20% | 206 (34.3%) | 91 (49.5%) | |
| Unknown | 5 (0.8%) | 6 (3.3%) | |
|
| <0.001 | ||
| Grade 1 | 57 (9.5%) | 5 (2.7%) | |
| Grade 2 | 304 (50.6%) | 74 (40.2%) | |
| Grade 3 | 121 (20.1%) | 63 (34.2%) | |
| Unknown | 119 (19.8%) | 42 (22.8%) |
| Study | No. institutions | Country | Sample size ( | No. of NSM procedures | No. of | Objective | Median follow-up duration (months) | Key findings |
|---|---|---|---|---|---|---|---|---|
| Stanek | Single | Czech Republic | 105 | 210 | 105 | Risk-reducing effectiveness of NSM | 50 | Cancer rates: NSM group, 0%; surveillance group, 8.6% cancer |
| Garstka | Single | Germany | 307 | 607 | 307 | Ipsilateral recurrence rates in NSM | 42 | No new cancers in prophylactic NSM |
| Manning | Single | USA | 89 | 177 | 89 | Indications and outcomes in | 28 | Therapeutic NSM: no recurrence |
| Webster | Single | USA | 105 | 114 | 105 | Long-term oncological safety of NSM | 70 | 2.6% locoregional recurrence |
| Valero | Single | USA | 192 | 384 | 117 | Outcomes of bilateral prophylactic NSM | 36.8 | 0% new breast cancer diagnoses |
| Jakub | Multiple | USA | 346 | 548 | 346 | Oncological safety of prophylactic NSM for | 34 | No new breast cancers occurred |
- —Korean Society of Surgical Oncology
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBreast Implant and Reconstruction · BRCA gene mutations in cancer · Breast Cancer Treatment Studies
Introduction
Nipple-sparing mastectomy (NSM) with reconstruction preserves the nipple–areola complex, potentially improving patient satisfaction with body image compared with skin-sparing mastectomy (SSM). A recent systematic review^1^ further support generally positive psychosocial outcomes associated with risk-reducing mastectomy (RRM), although patient-reported experiences regarding aesthetic results and body image vary, emphasizing the need for the cautious interpretation of these findings. NSM, by keeping the nipple–areola complex while removing the underlying breast tissue, marks a significant advance in breast cancer management, providing both oncological safety and cosmetic benefits^2–5^. Several studies^6–8^ have demonstrated that NSM achieves comparable oncological outcomes to SSM or conventional total mastectomy, with no significant difference in recurrence rates and overall survival. Furthermore, NSM is increasingly being used for patients undergoing neoadjuvant chemotherapy and those with locally advanced breast cancer, particularly when immediate reconstruction is planned^9,10^.
Although many studies have been reported on the oncological outcomes of NSM, there is very limited data on its safety and effectiveness in patients with pathogenic variants (PV) or likely pathogenic variants (LPV) of the BRCA1/2 genes. Given that BRCA1/2-related breast cancers are often diagnosed at a younger age and tend to have more aggressive tumour biology, evaluating the safety of NSM in this subgroup is crucial^11,12^. In particular, there have been no studies investigating the oncological outcomes of NSM in patients with BRCA1/2-related breast cancer in an Asian population.
In BRCA1/2 PV/LPV carriers diagnosed with breast cancer, the risk of contralateral breast cancer (CBC) events increases progressively over time, with cumulative incidence rates reaching 23% for BRCA1 and 17% for BRCA2 mutation patients at 10 years after the initial diagnosis^13^. These findings highlight the critical need for personalized surveillance plans and risk-reducing strategies, including surgical interventions with NSM, to address cancer risks in this high-risk population. Moreover, the role of NSM as a preventive measure in unaffected carriers of BRCA1/2 PV/LPV also needs thorough investigation. These individuals frequently struggle with the decision whether to undergo preventive surgeries to reduce their risk of cancer. It is therefore essential to determine whether NSM can serve as an effective risk-reducing strategy for these high-risk individuals, while maintaining as high a quality of life and satisfaction as possible.
The aims of this study were to assess the oncological outcomes of NSM for patients with breast cancer with BRCA1/2 PV/LPV and the contralateral preventive effectiveness of NSM in these high-risk patients.
Methods
Study population and data collection
A multicentre retrospective study was conducted by the Korea Robot-endoscopic Minimal Access Breast Surgery Study Group (KoREa-BSG), a surgical study group within the Korean Breast Cancer Society. As part of this study, women who underwent NSM and received germline BRCA1/2 tests between May 2006 and June 2022 were retrospectively identified across 19 institutions in Korea. The study included women aged 20–80 years who underwent NSM, regardless of whether the surgery was for therapeutic or risk-reducing purposes. Individuals who were diagnosed with distant metastasis at the initial presentation were excluded from the study.
Information was collected on demographic data, the clinical characteristics of patients and tumours, surgical details, and follow-up outcomes from a review of the medical records of each participating institution. Pathological and clinical staging in this study were determined according to the 8th edition of the American Joint Committee on Cancer classification^14^. The results of germline BRCA1/2 testing were categorized into five groups: BRCA1 PV/LPV, BRCA2 PV/LPV, variants of uncertain significance, negative, and equivocal. Among these, individuals with variants of uncertain significance, negative, or equivocal results were collectively classified as BRCA negative for the purposes of analysis. According to the American College of Medical Genetics and Genomics guidelines^15^, the term ‘likely pathogenic’ is used for variants with greater than 90% certainty of being disease causing even though they do not yet meet the highest level of evidence required for definitive pathogenic classification. Therefore, LPVs are routinely categorized alongside PVs for clinical analyses and decision-making.
Locoregional recurrence was defined as any recurrence occurring in the ipsilateral chest wall, skin, subcutaneous tissue, or pectoralis muscle, which was categorized as local recurrence, or within the ipsilateral axillary, supraclavicular, internal mammary, or infraclavicular lymph nodes, which was classified as regional recurrence. Distant metastasis was defined as any recurrence occurring outside the regions classified under local recurrence or regional recurrence. Data on recurrence events were extracted from electronic medical records, whereas survival information was sourced from both institutional electronic records and the Korean National Statistical Office database.
In this study, postoperative surveillance generally followed the clinical guidelines of the Korean Breast Cancer Society. According to these guidelines, physical examination and history taking are performed during outpatient clinic visits every 6 months for the first 3 years, every 6–12 months for the next 2 years, and annually thereafter. Imaging of the breast, including mammography or breast ultrasound, is performed every 6–12 months, with breast magnetic resonance imaging added if clinically indicated. Systemic imaging to detect distant metastasis was performed every 6–12 months as needed, depending on the patient’s disease stage.
The primary outcome in this study was the oncological safety of NSM, assessed by comparing ipsilateral local recurrence rates between patients with and without BRCA1/2 PV/LPV. The secondary outcome was cancer incidence in patients who underwent contralateral risk-reducing NSM (RRNSM) versus those who did not.
This study was conducted in accordance with the ethical principles of the Declaration of Helsinki. The study was approved by the Institutional Review Board of Samsung Medical Center (Approval no. 2022-01-195), as well as the institutional review boards of each participating institution. The requirement for informed consent was waived because of the retrospective nature of the study.
Statistical analysis
Variables were compared between groups using the χ^2^ test or Fisher's exact test for categorical variables and the t test or Wilcoxon rank-sum test for continuous variables. Kaplan–Meier curves were generated for local recurrence-free survival, regional recurrence-free survival, distant metastasis-free survival, and overall survival with the corresponding outcomes of log-rank tests. All statistical analyses were conducted using SPSS^®^ version 27 (IBM, Armonk, NY, USA) and R version 4.2.2 (Foundation for Statistical Computing, Vienna, Austria). All statistical tests were two-sided, with P < 0.050 considered statistically significant, and results are reported with 95% confidence intervals (c.i.).
Results
Patient demographics
In all, 787 women (906 NSMs) were included in the study. There were two unaffected individuals with BRCA1/2 PV/LPV who underwent bilateral RRNSMs. The median follow-up period was 59.3 (interquartile range 44.0–82.8) months, and the median age of the cohort was 39 (range 23–79) years. Sentinel lymph node biopsy (SLNB) was performed in 784 NSMs (86.5%, 784 of 906) and 198 patients (25.2%, 198 of 785) received neoadjuvant chemotherapy.
Among the 746 patients with unilateral breast cancer, 659 underwent unilateral NSM only, 78 underwent unilateral NSM with contralateral RRNSM, and nine underwent unilateral total mastectomy with contralateral RRNSM, with 112, 60, and six BRCA1/2 PV/LPV carriers in each group, respectively. In addition, the cohort included 39 patients with bilateral breast cancer who underwent bilateral NSM, of whom six were BRCA1/2 PV/LPV carriers and 33 were non-carriers (Table 1).
Among the 785 patients with breast cancer, excluding the two unaffected individuals with BRCA1/2 PV/LPV who underwent bilateral RRNSMs, there were differences in baseline characteristics between the BRCA1/2 PV/LPV and BRCA1/2-negative groups (Table 2). The number of patients aged ≤ 40 years was significantly higher in the BRCA1/2 PV/LPV than BRCA1/2-negative group (69.6 versus 59.7%, respectively; P =0.039). In addition, the BRCA1/2 PV/LPV group had a higher proportion of patients who were hormone receptor-negative (32.6 versus 17.0%; P < 0.001) and a higher prevalence of triple-negative breast cancer (27.2 versus 7.5%, P < 0.001). The proportion of patients with a Ki-67 index ≥ 20% was also significantly higher in the BRCA1/2 PV/LPV than BRCA1/2-negative group (49.5 versus 34.3%; P < 0.001), suggesting a more aggressive tumour biology in the BRCA1/2 PV/LPV cohort. Regarding axillary surgery, the distribution differed significantly between the two groups (P = 0.001), with the BRCA1/2 PV/LPV group having a higher proportion of patients undergoing axillary lymph node dissection following SLNB (21.2 versus 18.6%), as well as a higher overall rate of axillary lymph node dissection (25.5 versus 22.8%).
Results of BRCA1/2 genetic testing
In this retrospective study, BRCA1 and BRCA2 PV/LPV were identified in 85 (10.8%) and 101 (12.8%) individuals, respectively (Table S1). Most individuals were confirmed negative for BRCA1/2 mutations (522 patients, 66.3%). Variants of unknown significance and equivocal results were identified in 76 (9.7%) and 3 (0.4%) patients, respectively.
Ipsilateral local recurrence (oncological outcomes of NSM according to BRCA1/2 mutation status)
To evaluate the oncological safety of NSM in BRCA1/2 PV/LPV carriers, ipsilateral local recurrence rates were analysed according to BRCA1/2 mutation status. For this analysis, patients with unilateral breast cancer who underwent ipsilateral NSM were selected (Table 1, groups A and C). No significant difference in local recurrence was observed between the 172 patients with BRCA1/2 PV/LPV and the 565 patients without BRCA1/2 PV/LPV. Specifically, 11 local recurrence events (6.4%, 11 of 172) occurred in the BRCA1/2 PV/LPV group, compared with 42 events (7.4%, 42 of 565) in the BRCA1/2-negative group. There was no significant difference in local recurrence-free survival between the two groups (log-rank P = 0.865; Fig. 1). Furthermore, no significant differences were noted in regional recurrence-free survival, distant metastasis-free survival, or overall survival (log-rank P = 0.707, P = 0.156, and P = 0.373, respectively; Fig. S1).
Ipsilateral local recurrence-free survival in patients with unilateral nipple-sparing mastectomy according to BRCA1/2 statusThis analysis evaluated the impact of nipple-sparing mastectomy on ipsilateral local recurrence-free survival in 737 patients with unilateral breast cancer (after excluding nine patients who underwent unilateral total mastectomy). The P value was calculated using a log-rank test. PV/LPV, pathogenic variant/likely pathogenic variant.
CBC occurrence (impact of RRNSM on CBC incidence)
To evaluate the impact of RRNSM on CBC, the incidence of CBC was analysed according to BRCA1/2 mutation status. For this analysis, patients with unilateral breast cancer were selected and classified into two groups according to whether or not they underwent contralateral RRNSM (Table 1, group A versus groups B + C). Among the 659 patients with unilateral NSM who did not undergo RRNSM, CBC occurred in 22 patients (3.3%), whereas no cases were reported among the 87 patients who underwent RRNSM. There was no significant difference in cumulative CBC occurrence between the two groups (log-rank P = 0.101; Fig. 2a). In the subgroup of 178 patients with BRCA1/2 PV/LPV, CBC occurred in five of 112 patients (4.5%) who did not undergo RRNSM, whereas no cases were observed among the 66 patients who underwent RRNSM. Kaplan–Meier survival analysis in this subgroup also demonstrated no statistically significant difference in cumulative CBC occurrence between the two groups (log-rank P = 0.075; Fig. 2b).
Cumulative incidence of contralateral breast cancer according to contralateral RRNSM status a Cumulative incidence of contralateral breast cancer in patients with unilateral breast cancer who did not (659 patients) or did (87 patients) undergo contralateral RRNSM. b Cumulative incidence of contralateral breast cancer in patients identified as BRCA1/2 PV/LPV carriers who did not (112 patients) or did (66 patients) undergo contralateral RRNSM. The P values were calculated using log-rank tests. RRNSM, risk-reducing nipple-sparing mastectomy; PV/LPV, pathogenic variant/likely pathogenic variant.
Pathological results of RRNSM
Among the patients with unilateral breast cancer, 87 underwent contralateral RRNSM for risk reduction, including 66 with BRCA1/2 PV/LPV and 21 without. Among these 87 patients with contralateral RRNSM, benign tumours were found in 85 (65 with BRCA1/2 PV/LPV and 20 without), whereas incidental ductal carcinoma in situ was identified in two patients, one with BRCA1/2 PV/LPV and one without. In addition, two individuals underwent bilateral RRNSMs, both of whom were BRCA1/2 PV/LPV carriers. The final pathological report of both breasts in these carriers revealed only benign tumours, with no incidental cancer identified.
Discussion
The results of this study demonstrate that NSM is a viable and safe surgical option for patients with breast cancer with BRCA1/2 PV/LPV, showing no significant difference in ipsilateral local recurrence rates between BRCA1/2 PV/LPV carriers and non-carriers. Furthermore, the risk-reducing potential of contralateral RRNSM was evident, because no cases of CBC were observed among individuals with BRCA1/2 PV/LPV who underwent the procedure, although no statistically significant difference was observed. The findings of the present multicentre, retrospective study provide valuable insights into the oncological safety and preventive benefits of NSM in patients with BRCA1/2 PV/LPV.
One of the primary concerns regarding NSM in BRCA1/2 PV/LPV carriers has been the potential risk of local recurrence due to the preservation of the nipple–areola complex. However, recent studies^4,16–20^ have reported on the oncological safety of NSM as a risk-reducing mastectomy option for BRCA1/2 PV/LPV carriers (Table 3). Jakub et al.^18^ analysed 548 cases of prophylactic NSM in 346 BRCA mutation carriers across multiple institutions, reporting no new breast cancer events during a median follow-up of 34 months. Valero et al.^21^ evaluated 384 bilateral prophylactic NSMs in 192 patients, including 117 BRCA1/2 mutation carriers, and found no new breast cancer cases during a median follow-up of 36.8 months. Similarly, Webster et al.^4^ conducted a long-term analysis of 114 cases of therapeutic NSM in 105 BRCA1/2 mutation carriers over a median follow-up of 70 months, reporting a locoregional recurrence rate of only 2.6%. To date, there is a notable lack of research on the safety of NSM or RRNSM in BRCA1/2 PV/LPV carriers within the Asian population^22^. The present study bridges this gap as the first and largest multicentre cohort in Asia to evaluate oncological outcomes and the preventive potential of NSM in this high-risk group. The findings of no significant difference in ipsilateral local recurrence rates between BRCA1/2 PV/LPV carriers and non-carriers align with those of previous studies, suggesting that NSM offers comparable oncological safety to conventional mastectomy techniques, even in high-risk populations.
Survival analyses in the present cohort revealed an interesting trend. Patients with BRCA1/2 PV/LPV experienced more frequent events early on, but the survival curves subsequently crossed during follow-up. This pattern could be explained by the more aggressive tumour biology and higher prevalence of the triple-negative subtype in the BRCA1/2 PV/LPV group, leading to earlier recurrence. Over time, however, the curves converge, suggesting that the initial adverse impact may diminish. It is also important to note that the risk of local recurrence could be underestimated, because patients who developed distant metastasis or died were censored and therefore not recorded for subsequent local events. These findings underscore the complexity of interpreting recurrence patterns in genetically high-risk populations.
A previous systematic review and meta-analysis^23^ and a study^24^ have reported that, among patients undergoing breast-conserving surgery, BRCA1/2 mutation carriers have a higher risk of ipsilateral breast tumour recurrence than non-carriers^23,24^. However, a recent study by Moshe et al.^25^ analysing patients who underwent SSM or NSM reported that BRCA1/2 mutation status did not affect the local recurrence rate. This may suggest that mastectomy has a more pronounced impact in reducing ipsilateral breast tumour recurrence, although further studies are warranted to confirm this. Regarding occult malignancy, studies conducted in various countries^26–28^ have shown that the incidence of occult malignancy in the contralateral breast undergoing RRM in BRCA1/2 mutation carriers ranges from 2.4 to 11.3%. In a recent study from a single institution in Korea^29^, among 320 breast cancer patients who underwent contralateral RRM, seven cases (2.2%) of occult malignancy were identified in BRCA1/2 mutation carriers. Similarly, the present study showed a low rate of incidental malignancy; however, given the small number of cases and the inclusion of only patients who underwent NSM, the generalizability of this finding is limited. In line with this, Thompson et al.^30^ reported that BRCA1/2 mutation status was not a statistically significant factor influencing the risk of occult malignancy in patients undergoing contralateral RRM. Further studies with larger cohorts and prospective randomized designs are needed to better understand the risk of local recurrence and incidental malignancy in BRCA1/2 mutation carriers.
Previous studies^31,32^ have reported that RRM reduces the risk of breast cancer; however, its overall survival benefit remains controversial. According to the most recent study by Blondeaux et al.^33^, RRM or risk-reducing salpingo-oophorectomy may provide overall survival gain in patients with BRCA1 mutations identified before the age of 40 years. In addition, long-term follow-up results for patients with triple-negative breast cancer with confirmed BRCA1/2 mutations showed that 82.8% of CBC events were of the triple-negative breast cancer subtype, and 62.5% of these patients received systemic chemotherapy again^34^. Therefore, from a long-term perspective, patients may opt for RRM considering the future risk of CBC and their personal preferences. Compared with conventional mastectomy or SSM, both of which do not preserve the nipple–areolar complex, NSM has been associated with greater patient satisfaction, particularly in terms of sexual and psychosocial wellbeing^35^. Therefore, choosing NSM with immediate reconstruction can offer the benefits of risk reduction and potentially favourable oncological outcomes, while also aiming to enhance overall patient satisfaction. In particular, the cohort in the present study had a relatively young median age of 39 years. Given the long life expectancy in this population, multiple factors need to be considered, including oncological outcomes of surgery, cosmetic benefits, quality of life, fertility preservation, and family planning. In this context, a multidisciplinary approach and shared decision-making that focuses on tailoring treatment strategies to patient preferences and clinical factors should be further highlighted.
With recent advances in minimal access breast surgery, robot-assisted NSM (RANSM) has emerged as a new option for NSM. RANSM has demonstrated favourable oncological outcomes and superior cosmetic results in women with early breast cancer or BRCA mutations, with multiple studies^36–39^ reporting no significant difference in complication rates compared with conventional NSM while maintaining postoperative quality of life. Several ongoing multicentre trials, including randomized studies in Korea (NCT05490433) and the USA (NCT05720039), are currently evaluating the safety, oncological outcomes, and patient satisfaction associated with RANSM^40^. The findings from these studies are expected to provide valuable insights into whether RANSM can serve as an alternative to conventional NSM for high-risk patients, and whether it could offer superior oncological outcomes and patient satisfaction as a risk-reducing technique.
Although this study provides important evidence supporting the oncological safety of NSM in patients with BRCA1/2 PV/LPV, several limitations should be noted. First, the retrospective design may have introduced selection bias, and the relatively short median follow-up period of 60 months may not fully capture long-term recurrence patterns. However, although several studies have assessed the oncological safety of NSM in BRCA mutation carriers, most have been limited to single-centre cohorts, and multicentre data remain limited. In particular, evidence from Asian populations is notably lacking. This appears to be the first multicentre retrospective analysis conducted in an Asian population that includes patients who underwent NSM with known BRCA1/2 PV/LPV status. By analysing oncological outcomes and the preventive effect of NSM on contralateral breast cancer in this genetically high-risk population, the present study helps fill an important gap in the literature and provides clinically meaningful insights into the surgical management of BRCA mutation carriers.
Second, although multivariable analysis could have improved the validity of recurrence and survival outcomes by adjusting for confounding factors, it was not feasible due to incomplete and inconsistent reporting of key variables such as adjuvant treatment details, Ki-67 index, and other potential prognostic factors across participating institutions. Moreover, the influence of unmeasured or unknown confounding factors could not be excluded due to the retrospective design of the study.
Third, data on bilateral salpingo-oophorectomy status, a known protective factor for breast cancer development, contralateral events, and recurrence, were not comprehensively collected. Therefore, the potential influence of bilateral salpingo-oophorectomy could not be evaluated in this study.
Future prospective, multicentre studies with standardized data collection and longer follow-up are warranted to confirm these findings and provide further insights into the preventive and therapeutic impacts of NSM in high-risk populations.
In this retrospective study, NSM was found to be a safe and effective surgical option for patients with breast cancer with BRCA1/2 PV/LPV. It was associated with a low risk of ipsilateral local recurrence and a reduced incidence of CBC in affected BRCA1/2 PV/LPV carriers. These findings support the consideration of NSM as a potential surgical approach in the management of high-risk patients and may contribute to improved quality of life. Further research is needed to validate these findings and to explore the long-term impact of NSM in this population.
Collaborators
The members of the KoREa-BSG are: Joo Heung Kim (Department of Surgery, Yongin Severance Hospital, Yonsei University College of Medicine, Yongin, Korea); Beom Seok Ko (Department of Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea); Ku Sang Kim (Department of Surgery, Kosin University College of Medicine, Gospel Hospital, Busan, Korea); Young Jin Choi (Department of Surgery, Chungbuk National University Hospital, Cheongju, Korea); Hye Yoon Lee (Department of Surgery, Korea University Ansan Hospital, Ansan, Korea); Sang Eun Nam (Department of Surgery, Konkuk University School of Medicine, Seoul, Korea); Zisun Kim (Department of Surgery, Soonchunhyang University Bucheon Hospital, Bucheon, Korea); Jong Eun Lee (Department of Surgery, Soonchunhyang University Cheonan Hospital, Cheonan, Korea); Eunhwa Park (Department of Surgery, Dong-A University Hospital, Dong-A University College of Medicine, Busan, Korea); Hyuk Jai Shin (Department of Surgery, Myongji Hospital, Hanyang University Medical Center, Goyang, Korea); Min Kyoon Kim (Department of Surgery, Chung-Ang University Hospital, Seoul, Korea); Seong Uk Kwon (Department of Surgery, Konyang University Hospital, Daejeon, Korea); Jeea Lee (Department of Surgery, Uijeongbu Eulji Medical Center, Eulji University, Uijeongbu, Korea); and Jee Ye Kim (Department of Surgery, Yonsei University College of Medicine, Seoul, Korea).
Supplementary Material
zraf168_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ntowe KW, Lee MS, Yi VN, Kaplan SJ, Phillips BT, Chiba A et al Short-term patient-reported outcomes following bilateral risk-reducing mastectomy for patients at a high risk for breast cancer: a systematic review. Ann Surg Oncol 2025;32:2510–252539755890 10.1245/s 10434-024-16805-5PMC 11888891 · doi ↗ · pubmed ↗
- 2Galimberti V, Vicini E, Corso G, Morigi C, Fontana S, Sacchini V et al Nipple-sparing and skin-sparing mastectomy: review of aims, oncological safety and contraindications. Breast 2017;34(Suppl 1):S 82–S 8428673535 10.1016/j.breast.2017.06.034PMC 5837802 · doi ↗ · pubmed ↗
- 3Galimberti V, Morigi C, Bagnardi V, Corso G, Vicini E, Fontana SKR et al Oncological outcomes of nipple-sparing mastectomy: a single-center experience of 1989 patients. Ann Surg Oncol 2018;25:3849–385730225833 10.1245/s 10434-018-6759-0 · doi ↗ · pubmed ↗
- 4Webster AJ, Shanno JN, Santa Cruz HS, Kelly BN, Garstka M, Henriquez A et al Oncologic safety of nipple-sparing mastectomy for breast cancer in BRCA gene mutation carriers: outcomes at 70 months median follow-up. Ann Surg Oncol 2023;30:3215–322236604360 10.1245/s 10434-022-13006-w · doi ↗ · pubmed ↗
- 5Kelly BN, Faulkner HR, Smith BL, Korotkin JE, Lanahan CR, Brown C et al Nipple-sparing mastectomy versus skin-sparing mastectomy: does saving the nipple impact short- and long-term patient satisfaction? Ann Surg Oncol 2022;29:1033–104034498158 10.1245/s 10434-021-10767-8 · doi ↗ · pubmed ↗
- 6Moo TA, Pinchinat T, Mays S, Landers A, Christos P, Alabdulkareem H et al Oncologic outcomes after nipple-sparing mastectomy. Ann Surg Oncol 2016;23:3221–322527380643 10.1245/s 10434-016-5366-1 · doi ↗ · pubmed ↗
- 7Petit JY, Veronesi U, Orecchia R, Curigliano G, Rey PC, Botteri E et al Risk factors associated with recurrence after nipple-sparing mastectomy for invasive and intraepithelial neoplasia. Ann Oncol 2012;23:2053–205822231025 10.1093/annonc/mdr 566 · doi ↗ · pubmed ↗
- 8Wu ZY, Kim HJ, Lee JW, Chung IY, Kim JS, Lee SB et al Breast cancer recurrence in the nipple–areola complex after nipple-sparing mastectomy with immediate breast reconstruction for invasive breast cancer. JAMA Surg 2019;154:1030–103731461141 10.1001/jamasurg.2019.2959 PMC 6714008 · doi ↗ · pubmed ↗